
Abstract
Background
Malignancies affecting the gastrointestinal tract are among the principal threats to global public health. In Ghana, these cancers are responsible for a significant number of hospitalizations and mortalities at major health facilities across the country. The increasing incidence of these malignancies necessitates an investigation of the association between lifestyle (modifiable risk factors) and these disorders.
Main Objective
To determine the association between lifestyle and gastrointestinal cancers of patients attending the Korle Bu Teaching Hospital (KBTH).
Study Design
This was a cross-sectional prospective study where demographic data were obtained from consenting patients diagnosed with gastrointestinal cancer at the oncology and surgical clinics of the KBTH. Diagnostic investigations, gastrointestinal cancer phenotype, year of diagnosis and treatment(s) received were also obtained from the participants. Information on smoking status, alcohol consumption, sources of dietary proteins, daily intake of water, and frequency of fruit intake were also obtained from the participants. Odds ratio and P-values were determined to ascertain whether there might be a significant association between gastrointestinal cancers and specified lifestyle.
Results
Colorectal cancers were the most prevalent form of gastrointestinal cancers among the participants. Alcohol consumption or smoking habits were not significantly associated with onset of gastrointestinal cancers among the study participants. There was a significant association but weak correlation between red meat consumption and the colorectal cancer.
Conclusion
This study shows consumption of red meat to be a modifiable risk factor that is associated with lower gastrointestinal cancers in the study participants. Further longitudinal studies using large number of participants is needed for confirming the observations from this current study.
Introduction
Globally, cancers affecting the colon, stomach, liver and rectum are notable forms of gastrointestinal cancers, and they accounted for 20.1% of all new cancer cases for all ages and gender in the year 2020. 1 Other forms of gastrointestinal cancers that were recorded globally that year were cancers affecting the oesophagus, pancreas, oral cavity, gallbladder, salivary glands and anus, which together represented 8.9% of all new cancer cases. 1 In Ghana, liver cancer accounted for 14.4% (3452 cases) of all new cancer cases and was the highest cause of cancer-related deaths (3166 deaths) in the same year under review. 2 Cancer affecting the stomach (769 cases; 674 deaths) was also a notable form of gastrointestinal cancer in Ghana in the year 2020. 2 The remaining eight cancers collectively accounted for 1875 new gastrointestinal cancer cases and 1455 associated deaths in the year 2020, highlighting the very high rate of mortality of affected individuals in Ghana. Incidentally, liver and stomach cancers were more prevalent in males than females in Ghana, which suggests that gender is a probable risk factor for these gastrointestinal cancers. 2
Several risk factors have been identified to be associated with the incidence of cancer affecting the various components of the gastrointestinal tract. These factors are broadly classified as non-modifiable and modifiable risk factors.3,4 Increasing age and family history are non-modifiable risk factors usually associated with most cancer phenotypes, including gastrointestinal cancers.5,6 The lifestyle of an individual can also increase the risk of oncogenesis of the gastrointestinal tract aside a possible genetic disposition. This lifestyle (modifiable risk factors) include obesity, reduced physical activity, cigarette smoking, and increased consumption of salt, red meat and alcohol.5,7-13 In addition to these general risk factors, specific factors enhance the oncogenesis of selected components of the gastrointestinal tract. Helicobacter pylori infection is a risk factor that is usually associated with gastric cancers. 14 Mutations in human DNA mismatch repair genes (hMLH1, hMSH2 and hMSH6) have also been implicated in colorectal cancers. 15 Chronic liver disease, hepatitis infections and liver cirrhosis are risk factors for liver cancer. 16
Even though numerous studies have reported on risk factors associated with selected gastrointestinal cancers, there is the need to constantly review the role of these diverse risk factors on prevalence due to the consistent increase in incidence of the disease. For instance, the known causes of liver cancer in Ghana a decade ago may not necessarily be solely responsible for the increased incidence of the disease, as recorded in the year 2020, due to dynamic lifestyles. It is also crucial to constantly investigate country-specific lifestyles that have predominant implications on the prevalence of these diverse cancers. This study specifically investigated the current lifestyle of Ghanaian patients diagnosed with a gastrointestinal cancer in order to obtain insights on the association of lifestyle with the disease in Ghana.
Methodology
Study Design and Population
This was a cross-sectional prospective study of patients diagnosed with gastrointestinal cancer at the time of data collection (Figure S1). Participants for the study were selectively recruited from the oncology and surgical clinics of the Korle Bu Teaching Hospital (KBTH) from March - July 2020. Surgery is a major treatment option for most gastrointestinal cancers hence, the reason for choosing the Department of Surgery and the Radio-Oncology Unit of the KBTH as sites for recruitment of participants for this study.
Clinical information in hospital folders were used to identify gastroinetsinal cancer patients attending the oncology and surgical clinics of the KBTH. All patients that were initially identified for the study expressed their willingness to participate in the data collection (Figure S2). These patients were recruited for the study because they were not diagnosed with benign gastrointestinal tumors, were not too ill to answer the questionnaire and spoke a language for which a translator could be provided for data collection. Convenient paper questionnaire was used for collection of the relevant data from the study participants.
Ethical Consideration for the Study
Ethical approval for this study was obtained from the KBTH Institutional Review Board via the Department of Community Health (UGMS-CHDRC/080/2020) of the University of Ghana Medical School, Accra, Ghana. Prior to data collection, written informed consent was obtained from the patients for their anonymized information to be used for the purposes of this study.
Data Collection and Analysis
A paper-based questionnaire was designed to obtain information on the demographics, diagnostic investigations, gastrointestinal cancers, year of diagnosis and treatment(s) received by the study participants. Additional information on the smoking status, alcohol consumption, sources of dietary proteins, daily intake of water, and frequency of fruit intake were obtained from the participants using the questionnaire. The information on nutrition obtained from the study participants relied on their ability to vividly recollect the constituent composition of their dietary foods. All data were handled anonymously and confidentially. Anonymity was ensured by the use of codes generated from the respondents’ initials. Data were stored and analyzed electronically using Microsoft Office (Excel) version 2016. The occurrence of all categorical data obtained in this study were expressed as percentages or cumulative frequencies.
A 2×2 contingency table was generated and used to calculate the odds ratio at 95% confidence interval for each category of GI cancers and a specified lifestyle. 17 For each contingency table, patients diagnosed with a category of GI cancers under consideration was considered as bad outcome and all other patients were classified as a control group for that category of GI cancers. P-values were calculated in Microsoft Office (Excel) version 2016 using the upper and lower limits of the 95% confidence interval and z-statistic from each odds ratio calculation. P-value<.05 was considered statistically significant. The lifestyle of the study participants that were investigated for their association with gastrointestinal cancers were history of smoking, alcohol consumption, red meat consumption, seafood consumption, poultry and products consumption, and consumption of dietary plant proteins. Infrequent intake of fruits and insufficient daily water intake were also investigated for their association with gastrointestinal cancers.
The reporting of this study conforms to STROBE guidelines. 18
Results
Demographic Information of the Study Participants
Demographic information of the study participants.

Total number of respondents = 115.
aOne participant was recorded for each of the 10 indicated ethnicities.
Types of Gastrointestinal Cancers and Therapies Received by the Study Participants
Gastrointestinal cancers identified in the study participants.

Anal, colorectal and illeocaecal cancers were categorized as Lower GI cancers. Liver, pancreatic and gallbladder cancers were categorized as Mid-GI cancers. Oesophageal and gastric cancers were classified as Upper GI cancers. Total number of respondents = 115.

Analysis of forms of gastrointestinal cancers affecting the study participants. a. Gender of the study participants. b. Year of diagnosis of the gastrointestinal cancer. Coloured legends denote the forms of gastrointestinal cancers. Total number of participants (n) = 115.
Treatments received by the study participants.
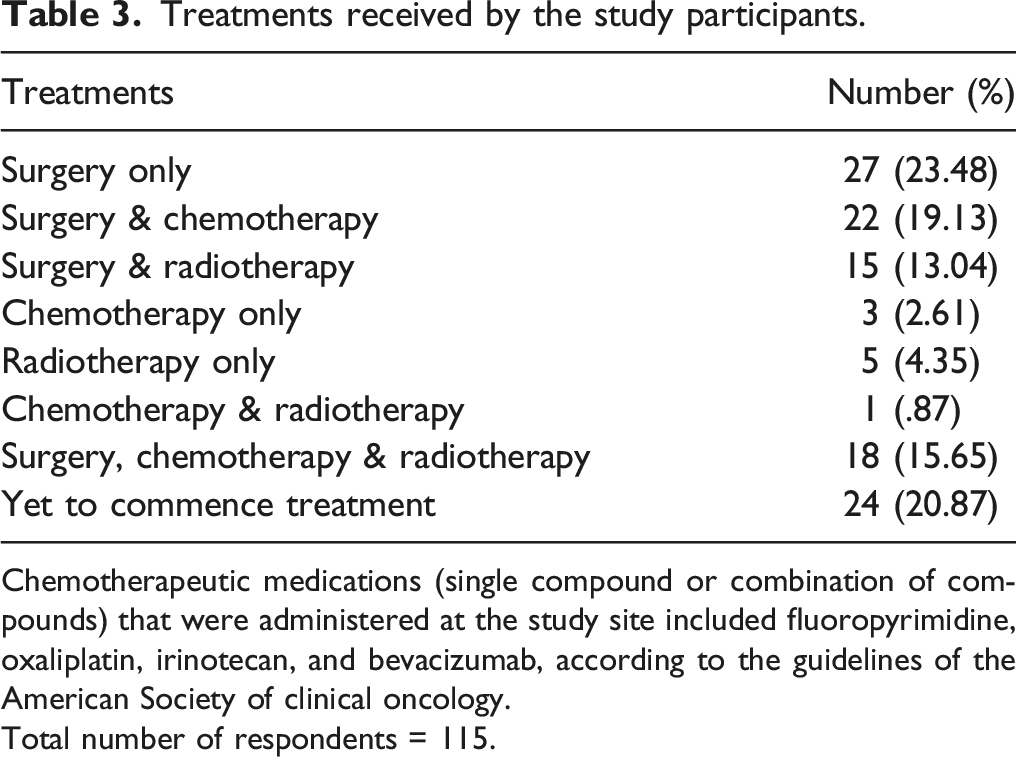
Chemotherapeutic medications (single compound or combination of compounds) that were administered at the study site included fluoropyrimidine, oxaliplatin, irinotecan, and bevacizumab, according to the guidelines of the American Society of clinical oncology.
Total number of respondents = 115.
Alcohol consumption and smoking status of the study participants
Regular alcohol consumption was recorded for 38 (33.0%) participants, and they indicated their preference for beer, wines, spirit or liquor (Figure 2(A)). Seventy-five participants were not consumers of alcoholic beverages and they had no history of alcohol consumption in their lifetime. Ileocaecal cancer was the only gastrointestinal cancer that was not recorded among the 75 participants with no history of alcohol consumption. This study also revealed that 13 out of the 115 (11.3%) participants were ex-smokers and they were diagnosed of either anal, colorectal, gastric or oesophageal cancers (Figure 2(B)). One participant was a current cigarette smoker diagnosed of colorectal cancer. Moreover, 101 (87.8%) participants had never smoked either cigarette or marijuana during their lifetime. There was no association between alcohol consumption and the gastrointestinal cancers of the study participants (Table 4). Also, there was no association between history of smoking and lower gastrointestinal cancers or upper gastrointestinal cancers. Analysis of alcohol consumption and smoking status of the study participants. a. Alcohol consumption by the study participants. b. Smoking status of the study participants. Coloured legends denote the types of gastrointestinal cancers. Total number of participants (n) = 115. Analysis of association between history of smoking or alcohol consumption and gastrointestinal cancers. Lower GI cancers denote anal, colorectal and illeocaecal cancers. Mid GI cancers denote liver, pancreatic and gallbladder cancers. Upper GI cancers denote oesophageal and gastric cancers. Even though P-value<.05, they were not considered as statistically significant associations because OR = 1 was within the 95% CI. aOR could not be determined because the study participants did not include Mid GI cancer patients having a history of smoking.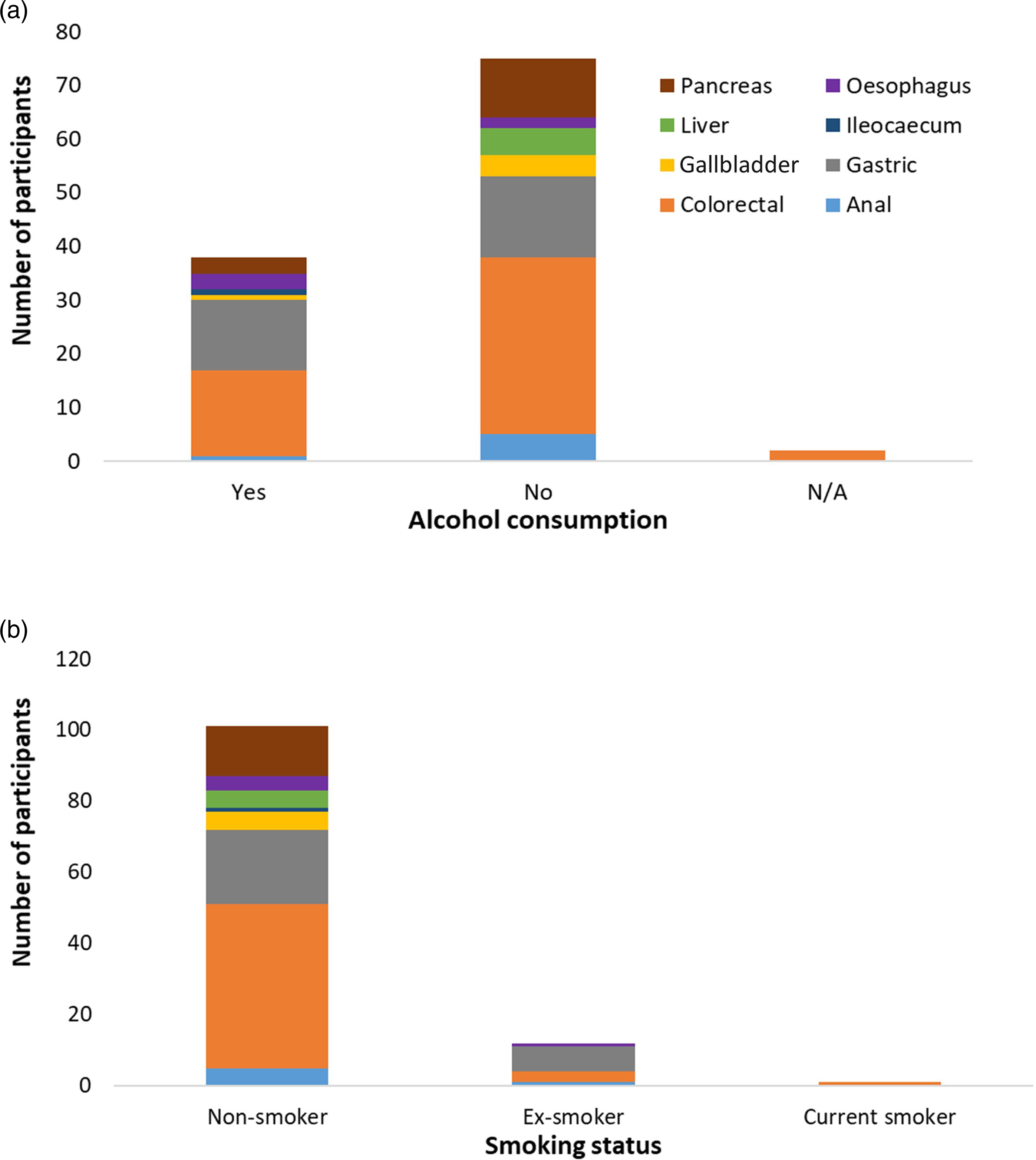

Dietary Protein, Fruits and Water Consumption by the Study Participants
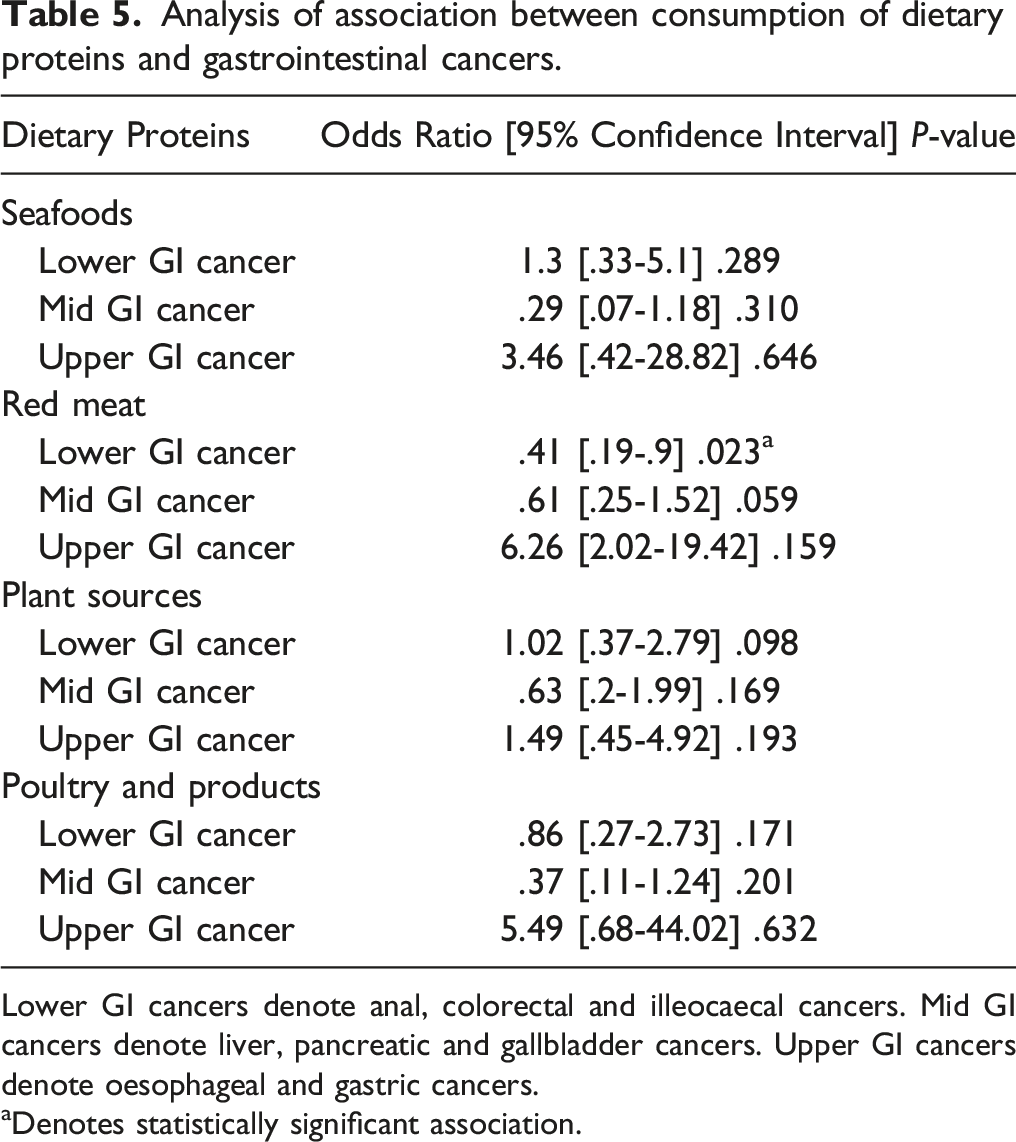
The study revealed that seafoods, poultry and poultry products, plant sources and red meat were the main constituents of proteins in the diets of the study participants (Figure 3(A)). Snails and canned foods were minor sources of proteins in the diet of the study participants. This study showed no association between seafoods consumption, dietary plant protein consumption or poultry consumption and the gastrointestinal cancers of the participants. A statistically significant association but with a weak correlation was shown between red meat consumption and colorectal cancer (Table 5; Table S1). Analysis of protein diet, fruits and water consumption by the study participants. a. Source of dietary proteins of the participants. b. Daily intake of fruits by the study participants. c. Daily intake of water by the study participants. Coloured legends denote the types of gastrointestinal cancers. Number of study participants (n) = 115. Analysis of association between consumption of dietary proteins and gastrointestinal cancers. Lower GI cancers denote anal, colorectal and illeocaecal cancers. Mid GI cancers denote liver, pancreatic and gallbladder cancers. Upper GI cancers denote oesophageal and gastric cancers. aDenotes statistically significant association.
Analysis of association between insufficient intake of water or insufficient intake of fruits and gastrointestinal cancers.

Lower GI cancers denote anal, colorectal and illeocaecal cancers. Mid GI cancers denote liver, pancreatic and gallbladder cancers. Upper GI cancers denote oesophageal and gastric cancers.
Infrequent fruit intake denotes participants that indicated they never consume fruits or participants that did not often consume fruits (Fig. 3(B)).
Even though P-value<.05, they were not considered as statistically significant associations because OR = 1 was within the 95% CI.
Discussion
This study investigated specific lifestyle (modifiable risk factors) that might be associated with gastrointestinal cancers in the context of the Ghanaian population. Colorectal cancers were the most prevalent forms of gastrointestinal cancers identified from the study participants attending the KBTH from March - July 2020. This observation is in accordance with a previous study conducted at the same study site in 2014 using the hospital registry, which also demonstrated that colorectal cancers were the most common gastrointestinal cancers recorded from patients attending the health facility. 19 In contrast, data from the World Health Organization indicated liver cancer was the most prevalent amongst the new cases of gastrointestinal cancers recorded in Ghana in the year 2020. 2 Liver cancer patients were among the less prevalent gastrointestinal cancer cases recorded in this study presumably because liver cancer patients were reluctant or unavailable to participate in this study.
The study also demonstrated that gastrointestinal cancers were prevalent in patients from 50 years to 79 years and least common in patients below 30 years. This data corroborates the recommended practise of screening both males and females between the ages of 50 and 70 years for colorectal cancer.
Two-thirds of the study participants had no history of alcohol consumption while the remaining one-third consumed less than 14 units of alcohol per week, thus, their habit was not classified as heavy drinking of alcohol. This study found that there might be no significant association between the gastrointestinal cancers and alcohol consumption of the participants. This observation is in accordance with a previous study, which reported that alcohol consumption is a risk factor for colorectal cancer in individuals with a habit of consistently high alcohol intake. 10 It is possible that a subset of the study participants consistently consumed high amount of alcohol prior to diagnosis with a gastrointestinal cancer and later adapted to no alcohol intake or reduced alcohol intake in order to minimise the risk of exacerbating the symptoms associated with the disease condition. If this assumption is valid, it highlights a potential limitation of the study design and a plausible explanation for the no significant association between alcohol consumption and the gastrointestinal cancers reported by this study.
Smoking is also a notable risk factor implicated in diverse forms of cancers, beyond cancers affecting the gastrointestinal tract. 20 A previous study specifically reported that smoking increased the risk for pancreatic cancer by a factor of 2-fold. 21 Most of the participants in this study indicated they had no history of smoking either cigarettes or marijuana. Additionally, none of the participants for this study who had a history of smoking was diagnosed of pancreatic cancer. The prevalent gastrointestinal cancers reported by the study participants who had a history of smoking were gastric and colon cancers. Since colon and gastric cancers were also prevalent among the non-smoking participants, these cancers might not be caused by a history of smoking in these participants.
Generally, the dietary foods consumed by most Ghanaians are usually less difficult to accurately recollect because of the relatively constant constituents of their diets. Occasionally, a variety of other diets are also consumed even though they do not constitute their routine nutritional needs. This study relied on the ability of the study participants to recollect the constituents of their nutritional needs, including foods consumed either regularly or infrequently. Dietary proteins such as seafoods, red meat, plant proteins, poultry and eggs are integral staple foods among the Ghanaian population. These protein constituents are usually complemented with carbohydrate rich-diets, originating from plant cereals, plantain, and edible stem and root tubers of plants.
Red meat and high salt consumption have previously been reported as modifiable risk factors for colorectal cancer.22,23 Data from this study provided an indication that consumption of red meat such as beef, lamb, pork, veal, venison, mutton and goat meat might be associated with gastrointestinal cancers. Even though consumption of poultry and eggs was reported by most of the participants, the data suggests that it might not be significantly associated with the gastrointestinal cancers reported in this study. Additionally, the consumption of seafoods such as salted fish, fish, crab, lobster and prawns might also not be significantly associated with gastrointestinal malignancies. A plausible explanation could be these seafoods may not contain the required high salt concentration to be a potential risk factor for gastrointestinal cancers in the Ghanaian population. The study also showed that consumption of dietary proteins from plant sources might not be significantly associated with gastrointestinal cancers most likely because the fibres in these plant foods are immensely beneficial for human health.
The intake of fruits by the study participants was very low and the daily intake of water was also marginally below the recommended quantity in the USA. A previous study has reported that daily consumption of 2.7 L of water was considered adequate for women and 3.7 L of water was recommended for men. 24 Despite this previous report, data from this current study suggests that low intake of water (maximum of 2 L a day for both gender) and fruits may not be significantly associated with the malignancies of the gastrointestinal tracts of the study participants.
The total number of patients that participated in this study was relatively small. Additionally, there was an uneven distribution of the participants across the various gastrointestinal cancer phenotypes. As a result, there were gastrointestinal cancer phenotypes that had insufficient participants for meaningful statistical analysis. In order to circumvent this limitation, the gastrointestinal cancer phenotypes that were recorded by the study were categorized into Lower, Mid and Upper gastrointestinal (GI) cancers. This approach generated relatively sufficient number of participants for each category of GI cancers and facilitated meaningful statistical analysis.
The design of this current study and recruitment of the participants are prone to Incidence-Prevalence bias. For example, gastrointestinal cancer patients that were at the late stage of the disease condition might be unconsciously excluded from the study during data acquisition because of their inability to complete the questionnaire during sample collection. These late-stage gastrointestinal cancer patients may also require extra clinical care, hence they are more likely to be found at intensive care units of the hospital. Consequently, collecting data from out-patient departments will create a bias against the recruitment of these late-stage gastrointestinal cancer patients for the study. Patients at the very early stages of developing gastrointestinal cancers are also unlikely to be recruited in the study because these patients may not yet be experiencing clinical symptoms that might necessitate a visit to the hospital. Moreover, the study was conducted at a tertiary hospital in Ghana, which mainly receives patients that have been referred from other hospitals and clinics. Patients at the very early stages of development of gastrointestinal cancers are more likely to be identified at primary and secondary healthcare facilities, instead of a tertiary hospital. Thus, these patients are less likely to be recruited in the study, thereby leading to a bias in the incidence of the gastrointestinal cancer phenotypes reported by this study. These potential bias in the recruitment of study participants could account for the inconsistencies in the prevalence of the eight gastrointestinal cancer phenotypes recorded in this study, in comparison to the country-specific (Ghana) data from the World Health Organization.
According to the Globocan country-specific data for Ghana, liver and stomach cancers were the most prevalent new gastrointestinal cancer cases recorded in the year 2020. Other forms of gastrointestinal cancers recorded that year were oesophageal, colorectal, pancreatic and anal cancers. The lowest incidence of new cancer cases affecting a component of the gastrointestinal tract were salivary gland cancers and gallbladder cancers, implying these were rare gastrointestinal cancers in Ghana. 2 The current study recorded five participants were diagnosed with a gallbladder cancer but none of the participants recruited for the study was diagnosed with a cancer affecting the salivary gland. The absence of a participant diagnosed with a salivary gland cancer in this study could partly be attributed to the relatively small number of patients recruited for the study and also by the study design. Generally, cross-sectional studies have a very low tendency of detecting rare diseases among the population for downstream analysis of association between risk factors and disease outcome. This limitation of a cross-sectional study, together with its inability to accurately measure disease incidence or prevalence and the associated difficulty in confidently interpreting statistical associations, were major drawbacks of the current study. 25 Nonetheless, this study have identified vital observations that could be investigated in-depth using well-structured longitudinal studies. These observations include: (i) red meat consumption might be associated with gastrointestinal malignancies in the Ghanaian population (ii) the diverse seafoods might not constitute significant risk factors for gastrointestinal malignancies despite their salt content (iii) insufficient daily intake of water (maximum of 2 L) or fruits might not be directly associated with gastrointestinal malignancies even though regular consumption is essential for wellbeing (iv) regular consumption of poultry and eggs might not constitute significant risk factors for gastrointestinal malignancy in the Ghanaian population.
Conclusion
This study shows that red meat consumption is associated with colorectal cancers in Ghana and could be a modifiable risk factor that predisposes Ghanaians to the incidence of the disease. Longitudinal studies using large number of participants is needed for confirming the observations from this study, and would provide a strong basis to advocate for public awareness as a contribution towards controlling the increasing prevalence of gastrointestinal cancers in Ghana.
Supplemental Material
Supplemental Material - Cross-Sectional Study for Investigation of the Association Between Modifiable Risk Factors and Gastrointestinal Cancers at a Tertiary Hospital in Ghana
Supplemental Material for Cross-Sectional Study for Investigation of the Association Between Modifiable Risk Factors and Gastrointestinal Cancers at a Tertiary Hospital in Ghana by Naa Adzoa Adzeley Boi-Dsane, MD, Vincent Amarh, PhD, Sandra Enyonam Tsatsu, MD, Sarah Vuunipuo Bachelle, BSc, Antoinette Afua Asiedua Bediako-Bowan, MD, FWACS, PhD, Nii Koney-kwaku Koney, PhD and Bartholomew Dzudzor, PhD in Cancer Control
Footnotes
Acknowledgments
The authors are extremely grateful to the study participants and the staff of the oncology and surgical clinics of the KBTH.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed that no financial support was obtained for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from the Institutional Review Board of the Korle-Bu Teaching Hospital via the Department of Community Health (UGMS-CHDRC/080/2020). Statement of Human and Animal Rights: All procedures in this study were conducted in accordance with the Institutional Review Board of the Korle-Bu Teaching Hospital (UGMS-CHDRC/080/2020) approved protocols.
Informed Consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.