
Abstract
This survey was conducted to determine the head and neck cancer (HNC) treatment strategies followed by oncologists in Chinese hospitals. It was a questionnaire-based survey, conducted from October 2017 to January 2018 in 100 random tertiary hospitals in 21 cities of China to elicit information from oncologists on the management practices for treating HNC in China. A validated, structured questionnaire was used for formal investigation with oncologists. The questions regarding HNC types, treatment strategies used for locally advanced head and neck cancer (LA HNC) and recurrent/metastatic head and neck cancer (r/m HNC), diagnosis and prognostic factors were included. The results were presented as percentages. Among the 272 oncologists, 93.4% were from tertiary care hospitals, with 35.3% and 36.4% patients from radiotherapy (RT) and oncology department, respectively. Nasopharyngeal carcinoma was the most commonly treated type of HNC according to 65.1% oncologists. Patients aged >75 years have worse prognosis and 65% oncologists corroborated that age of the patients influences treatment decision. Most of the oncologists (77.6%) preferred chemotherapy (CT) + anti–epidermal growth factor receptor targeted therapy as the first-line therapy for r/m HNC. Approximately 95% of oncologists considered induction chemotherapy (ICT) to retain organ functions and tumor shrinkage and 43.4% preferred ICT followed by chemoradiotherapy or ICT combined with RT followed by targeted therapy for LA HNC. For the management of HNC, Chinese oncologists recommended ICT with RT and targeted therapy for LA HNC and CT regimen combined with targeted therapy for r/m HNC.
Keywords
Background
Head and neck cancer (HNC) has been reported as the sixth most common cancer globally, 1 with more than 600 000 newly diagnosed cases each year. 2 According to the National Central Cancer Registry of China, cancer statistics of China 2015, the total incidence of oral cavity and pharyngolaryngeal cancer was estimated as 48.1 per 100 000 with a mortality of 22.1, and incidence of nasopharyngeal cancer (NPC) was estimated as 60.6 with a mortality of 34.1 in China, in 72 local population-based cancer registries. 3 The incidence of HNC also has a large geographical variability across China. Among the 7 Chinese administrative regions, the incidence and mortality of HNC, specially NPC, are higher in South China including Guangxi, Guangdong, and Hunan provinces, compared to other regions, and lowest in North China, possibly due to early-life exposure to carcinogenic agents, 4,5 environmental pollution due to urbanization and industrialization, increase in the aged population, smoking, alcohol, betel nut chewing, and human papillomavirus (HPV) infection. 6 -8
There is evidence of a definite causal relationship between HPV infection and oropharyngeal cancer and has been regarded as one of the major risk factor for HNC prognosis. 9 In the United States and several European countries, approximately 60% to 80% of oropharyngeal cancers are related to HPV infection 10 -12 ; however, in the Chinese population, the HPV infection rate is relatively low. 1 In addition to HPV infection, age is also a major risk factor for HNC and has led to a rapid increase in cancers of the oral cavity and oropharynx with a median age of 62 years at diagnosis. Additionally, more than half of the oral cavity and oropharynx cancer deaths in 2012 occurred in patients of age ≥65 years. 13
The most frequent tumor sites of HNC are the larynx, oral cavity, and oropharynx. Additionally, HNCs also include NPC and paranasal and nasal sinus cancer. 2 As majority of the patients are in locally advanced stage, the management of HNC is often complex with combined therapies such as surgery, radiotherapy (RT), and chemotherapy (CT). When the goal is organ preservation or in case of unresectable cancer, a combination of RT and CT remains standard treatment. 1,14,15 Although multiple studies are available on the incidence and mortality of different types of HNCs in China, 7,16,17 no report exists regarding the clinical practices followed for HNC management in Chinese hospitals. In this study, we evaluated HNC treatment strategies by oncologists in randomly selected Chinese hospitals through a questionnaire-based survey and to confirm whether HNC treatment guidelines are being followed.
Materials and Methods
Study Design and Duration
This study was a questionnaire-based survey to elicit information from oncologists on the management practices for treating HNC in China. The design of the questionnaire and the survey was developed and conducted on the basis of established methodologies. 18,19 During October 2017 to January 2018, we planned to enroll an estimated 300 randomly selected oncologists from 100 randomly selected tertiary care hospitals in 21 Chinese cities.
Questionnaire Development
The entire survey was conducted in 4 stages, which included questionnaire development (stage 1), questionnaire finalization via a pretest (stage 2), formal investigation (stage 3), and statistical analysis (stage 4).
During stage 1, the project team members learnt and understood the relevant guidelines, social medical methodologies, which was followed by determination of presurvey questionnaires and sampling strategies. Finally, a questionnaire was developed after consulting 9 HNC experts. The second stage included the preexperiment procedure to confirm the reliability and validity of the developed questionnaire. A total of 40 head and neck specialist oncologists were selected from Beijing, Shanghai, Wuhan, Shenyang, and Guangzhou to conduct preexperiments. The pretest was conducted by a medical scientific liaison (MSL) as an interviewer with the HNC specialists. The interviewer observed, oncologist’s feedback, comparison of test results at 2 different times before and after, testing of technical details such as consistency and comprehensibility of the questionnaire, formal investigations based on test results, and expert opinion questionnaire. There were 40 responses, and Cronbach α measure was used to test for internal consistency of the questionnaire items. The final questionnaire contained 46 questions. The results revealed Cronbach α of approximately 0.7, which is considered to be optimal for consistency. 20 The Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy and Bartlett test of sphericity showed that the results were suitable for factor analysis (KMO = 0.684; Bartlett test of sphericity = 1536.64). Factor analysis results showed that the 34 items of the scale were divided into 6 dimensions, the cumulative variance contribution rate was 40.976% (>40% is good), and the structural validity is better. Of the 46 questions, 34 items were categorized into 6 dimensions: (1) treatment department (Q 19, 25, 26, 45, 46); (2) first consultation for HNC (Q 11, 30); (3) HPV diagnosis, prognostic value of HPV, age, and epidermal growth factor receptor (EGFR) test (Q 9, 12, 14, 15, 21, 24, 27, 31); (4) first-line therapy for metastatic recurrence HNC (Q 13, 44); (5) treatment regimens, management of HNC, and toxicity (Q 10, 17, 28, 33, 34, 35, 36, 37, 38, 39, 40); and (6) targeted therapy (Q 18, 22, 23, 32, 42, 43). The remaining 12 questions (Q 1, 2, 3, 4, 5, 6, 7, 8, 16, 20, 29, 41) were demographic characteristics and asked the respondents about their demographic characteristics, such as department, designation, experience, and geographical location; hence, they were not included in any dimension (Supplementary Table 1).
The third stage included formal investigation with the help of the finalized questionnaire for a large-scale survey, as described in the study design. Prior to the face-to-face interview, the MSLs were trained on interview techniques and questionnaire completion to ensure consistency in the quality of the responses. The survey included oncologists from tertiary Chinese hospitals from different cities, working in various departments such as RT, otolaryngology, oral surgery, HNC oncology, oncology, and chemoradiotherapy (CRT). The oncologists included in the survey were selected randomly using a software and were the ones who had the right to take treatment-related decisions. The fourth and the final stage consisted of analysis of the survey and populating the outcomes according to the dimensions used in the questionnaire.
As the study did not directly involve any patients, in accordance to the International Conference on Harmonization Good Clinical Practice guidelines, 21 ethics committee approval and informed consent from the patients were not sought.
Outcomes and Analysis
The evaluated outcomes were mostly HNC-type treated, treatment strategies used for locally advanced head and neck cancer (LA HNC) and recurrent/metastatic head and neck cancer (r/m HNC) and effect of HPV test and age on HNC prognosis. All responses to the survey questionnaire were analyzed using descriptive statistics and data were represented in form of percentage. During the analysis, completed questionnaires with missing data or missing essential information regarding the oncologist interviewed were excluded. Multiple questionnaires completed by the same oncologist were also excluded.
Results
The survey included 272 oncologists from 100 randomly selected tertiary care and other Chinese hospitals in 21 cities (Figure 1). Of these, 96 (35.3%) oncologists were from department of RT and 99 (36.4%) were from department of oncology (Q1), 254 (93.4%) oncologists were from tertiary care hospitals (Q2), and 204 (75%) oncologist’s hospitals were university-affiliated hospitals (Q3). Facility of multidisciplinary team (MDT) to treat with patients with HNC was available in the hospitals of 194 (71.3%) oncologists (Q16). Most commonly treated type of HNC was NPC as reported by 177 (65.1%) of the oncologists (Q20). The detailed demographic characteristics are present in Table 1.

Geographical distribution of oncologists across China.
Demographic Characteristics.

Abbreviations: HNC, head and neck cancer; MDT, multidisciplinary team.
Departments of Treatment
The departments for treatment were broadly categorized into 3 departments, namely RT, oncology, and surgery. Figure 2A depicts the department in which best treatment is present for LA HNC and r/m HNC and departments in which most likely treatment is provided for both LA HNC and r/m HNC in the Chinese hospitals (Q19, Q25, Q45, Q46). Figure 2B shows the department at which the patients with HNC come in their first visit, which showed 78% oncologists reporting that patients approaching head and neck surgery department at the first visit (Q26).

Major departments of treatment. A, Treatment departments. B, Department for first visit of patients with HNC. HNC indicates head and neck cancer
Phase and Status of the Patients With HNC on the First Visit
To know the phase and status of patients with HNC in the first visit, oncologists were asked 2 questions. In response to the question (Q30), on phase of patients with HNC, 78.3% responded that the patients were on locally advanced stage, followed by 11.8% for relapsed stage and only 9.9% for early stage. Regarding the status of the patients with HNC, 52.6% of the oncologists reported that the patients were in locally inoperable stage, whereas 18% were for late surgery stage, 16.5% for early surgery stage, and 12.9% were at relapsed stage.
Head and Neck Cancer Diagnosis and Prognosis
Questions related to HPV and EGFR testing for diagnosis and prognosis purpose were asked to the oncologists. Approximately 49% and 67.3% oncologists, respectively, agreed that EGFR (Q31) and HPV testing (Q27) should be performed on treated patients with HNC to know the treatment efficacy. Method followed for HPV detection was primarily polymerase chain reaction (PCR) technique as reported by 62.1% of the oncologists (Q12). Human papillomavirus test for prognosis should be considered on patients with HNC, which was agreed by 72% of oncologists (Q9). However, 40.8% of the oncologists believed that there was no effect on the treatment decision and thus would not prefer HPV testing (Q21). Prognosis in patients aged >75 years was considered worse than patients aged <65 years by 65.1% of oncologists, and treatment is influenced by increasing age for HNC (Q14). The details are presented in Table 2. The prognosis parameters assessed were (Q15) adverse events (AEs)/severe AE, quality of life, disease prognosis, OS, and PFS, of which >73% oncologists had knowledge of Overall survival (OS) and progression free survival (PFS) which was relatively much higher than other parameters (Figure 3).

Outcomes of treatment.
Diagnosis and Prognosis.

Abbreviations: HNC, head and neck cancer; HPV, human papillomavirus.
First-Line Therapy for r/m HNC
The oncologists were asked 2 questions in this dimension discussing the first-line therapy for r/m HNC. In the first question (Q13), only first-line CT for r/m HNC was considered and 45.2% of the oncologists preferred TP regimen (taxane + cisplatin) as first-line CT for r/m HNC, followed by TPF regimen (taxane + cisplatin + 5-fluorouracil [5-FU]), PF regimen (cisplatin + 5-FU), and other CT and TF regimen (taxane + 5-FU). The second question (Q44) discussed the first-line therapy regimen for r/m HNC and 77.6% of oncologists preferred CT combined with anti-EGFR targeted therapy as the first-line therapy (Figure 4A and B).

Treatment regimen for recurrent metastatic HNC. A, First-line CT for r/m HNC. B, First-line therapy for r/m HNC. CT indicates chemotherapy; r/m HNC, recurrent/metastatic head and neck cancer.
Treatment Regimens, Management of HNC, and Toxicity Related to Treatment of LA HNC
Induction chemotherapy (ICT) for LA HNC to retain organ functions (Q10) and tumor shrinkage (Q33) in cases of large tumors was considered by 93% and 96% oncologists, respectively. A total of 72% of the total oncologists agreed for considering maintenance therapy after remission of first-line treatment (Q28; Table 3). In response to management of LA HNC, most of the oncologists preferred to consider ICT followed by CRT or ICT followed by RT combined with anti-EGFR targeted therapy (Q35; Figure 5A). The preferable CT regimen prescribed by oncologists for patients with LA HNC who chose CRT (Q34) was cisplatin (100 mg/m2) followed by cisplatin (75-80 mg/m2 every 3 weeks [Q3W]; Figure 5B). The most preferable therapy prescribed by oncologists for patients who were economically strong was CT (TPF) combined with anti-EGFR targeted therapy (Q17; Figure 5C). Among patients with LA HNC who were not able to tolerate cisplatin (100 mg/m2), some of the oncologists preferred low-dose cisplatin combined with RT and others preferred anti-EGFR-targeted therapy combined with RT or CT (Q37; Figure 5D).
Management of LA HNC With Induction Chemotherapy.

Abbreviations: LA HNC, locally advanced head and neck cancer.
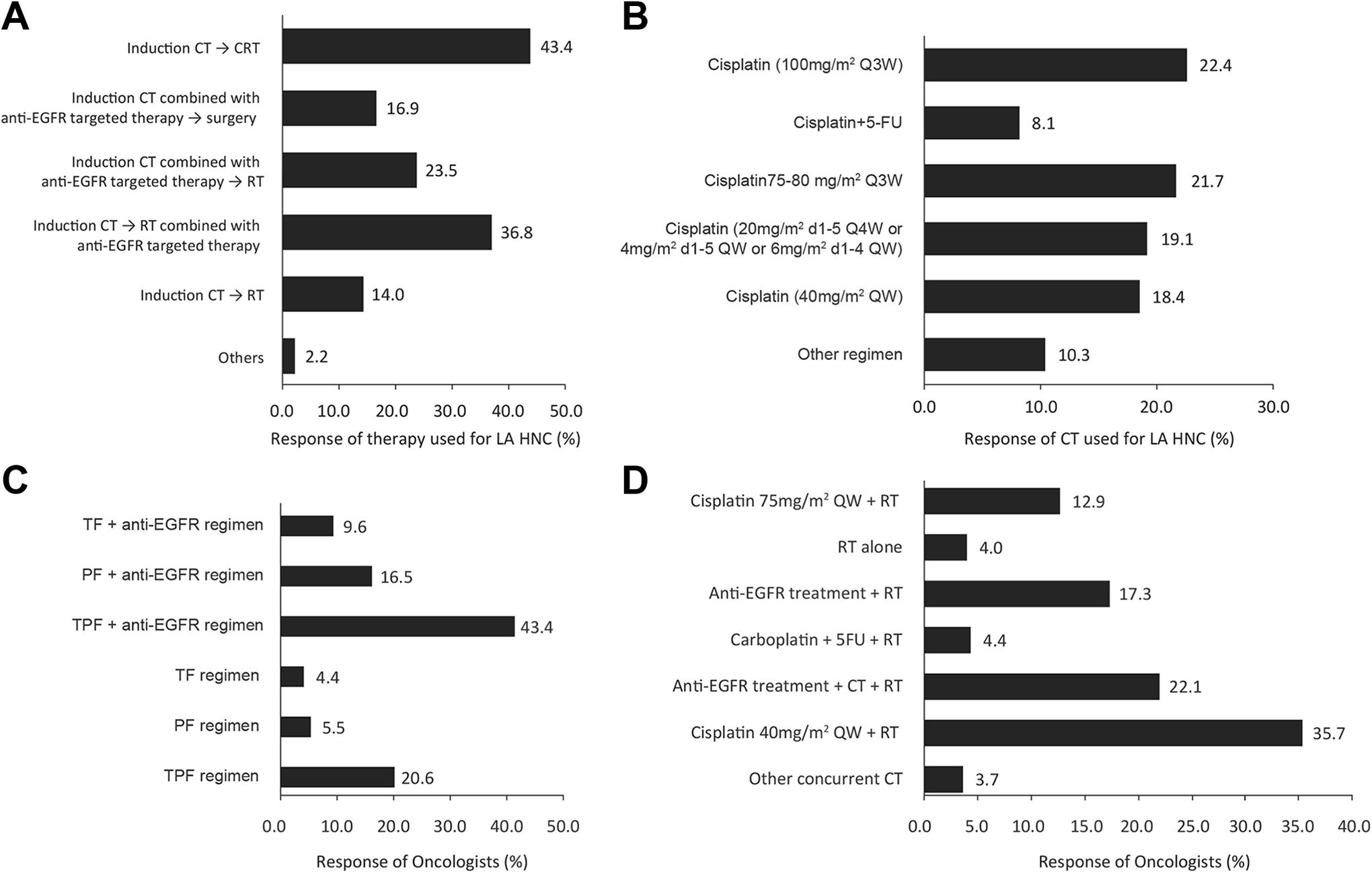
Management of LA HNC. A, Management of LA HNC with ICT. B, Preferable CT regimen for LA HNC who choose CRT. C, Preferable therapy for patients with LA HNC with permittable economic conditions. D, Preference of treatment for LA HNC if cisplatin (100 mg/m2 every 3 weeks) is intolerable. CRT indicates chemoradiotherapy; CT, chemotherapy; ICT, induction chemotherapy; LA HNC, locally advanced head and neck cancer.
According to 90.1% of oncologists, patients with renal dysfunction were considered unsuitable for prescription of high-dose cisplatin (100 mg/m2, Q3W), with 73.2%, 65.4%, 52.9%, and 49.6% oncologists considering age >70 years, Eastern Cooperative Oncology Group (ECOG) Perfornamace Status ≥2, cardiopulmonary dysfunction, and hearing loss as factors for unsuitability of high-dose cisplatin (Q40). The major concerns for ICT included were AEs and inaccurate effect related to ICT (Q39). In addition to these, poor economic condition of patients to be treated with ICT was considered a concern by 41.2% of the surveyed oncologists (Q39). The responses for concern for using ICT are presented in Table 3.
In response to the similarity of efficacy for low-dose (40 mg/m2 QW or 20 mg/m2 d1-d5 Q4W or 6 mg/m2 d1-4 QW, etc) weekly cisplatin + RT and high-dose cisplatin (75-100 mg/m2, Q3W) + RT regimen, 8.5% of oncologists strongly agreed and 51.5% agreed that both these regimens were similar in efficacy, while 29.8% were not sure, 9.6% disagreed, and 0.7% strongly disagreed for the similarity between the 2 management strategies (Q36). In response to the similarity in toxicity of the above regimens, 7.4% strongly agreed and 36.4% agreed that the toxicity levels for both the regimens are similar, while 27.2% were not sure, 27.2% disagreed, and 1.8% strongly disagreed for the similarity in toxicity for both the regimens (Q38).
Targeted Therapy
The dimension under the targeted therapy covered questions related to advanced targeted therapy for LA HNC and r/m HNC. Of all, 83.4% of oncologists considered targeted therapy for first-line therapy in case of r/m HNC (Q18) and 71.7% of the oncologists chose cetuximab as the preferred targeted therapy agent for r/m HNC (Q22). Anti-EGFR targeted therapy was considered by 84.2% of the oncologists for LA HNC (Q43). In the response to management with targeted therapy for LA HNC, 39% of oncologists preferred to use combination therapy of anti-EGFR with RT and CT (Q42); 41.5% oncologists reported considering PD-1/PD-L1 immunotherapies as third or later treatment lines, if permitted (Q23). Responses are summarized in Table 4.
Targeted Therapy.

Abbreviations: CT, chemotherapy; CRT, chemoradiotherapy; EGFR, epidermal growth factor receptor; HNC, head and neck cancer; ICT, induction chemotherapy; LA, locally advanced; r/m HNC, recurrent/metastatic; RT, radiotherapy; PD-1, Programmed cell death-1; PD-L1, Programmed cell death ligand 1.
Discussion
The present questionnaire-based survey among the oncologists across China on the management of HNC showed that the questionnaire is reliable and valid on the basis of Cronbach α measure, KMO measure of sampling adequacy, and Bartlett test of sphericity. The main treatment objective stated by the respondents was to provide best efficacious therapy with less AEs for patients with HNC keeping in consideration of the characteristics such as age, comorbid conditions, tolerability, and economic condition.
The present survey included majority of the hospitals from southeastern China including Guangdong province. Among the different types of HNC, NPC was the most responded type of HNC being treated by the included oncologists. This may be due to higher numbers of oncologists from Guangdong province, which has been reported to have higher prevalence of NPC in earlier epidemiological studies. 4,5
Majority of the oncologists were from RT and oncology departments associated with tertiary care hospitals which had MDT to treat HNC and had ongoing multicenter clinical trial on HNC. Oncologists included were attending physicians, associate chief physician, and chief physician having good number of years of experience ranging from 5 to 20 years. Approximately, 90% of the oncologists were interested to participate in clinical trials and were involved in some or the other activities for the benefits of patients with HNC such as regular follow-up, health education, and disease surveillance. Reflected from the above results, a majority had elaborately opined that various facilities such as separate and special departments are required for treating patients with HNC, even while working closely with MDTs. Chinese Expert Consensus recommends an MDT for treating HNC. 1 An MDT is a board of experts who may come together in a common platform to discuss any disease or a case for better clinical solution. An MDT for discussing HNC generally includes departments of ear, nose, and throat, oral maxillofacial and head and neck surgery, radiation therapy, medical oncology, pathology, and radiology. 22,23 In addition to better facilities in the hospitals, respondents included from the hospitals were experienced oncologists who were willing to keep themselves updated by participating in clinical trials and also benefit the patients with HNC by running different activities for patients cause.
In the present survey, we observed that Chinese oncologists in majority of the hospitals generally managed their patients with HNC in accordance to the National Comprehensive Cancer Network (NCCN) guidelines and the Chinese Expert Consensus. 1,24,25 As per the 2018 NCCN guidelines, concurrent cisplatin and RT or Cisplatin-based ICT followed by RT should be considered as the first-line therapy for LA HNC. Additionally, ICT cetuximab or carboplatin is recommended to be used along with RT for better OS and PFS outcomes in LA HNC. 25 Anti-EGFR-targeted molecule cetuximab showed an overall increase in the OS and PFS when combined with RT compared to RT alone, without increasing the local toxicities in a large, multinational randomized clinical trial on patients with LA HNC. 26 Another clinical trial on the same lines showed that cetuximab combined with RT improved the 5-year OS compare to RT alone. Additionally, a better survival rate was also observed among patients with LA HNC who experienced cetuximab-induced rash of grade 2 or above compared to the patients with no or grade 1 rash. 27 Responses from our survey revealed that the majority of the oncologists treated the patients according to the prescribed guidelines for LA HNC. Few oncologists deviated from the guidelines which may be due to idiosyncratic reasons, choice of treatment by the patients, and poor economic condition of patients. Most of the oncologists preferred ICT followed by concurrent chemoradiation (Figure 5A). It implies that most of the oncologists managing LA HNC in China are completely aware of the current standard guidelines and a rational approach is being made for the treatment; however, only few of the oncologists did not follow the guidelines which may be due to various reasons such as patients unable to tolerate the therapy leading to serious AEs and discontinuation of therapy.
The recommended guidelines for the first-line therapy of r/m HNC consists of taxanes/cisplatin/5-FU combined with cetuximab. 1,24 In accordance with the guidelines, we also observed that majority of the oncologists preferred CT (mainly TP/TPF regimen) combined with anti-EGFR-targeted therapy (primarily cetuximab), suggesting that the oncologists managed the patients under r/m HNC according to the recommended guidelines. A randomized clinical trial investigated the efficacy of cetuximab combined with PF regimen CT as first-line therapy in patients with r/m HNC and showed an improved OS compared to PF regimen CT alone. 28 A phase III randomized trial by the ECOG revealed that addition of cetuximab to CT regimen improved the response rate, increased the survival rate, and caused moderate increase in OS and PFS compared to CT alone in patients with r/m HNC alongside causing AEs such as cetuximab induced rash. 29 The NCCN guidelines 2017 also recommends targeted molecules such as afatinib and PD-1/PD-L1 as second line or later treatment lines for r/m HNC. 24 In the present survey, we observed that few oncologists used afatinib and were willing to use PD-1/PD-L1 as second-line treatment for r/m HNC if permitted. This observation is indicative of high level of awareness for treatment options among the oncologists in China for the management of HNC.
The 2017 Spanish Society of Medical Oncology guidelines for HNC and 2013 Chinese Expert Consensus have recommended to consider ICT for retaining the organ functions and tumor shrinkage for larger tumors in LA HNC. 30 Similarly, in our survey, approximately 95% of the oncologists considered ICT for retaining the organ functions and tumor shrinkage in patients with LA HNC. Thus, it may be inferred that the oncologists included in our survey followed the prescribed guidelines for treating patients with HNC.
Human papillomavirus infection is a recognized causal factor associated with HNC, 31 but its prevalence in Chinese population is relatively low. 1 In the latest NCCN guidelines, HPV test is strongly recommended in HNC and specially in oropharyngeal cancers. 24 In the present survey, majority of the oncologists responded with positive answers when questioned for HPV testing on treated patients with HNC and agreed that HPV testing should be performed for risk factors and as a prognostic marker. However, there were few oncologists who did not agreed with the guidelines and gave reasons like “Chinese people have low incidence of HPV,” “no effect on treatment decisions,” “patient refusal,” and “immature technical conditions to test HPV.” The hospitals used mainly PCR technique followed by fluorescence in situ hybridization and p16 IHC techniques to detect the HPV among the patients with HNC, which is in accordance to the latest guidelines of NCCN. 24 These findings imply that although HPV prevalence is low in the China, oncologists are following the guidelines of NCCN and only few oncologists don’t follow this, which may be due to personal assumptions or other reason mentioned above. An Italian survey on HPV among oncologists revealed that most of them were aware of HPV related to cancer, especially oropharyngeal cancer, and had a positive attitude toward HPV vaccination. 31 Another survey in HPV screening and use on US oncologists revealed that only half of the respondents used HPV for screening and even less than 15% used the reports in direct care for oropharyngeal cancers. 32 A study assessing the knowledge, attitudes, and beliefs of head and neck surgeons regarding HPV education and vaccination through a questionnaire based-survey found that majority of the surgeons were aware about HPV and showed positive attitude for HPV education and vaccination to treat HNC efficiently. 33
Age has a negative impact on prognosis of HNC. 2 It is also regarded as an independent predictor of outcome, morbidity, and mortality due to decreased cardiac output, impaired renal blood flow, along with reduction in pulmonary function with advancing age. 34 In addition to this, elderly patients are less resistant to postoperative infections due to the progressive impairment of the immune system. 34 In our survey, majority of the oncologists agreed that patients with age >75 years have worse prognosis for HNC compared to patients below 65 years age. Thus, our respondents reported in line with the previous literatures and implies that a rational approach is being followed to treat elderly patients with HNC. This fact is supported by the response of another question which asked for treatment influence on patients with age >70 years. Majority of the respondents supported for change in treatment line for elderly patients with HNC. Earlier studies have suggested that elderly patients, although healthy, are less likely to receive standard treatment compared to younger patients despite observations that elderly patients may benefit from aggressive treatment despite CT toxicities and complex surgeries. 35 -38
There were few limitations in the survey. Firstly, smoking which is a major risk factor for HNC 2 was not included in the survey questionnaire as the questionnaire was not directly involved with patients. Secondly, there was no question related to therapy regimen on patients >70 years, since influence on treatment strategy was agreed by most of the oncologists for elderly patients with HNC. However, there are still no specific guidelines for the treatment of elderly patients with HNC. The third limitation was that the survey did not take into consideration the treatment practices according to oncologists’ experience as it could have added more to the strength of the study. The fourth limitation was that it was a one-time survey which may not reflect the changes in the trends of management. 39 And finally, the fifth limitation was that the study did not include any hospital/oncologist from the eastern, northern part of China, which would have added more to the treatment strategies followed by oncologists all across China.
Conclusion
The findings revealed that most Chinese oncologists recommended ICT with RT and targeted therapy for LA HNC and TPF regimen combined with targeted therapy for r/m HNC, which was in accordance with NCCN guidelines (2017 and 2018) and Chinese Expert Consensus 2013 for HNC management. Further research is warranted to establish the guidelines recommendation for targeted therapy and PD-1/PD-L1 for management for HNC.
Supplemental Material
Supplemental Material, Supplementary_Table - Management Practices of Head and Neck Cancer in Chinese Tertiary Care Hospitals: A Multicenter Questionnaire-Based Survey Among Oncologists
Supplemental Material, Supplementary_Table for Management Practices of Head and Neck Cancer in Chinese Tertiary Care Hospitals: A Multicenter Questionnaire-Based Survey Among Oncologists by Zhao Anwei, Sun Xin, Tang Qiao Fei, Jin Ziyu and Fa-Yu Liu in Cancer Control
Footnotes
Authors’ Note
A written consent was obtained from the oncologists participating in the survey for publication of the data, obtained from the survey. As the study did not directly involve any patients, in accordance to the International Conference on Harmonization (ICH) Good clinical practice (GCP) guidelines, ethics committee approval and informed consent from the patients were not sought. Z.A., S.X., and F.Y.L. performed the conception, design, and conduct of the study. T.Q.F. and J.Z. did the analysis and interpretation of the data. The drafting of the paper and revising it critically for intellectual content was performed by Z.A., S.X., and F.Y.L. Final approval of the version to be published was approved by all the authors and that all authors agree to be accountable for all aspects of the work. Zhao Anwei and Sun Xin contributed equally.
Acknowledgments
The authors thank Dr Md Ubedul Hoda and Mr Karan Sharma (Indegene Pvt Ltd, Bangalore, India) for providing necessary medical writing and technical assistance in the development of this manuscript, as funded by Merck Serono China, an affiliate of Merck KGaA, Darmstadt, Germany.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors declare that they received research funding from Merck Sereno Co Ltd, an affiliate of Merck KGaA, Darmstadt, Germany, to conduct the study. The authors state that they had full control of all primary data and agree to allow the journal to review their data if requested.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Merck Sereno Co. Ltd, an affiliate of Merck KGaA, Darmstadt, Germany.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.