
Abstract
Traditional methods of cancer treatment are usually based on the morphological and histological diagnosis of tumors, and they are not optimized according to the specific situation. Precision medicine adjusts the existing treatment regimen based on the patient’s genomic information to make it most suitable for patients. Detection of genetic mutations in tumors is the basis of precise cancer medicine. Through the analysis of genetic mutations in patients with cancer, we can tailor the treatment plan for each patient with cancer to maximize the curative effect, minimize damage to healthy tissues, and optimize resources. In recent years, next-generation sequencing technology has developed rapidly and has become the core technology of precise targeted therapy and immunotherapy for cancer. From early cancer screening to treatment guidance for patients with advanced cancer, liquid biopsy is increasingly used in cancer management. This is as a result of the development of better noninvasive, repeatable, sensitive, and accurate tools used in early screening, diagnosis, evaluation, and monitoring of patients. Cell-free DNA, which is a new noninvasive molecular pathological detection method, often carries tumor-specific gene changes. It plays an important role in optimizing treatment and evaluating the efficacy of different treatment options in clinical trials, and it has broad clinical applications.
Tumorigenesis is characterized by uncontrolled cell growth leading to cancer. 1 -3 Normal cells can become cancerous due to genetic mutations and epigenetic modifications. 4 -6 Patients with different cancer have different genetic mutations and epigenetic modifications, which increase the complexity and heterogeneity of tumors. 7,8 In addition, intratumoral heterogeneity increases over the course of disease development, making the treatment of tumors particularly challenging. 9 -12
The development of next-generation sequencing (NGS) technology and bioinformatics has decoded a large number of cancer genome data, which has also promoted the development of targeted therapy and immunotherapy, especially for invasive cancer types that do not respond to traditional treatment options1 3 -15 (Figure 1). Through the detection of cell-free DNA (cfDNA) genetic information in cancer cells, immune cells, or liquid biopsy samples by NGS, we can access key genetic mutations in patients with cancer. Assessment of these mutations can help inform whether patients will respond to targeted therapy or immunotherapy. Furthermore, new treatment options can be developed by creating new drugs to target these mutations. 16 -18 Immune drugs induce the body’s immune system to attack and treat tumors and develop more effective immunological checkpoint inhibitors or Chimeric Antigen Receptor T-Cell Immunotherapy(CAR-T) or cancer vaccines. 19 -21
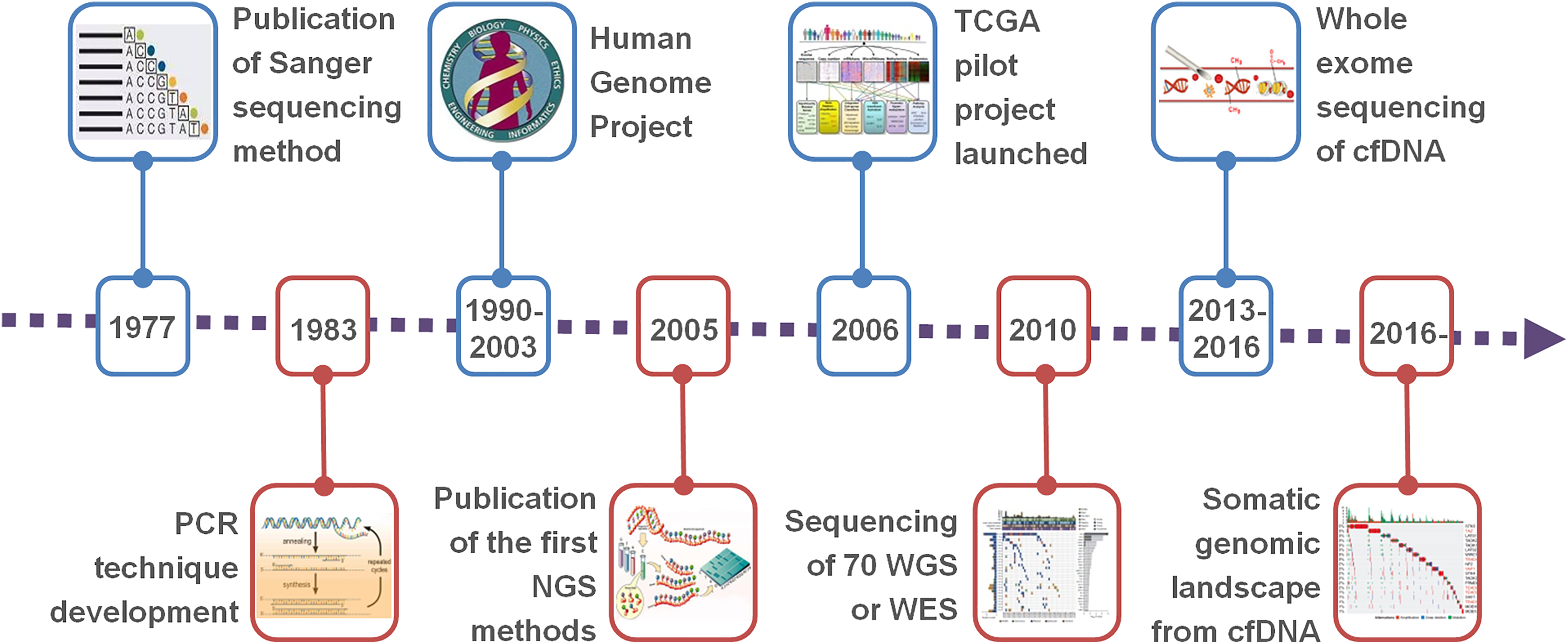
Time line of major achievements in sequencing technologies.
Precision Medicine and Tumor Gene Detection
Precision medicine is a new term, replacing individualized medicine. There are many overlaps between precision medicine and individualized medicine. 22 -24 However, precision medicine mainly refers to adjusting the existing treatment plan according to the patient’s genomic information, making it most suitable for patients, while individualized medicine is often based on creating new treatment methods or plans based on the patient’s genomic information. 25 -27 This process is lengthy and may not benefit patients with cancer. For this reason, the National Research Council, which is responsible for the management of science, technology, engineering, and mathematics in the United States, recommended replacing “individualized medicine” with “precision medicine” in 2011. 28 In early 2015, President Barack Obama launched the Precision Medicine program. At the same time, at the end of 2015, China also launched the “Precision Medicine” program and included it in the 13th Five-Year Plan of China. 29
As it pertains to precision medicine for cancer treatment, detection of genetic aberrations is the basis of developing effective treatment options. 30 -32 Through the analysis of genetic mutations in patients with cancer, we can tailor the treatment plan for each patient with cancer to maximize the curative effect, minimize the damage, and optimize the resources. 33 -36
Next-Generation Sequencing and Precise Targeting Therapy for Tumors
Next-generation sequencing, also known as large-scale parallel sequencing, can simultaneously sequence millions or even billions of DNA molecules, achieving the goal of large-scale, high-throughput sequencing. 37 -40 This makes NGS a revolutionary progress following Sanger sequencing (first-generation sequencing). 8,41,42 In recent years, NGS technology has been developed and applied rapidly, especially in cancer gene detection. In the United States, medical NGS services (FMI and MSK) from commercial companies and academic institutions were approved by Food and Drug Administration (FDA) in 2017, suggesting that NGS has been formally applied in clinical practice. 43 At the same time, the approval process for various medical NGS services is also accelerating. In 2017, the National Cancer Institute launched a National Cancer Precision Medical Survey, which found that 75.6% of oncologists in the United States are using NGS gene detection technology to guide cancer treatment. 44
From 2018 to 2019, 5 cancer NGS products were approved by National Medical Products Administration, suggesting that NGS has officially entered the stage of clinical application in China. 45 -47 Currently, the FDA has approved concomitant diagnostic technologies in oncology, such as immunohistochemistry (IHC), in situ hybridization (fluorescence in situ hybridization/chromogenic in situ hybridization), real-time fluorescence quantitative polymerase chain reaction, and NGS. 48 Excluding IHC, the other 3 are gene detection techniques; among them, NGS has become the core technology of precise targeted therapy and immunotherapy for cancer. 49 -52
The NGS mutation profiles obtained from different tumors have led to the emergence of targeted therapies for tumors, which include identifying mutations in signaling pathways and blocking them with existing or newly developed drugs. 53 -56 The detected mutations are classified as driver mutations if they are critical to the maintenance of tumors and passenger mutations if they have no definite role in the maintenance of tumors. 57 -60 This classification therapy led to the development of imatinib, a constitutive inhibitor of BCR-ABL kinase, for the treatment of leukemia. 61 -63
At present, targeted therapeutic drugs include small molecule inhibitors and macromolecular monoclonal antibody drugs. For drugs with definite targets, it is necessary to use gene detection before they can be used (Figure 2).

Epigenetic drugs for cancer therapy. Epigenetic drugs being studied for human cancer are listed.
Next-Generation Sequencing and Immunotherapy for Tumors
In 2018, a study in Nature Medicine showed that when a patient with metastatic breast cancer did not respond to several kinds of chemotherapy and had a life expectancy of only a few months, somatic cell mutations were detected by NGS technology, and immunotherapy was administered to completely eliminate the tumor. 64 Thus, the genomic information of tumors detected by NGS can identify patients who may respond to immunotherapy, use immunodrugs to induce the body’s immune system to attack and treat tumors, or develop more effective immune checkpoint inhibitors or CAR-T or cancer vaccines. 65 -67
Under normal physiological conditions, the immune system recognizes and eliminates mutant cells. 68 However, tumors occur when cancer cells escape the immune system by creating an immunosuppressive environment. 69 -72 Therefore, the focus of recent research has shifted from targeted therapy to immunotherapy, hoping to be used to treat more patients with cancer. This is as a result of immune escape being common for all tumors, and restoring the immune system can help destroy tumors.
Immunotherapy is not equally effective for all types of tumors, and the efficacy varies from patient to patient. 73 -77 The possible reasons are the heterogeneity of T cells and tumor cells and their complex interactions in the tumor microenvironment. 78 -81 Immunogenomics is a relatively new field of cancer research. The detection and analysis of whole-genome sequencing (WGS), whole-exome sequencing (WES), and RNA sequencing (RNA-Seq) on T cells and tumor cells by NGS technology can obtain genome maps of tumors and immune cells, which can help to customize treatment schemes for specific characteristics of tumors and increase the possibility of success. 82 -84 At the same time, NGS technology can be used to evaluate the changes in biomarkers of immunological checkpoint inhibitors, such as tumor mutational burden (TMB), microsatellite instability, and PD-L1 amplification and other therapeutic effects, drug resistance, and genetic mutations related to hyperprogression. 64,85 -87
In cancer vaccines, the immune system is stimulated to produce antibodies. 88 In adoptive T-cell therapy, T cells are isolated from the body, stimulated and amplified in vitro, and then infused back into the patient. 89 -91 Genetic modification of T cells (CAR-T cells) by chimeric antigen receptors can improve the immune response of T cells. 92 Detection and analysis of WGS, WES, and RNA-seq in T cells and tumor cells by NGS technology will help to improve the design of CAR-T cells and the selection of new antigens. Tumor cells secrete and express new antigens on the surface of cells to escape recognition of T cells. 93 -96 Patient-derived T cells can grow in vitro and can be stimulated with these new antigens to elicit a strong T-cell response. 97 To further enhance the ability of T cells to recognize tumors, CAR-encoded DNA was introduced into T cells (CAR-T cell therapy). 98 Therefore, once T cells increase, they will be transferred back to the patient, where they can now recognize tumor antigens, thereby improving the effectiveness of inducing cancer cell death and clearance. Detection and analysis of WGS, WES, and RNA-seq in T cells and tumor cells by NGS technology will help to improve the design of CAR-T cells and the selection of new antigens.
The progress of NGS technology and bioinformatics is expected to improve the recognition of new antigens and the effectiveness of cancer vaccines. 99 -102 Single-cell genomics will be particularly helpful in revealing the expression, mutation of tumor genes, and the heterogeneity of new immune cells in the same tumor, which can be used to develop cancer vaccines targeting different clonal populations in tumors. 103 -106 Therefore, NGS technology (WGS, WES, RNA-seq, ChIP-seq, NGS panel, etc) has become the core development and application technology of precise targeted therapy and immunotherapy for cancer. It can help us better understand tumors, tumor microenvironment, and T cells and then provide personalized treatment programs for patients with cancer.
Next-Generation Sequencing and cfDNA Detection
“Liquid biopsy” is often used to analyze cfDNA in plasma and other body fluids (such as pleural effusion, ascites, and cerebrospinal fluid), as well as circulating tumor cells (CTCs) and other nucleic acids (such as RNA and microRNA) in blood. 107 -109 Circulating tumor cells in blood exist at very low concentrations, usually less than 10 CTCs per milliliter of blood, even in patients with metastatic disease. 110 This low concentration characteristic greatly limits the diagnostic and analytical potential of CTCs. Compared with CTC, the proportion of cfDNA contributed by cancer cells was significantly higher. 111 In advanced patients with hepatocellular carcinoma (HCC), DNA fragments carrying cancer-specific mutations account for more than 50% of cfDNA. 105 It is also because the proportion of cancer-derived DNA in cfDNA is higher than that of CTCs in nucleated blood cells, and therefore, the analysis of cfDNA is more widely used in cancer management than that of CTCs.
From early cancer screening to treatment guidance for patients with advanced cancer, liquid biopsy is increasingly used in cancer management. Liquid biopsy may overcome the limitations of tumor markers (mainly proteins or glycoproteins) in conventional tissue samples. 112 -115 Cancer-related mutations, including single-nucleotide mutations, copy number changes, methylation changes, and DNA fragmentation patterns have been detected in cfDNA of patients with various cancer by NGS technology (Figure 3). 74,116 -118

Time line of the main important discoveries of circulating tumor DNA.
Most cancers are relatively asymptomatic in their early stages. 119 As such, most patients are diagnosed with advanced cancers. In this regard, liquid biopsy can be used for cancer surveillance and diagnosis. Detection of genetic mutations by enlarging the target region can improve sensitivity. 120 Mutations from tumors can be used to monitor clinical progress and detect residual lesions after treatment. 116,121 -123 Abnormal methylation signals in cfDNA molecules enable detection of ultra-early tumors, and genome-wide methylation histological analysis of plasma DNA tissue location can be used as a “whole-body molecular imaging” method to identify potential tissue origins of mutations detected in cfDNA. 124 -127
An important application of cfDNA analysis is to guide treatment decisions, especially in targeted therapy. 128 -130 For example, liquid biopsy to analyze EGFR mutations has been widely used to guide the use of epidermal growth factor receptor-tyrosine kinase inhibitors. 131 Many studies have demonstrated that targeted large-scale parallel sequencing can be used to identify cancer-related driver mutations in the cfDNA of patients with HCC. 132 -134 Further studies have shown that the mutation characteristics of cfDNA reflect the state of the corresponding tumor tissues. 114,135,136 Of course, the potential of cfDNA mutation analysis for cancer treatment management should not be underestimated. 137 An NGS-based liquid biopsy provides a noninvasive method for large-scale assessment of mutation profiles in patients with advanced cancer (Figure 4).

Multitude of factors secreted in the circulatory system with the sustained growth of tumor. A liquid biopsy contains wealth of information relevant to determining tumor status, metastatic potential, and likelihood of relapse. Some of the contributing factors to making such an assessment include circulating tumor cell (CTC) counts, CTC genetic profile and protein expression, levels of circulating tumor DNA/RNA, and the presence or absence of known mutations or epigenetic signatures. A thorough analysis of liquid biopsies from patients with cancer screening for these factors can reveal essential information for personalized care.
Recent studies have shown that TMB can predict the clinical response of patients to immunotherapy in a variety of solid tumors. 138 -140 Tumor mutational burden detection based on NGS and cfDNA can be used to predict the therapeutic response of patients with non-small-cell lung cancer to the PD-L1 immunosuppressant atezolizumab, and its immunotherapeutic effect is independent of the expression of PD-L1. 141 -143
Conclusion
Cancer is a relatively heterogeneous disease with multiple causes and carcinogenic driving events. The analysis of cfDNA mutations based on NGS can better characterize patients, and it can be applied to early cancer screening and treatment guidance for patients with advanced cancer. It can optimize patient’s treatment and evaluate different treatment options in drug trials.
Footnotes
Authors’ Note
T.-M.W., J.-B.L., W.L., and G.-R.W. contributed equally to this work. Y.S.M. and D.F. designed the study. All authors performed the statistical analyses and interpreted the data. D.F. wrote the manuscript. All authors contributed to the final version of the manuscript and approved the final manuscript.
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported partly by grants from the National Natural Science Foundation of China (81972214, 81772932, 81472202, 81201535, 81302065, 81671716, 81301993, 81372175 and 81472209), The Fundamental Research Funds for the Central Universities (22120170212 and 22120170117), The Scientific Research Fund Project of Anhui Medical University (2018xkj058), Shanghai Natural Science Foundation (12ZR1436000), Shanghai Municipal Commission of Health and Family Planning (201540228), Special Funding Fund for Clinical Research of Wu Jieping Medical Foundation (320.6750.14326), Nantong Science and Technology Project (YYZ15026), The Peak of Six personnel Foundation in Jiangsu Province (WSW-009), The Fifth Phase of 333 Talents Engineering Science and Technology Project of Jiangsu Province (2017205), and Jiangsu Province Science Foundation for Youths (BK2012101).