
Abstract
Introduction:
Cryotherapy is a cold-based ablative therapy used primarily as second line therapy in patients with Barrett’s esophagus (BE) who have persistent dysplasia after undergoing endoscopic treatment with radiofrequency ablation (RFA). Few studies have described the use of cryotherapy as a primary treatment modality for dysplastic or neoplastic BE.
Aim:
To evaluate the efficacy of cryotherapy as primary treatment of dysplastic and/or neoplastic BE by conducting a systemic review and meta-analysis.
Methods:
A systematic search of Medline, Embase, and Web of Science was performed from January 2000 through March 2020. Articles included were observational studies and clinical trials which included patients who had biopsy confirmed dysplastic or neoplastic BE (i.e., high grade dysplasia (HGD), low grade dysplasia (LGD) or intramucosal adenocarcinoma (ImCA)), underwent ≥1 session of cryotherapy, and had a follow-up endoscopy. Primary outcomes were pooled proportions of patients achieving complete eradication of dysplasia (CE-D) and/or intestinal metaplasia (CE-IM) by using a random effects model.
Results:
Fourteen studies making up 405 patients with follow-up ranging from 3-54 months were included. In 13 studies, a total of 321/405 patients achieved CE-D with a pooled proportion of 84.8% (95% confidence interval [CI] 72.2-94.4), with substantial heterogeneity (I2 = 88.3%). In 13 studies, a total of 321/405 patients achieved CE-D with a pooled proportion of 84.8% (95% confidence interval [CI] 72.2-94.4), with substantial heterogeneity (I2 = 88.3%). Subgroup analysis of only high-quality studies revealed a pooled proportion of CE-D 91.3% (95% CI, 83.0-97.4, I2 = 69.5%) and pooled proportion of CE-IM of 71.6% (95% CI, 59.0-82.9, I2 = 80.9%). Adverse events were reported in 12.2% patients.
Conclusion:
Cryotherapy is a safe and effective primary therapy for dysplastic/early neoplastic BE. CE-D and CE-IM rates are comparable to those for other ablation modalities, including RFA. Cryotherapy should be considered for primary therapy of dysplastic BE and early esophageal neoplasia.
Introduction
Barrett’s esophagus (BE) is a histologic diagnosis referring to metaplastic columnar epithelium which replaces the stratified squamous mucosa that normally lines the distal esophagus. 1,2 Proposed pathophysiology is chronic esophageal injury, mediated at least in part by gastric contents in gastroesophageal reflux disease (GERD), causing the damaged squamous cells to be replaced by mucus-secreting columnar cells, with contribution from genetic and other risk factors. 2 BE is the strongest known risk factor for development of esophageal adenocarcinoma (EAC). 3 Studies have proposed a multistep pathway, the metaplasia-dysplasia-adenocarcinoma sequence, for the development of esophageal cancer. 4
The increasing incidence of EAC over the last few decades is worrisome. This rise, particularly among the Caucasian population in the US, has been estimated to have increased at least 6 folds over the last 3-4 decades. 5 These numbers have also been paralleled by an increase in disease related mortality. 5 EAC generally has a poor prognosis given the late onset of symptoms and rapid progression of the tumor. Unfortunately, despite increasing efforts to improve surveillance, diagnosis, and treatment, the overall 5-year survival remains less than 15-20%. 5,6 These statistics further re-enforce the need to identify risk factors for BE and the need for early endoscopic detection, followed by tailored surveillance strategies for early detection of dysplasia or EAC. Patients with EAC limited to the mucosa (T1a) appear to have better outcomes with both endoscopic and surgical treatment, with 5-year survival rates greater than 80%. 7 Endoscopic ablation techniques are frequently used to eliminate dysplastic BE and therefore decrease the risk of progression to EAC. 8,9
Endoscopic treatment modalities in use today include multipolar electrocoagulation (MPEC), argon plasma coagulation (APC), radiofrequency ablation (RFA), and cryotherapy. Currently, the most commonly utilized first-line treatment is RFA, with studies reporting CE-D to be as high as 90.5-95% in LGD 1,10 and 81% in HGD. 1 In the last decade, endoscopic cryotherapy has emerged as yet another ablative technique, 11 first reported for endoscopic use with a liquid nitrogen spray based device in 2005. 12 Another device using compressed carbon dioxide has proven to be effective therapy for elimination or treatment of Barrett’s neoplasia, 13,14 and a third most recently developed system utilizing a nitrous-oxide based (the cryo-balloon) ablation system has also demonstrated promising results. 15,16
A meta-analysis of 11 studies suggested cryotherapy as a safe and efficacious second-line therapy for patients who were previously treated with RFA and have persistent dysplasia or intestinal metaplasia (IM). 17 The study reported that cryotherapy was able to successfully achieve CE-IM and CE-D in approximately 50% and 75% of the patients, respectively. 17 A small number of studies have evaluated the use of cryotherapy as a primary treatment modality, given its remarkable safety profile. One study utilizing cryoablation treatment reported CE-IM of 41% (p = 0.02) and CE-D of 79% (p = 0.15), with as high as 88% of patients with HGD achieving CE-D (p = 0.99). 18 A recent meta-analysis of 6 studies found the efficacy of cryotherapy as a first line therapy to be 69% for CE-IM and 97% for CE-D. However, the meta-analysis only included full text studies and inadvertently missed some key studies. Based on high reported rates of CE-IM and CE-D with cryotherapy, and its encouraging safety profile, we aimed to perform an updated systematic review and meta-analysis to evaluate the efficacy of cryotherapy as primary treatment for BE.
Methods
All procedures used in this meta-analysis were consistent with the PRISMA (Meta-analysis Of Observational Studies in Epidemiology) criteria for observational studies. 19
Selection Criteria
The studies considered in this meta-analysis were case-control studies, cohort studies, or clinical trials of use of cryotherapy for BE. Only the studies that included biopsy confirmed dysplastic or neoplastic BE (LGD, HGD, ImCA) who underwent ≥1 session of cryotherapy (either liquid nitrogen, carbon dioxide gas, or balloon-based or focal liquid nitrous oxide) with follow-up endoscopy were included. We included patients with initial treatment for ImCA with endoscopic mucosal resection (EMR). We excluded patients that were treated with RFA, MPEC, APC, chemoradiation or other ablative therapies prior to cryotherapy. We also excluded patients that were treated for non-dysplastic BE. Studies with published full text or abstract form were included to prevent reporting bias. If more than 1 publication from a study or institution was identified, the most recent publication with relevant information was included for meta-analysis to avoid duplicate data.
Data Sources and Search Strategy
We conducted a comprehensive search of Ovid MEDLINE In-Process & Other Non-Indexed Citations, Ovid MEDLINE, Ovid Embase, Ovid Cochrane Central Register of Controlled Trials, Ovid Cochrane Database of Systematic Reviews, Web of Science, and Scopus from January 2000 to March 2020. The search strategy was designed and conducted by study investigators (R.T. and V.K.) and experienced library staff, independently. The search was limited to studies in the English language. Controlled vocabulary supplemented with keywords was used to search for studies of cryotherapy use for BE. Main keywords used in the search were the following: barrett,* esophag,* oesophag,* barrett esophagus, esophageal diseases, dysplas,* metaplas,* columnar,* esophagitis, peptic/or esophageal stenosis, cryosurgery,* cryother,* cryoablat,*cryogen,* freeze,* cryo,* cancer*, carcinoma* or adenocarcinoma*. The detailed search strategy is described Online Appendix 1.
Two authors (R.T. and V.K.) independently reviewed the titles and abstracts of the identified studies, and those that did not answer the research question of interest were excluded. The abstracts and full texts of the remaining articles were reviewed to determine inclusion criteria fulfillment. The reference lists of articles with information on the topic were also reviewed for additional pertinent studies. We then manually searched the abstracts from major gastroenterology conferences from 2000 to 2020. A flow diagram of included studies is shown in Figure 1.

Flow diagram of study selection process.
The modified version of Newcastle-Ottawa scale was used to assess the methodologic quality of the included studies by 2 investigators (R.T. and M.H.). 20,21 Using this scale, studies were accessed by 6 questions (representative of community, cohort size, EMR before cryotherapy, number of cryotherapy sessions, verification of no prior ablative treatment before cryotherapy, adequacy of follow up) (Supplementary Table 1). Studies with a cumulative score >3 were considered high quality. Any discrepancies were addressed by a joint re-evaluation of the original article.
Data Abstraction
Data was independently abstracted to a predetermined collection form by 2 investigators (R.T. and M.H.). Data collected for each study included study setting and design, year of publication, location, patient characteristics, histological pathology before cryotherapy, length of BE segment and follow up period. Conflicts in data abstraction were resolved by consensus, referring to the original article.
Outcomes Assessed
Our primary analysis focused on calculating pooled proportions of patients achieving CE-D and/or CE-IM. We also performed subgroup analyses to calculate pooled proportion of CE-D and CE-IM for full text studies, high quality studies and studies with liquid nitrogen cryotherapy, separately. Adverse events, when reported, were also extracted.
Statistical Analyses
Our primary outcome of the pooled analysis was clinical cure rates. The random-effects model described by DerSimonian and Laird 22 was used to calculate weighted pooled resolution rate (WPR). We calculated WPR with corresponding 95% CIs for the overall analysis as well as subgroup analyses. Data was weighted on the basis of sample size in each study to calculate WPR. Freeman-Tukey double arcsine transformation was used to avoid giving more weight to studies with prevalence estimates that are too large or too small. We assessed heterogeneity within groups with the I 2 statistic, which estimates the proportion of total variation across studies that is due to heterogeneity in study patients, design, or interventions rather than chance; I 2 values greater than 50% suggest substantial heterogeneity. 23 All P values reported were 2-tailed and considered statistically significant if < 0.05. For all tests (except for heterogeneity), a probability level less than .05 was considered statistically significant. Publication bias was assessed by visual inspection of funnel plots and numerically using LFK (Luis Furuya-Kanamori) estimate on a Doi plot (No asymmetry: LFK index within ±; minor asymmetry: LFK index exceeds ±1 but within ±2; major asymmetry: LFK index exceeds ±2). Publication bias was considered if the given analyses had major asymmetry on the inspection of funnel plots. If publication bias was found on funnel plot, we used the trim and fill for adjusting publication bias. 23,24 OpenMetaAnalyst version 10.10 was used for all statistical calculations. 25
Results
Search Results
The described search strategy revealed 1478 potentially relevant studies; titles and abstracts were screened and full manuscripts were obtained for relevant articles (Figure 1). In all, 109 articles were reviewed, of which 95 were excluded for various reasons (Figure 1). A total of 14 studies were included in this meta-analysis. 13,18,26 -37 Of those, 9 were full text articles and 5 were abstracts.
Quality of Included Studies
The quality of included studies is presented in Supplementary table 1. In all, 8 studies were high quality and 6 were low quality. Median NOS score was 3.5 (range 1.5-4.5).
Characteristics of Included Studies
Among the 14 included studies, 6 were retrospective and 8 were prospective. 11 studies were single center and 3 were multicenter. Cryotherapy was most commonly performed using liquid nitrogen (n = 11), however carbon dioxide gas (n = 2) and nitrous oxide balloon treatment (n = 1) were also included. There was a median of 4 cryotherapy sessions per patient. Most patients were older (mean age range 60.5 to 70.9), male, and had long-segment BE (median of 4.6 cm). The median follow-up period was 22.45 months or 1.8 patient years for CE-D (range 3-54 months, Table 1).
Study and Patient Characteristics.

BE: Barrett’s esophagus; EAC: esophageal adenocarcinoma; ImCA: intramucosal carcinoma; LGD: low grade dysplasia; HGD: high grade dysplasia; IND: indefinite for dysplasia; IM: intestinal metaplasia; EMR: endoscopic mucosal resection; APC: Argon; SC: single center; MC: multicenter; NR: not recorded.
Pooled Rate of CE-D
In 13 studies, a total of 321/405 patients achieved CE-D with a pooled proportion of 84.8% (95% confidence interval [CI] 72.2-94.4), with substantial heterogeneity (I 2 = 88.3%) (Figure 2). No publication bias was seen on Doi plot (Supplementary Figure 1).

Efficacy of cryotherapy as primary treatment for complete eradication of dysplasia.
Pooled Rate of CE-IM
In 12 studies, a total of 244/393 patients achieved CE-IM with a pooled proportion of 64.2% (95% confidence interval [CI] 52.9-74.8), with substantial heterogeneity (I 2 = 77.9%, Figure 3). Mild asymmetry was seen on the doi plot (Supplementary Figure 2).
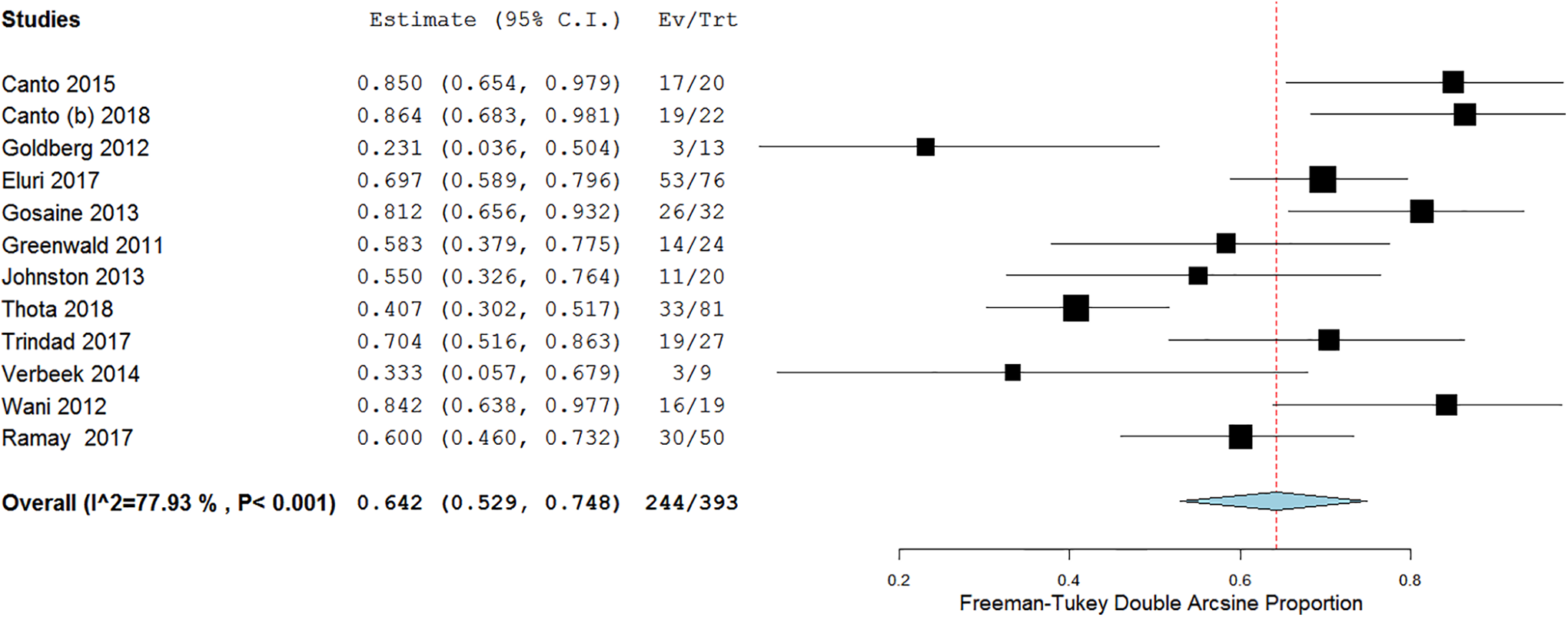
Efficacy of cryotherapy as primary treatment for complete eradication of intestinal metaplasia.
Pooled Rate of CE-D With Liquid Nitrogen Cryotherapy
A total of 10 studies reported the rates of CE-D with liquid nitrogen cryotherapy. On meta-analysis, the pooled proportion of CE-D was 83.6% (95% CI, 68.2-94.9, I 2 = 90.58%).
Pooled Rate of CE-IM With Liquid Nitrogen Cryotherapy
A total of 9 studies reported the rates of CE-IM with liquid nitrogen cryotherapy. On meta-analysis, the pooled proportion of CE-IM was 61.4% (95% CI, 49.5-72.8, I 2 = 77.33%).
Pooled Recurrence Rates
A total of 4 studies assessed the rate of recurrence after cryotherapy. Follow-up period was variable among those. Of a total of 85 patients, 15 had recurrence of HGD with pooled rate of 17.6%. Four studies evaluated for recurrence rates of IM. Of those, 41 of 116 patients developed recurrence with a pooled rate of 35.3%.
Pooled Rate of Persistent Intestinal Metaplasia, Dysplasia and Progression to Cancer
A total of 6 studies evaluated the rates of persistent IM and dysplasia. The pooled rate of persistent IM was 13.7% and for persistent dysplasia was 7.3%. A total of 2 studies evaluated for progression of cancer with rate of 3.8% (3/77 patients).
Subgroup Analyses
Full Text Studies
A total of 9 full text studies reported the rates of CE-D. Subgroup analysis of only full text studies revealed a pooled proportion of CE-D 88.4% (95% CI, 79.6-95.2, I 2 = 72.7%).
A total of 8 full text studies reported the rates of CE-IM. Subgroup analysis of only full text studies revealed a pooled proportion of CE-IM 65.9% (95% CI, 51.4-79.1, I 2 = 80%).
High Quality Studies
A total of 8 studies reporting CE-D were considered high quality. Subgroup analysis of only high-quality studies revealed a pooled proportion of CE-D 91.3% (95% CI, 83.0-97.4, I 2 = 69.5%).
A total of 8 studies reporting CE-IM were considered high quality. Subgroup analysis of only high-quality studies revealed a pooled proportion of CE-IM 71.6% (95% CI, 59.0-82.9, I 2 = 80.9%).
Adverse Events
Of the included studies, 11 studies reported individualized adverse events. One study was excluded from the analysis, because the study reported adverse effects in proportion to the number of procedures performed rather than patients. 27 The rate of adverse events was 12.2% (45/367). Most common adverse events were esophageal strictures (n = 27) followed by post procedural pain (n = 10). Gastric perforation was reported in 2 patients in the cohort, one following carbon dioxide gas delivery and the other with liquid nitrogen-based spray therapy. Both patients were successfully managed with surgical intervention. Bleeding was reported in 2 patients but the severity of the bleed was not stated. Two patients from the cohort developed esophagitis as a post-procedural side effect (4.4%; 2/45). No deaths related to cryotherapy treatment were reported in any of the studies.
Discussion
Endoscopic ablative therapy is a widely accepted treatment modality for dysplastic BE and/or early esophageal neoplasia. Techniques such as RFA and cryotherapy have been shown to be effective at downgrading dysplasia and reversing IM to neosquamous epithelium in several prior studies. However, cryotherapy has been primarily reported as second line therapy for patients who do not achieve CE-D or CE-IM with RFA. Our primary aim through this systematic review and meta-analysis was to determine the efficacy of cryotherapy as first-line treatment in patients with dysplastic BE and/or early esophageal neoplasia. The reported efficacy of RFA in the literature is comparable to the efficacy of cryotherapy in our study. One meta-analysis of 18 studies with 3802 patients reported CE-D in 91% and CE-IM in 78% with RFA. 10 Our analysis of shows that cryotherapy is an effective modality for treatment of dysplastic BE with a pooled rate of achieving CE-D of 84% and a pooled rate of achieving CE-IM of 64%. This suggests cryotherapy may be an effective endoscopic ablative modality for first-line therapy in patients with dysplastic and early neoplastic BE.
There may be several advantages to using cryotherapy over RFA for first line treatment of dysplastic BE and/or early esophageal neoplasia. RFA is technically challenging in patients who have a tortuous esophagus, significant esophageal stricturing or nodular BE, 11 whereas cryotherapy is not significantly limited by these anomalies. Cryotherapy penetrates deeper into tissue with less injury to the tissue architecture and subsequently has a lower risk of stricture formation and post-procedural discomfort compared to heat-based ablative modalities. 11 Cryotherapy has been successfully performed on patients with bleeding diathesis or anticoagulation. 18
The first pilot study for use of cryotherapy in Barrett’s esophagus was reported by Johnston et al in 2005 and included 11 patients who were treated with liquid nitrogen-based spray cryotherapy. Of the 9 patients who completed the study, all achieved CE-IM at the end of treatment. 12 Over the years, 2 additional endoscopic cryotherapy platforms have been developed, one utilizing compressed carbon dioxide spray and the other utilizing a nitrous-oxide balloon-based ablation system. Studies utilizing any of these 3 cryotherapy treatment modalities were included in our analysis.
There are important differences between the 3 modalities of cryotherapy, including delivery platform/gas used, freezing temperature, and dosimetry. The most largely represented delivery method in our analysis is liquid nitrogen-based spray cryotherapy (G2 system from 2007 to 2012 and the truFreeze device from 2013 to present; CSA Medical, Lexington, MA). In this system, liquid nitrogen is delivered at −196 °C via a 7F flexible catheter which is introduced through the biopsy channel of a standard endoscope. Several freeze-thaw cycles are performed. A decompression tube is utilized to vent the esophagus and the stomach to reduce the risk of perforation due to the rapid expansion of nitrogen gas. Dosimetry ranges from 20 seconds x 3 applications (with intermittent thawing between sprays) or 30 seconds x 2 applications for flat dysplastic BE.
Subgroup analysis of studies that use liquid nitrogen cryotherapy revealed efficacy of 83% for CE-D and 61% for CE-IM. A recent retrospective analysis published last year compared RFA and liquid nitrogen spray cryotherapy and concluded that patients who received cryotherapy had comparable rates of achieving CE-D (78.8% vs 87.5%, p = 0.15) but lower rate of achieving CE-IM (66.7% vs 41.3%, P = 0.002) compared to RFA. 18 Similar rates of achieving CE-D and CE-IM have been shown in prior studies as well. In 2010, Greenwald et al published their results of 17 patients treated with liquid nitrogen-based spray cryotherapy. They reported complete eradication of HGD (CE-HGD), CE-D, and CE-IM of 94%, 88%, and 53%, respectively. 27 A larger, multi-center, retrospective cohort which included 60 patients with high grade dysplasia, reported similar findings with 97% of patients having achieved CE-HGD, 87% achieved CE-LGD, and 57% achieved CE-IM. 38
Two studies in our meta-analysis used a liquid carbon dioxide-based cryotherapy system (Polar Wand; GI Supply, Camp Hill, PA). This is a through the scope system which utilizes multiple freeze-thaw cycles and also requires continuous gastric decompression. It freezes the mucosa at −80 oC. The catheters for this device were discontinued in March 2016 by the manufacturer and it is no longer in use.
The third method of delivery included in our analysis involves the use of a new contact cryoballoon focal ablation system (C2 Therapeutics, Inc, Redwood City, CA). This is a portable, battery-powered system in which liquid nitrous oxide is converted to gas within a single-use low pressure compliant balloon freezing targeted mucosa to −85 oC. The cryogen can be directed toward the targeted mucosa by rotating the catheter and/or sliding it up and down within the balloon. It is applied as a single application of 6-12 seconds. A decompression tube is not necessary in this system. Canto et al reported their results from 22 treatment naïve patients. CE-HGD, CE-LGD, and CE-IM rates were 100%, 100%, and 86%, respectively, 19 which are very comparable to the CE-D and CE-IM rates of RFA. 10
There were no significant differences in the calculated rates of CE-D and CE-IM in our subgroup analysis. Our calculated adverse-events rate was 12.2%. Due to limited data on the reported adverse events, we did not attempt to analyze their pooled rates. The most common adverse events reported were esophageal stricture and chest pain. There were no deaths reported in any of the studies.
The strengths of our study include a comprehensive literature review which presents data from all available papers on this topic. Our meta-analysis includes well-defined inclusion criteria (carefully excluding redundant studies), estimation of CE-IM and CE-D rates, with detailed extraction of adverse events and rigorous evaluation of study quality. We excluded all the studies which had included patients who were previously treated with another modality of ablation.
Our study has some limitations. The individual studies included in our meta-analysis varied in several ways including study design, differences in delivery of cryotherapy (liquid nitrogen vs. CO2 vs. nitrous oxide), number of sessions of cryotherapy and follow up period. There is therefore significant heterogeneity but that is to be expected when different technologies are at play over a period of time with different dosimetry and treatment algorithms. Additionally, all the included studies are observational in nature, hence the quality of evidence available from the current body of literature is low.
Conclusion
Cryotherapy is a well-established endoscopic ablative modality which induces tissue injury through mucosal freezing with liquid nitrogen, carbon dioxide gas, or balloon-based nitrous oxide. This systematic review and meta-analysis demonstrates cryotherapy as primary treatment for dysplastic BE and/or early esophageal neoplasia can achieve rates of CE-D and CE-IM similar to those reported for RFA, with an acceptable adverse event profile.
In addition, Cryotherapy is increasingly being used as a “salvage” therapy in patients who do not achieve CE-IM or CE-D with RFA and for palliative endotherapy in patients with locally advanced esophageal cancer. It is also to be noted that Cryotherapy is an effective option for first line treatment, especially in patients with esophageal anatomic challenges that make RFA treatment technically challenging.
In our meta-analysis, we found endoscopic Cryotherapy to be effective for treatment of dysplastic BE and associated early esophageal neoplasia in patients naïve to ablative therapy with >80% achieving CE-D and 63% achieving CE-IM. Therefore, Cryotherapy could also be offered to patients as first line treatment for dysplastic BE and early esophageal neoplasia, when discussing treatment options. Further studies with standardized treatment protocols and long-term follow-up to demonstrate durability will further clarify the role and efficacy of the currently available cryotherapy modalities and how they compare to the non-cryoablation platforms used in BE endotherapy.
Supplemental Material
Supplemental Material, sj-pdf-1-ccx-10.1177_1073274820976668 - Efficacy of Cryotherapy as a Primary Endoscopic Ablation Modality for Dysplastic Barrett’s Esophagus and Early Esophageal Neoplasia: A Systematic Review and Meta-Analysis
Supplemental Material, sj-pdf-1-ccx-10.1177_1073274820976668 for Efficacy of Cryotherapy as a Primary Endoscopic Ablation Modality for Dysplastic Barrett’s Esophagus and Early Esophageal Neoplasia: A Systematic Review and Meta-Analysis by Raseen Tariq, Sarah Enslin, Maham Hayat and Vivek Kaul in Cancer Control
Supplemental Material
Supplemental Material, sj-pdf-2-ccx-10.1177_1073274820976668 - Efficacy of Cryotherapy as a Primary Endoscopic Ablation Modality for Dysplastic Barrett’s Esophagus and Early Esophageal Neoplasia: A Systematic Review and Meta-Analysis
Supplemental Material, sj-pdf-2-ccx-10.1177_1073274820976668 for Efficacy of Cryotherapy as a Primary Endoscopic Ablation Modality for Dysplastic Barrett’s Esophagus and Early Esophageal Neoplasia: A Systematic Review and Meta-Analysis by Raseen Tariq, Sarah Enslin, Maham Hayat and Vivek Kaul in Cancer Control
Supplemental Material
Supplemental Material, sj-pdf-3-ccx-10.1177_1073274820976668 - Efficacy of Cryotherapy as a Primary Endoscopic Ablation Modality for Dysplastic Barrett’s Esophagus and Early Esophageal Neoplasia: A Systematic Review and Meta-Analysis
Supplemental Material, sj-pdf-3-ccx-10.1177_1073274820976668 for Efficacy of Cryotherapy as a Primary Endoscopic Ablation Modality for Dysplastic Barrett’s Esophagus and Early Esophageal Neoplasia: A Systematic Review and Meta-Analysis by Raseen Tariq, Sarah Enslin, Maham Hayat and Vivek Kaul in Cancer Control
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Vivek Kaul is a consultant for CSA Medical (Now Steris Corp) and Cook Medical.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.