
Abstract
Purpose
To evaluate the role of sentinel lymph node (SLN) biopsy in patients with conjuctival melanoma (CjM).
Study design
Retrospective observational cohort study and literature review.
Subjects
Slovenian patients with CjM are included in the study.
Methods
Prospectively collected data of CjM patients treated from June 2005 to December 2016 were retrospectively analyzed.
Main outcome measures
The numbers of SLN biopsy procedures, positive and false positive SLN, and local and regional relapses have been described together with overall survival.
Results
From June 2005 until December 2016, 24 patients with CjM were treated. The median follow-up time was 65.3 months. The mean Breslow thickness was 1.5 mm (sd = 1.8 mm), and ulceration was present in 29% of cases. Altogether, 14/24 (58%) SLN biopsy procedures were performed. SLN was positive in 2/14 (14%) cases. The estimated 5-year overall survival (OS) of the group was 72.5%, with a median survival of 151 months (95% CI 77–224). From January 2013 to January 2020, five (5/140, 3%) authors reported results comparable to our study.
Conclusion
Our results confirm that CjM is a rare disease with approximately 14% of positive SLN. At the moment, there are no firm conclusions regarding who would benefit most from SLN biopsy or whether or not CLND should be offered. Data from literature emphasize the need for consistent and uniform staging and future multicentric studies.
Introduction
Conjuctival melanoma (CjM) is the second most common primary malignancy of the ocular surface and constitutes 5% of all the melanomas of the eye. It occurs with an annual incidence of 0.2–0.7/1.000.000.1,2 Tumors are common among the Caucasian population and the elderly. 3
This rare tumor emerges from atypical melanocytes in the basal layer of the epithelium. 4 The most important risk factors are conjunctival melanocytic intraepithelial neoplasia or primary acquired melanosis (PAM), previous nevi, and UV exposure. 5
Although there are similarities between clinical appearance and association with UV exposure, CjM presents itself differently in biological behavior in comparison to cutaneous melanoma; for example, it is associated with higher recurrence rates after primary therapy. 6 The overall frequency of a local recurrence is estimated to be approximately 40%. 4
Analogous to cutaneous melanoma, CjM is believed to have spread to regional lymph nodes in 19% of cases at the time of discovery. The first regional lymph nodes affected by nodal spread are usually pre-auricular, and rarely submandibular or deep cervical. 3 Tumor thicknesses of >2 mm and large basal diameter but also non-epibulbar location, positive resection margins, orbital extension, nodular tumours, “de novo” emergence, and ulceration are associated with a higher risk of nodal metastases.1,7-9
Since sentinel lymph node (SLN) biopsy gives important prognostic information in the case of cutaneous melanoma, the same procedure was proposed for CjM patients. Indeed, it has been shown that positive SLN correlates significantly with death from CjM. 1 Detection of subclinical micrometastases in regional lymph nodes followed by completion lymph node dissection (CLND) of the neck was thought to offer CjM patients a survival advantage. 8 Although the procedure has been widely used, the efficacy of this approach in CjM is not completely clear due to the low incidence of the disease and frequency of SLN positive cases.2,4,11
Interestingly, in recent years, our understanding of the importance of CLND after positive SLN biopsy has been comprehensively altered based on the results of two prospective randomized trials which showed that CLND offers no survival benefits when compared to follow-up US scans for patients with cutaneous melanoma.12,13
Evidence of cutaneous melanoma raises the question of whether CLND should be offered to patients with CjM in order to improve regional control and perhaps even survival. Due to a lack of randomized prospective studies, the only available data addressing the topic of SLN biopsy in CjM comes from clinical registries and researchers’ reports.
The aim of our study was to evaluate the frequency of regional lymph node metastases of CjM patients in Slovenia and to compare our results with available literature data.
Methods
For this retrospective observational cohort study with a systematic review of the available literature, data of Slovenian CjM patients were analyzed. Analysis of prospectively collected data from the Institute of Oncology Ljubljana clinical registry and the national Cancer Registry was performed. Patients with CjM treated from June 2005 to December 2016 were included.
All patients were initially diagnosed and treated at the Eye Hospital of the University Medical Centre of Ljubljana, where primary tumors were excised. All CjM specimens were examined by two experienced pathologists specialized in melanocytic lesions. After tumor removal and confirmation of CjM, if indicated, SLN biopsy was performed at the Institute of Oncology Ljubljana within 6 weeks following tumor resection. The indications were as follows: tumour thickness > 1 mm in 5 patients, non-limbal location in 4 patients, > 1 mitosis/mm2 in 3 patients, and in two cases it was performed after local recurrence. The procedure was performed according to standard recommendations including subconjunctival injection of 0.2 mL of Tehnecium-99m (Tc-99m) and dynamic and static imaging with a gamma camera (lymphoscintigraphy). After lymphoscintigraphy, the SLN was surgically excised with the assistance of a sterile, handheld gamma probe through a 3 cm incision placed over the area of high radioactivity. No touch technique was used with regard to the node. Blue dye subconjunctival injections were used in earlier cases and later omitted due to the danger of residual blue staining. The excised SLNs were histologically evaluated using a “bread loaf” approach. In case adjuvant treatment of the primary tumor was required (wider local excision or strontium-90 (Sr90) beta radiotherapy of the tumour bed), it was performed at the time of the SLN biopsy.
In case of positive SLN, CLND was performed which included superficial parotidectomy and lymph nodes levels I to V according to the American Head and Neck Society classification. 17 The procedure was also performed in cases of clinically detected metastatic lymph nodes.
After the SLN biopsy, patient progress was followed according to a schedule: a clinical exam every 3 months for the first 2 years, then every 6 months until the fifth year, and thereafter by an ophthalmologist every 6 months. Local recurrence was defined as the recurrence of histologically proven invasive CjM. Regional and distant metastases were identified clinically and/or via US, MRI, PET-CT, or CT, and confirmed with fine needle aspiration biopsy (FNAB) followed by histological examination of the removed lymph nodes. Follow-up was closed on March 14, 2020. The clinical records of all consecutive patients were reviewed with regard to age, sex, time of diagnosis, tumor location at presentation, regional and distant metastases at presentation, time of SLN biopsy, and outcome of interest (local recurrence, regional metastases, distant metastases, death from CjM, and death from any other cause). Histopathological records for each patient were reviewed for tumor thickness, presence of ulceration, and mitotic rate. Patients were staged according to the American Joint Committee on Cancer (AJCC) Cancer Staging Manual (8th edition), and pathological criteria were used for primary tumor definition.
Clinicopathological characteristics were summarized as frequencies and percentages for categorical and means for continuous variables. Overall survival (OS) was defined as the interval from the date of diagnosis to the date of death, and was censored for the last follow-up date. The survival curve was plotted using the Kaplan–Meier method. The analysis was conducted using IBM SPSS software version 26, and P-value < .05 was considered statistically significant.
The literature review was conducted using advanced searches of the PubMed biomedical literature database with the following indicators; (conjunctiva AND melanoma) OR conjunctival melanoma AND (sentinel node biopsy OR epidemiology OR incidence OR genetic). A manual search was also performed for articles referenced in bibliographies that were not initially retrieved by the search, as well as in specific areas in which information was lacking. All articles published in English between January 2013 and January 2020 were reviewed and the most suitable were included in the study comparison.
Results
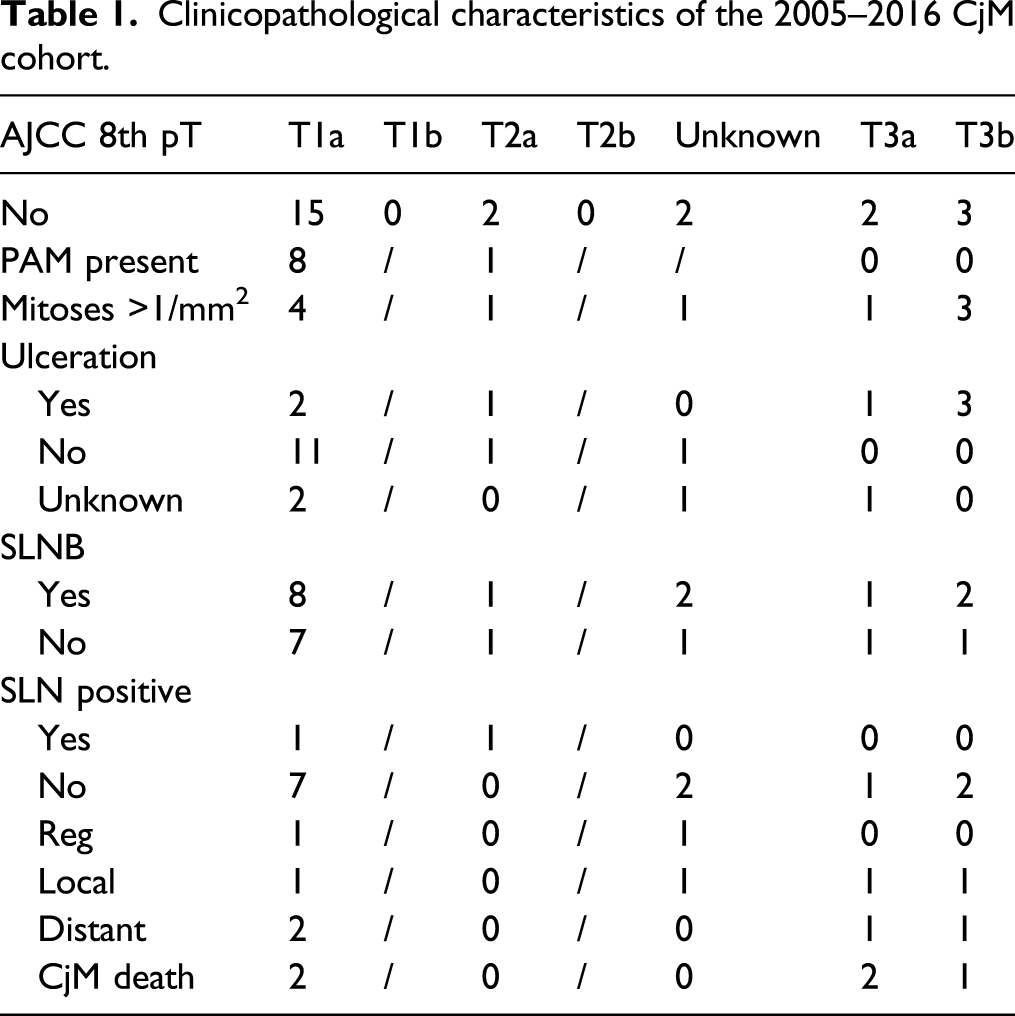
From June 2005 until December 2016, 24 patients with CjM were treated at the Institute of Oncology Ljubljana. The mean age at the time of CjM diagnosis was 60.8 years. There were 17 (71%) female and 7 (29%) male patients. All primary tumors were treated with wide local excisions by the ophthalmologist. In 15/24 (62.5%) patients, the disease affected the left eye, while 9/24 (37.5%) patients had right eye CjM. The locations of the tumor were as follows: limbus in 7/24 (29%) cases, bulbar in 13/24 (54%) cases, tarsal in 3/24 (12%) cases, and unknown in 1/24 (4%) case.
Mean tumor thickness was 1.5 mm (sd = 1.8 mm) and ulceration was present in 7/24 (29%) cases. In 4/24 (17%) the information was unavailable. PAM was noticed in 9/24 (37%) cases.
In total, 14/24 (58%) SLN biopsy procedures were performed, while eleven patients did not undergo the SLN biopsy and in one case the procedure was repeated due to a new primary tumor.
Residual blue staining of conjunctiva was noticed for a few days in all the patients with whom blue dye was used (8/14). In one case transient paresis of the marginal mandibular nerve was reported (1/14, 7%).
The removed SLN was positive in 2/14 (14%) cases. Metastases measured 0.3 mm and 0.6 mm. After completion of lymph node dissection, no other metastases were discovered (60 and 35 lymph nodes were removed).
Regional lymph nodes were clinically detected and removed during follow-ups for two patients with no previous SLN biopsy (2/24, 8%). Altogether, lymph node metastases were discovered in 4 patients (4/24, 17%).
The median follow-up time was 65.3 months. During that time, four patients (4/24, 17%) developed distant metastases. Four patients (4/24, 17%) had local recurrence on conjunctiva that required reoperation and/or radiotherapy.
Clinicopathological characteristics of the 2005–2016 CjM cohort.
The estimated 5-year overall survival (OS) of the group was 72.5%, with a median survival of 151 months (95% CI 77–224). There was no survival difference between female and male patients (P = .321). The Kaplan–Meier survival curve of patients is shown in Figure 1. Survival of Slovenian CjM patients.
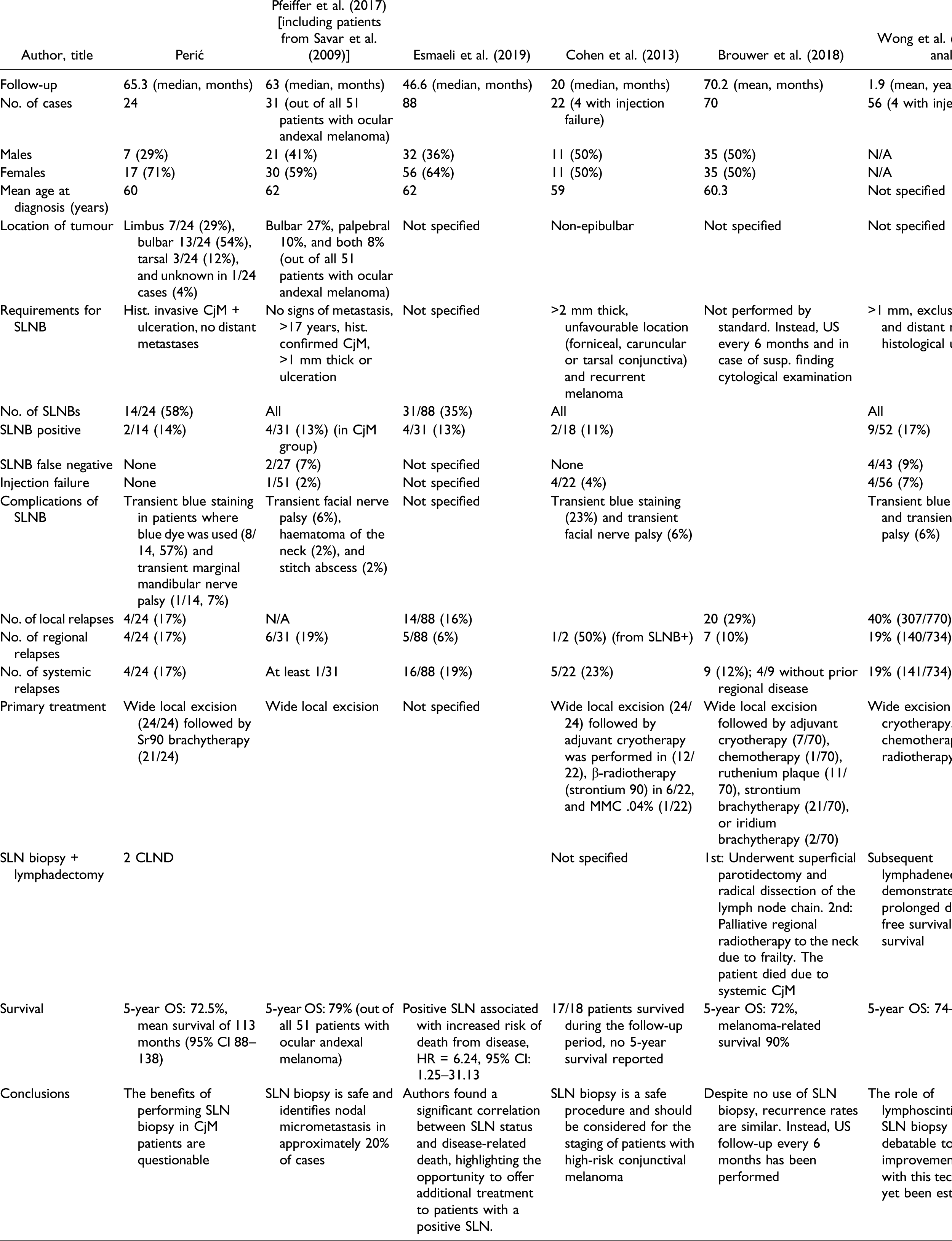
SLN procedure for CjM; summary of the results.
Discussion
With this retrospective observational study, we have added another 24 CjM cases to existing reports of this rare melanocyte tumor. The number of cases diagnosed in Slovenia from 2005 to 2016 is no surprise since the rarity of the disease has previously been noted by other authors.4,7,8,14 Since an incidence of 0.15-0.78/100.000 has been reported recently, the number of diagnosed patients in this study is slightly higher than expected. 2 The fact that 42% of the patients were diagnosed in the last 3 years could indicate that the incidence of the disease is rising in Slovenia.
Fourteen patients (58%) had SLN biopsies performed during that period. The number of procedures is relatively low considering other reports; Pfeiffer and Esmaeli reported 31 cases, Cohen 22 SLN biopsy procedures, and Wong’s meta-analysis included data from 52 patients.1,4,8,14 Only the results reported by Cohen featured prospectively collected data; all the other researchers relied on retrospective results.1,8,14
When attempting to compare the results of previous reports to our findings, various obstacles are encountered. Though the age and distribution of patients are quite similar, the median follow-up times range from 20 to 65 months in different studies. However, the main obstacle is unclear or missing staging (TNM according to the AJCC Cancer Staging Manual) and various indications for SLN biopsy procedure. While some advocate SLN biopsy in the case of histological confirmation of CjM with no signs of distant metastases, and tumor thickness of at least 1 mm or presence of ulceration, others recommend it for tumor thickness of >2 mm, non-limbal location, and recurrence after previous PAM removal.5,8,14
In our group of patients undergoing SLN biopsy, only half of them reached tumor thickness of >1 mm, and biopsy was proposed to others due to high mitosis count, unfavorable tumor location, or invasive CjM discovered after previous PAM removal. Despite such factors, which have been associated with higher risk of metastases in the past, the number of positive SLN was low, only 2/14 (14%). The percentage of positive SLN is still quite similar to other reports, where it varies from 11 to 17%.4,8,14 Both SLN-positive patients had tumor thickness of >1.5 mm and >10 mitosis/mm2, which indicates that the risk of disease progression to regional lymph nodes increases with tumor thickness and mitoses, similar to cutaneous melanoma. These results concur with the proposal that SLN biopsy should be offered based on the presence of at least two of the high-risk features: non-limbal location, >2 mm thickness, ulceration, and >1 mitotic figure per mm2. 4 Tumor thickness of >2 mm, presence of ulceration, positive SLN, and mitotic rate were all recently associated with lower disease-specific survival or increased risk of death from disease. 1
The triple technique of SLN detection employed correctly identifies the SLN in 99% of cases. 15 Failure of the method is associated with false negative (FN) rate. One of the important risk factors of the failure to retrieve the correct node in cases of cutaneous melanoma is due to tumors located in the head and neck region. 16 Although FN rate is not always reported, Pfeiffer and Wong described the FN rate of 7–9% of CjM cases.4,8 We managed to detect the SLN in all our patients in the preauricular or submandibular regions with no FN results.
The specific node location can lead to injection failure and certain postoperative complications. 4 In our cohort, palsy of the mandibular branch of the facial nerve was present in one case, which accounts for 7% of nerve damage. We did not experience injection failure. The complication rate was similar to other reports where transient nerve damage was described in 6% of cases and injection failure in 7% of cases.4,8,14
FN lymph nodes are discovered due to regional relapses during follow-up or due to CLND. Though data of regional relapses are usually presented by authors and vary from 6 to 19%, data about CLND are scarce. 14 We performed CLND in both patients with positive SLN and in both cases histology revealed no additional metastatic lymph nodes.
The issue of CLND in CjM patients is controversial, as the results of two prospective studies in cases of cutaneous melanoma have shown that there was no survival difference between the group of patients with cutaneous melanoma who had CLND due to positive SLN, and those who had the procedure after regional relapse.12,13
Positive SLN was associated with an increased risk of death from disease (HR = 6.24, 95% CI 1.25–31.13). 1 However, by treating cutaneous melanoma patients, we have learned that the size of metastatic deposits in SLN also correlates with prognosis. It has been well established that micrometastatic disease (<0.1 mm) is associated with similar survival rates as negative SLN in case of cutaneous melanoma. Even tumor deposits of sizes <1 mm have a good prognosis with 85% 5-year survival. 17 In our cohort, both patients with positive SLN had CLND due to metastases of <1 mm, and in both cases, histology revealed no additional metastatic lymph nodes. Even though SLN metastases indicate an increased risk of death, it is difficult to conclude whether and which patients should proceed with CLND. Another possibility for patients with positive SLN could be US follow-up. 15
In our study, 17% of patients had a regional spread of the disease and the same number of patients had distant metastases. Results are similar to other reports (regional disease 10–19% and systemic 19–23%).4,8,11,14 A slightly lower percentage of regional disease (6%) was reported by Esmaeli. 10 One interesting observation to note is that out of 5 patients who died due to CjM, only two had had previously clinically or pathologically detected regional lymph node metastases.
The estimated 5-year OS of our group of patients was 72.5%, with no differences between male or female patients. The estimate is in concordance with a composition of five large studies, which revealed 5-year survival rates between 74% and 86%, with one study reporting a 5-year estimate of CjM-related deaths of 7%.4,8,11,14
Information about SLN is one of the most important prognostic factors in cutaneous melanoma that enables clinicians to decide which patients need adjuvant targeted therapy or immunotherapy.15,16 Recently, successful use of programed cell death 1 (PD-1) inhibitors has been reported in metastatic CjM. 10 Based on this, it has been proposed that CjM patients with positive SLN, and thus increased risk of death, could also be candidates for adjuvant systemic treatment. 1
We are aware of the limitations of our study as a retrospective analysis of a small population of CjM patients. However, we present national data and not only a single-center experience. Adding a pathological T category according to the AJCC 8th edition enabled us to focus only on invasive melanoma and to exclude the possible bias of in situ lesions. Tumor staging and reporting of ulceration in our group of patients could prove invaluable for future meta-analysis of SLN biopsy in CjM.
Conclusion
In conclusion, our results confirm that CjM is a rare disease with approximately 14% of positive SLN. Currently, there are no firm conclusions regarding who could benefit most from SLN biopsy and whether or not CLND should be offered. Data from literature emphasize the need for consistent and uniform staging and future multicentric studies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The study was conducted in accordance with recommendations of Ethical Committee at The Institute of Oncology Ljubljana (NAV–613–8010–Ver 10 / February 20, 2020) and the ethical standards laid down in an appropriate version of the 1964 Declaration of Helsinki.
Informed consent
All patients provided written informed consent including study participation prior to treatment.