
Abstract
Background
Prevention strategies for cancer are necessary. Health workers who often serve as role models bear responsibility for prevention counseling and programs. However, whether their habits and behaviors reflect prevention goals are unknown. We describe the prevalence of cancer risk factors and prevention behaviors in health workers of a referral cancer center in Mexico City.
Methods
Cross-sectional study in which workers of the National Cancer Institute were invited to participate in a prevention program, risk factor survey, and nutrition, psychological, and genetic counseling were included. The likelihood of cancer was calculated based on the presence of risk factors. Factors associated with prevention behaviors were identified by logistic regression.
Results
We recruited 301 workers; 77% were women. The median self-reported BMI was 26.4 kg/m2, 9.97% smoked, 78% drank alcohol, and 89% did not get at least 150 min/week of physical activity. In women, age (OR = 1.3 95%CI 1.01-1.06) and physical activity of 150 min/week (OR = 2.52 95% CI 1.28-4.96) were associated with cancer prevention behaviors. No risk factors were associated with healthy behaviors among men.
Conclusion
Health workers may have unhealthy lifestyles and behaviors, is essential to create supportive environments to promote cancer prevention counseling and programs effectively.
Introduction
Cancer is one of the leading causes of morbidity and mortality worldwide, accounting for approximately 10 million deaths in 2020, 1 many of which were caused by potentially modifiable risk factors. Therefore, the relevance of prevention as a means to reduce the global burden of this disease is strongly supported. 2 Furthermore, modifying or avoiding some risk factors such as tobacco use, overweight or obesity, alcohol use, sexually transmitted HPV infection, hepatitis, or other carcinogenic infections can significantly reduce the burden of cancer.2,3
In Mexico, cancer is the third cause of mortality, mainly due to breast, cervical, lung, colon, and prostate cancer.4,5 The burden of these types of preventable cancer is unnecessarily high because of the high prevalence of risk factors for these types of cancer in the Mexican population. 6 Early detection programs for breast and cervical cancer have expanded in Mexico in recent years, but the coverage of these programs in higher-risk populations is still low. 6 This should be strengthened, since it is well known that between 30-50% of cancers can be prevented by avoiding risk factors and implementing existing evidence-based prevention strategies.7,8
Individuals interested in cancer prevention face many challenges and barriers in low-and middle-income countries, 9 resulting in delayed cancer diagnosis and poorer survival. These barriers include low education level, lack of formal employment and social security, low income, and living in rural settings. However, these barriers are not the typical ones faced by health workers. Research among health workers, especially nurses, has reported barriers to health that include poor nutrition, insufficient physical activity, sleep debt, few rest breaks, lack of regular check-ups and tests, tobacco and alcohol use, and drug abuse.10-15 Unfortunately, such modifiable behaviors could compromise cancer prevention efforts even in institutions devoted to cancer care.
A survey about the alignment of personal behaviors among individuals with primary or secondary cancer prevention goals has not been reported among health personnel working in cancer centers. Thus, this paper aims to describe cancer-related risk factors and prevention behaviors according to these factors in health workers of a referral cancer center in Mexico City.
Methodology
Cross-sectional epidemiological study. Data were collected between March and December 2019. We surveyed a sample of the health workers of the National Cancer Institute of Mexico (INCan), the leading oncology reference center in the country. The invitation to participate in the study was made open to all personnel assigned to the institute; we excluded subjects with a previous history of cancer or premalignant lesion. There were no other selection criteria. The sample was 15.7% of formal INCan workers who agreed to participate in a pilot cancer prevention program developed by the recently opened Prevention Research Center and to answer the risk factor questionnaire; the review the medical records of all the participants was approved by the Research Committee and Research Ethics Committee of INCan (2021/014), the data support without identifying the participants, for the replication of the analysis is in the Mendeley repository (DOI: 10.17632/34f2hybrwb.1). The reporting of this study conforms to STROBE guidelines. 16
The prevention program included a risk factor questionnaire that calculated the likelihood of developing specific potentially preventable cancers (cervical, breast, prostate, colon, and lung). Additionally, psychologists, geneticists, nutritionists, and general practitioners trained in cancer prevention provided personalized counseling. Follow-up visits with the psychologist and nutritionist were scheduled at least every month for 6 months. The appointments with the genetic counselor were scheduled depending on the needs of the participants. In the present paper, we only included baseline data collected.
The risk factor questionnaire contained 130 items, created after a systematic review of papers published between 2015 and 2019 about cancer risk factors. We searched MEDLINE via PubMed and Latin American and Caribbean Health Sciences via LILACS. We included papers in English and Spanish, dissertations, reports, and official documents. We used 3 combined queries as follows: (“2015/01/01” [Date–Publication]: “2019/12/31” [Date–Publication]) AND ((cancer of prostate, breast, cervix, lung, colon [MeSH Terms]) OR (cancer of prostate, breast, cervix, lung, colon [MeSH Terms])) OR (cancer of prostate, breast, cervix, lung, colon [text word]) AND ((risk factors [text word]) OR (risk factors [text word])) OR (risk factors [text word]). We extracted the resulting titles and abstracts into a spreadsheet. Papers showing measures of association were assigned a higher priority, and the questions were drafted considering this review. The questionnaire was revised by a panel of expert oncologists in charge of the prevention programs at INCan, and nutritionists who considered the international recommendations for diet and exercise. 17 The questionnaire also included early detection behaviors for each type of cancer, information that was corroborated in the medical records of each participant. This panel of experts was in charge of validating the questionnaire´s content by discussion and consensus.
All the participants received recommendations based on national Clinical Practice Guidelines depending on their likelihood of developing any of the main types of cancer; this included primary and secondary prevention strategies, such as maintaining of healthy lifestyles, and identification of risk groups for hereditary cancer, among other.18-22 These likelihoods were calculated using their risk factors, computed through simulation of the probability distribution for each variable based on statistical parameters; we simulated the binary response (0: not cancer 1: cancer) in a hypothetical Mexican cohort, in which a predictive logistic regression model (logit) was adjusted for each type of cancer. 23 The magnitude of the association for each factor was estimated based on the literature review, only evidence-based factors were included getting the following goodness of fit results: breast (specificity .630, sensitivity .861, Area Under the Curve AUC .83); cervical (specificity .816, sensitivity .668, AUC .82); prostate (specificity .763, sensitivity .521, AUC .70); colon (specificity .995, sensitivity .30, AUC .67) and lung (specificity .912, sensitivity .435, AUC .78). The likelihood was categorized into tertiles to individualize the recommendations for timely detection that were given during follow-up.
Statistical Analysis
The total working population of INCan at that time was 1900 employees, considering a maximum expected frequency of 50% in any of the risk factors, an acceptable, marginal error of 5% with a confidence level of 90%, a sample size of 237 participants. We achieved the participation of 301 workers,
We used descriptive statistics for each risk factor and prevention behavior. The statistical differences between sex and likelihood groups were computed using the chi-square test and Student’s t-test or Mann–Whitney U test according to the variable distribution. Using a logistic regression model, we identified the variables associated with secondary prevention behaviors adjusted for the likelihood of developing cancer-based on known risk factors. We calculated the goodness of fit by the Hosmer-Lemeshow test and the classification ability by the receiver operating characteristic (ROC) curve. A P-value < .05 was considered statistically significant. All analyses were performed with Stata v.14.
Results
Health Status of the Working Population.

aP50 (P25-P75).
bNurses, nutritionists, other type of technicians.
cServings per day.
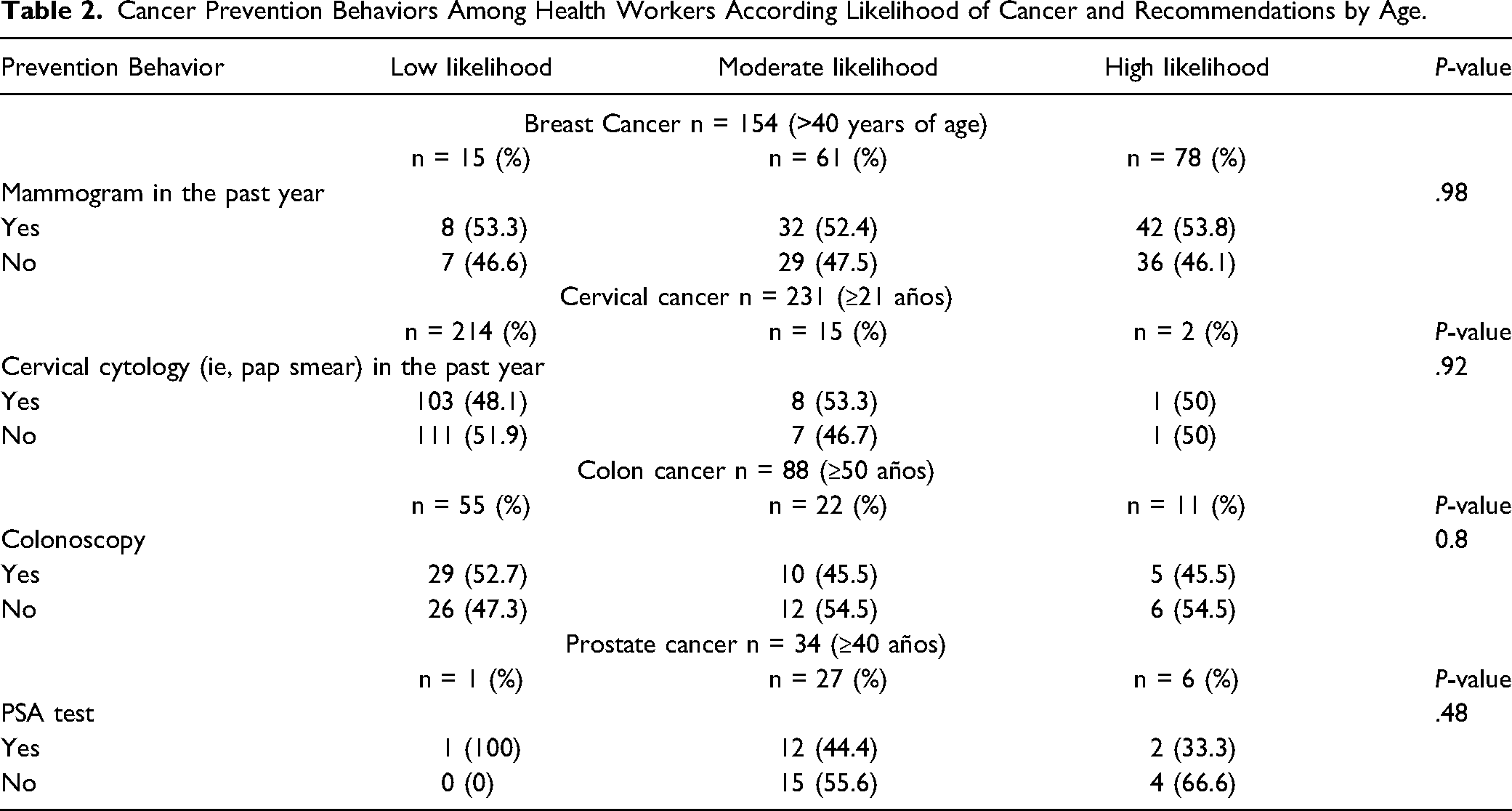
Cancer Prevention Behaviors Among Health Workers According Likelihood of Cancer and Recommendations by Age.
Multivariate Logistic Regression of Participation in Early Detection Screening of Cancer Among Female Health Workers.
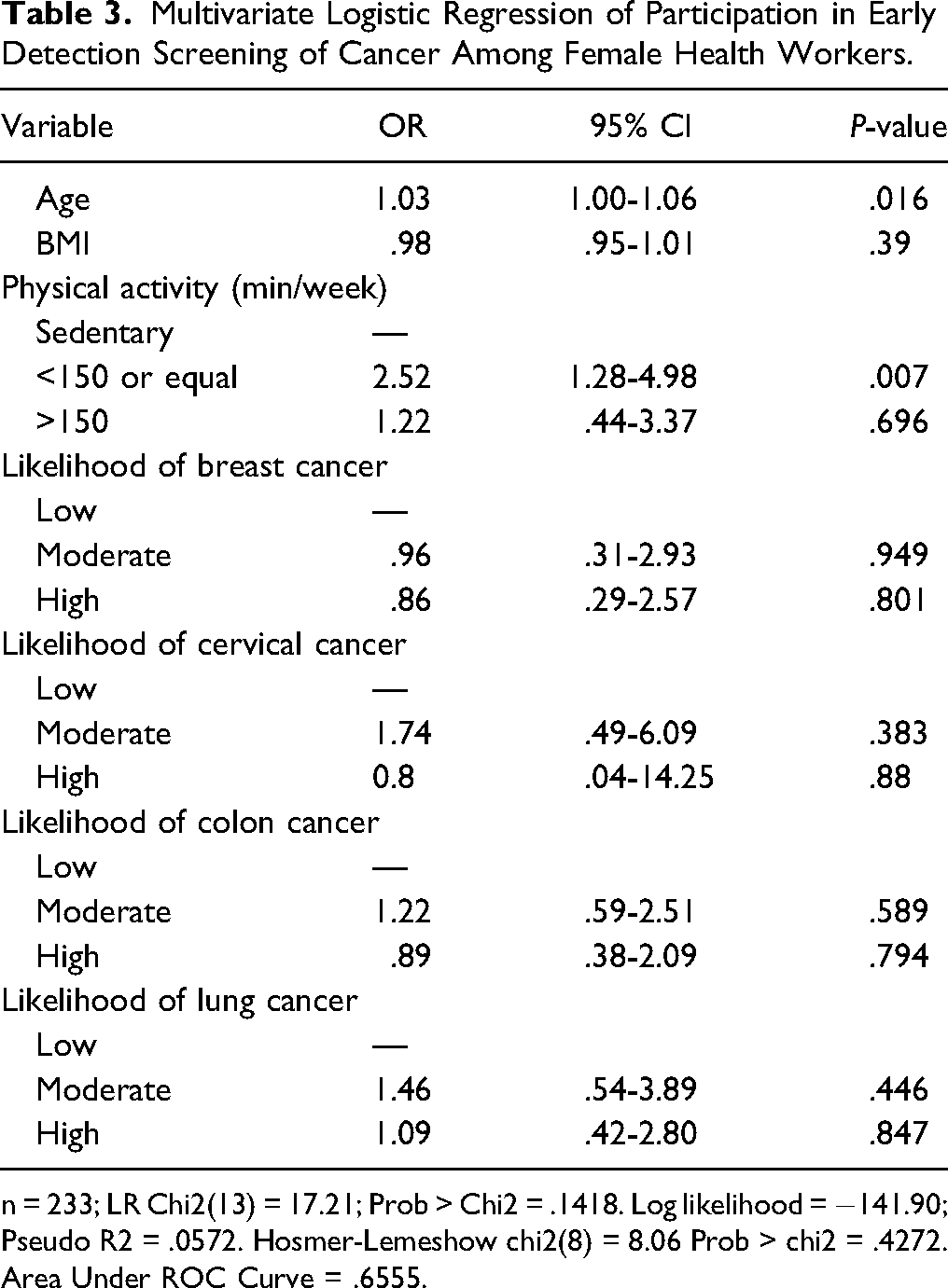
n = 233; LR Chi2(13) = 17.21; Prob > Chi2 = .1418. Log likelihood = −141.90; Pseudo R2 = .0572. Hosmer-Lemeshow chi2(8) = 8.06 Prob > chi2 = .4272. Area Under ROC Curve = .6555.
Discussion
This analysis of health workers from a cancer reference center in Mexico City showed the high prevalence of risk factors for cancer despite being aware of the issue. The health workers were mainly young adults (≈44 years); more than half were overweight and reported using tobacco and alcohol often and in high quantities, especially men. Both genders exhibited high levels of inactivity and consumption of high-calorie foods. We did not observe a significant relationship between the presence of such cancer-related risk factors and adherence to secondary prevention adjusted per age. We only identified that older participants and those who got 150 minutes of physical activity per week were more likely to comply with recommendations for screening tests for early cancer detection.
In 2018, 11.4% of Mexican people over 20 years smoked daily. We observed a lower prevalence among health workers at INCan (9.97%); however, the prevalence for workers men (12.5%) was higher than reported in the general population. Alcohol use followed a similar pattern. Regarding BMI, more than 50% of INCan participants self-reported as overweight or obese, which is consistent with national prevalence (39.1% and 36.1%, respectively); however, it was not associated with healthy behaviors. Regarding physical activity, health workers were more inactive (54.8%) than the general population (17.3%). 6 Health workers reported eating more fruits and vegetables and processed and high-calorie foods than the general population. Wood smoke exposure was lower in health workers than in the general population (12.9% and 14%, respectively).6,24
The health workers included in this analysis appear to exhibit health behaviors similar or worse (physical activity and consumption of processed and high-calorie foods) to those of the general population, even when they are aware of the consequences. Some studies have reported that nurses seem to have a high prevalence of obesity, probably due to unhealthy diet, physical inactivity, lack of sleep, and high-stress levels. This situation is frequent in developing and developed countries.25-27 Additionally, research suggests that the ability to deliver credible messages, recommendations, and advice to the general population is diminished when health workers do not adhere to prevention and health promotion guidelines themselves.28-30
Currently, there is little literature on healthy lifestyles and behaviors among health workers in Latin America, particularly about cancer prevention. Given the magnitude of cancer in Mexico and the population surveyed working at the country´s largest referral cancer center, we expected workers to engage in healthy habits and avoid cancer risk factors. However, our findings did not fully support our assumption.
Respect tests for early cancer detection, we found that female workers at INCan underwent screening tests more often than the general population. Among female health worker participants, 40.77% on average had a mammogram in the past year, compared with the general population (20-27.5% among women aged 40-69); 48.07% had cervical cytology tests, as opposed to the general population (28.9% of women over 20). 8 One explanation for this disparity, even though national prevention programs have been implemented in Mexico for more than two decades, is the lower accessibility to this type of service and the lack of follow-up and continuity of existing programs, among others. 31 Additionally, INCan has established programs that facilitate access to screening for its workers. On the other hand, women tend to seek medical attention more often. 32 Disappointingly, male workers reported a higher prevalence of many risk factors and unhealthy behaviors than women, but they did not engage in prevention behaviors. Not long ago, INCan and the National Health System reinforced prevention programs aimed at men through greater dissemination and access to them.
Improving the work and social environment of the Mexican population and promoting changes in health workers’ habits through preventive education is essential. Obesity,33,34 metabolic syndrome,35,36 cardiovascular diseases, 37 sleep disorders, 38 and depression 39 have been described as work-related health problems. Therefore, health workers must assist with prevention measures and disease control. In addition, some studies have demonstrated the direct relationship between one’s health habits and the ability to implement strategies targeted at the population.40-42 Therefore, health workers must maintain and promote healthy environments to disseminate preventive actions effectively.
This manuscript aimed to explore the prevalence of risk factors in a sample of the working population at INCan. An open invitation was issued to receive prevention assistance. It is possible that those who agreed to participate belonged to a specific group with a history of cancer that motivated them to seek attention. The self-reported body mass index presented here does not reflects the actual BMI, similarly, the measurement of many other variables can be limited by the use of a questionnaire. However, the high prevalence of some risk factors and the similarity of such report among the participants with that observed for the general population, through the National Health Surveys 6 that also use questionnaires, make us believe that the sample was not biased and it was representative of the working population at INCan. The methodology used to calculate the probabilities of developing any of the main types of cancer facilitated the identification of risk groups. To validate this model, it should be applied over time to this population. Despite the limitations of a cross-sectional study, this pilot study allowed us to identify specific modifiable cancer risk factors and behaviors by gender that must be examined more accurately in future studies to associate them with the presence of cancer and for the development or evaluation of prevention programs. Being a cross-sectional study, it is not possible to determine the causality of the associations. Also, the results may be affected by the nature of the pilot study since the sample included participants by convenience (participants themselves sought the care that the program offered). Types of bias and limitations involved are related to memory and conscious psychological reactions due to the sensitivity of some questions and the expectation of being health workers. Although the questionnaire only was validated in its content by a group of experts, with this first study, we hope to create a cohort of INCan workers that would allow validation, at least in this population, of a cancer risk calculator, which does not exist in Mexico. Likewise, other studies could be carried out that allow us to identify other social, economic, demographic, and cultural factors related to healthy behaviors in health personnel, already described in some other populations.43,44
While cancer prevention has become a significant concern in Mexico, implementing a national cancer control program has challenges. 45 Similarities of the workforce at INCan with the lifestyle and behaviors of the general Mexican population are an opportunity to make our institute an optimal setting to deliver cancer prevention education; this experience could be asses, adapted, and reproduced to reduce the impact of cancer in the country. In Mexico, as far as we know, there are no counseling programs for cancer prevention. Recently, doctors specializing in prevention have begun to be trained on who could be in charge of this, starting perhaps with the health personnel in charge of the health care of this group of patients. On the other hand, the National Cancer Institute has begun to create prevention care models in different regions of the country, which could give us information on the most effective strategies.
Conclusion
The health workers surveyed may have some unhealthy lifestyles and behaviors. Therefore, it is essential to create supportive environments to promote cancer prevention programs and counsel effectively. The similarities of the INCan workforce with important lifestyles and behaviors of the Mexican population, in general, are an opportunity to make our institute an optimal environment to provide cancer prevention education and evaluate the effects of cancer prevention programs. This could be adapted and replicated in others and for other populations to reduce the impact of cancer in the country.
Supplemental Material
Supplemental Material - Cancer Prevention Behaviors in Workers of a Referral Cancer Center in Mexico City: A Pilot Study on Early Detection Awareness for Cancer
Supplemental Material for Cancer Prevention Behaviors in Workers of a Referral Cancer Center in Mexico City: A Pilot Study on Early Detection Awareness for Cancer by Nancy Reynoso-Noverón, Chang Shine, LA Herrera-Montalvo, and Abelardo Meneses-García in Cancer Control.
Footnotes
Acknowledgements
The authors thank the medical specialists of the National Cancer Institute (INCan) for their technical assistance and administrative support, and are indebted to all the workers who agreed to participate in the study. Special thanks to the Board of Trustees of the National Cancer Institute for their support in carrying out cancer prevention initiatives.
Author contribution
NRN, LAHM, MGA composed the manuscript concept. NRN conducted the data collection. NRN, LAHM, MGA, SC performed the data analysis and interpretation. NRN and SC, drafted the manuscript; LAHM, MGA and SC critically revised it. All authors read and approved the final version for publication and guarantee all contents of the manuscript have been reviewed and commented upon by NRN, SC, LAHM, MGA in order to present them with the utmost accuracy and integrity.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s Note
The project was carried out thanks to the support of the Patronato INCan, and the efforts of the General Directorate, Research Directorate and specialists of the Institute. Health and IT personnel were hired exclusively for the development of the program.
Ethical approval
The project was approved by the Research Committee and Research Ethics Committee of INCan (2021/014), the data support is in Mendeley repository (doi: 10.17632/34f2hybrwb.1).
Transparency statement
As the corresponding author of this paper, I, Nancy Reynoso Noverón, ensure on behalf of myself and all authors the data accuracy, integrity, and transparency; no relevant data have been omitted; any disagreement between authors was resolved and described.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.