
Abstract
Background:
Pancreatic neuroendocrine tumors (PanNETs) constitute approximately 3% of pancreatic neoplasms. Like patients with pancreatic ductal adenocarcinoma (PDAC), some of these patients present with “borderline resectable disease.” For these patients, an optimal treatment approach is lacking. We report our institution’s experience with borderline resectable PanNETs using multimodality treatment.
Methods:
We identified patients with borderline resectable PanNETs who had received neoadjuvant therapy at our institution between 2000 and 2013. The definition of borderline resectability was based on National Comprehensive Cancer Network criteria for PDAC. Neoadjuvant regimen, radiographic response, pathologic response, surgical margins, nodal retrieval, number of positive nodes, and recurrence were documented. Statistics were descriptive.
Results:
Of 112 patients who underwent surgical resection for PanNETs during the study period, 23 received neoadjuvant therapy, 6 of whom met all inclusion criteria and had borderline resectable disease. These 6 patients received at least 1 cycle of temozolomide and capecitabine, with 3 also receiving radiation. All had radiographic evidence of treatment response. Four (67%) had negative-margin resections. Four patients had histologic evidence of a moderate response. Follow-up (3.0-4.3 years) indicated that all patients were alive, with 5/6 free of disease (1 patient with metastatic disease still on treatment without progression).
Conclusions:
A multimodality treatment strategy (neoadjuvant temozolomide and capecitabine ± radiation) can be successfully applied to patients with PanNETs who meet NCCN borderline resectable criteria for PDAC. To our knowledge, this is the first report of the use of a multimodality protocol in the treatment of patients with borderline resectable PanNETs.
Introduction
Pancreatic neuroendocrine tumors (PanNETs) are very rare malignant tumors. They have been reported to represent between 1% and 2% of all pancreatic neoplasms. 1 These tumors are the second most common neuroendocrine tumor sites, at 7% after gastrointestinal carcinoid. 2 The prognosis of patients with PanNETs is highly influenced by surgical resectability. Historically, for patients who present with resectable disease and undergo margin-negative surgical extirpation, the 5-year survival rate is greater than 60%. 3 -5 However, in patients who present with unresectable disease, this drops to less than 30%. 6 -9 A more recent single-institution study reported 5-year survival rates of 82% to 84% for resectable patients and only 40% to 69% for patients with unresectable disease, depending on the American Joint Commission on Cancer (AJCC) stage. 10 This compares to a 5-year survival rate of only 18% to 24% for patients with resectable adenocarcinoma of the pancreas and worse rates for unresectable disease. 11 Therefore, the ability to achieve complete surgical resection appears to confer a significant survival advantage.
The resectability of pancreatic tumors is influenced by tumor involvement of surrounding vessels such as the superior mesenteric vein, portal vein, gastroduodenal artery, hepatic artery, superior mesenteric artery, and distant metastases. Most tumors encroach on some of these vascular structures or are metastatic and are considered unresectable. However, there are some tumors with no distant metastases with only limited involvement of these vessels, and these are classified as borderline resectable. 12 There have been several studies that have reported favorable outcomes with neoadjuvant chemotherapy with or without radiation followed by complete surgical resection (R0) for borderline resectable pancreatic ductal adenocarcinoma (PDAC) compared to borderline resectable patients who did not undergo surgery. 13 -17 However, there have been no reports of a similar approach to the management of borderline resectable PanNETs, despite the fact that its prognosis is better than that of PDACs. Recently, we reported that the use of temozolomide and capecitabine in chemotherapy-naive patients with metastatic moderately or well-differentiated PanNETs resulted in a 70% objective response rate, with a median progression-free survival of 18 months. 18 We have an ongoing trial using multimodality neoadjuvant therapy for borderline resectable PDAC.
In light of these facts, we began using a multimodality approach to treat borderline resectable PanNETs. Borderline resectability for PanNETs was defined using the National Comprehensive Cancer Network (NCCN) criteria for borderline resectable PDAC. 19 We report our initial experience with this treatment approach.
Patients and Methods
Our institutional review board approved this study, and all patients included in our database gave written informed consent. We conducted a comprehensive review of our prospectively maintained database to identify all patients with PanNETs who had undergone surgery at our institution between 2000 and 2013. Inclusion criteria were patients with pathologically confirmed PanNETs who met the NCCN criteria for borderline PDAC and had no evidence of metastatic disease. In addition, the patients should have received neoadjuvant chemotherapy, with or without radiation. Patients were excluded if they had evidence of metastatic disease on preoperative clinical staging or did not meet the criteria for borderline disease as above.
The patient’s charts were reviewed to determine the reason for borderline resectability, the number of chemotherapy cycles received, and whether they received radiation and the doses received. Pre- and posttreatment computed tomography scans were reviewed, with responses measured and reported. Surgical reports were reviewed for the type of surgery, intraoperative margins, estimated blood loss, and complications. Postoperative complications were also evaluated and documented. Given the small patient numbers, statistics were descriptive.
Results
A total of 112 patients were identified who had undergone surgical resection for PanNETs at our institution. Upon further review, 89 of the patients presented with resectable disease and went straight for surgical resection. Twenty-three patients presented with disease unsuitable for primary resection due to either borderline resectability or metastatic disease. Of these 23 patients, 17 had metastatic disease. They underwent surgical resection of the primary tumor and cytoreduction of metastatic disease after neoadjuvant treatment. The remaining 6 patients had borderline disease and comprised the study population (Figure 1).
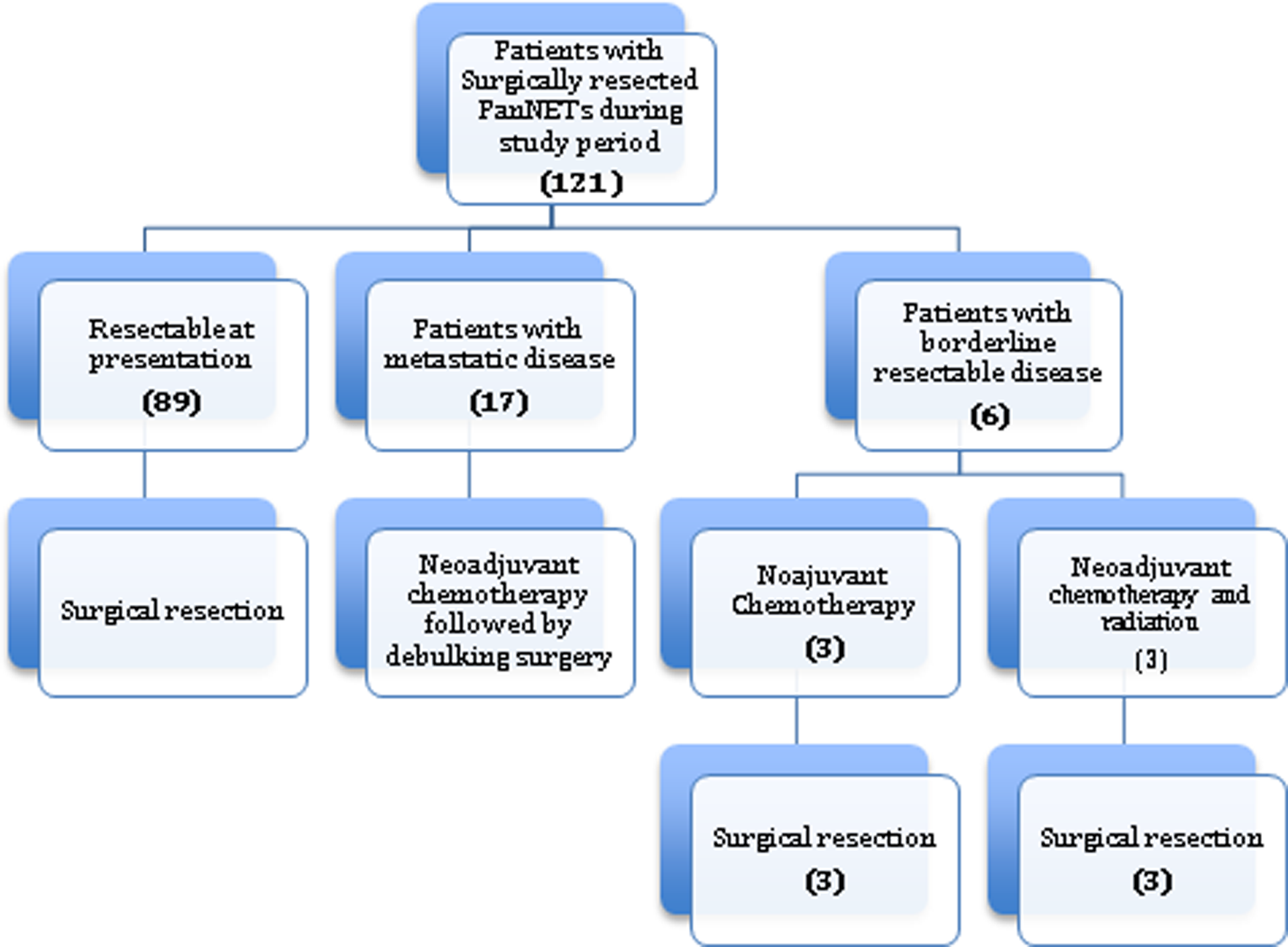
Study flow diagram.
The clinical and pathologic features of the patients are shown in Table 1. The mean age was 55 years, with a range of 24 to 70. The reasons for borderline resectability were portal vein, inferior vena cava, or superior mesenteric vein abutment in 5 patients. One patient had portal vein encasement along with abutment of the hepatic artery and superior mesenteric artery. All patients received at least 1 cycle of temozolomide and capecitabine (average number of cycles was 5; range of 1-15). Three patients received radiation in addition to chemotherapy. One received 50 Gy in 25 fractions along with infusional 5-fluorouracil. The second patient received 50 Gy over 25 fractions with concurrent capecitabine and a 4-Gy boost to the tumor. The third patient received 56 Gy in 28 fractions with temozolomide as a radiation sensitizer.
Clinical and Pathologic Features of the Patients.

Abbreviations: BMI, body mass index; NED, no evidence of disease; WHO, World Health Organization.
All patients had radiographic evidence of tumor regression after neoadjuvant treatment. In the case of 2 patients, the extent of regression amounted to a partial response by RECIST criteria, whereas the remaining had stable disease (Figure 2). An example of the radiographic response is shown in Figure 3. More importantly, all patients had sufficient tumor regression to receive successful resection of the primary tumor without vascular resection or reconstruction. Surgical margins were negative (R0 resection) in 4/6 patients (67%). In 2 patients, the margins were grossly negative, but pathologic evaluation was found to be positive (R1; retroperitoneal and portal veins, respectively).
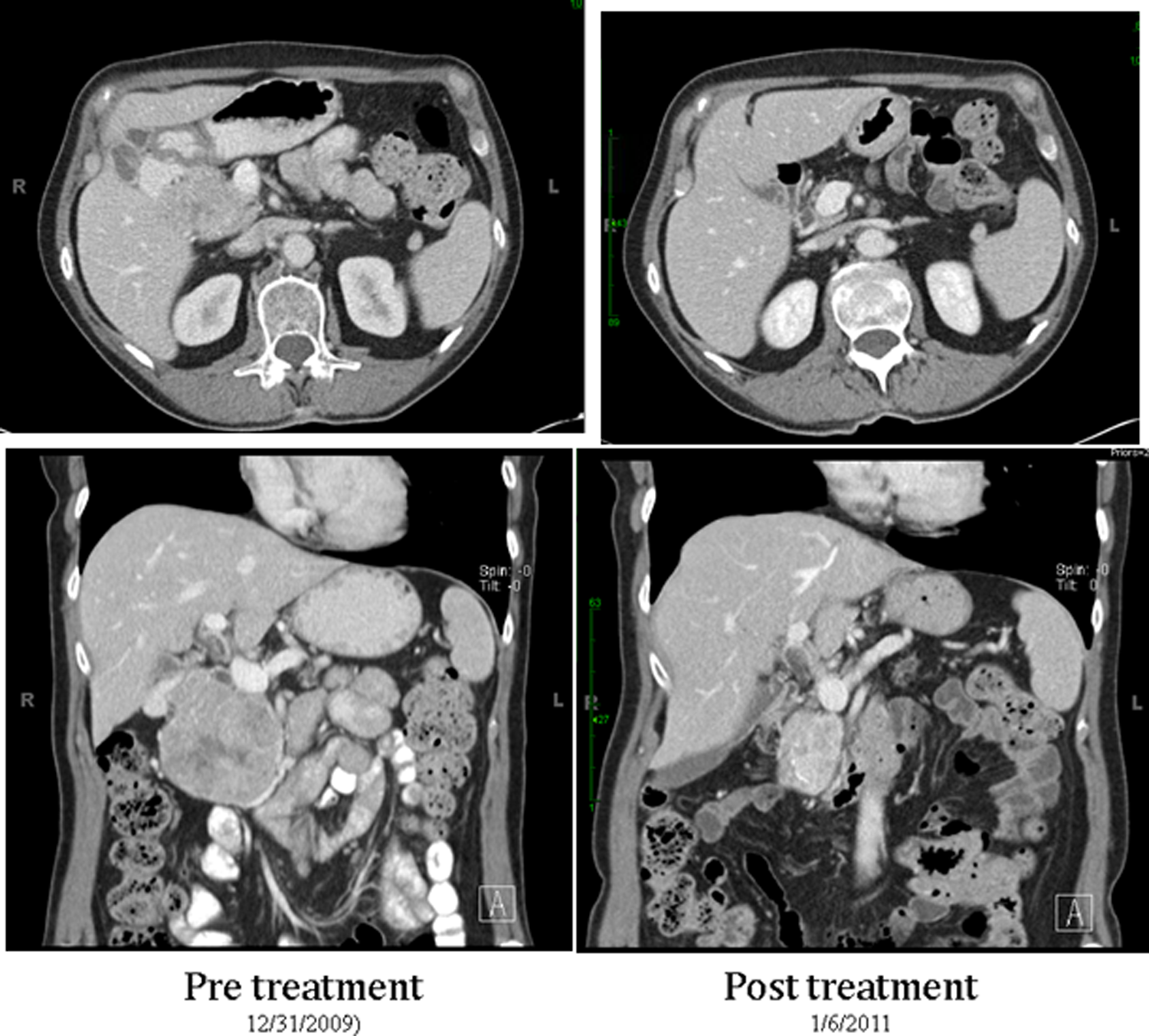
Example of tumor response.

Waterfall plot of response to neoadjuvant chemoradiation in 6 patients.
Surgical details and outcomes of the patients are shown in Table 2. Four patients had a Whipple procedure, and 2 had distal pancreatectomies, 1 with and 1 without splenectomy. The mean surgery duration was 442 minutes (range 254-517 minutes). The mean estimated blood loss was 375 mL (range 100-750 mL). Only 1 patient, who had an estimated blood loss of 750, received a blood transfusion in the perioperative period. The average length of stay was 17.5 days (range 6-45 days). None of the patients required vascular resection or reconstruction. There were no intraoperative complications or deaths. The 30-day morbidity rate was 67% (4/6 patients). Documented complications included a J-tube-site infection in 1 patient, type B pancreatic fistulae in 2 patients as well as a pulmonary embolus, portal vein thrombosis, and ascending cholangitis that occurred in the same patient.
Surgical Details of Patients.

Abbreviations: BL, borderline; DP, distal pancreatectomy; EBL, estimated blood loss; OR duration, operation time; IVC, inferior vena cava; PV, portal vein; SMV, superior mesenteric vein; SMA, superior mesenteric artery; SA, splenic artery; Abut, abutment; DVT, deep vein thrombosis; Encase, encasement.
Of note, there was 1 patient who had 12 miliary lesions in the liver on intraoperative ultrasound. Due to her age (24 years) and the lack of effective alternative treatment for her primary tumor, it was resected.
On pathologic review, 4/6 tumors were deemed to be well differentiated, grade 1 (low grade), and 2/6 were well differentiated, grade 2 (intermediate grade), based on the World Health Organization classification for neuroendocrine tumors. 20 Maximum tumor size ranged from 11 to 3.5 cm (mean 5.3 cm). Four patients had a Ki67 index of ≤2%. In the other 2 patients, the values were 4.6% and 15%. The median number of lymph nodes retrieved was 12. Half of the patients had no positive lymph nodes (0/26, 0/4, and 0/9, respectively). The other half had 1/1, 2/15, and 5/19 positive lymph nodes. The tumor response grade as determined by the College of American Pathologist criteria was 2 in 4 patients and 3 in the remaining 2. One patient demonstrated cellular effects of chemoradiation.
On last follow-up (range 36-52 months), 5/6 patients were alive with no evidence of disease, with none receiving any adjuvant therapy since surgery. Persistent disease in the liver was shown in the final patient at follow-up. She is receiving octreotide acetate and has had stable disease since surgery. Median progression-free survival has not been reached.
Discussion
Pancreatic neuroendocrine tumors are a relatively indolent malignancy especially when compared to their ductal adenocarcinoma counterpart. Although this speaks to the different biology of these tumors, surgical resection has been shown to affect survival in both cases. Complete surgical resection (R0) in PanNETs results in a 5-year survival rate of >60%, 3 -5 which drops to below 30% in patients who cannot have an R0 resection. 6 -9 Unfortunately, only 20% to 40% of patients diagnosed with PanNETs present with disease that is amendable to complete surgical extirpation. 21 -23 Recent developments in the surgical management of pancreatic adenocarcinoma have led to the identification of a group of patients deemed to have borderline resectable disease. 12 Several definitions have been proposed for this entity. 13,19,24 However, there is increasing consensus agreement on the definition advocated by the NCCN. 12,19 For this reason, we elected to use the NCCN definition. Several studies have reported improved survival in patients with borderline resectable pancreatic cancer who go on to have R0 resections after neoadjuvant chemotherapy with or without radiation compared to those who do not have surgery. 13 -17,25,26 One of the studies was performed at our institution, and we have an ongoing study for patients with borderline resectable pancreatic adenocarcinoma. 26 Indeed, conversion from borderline to resectable status allows for survival similar to that shown in patients who present with resectable disease and adenocarcinoma. Therefore, we rationalized that a similar approach to PanNETs using multimodality treatment might be reasonable.
We chose the combination of temozolomide and capecitabine because our previous work had shown that this regimen was highly effective for treatment of metastatic PanNET, resulting in an objective response rate of 70% and median progression-free survival of 18 months. 18 A literature search of PubMed using the key words pancreatic neuroendocrine therapy and neoadjuvant therapy revealed a case report that used a similar chemotherapy regimen in a patient who was found to have locally advanced disease at laparotomy for resection that was aborted. She received 8 cycles of chemotherapy after which she successfully had an R0 resection. 27 This provides support to the efficacy of the combination of capecitabine and temozolomide against PanNETs. It is noteworthy that 1 of the patients received only a single round of chemotherapy due to poor tolerance. She went on to receive 56 Gy of radiation with temozolomide as a sensitizer followed by surgical resection. Unfortunately, she was 1 of the patients with an R1 resection. However, the role of radiation is difficult to discern due to the limited number of patients.
In pancreatic adenocarcinoma, rates of conversion to resectability with neoadjuvant chemotherapy with or without radiation have been reported to be between 37% and 59%, with improved survival rates compared to patients who did not undergo surgery. 13,17,28 In our retrospective analyses, radiographic response did not meet RECIST criteria in most of our patients. However, in all patients, the response was sufficient to permit at least surgical resection, with no vascular resection or reconstruction. While pathologic evaluation did not demonstrate any case of complete response, all but 2 patients had negative margin resections (R0), while 2 patients had microscopically positive margins (R1).
To our knowledge, this is the first report of the use of a multimodality approach for the management of borderline resectable PanNETs. There is a possibility of selection bias based on the regional referral pattern. However, upon referral, all patients were discussed in a multidisciplinary tumor board and all who met borderline criteria were treated with the neoadjuvant approach. The retrospective nature of our study is an obvious weakness. We also do not have information on patients with borderline disease who received neoadjuvant treatment but did not undergo resection due to disease progression or other reasons. Unfortunately, in this rare malignancy, it is very difficult to accrue a large series of patients or to perform an adequately powered prospective randomized study.
Long-term follow-up and more clinical experience will be needed to study how these patients fare versus patients who present with resectable and metastatic PanNETs to determine whether this is an effective treatment strategy. In addition, this regimen may be effective in converting some patients with locally advanced disease to resectability.
In conclusion, neoadjuvant temozolomide and capecitabine ± radiation can be successfully used to treat patients with borderline resectable PanNETs with a high rate of R0 resections and no vascular resection, implying better patient outcomes. To our knowledge, this is the first report of the use of multimodality therapy (neoadjuvant chemotherapy ± chemoradiation and surgery) in the treatment of borderline resectable PanNETs.
Footnotes
Authors’ Note
No significant relationships exist between the authors and the companies/organizations whose products or services may be referenced in this article.
Acknowledgments
The authors thank Rasa Hamilton (Moffitt Cancer Center) for editorial assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.