
Abstract
Despite the growing elderly population, there is limited research specific to this demographic concerning breast reconstruction (BR). Lack of evidence-based BR recommendations in older populations may contribute to misconceptions and subsequent underutilization of BR, especially autologous BR. Patients who received either deep inferior epigastric perforator (DIEP) flap BR or tissue expander/implant (TE/I) BR by a single surgeon between July 2011 and July 2015 were surveyed postoperatively by using the psychometrically validated BREAST-Q questionnaire to determine patient satisfaction. Patients were categorized into younger and older cohorts based on median age (55 years) and further stratified based on the type of reconstruction. Of the 311 patients surveyed, 95 patients responded (31% response rate). Overall, younger patients (<55 years old, n = 42) compared with older patients (≥55 years old, n = 53) had significantly higher satisfaction with their outcome (mean difference [MD] 12.06; 95% confidence interval [CI]: 0.96-23.15; P = 0.034). In the TE/I group (n = 58), younger patients had significantly higher satisfaction with breasts (MD: 14.17; 95% CI: 2.58-25.75; P = .017) and outcome (MD: 18.25; 95% CI: 3.95-32.5; P = .010) with fewer complications (odds ratio [OR]: 3.29; 95% CI: 1.37-7.86; P = .010). In the DIEP flap group (n = 55), there was no significant difference inr any of the satisfaction outcomes between younger and older patients. Younger patients tend to be more satisfied and demonstrate fewer complications with implant-based BR. In contrast, both younger and older patients undergoing abdominally based autologous BR were equally satisfied with comparable outcomes.
Keywords
Introduction
In today’s evolving health-care system, patient reported outcomes (PROs) have considerable potential in the determination of surgical quality. In an era of patient-centered care, there is increased recognition among surgeons that many postoperative outcomes are best measured by the patient. 1 Currently, PROs play an important role in the planning of comparative effectiveness research and are used as primary outcomes in surgical trials. 2 With the Patient Protection and Affordable Care Act, new payment models such as the meaningful use and physician quality and reporting system encourages patient-reported data collection in surgery and targets funding of research from the patient-centered outcomes research Institute. 3 Thus, the evaluation of postoperative patient satisfaction with breast reconstruction is an important quality measure in breast cancer care, 4,5 and it plays a key role in determining patients’ and payers’ choices of services and providers. Furthermore, the various techniques available for breast reconstruction make choosing the “right” procedure daunting. Outcomes research can provide patients with objective, reliable information to assist in reconstructive decision-making. Thusly, understanding the impact of these procedures is important to delivering patient-centered care and health policy leaders’ decisions about appropriate allocation of health-care resources for reconstructive surgery. 6
Despite the growing elderly population, there is very limited research specific to this demographic in regard to breast reconstruction. Although the majority of women diagnosed with breast cancer are over the age of 55, rates of postmastectomy breast reconstruction (BR) performed for this age-group are but one-sixth that of younger cohorts. 7 -9 A pooled review of 32 studies reported 24 746 cases of BR in 407 570 mastectomy patients aged 60 years or older, corresponding to a pooled BR rate of only 6.1%. 7 With advances in screening, detection, and treatment, mortality from breast cancer has decreased in the last 3 decades. 10 With older patients having improved survival and longer lives after the breast cancer diagnosis, a stronger emphasis must be placed on improving their quality of life (QOL). Postmastectomy BR is an important component of doing so as studies have consistently shown improved breast-related QOL outcomes in patients that undergo reconstruction compared to those that do not. 8,11 -16
A recent 2016 systematic review showed that the studies comparing overall complication rates from BR between older and younger cohorts found no significant difference between the 2 groups. 7,11,17 -20 The review was unable to link the rates of complication to the type of reconstruction due to the lack of data provided by most of the included studies. 7 Only 4 studies in the review investigated the QOL and satisfaction of older patients using PROs of BR. These patients had significantly better scores in breast-related body image and breast-related psychosocial health compared to age-matched controls and mastectomy-only patients and did not differ significantly on such measures from their younger counterparts. 7,8,21 These studies also could not distinguish satisfaction between the various BR modalities.
Now that studies have demonstrated the equivalent benefit and similar complication rate of autologous BR in older and younger patients, additional questions arise concerning the relationship between PROs, age, and specific types of BR.
Although studies have looked at PROs in autologous versus alloplastic reconstruction, these studies failed to factor in age. 22 -24 Our study aims to answer this question by comparing PROs and complications between younger (<55 years old) and older (≥55 years old) patients who have undergone deep inferior epigastric perforator (DIEP) flap and tissue expander/implant (TE/I)-based BR.
Methods
Women who underwent BR by a single surgeon between July 2011 and July 2015 were identified using operative case logs. Following institutional review board approval, data were gathered from a retrospective chart review including patient demographics, type of reconstruction, and complications. All women were patients at H. Lee Moffitt Cancer Center and Research Institute, a National Comprehensive Cancer Center, under the care of the senior author.
Patients were categorized into younger and older cohorts based on median age (55 years) and subsequently stratified based of the type of reconstruction: DIEP-free flap or tissue expander to implant (TE/I) BR. In the TE/I group, patients who underwent nipple-sparing mastectomy, delayed reconstruction, radiation therapy, additional flap reconstruction, placement of acellular dermal matrix, and those with incomplete data were excluded. In the DIEP flap group, those with incomplete data were excluded.
A total of 311 patients were sent the BREAST-Q [BREAST-Q Reconstruction Module (Post Operative) 1.0] questionnaire postoperatively by mail and e-mail. Satisfaction scores were recorded on a scale of 0 to 100. The mean satisfaction scores between younger and older patients were compared and further stratified based on the type of BR. Complications were defined as dehiscence, infection, hematoma, full thickness skin loss, or flap loss requiring reoperation within 30 days.
Questionnaire
The BREAST-Q was developed according to international guidelines to specifically measure health-related QOL after different types of breast surgery and is independently validated. 25 -27 The reconstruction module used in this study measures health-related QOL and satisfaction after BR and is composed of 6 scales: (1) psychosocial well-being, (2) physical well-being, (3) sexual well-being, (4) satisfaction with breasts, (5) satisfaction with outcome, and (6) satisfaction with care.
Statistical Analysis
Satisfaction scores were analyzed using the independent samples t test and summarized as mean difference along with 95% confidence intervals (CIs). Association between categorical variables is summarized as odds ratio (OR) and 95% CI, and difference was assessed using fisher exact test. To adjust for multiple comparison, Bonferroni correction was applied. The significance level for all comparisons was set at 5% (P < .05). All analyses were performed using SPSS V22.0 statistical analysis software.
Results
Patient Demographics
Out of the 311 surveys distributed to BR patients, a total of 95 survey responses (31%) were received and included in our study. Patient responses collected ranged from 4 months to 6 years from their date of initial operation. The ages ranged from 23 to 82 years, with a median age of 55 years, and the mean body mass index was 27.8. A total of 33 (10.6%) patients experienced 1 or more complications. Out of these 33 patients, 9 complications were in patients under 55 years old (27%) and 24 complications were in patients 55 years and older (73%). Figure 1 illustrates the distribution schemata of our study.
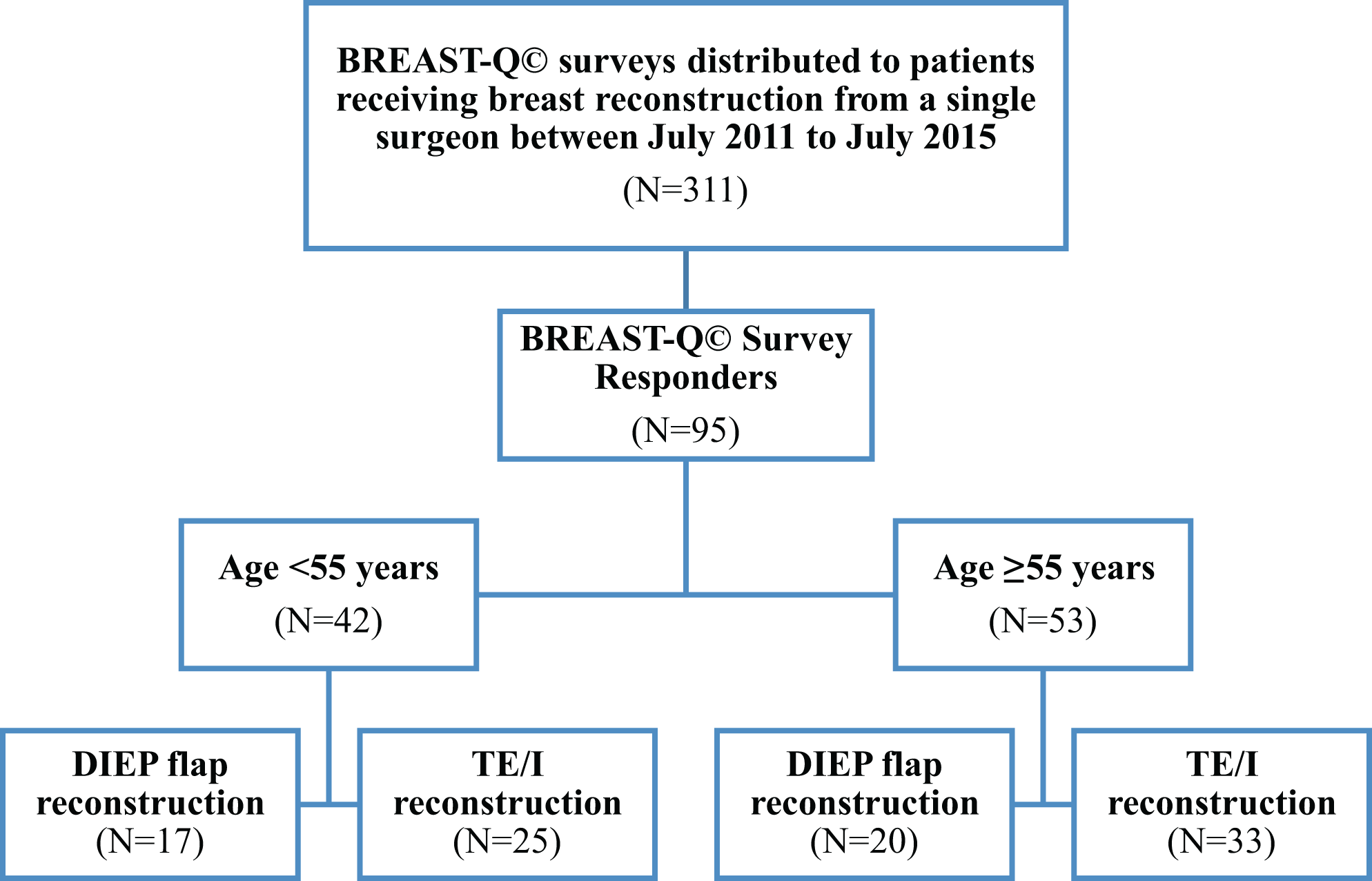
Patient distribution schemata.
Breast Reconstruction Mean Satisfaction Scores From BREAST-Q Survey
Mean satisfaction scores from the 6 domains of the BREAST-Q reconstruction module were grouped by age and BR procedure. These data are shown in Table 1.
Breast Reconstruction Mean Satisfaction Scores From the BREAST-Q Survey.

Abbreviations: BR, breast reconstruction; DIEP, deep inferior epigastric perforator; TE/I, tissue expander/implant.
Grouped BRs
Overall, younger patients (<55 years old) compared with older patients (≥55 years old) had significantly higher satisfaction with their outcome (mean difference [MD]: 12.06; 95% CI: 0.96-23.15; P = .034). This trend was consistent in the TE/I group (OR: 3.29; 95% CI: 1.37-7.86; P = .010) but not in the DIEP flap group (OR: 1.15; 95% CI: 0.07-18.79; P = .922). Mean satisfaction scores from both BR groups are shown in Figure 2.
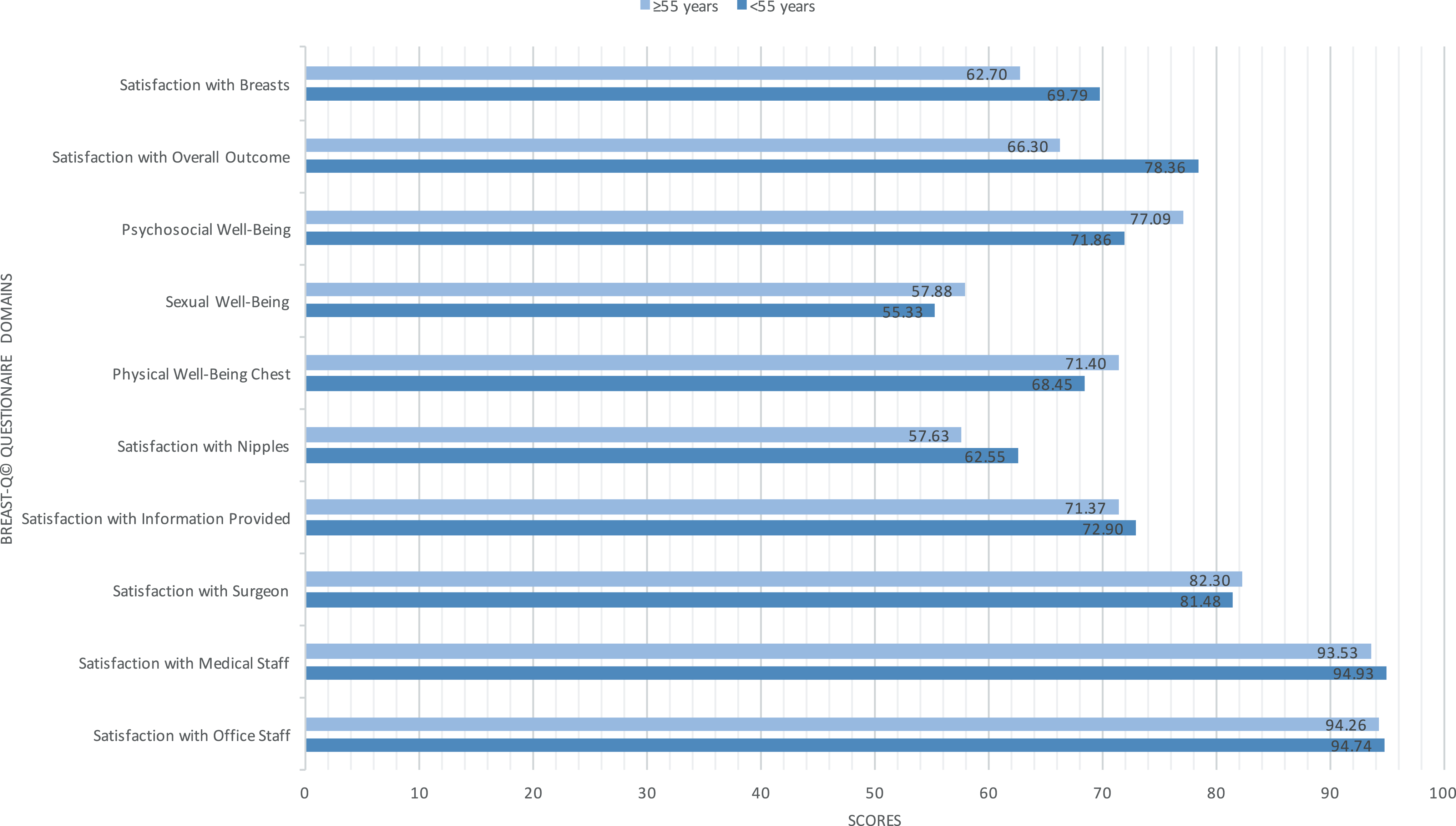
Grouped reconstructions mean satisfaction scores.
Tissue Expander/Implant BR
In the TE/I group, younger patients compared with older patients had significantly higher breast satisfaction (MD: 14.17; 95% CI: 2.58-25.75; P = .017) and satisfaction with overall outcome (MD: 18.25; 95% CI: 3.95-32.5; P = .010). Younger patients in this group also had fewer complications (OR: 3.29; 95% CI: 1.37-7.86; P = .010). Mean satisfaction scores from the TE/I group are shown in Figure 3.
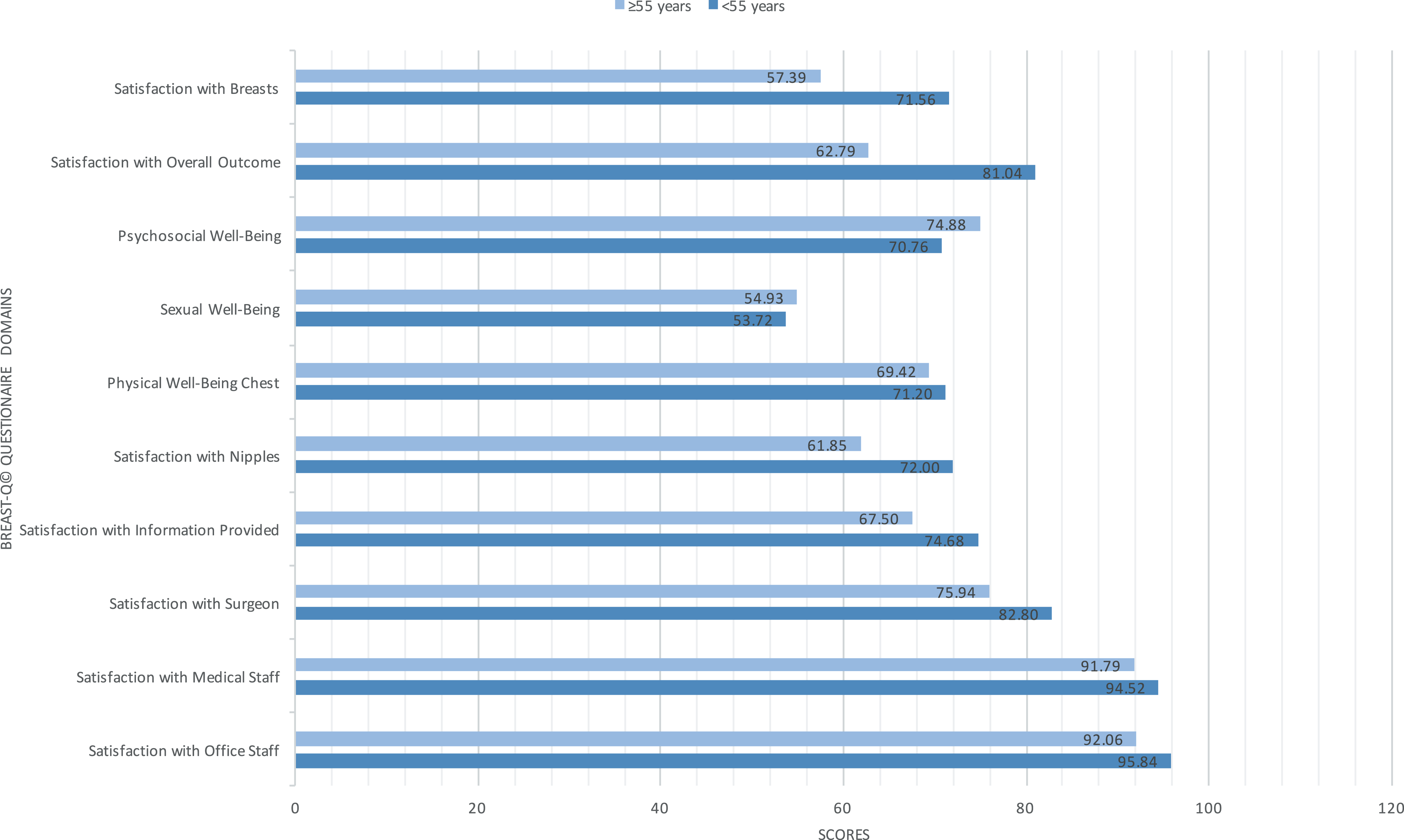
Tissue expander/implant reconstruction mean satisfaction scores.
Deep Inferior Epigastric Perforator Flap BR
In the DIEP flap group, older patients had higher satisfaction with breast, psychosocial well-being, sexual well-being, physical well-being for chest, satisfaction with information, satisfaction with surgeon and office staff. However, these differences were not statistically significant. There was also no significant difference in complication rates for the DIEP flap between younger and older patients. Mean satisfaction scores from the DIEP flap group are shown in Figure 4.
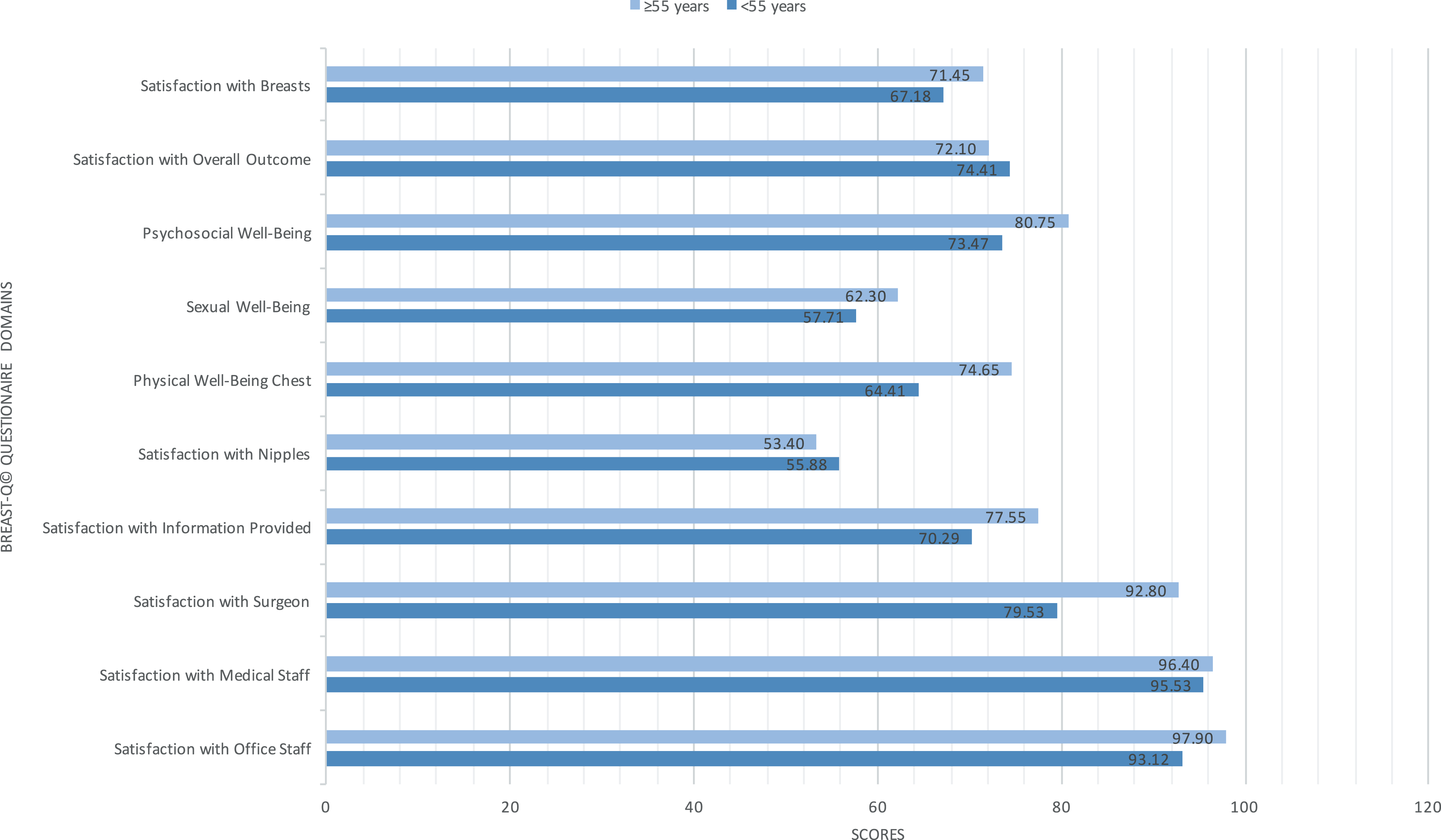
Deep inferior epigastric perforator (DIEP) flap reconstruction mean satisfaction scores.
Discussion
Lack of evidence-based recommendations for BR in older populations may partially explain their low rates of reconstruction and contribute to misconceptions about the operative risks and complications associated with autologous BR in this population. Of the limited number of BRs performed in older patients, implant-based reconstruction is the most common in the United States, despite higher complication rates reported in the elderly patients. 9,11,12,28 -33 Implant-based reconstruction may be more often performed based on assumptions that older patients will not tolerate the long anesthetic times that complex autologous reconstructions require and that such procedures will place greater physical demands on the patient and involve longer hospital stays than implant-based procedures. 11,33 This might then explain why women older than 65 years constitute only a lamentable 3% of autologous BR when they can benefit equally from such procedures.
Compiled data from multiple hospitals show that autologous reconstruction in the elderly patient has equivalent complications and satisfaction with both the procedure and QOL when compared to the younger cohort. 10 The rates of complications such as flap loss, fat necrosis, donor and breast site morbidity, wound healing, infection, and thromboembolic events (deep venous thrombosis or pulmonary embolism) were equally low for autologous reconstruction in older and younger patients and comparable to those found in the literature without age discrimination. 9,17,28 Recent evidence also found no association between age and a higher peri- and postoperative risk in autologous BR and that advanced age alone is not a predictor of poor outcomes after microvascular autologous BR 19 and microvascular flap reconstruction. 34 -37 A review of 6 studies by Walton et al 9 recommended that autologous reconstruction is a safe option that offered better outcomes as compared to implant-based reconstructions in older women, provided appropriate preoperative assessment was done. By a review of 44 papers, Hamnett et al 38 concluded better long-term outcomes with autologous reconstruction in this age-group, which correlated with improved survival and longevity of the reconstruction. A study by Ludolph et al 22 was the first to report the equivalent benefit of older patients undergoing autologous BR using the BREAST-Q questionnaire but did not assess age-related subjective outcomes in relation to autologous versus alloplastic BR. With such controversy over what type of BR should be performed for older women, our study aimed to elucidate some of these questions surrounding choosing the optimal BR modality for different age populations.
Our results showed that younger patients had significantly higher satisfaction with their overall outcome compared with older patients (P = .034). However, there were no significant differences with overall breast-related QOL measures between the 2 age cohorts, similar to the results found by other studies. 8,11 -16 There were also no statistically significant differences found in overall patient-reported satisfaction in any of the other BREAST-Q domains between the 2 age groups, a point that has been attested to by other studies the importance of considering BR in all ages. However, when stratifying for both age and type of reconstruction, our study showed differences in patient satisfaction between BR techniques that may be valuable when choosing the better tolerated modality.
In the TE/I group, younger patients compared with older patients had significantly higher breast satisfaction (P = .017) and satisfaction with outcome (P = .010), as well as fewer complications (P = .010). The increased satisfaction may reflect differences in the cohorts as younger women are often more likely to undergo bilateral reconstruction as well as nipple-sparing mastectomy, both of which have been associated with increased satisfaction. However, in this study patients who underwent nipple-sparing mastectomy were not included. Lipa et al 28 also described significantly higher rates of complication for implant-based reconstruction in patients aged over 65 years compared to patients of all ages (77% vs 37%), while complication rates for autologous reconstruction were similar between the 2 groups (35.3% vs 33.9%). A national audit of mastectomy and breast reconstruction 39 found implant-related complications to be higher in the elderly group than in the general population with the most common complication being infection, which required removal. Our results align with these past findings as we did find a significant difference in complication rates between older and younger patients in the TE/I group (P = .010), but this trend was not observed in the DIEP flap group.
In contrast, older patients showed higher satisfaction with DIEP flap reconstruction technique in almost all BREAST-Q domains, although not statistically significant. Previous studies found no significant difference in BREAST-Q satisfaction scores between younger and older patients for autologous BR, although these studies did not discriminate between the types of autologous methods that included the DIEP flap (DIEP), pedicled transverse rectus abdominus myocutaneous (pTRAM) flap, free TRAM, muscle-sparing free TRAM, and superior inferior epigastric perforator flap. 10,22,40 Interestingly, these previous studies also observed significant differences between the types of autologous BR performed in younger and older patients. A multicenter analysis of 1809 patients revealed that the DIEP flap the most often performed procedure in the younger cohort (37.5%), and pTRAM was the most common in the older cohort (46.6%). 10 Ludolph et al 22 also found a significant difference between using a DIEP and ms-TRAM flap with more ms-TRAM flaps performed in older patients (82%) compared to the younger group (59%), and Seidenstuecker et al 40 presented a rate of 41% of TRAM flaps in older patients as compared to 36% of younger patients. A suggestion has been put forth that these differences between autologous modalities performed in younger versus older patients might be explained by the surgeon’s belief that TRAM-based techniques are the more cautious approach and by the higher rate of previous operative abdominal procedures in the older group. 22 The results of our study hope to quell some of these concerns and establish that not only can the DIEP flap BR be successfully used in older patients with fewer complications experienced, but also it may even be the surgery of choice by this population.
Limitations
Limitations of our study include lack of baseline QOL data, low overall response rate, and variable time to follow up from initial surgery. The lack of baseline QOL data can make it difficult to know whether or not difference in preoperative satisfaction played in a role in the observed differences in our study. However, no significant differences in preoperative QOL between implant and autologous BR patients were found in previous studies. 41,42 In future studies, we plan to incorporate preoperative surveys with our prospective studies.
Postoperative follow-up time from initial surgery varied from 4 months to 6 years, since it was ad hoc as to when our research question was developed and executed. Previous outcomes-based studies have demonstrated variability in patient satisfaction depending on timing from completion of surgery. Additionally, certain patient and tumor characteristics were not included in this study such as symmetry procedures, radiation, chemotherapy, comorbidities, and so on, which could have influenced patient experience and, thus, satisfaction with outcome. Finally, the reasons for noncompletion of questionnaires were not specifically analyzed and this could be a potential source of bias in the study.
Conclusions
We have illustrated in our study that patient age influences PROs after different types of postmastectomy BR. When considering BR in older patients, autologous reconstruction techniques, such as the DIEP flap, may provide improved outcomes in terms of patient satisfaction when compared to implant-based reconstruction. The interplay between age and preoperative attitudes and expectations deserves to be explored further to understand the reasons behind these differences in satisfaction. Comprehensive preoperative information should be provided for both autogenous and autologous reconstruction so that patients can make a well-informed decision about their BR surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.