
Abstract
Accurate screening for Internet Gaming Disorder (IGD) in children and adolescents remains a challenge in routine clinical settings. This study evaluated the psychometric properties and diagnostic utility of the Inclusion of Videogame in the Self (IVS) scale, a brief pictorial tool assessing the perceived fusion between self and video game. A clinical sample of 189 children and adolescents (M = 13.0 years, SD = 3.2) completed the IVS, IGD, and Social Media Disorder (SMD) measures. While the five-item scale showed a solid factor structure and reliability, diagnostic accuracy was limited. A single item assessing the “relationship” with the favorite game emerged as a strong screening proxy, correlating with IGD and minimally with SMD. A cutoff score of 3 or higher yielded 100% sensitivity and a 45% false-positive rate. The Single-Item IVS shows promise as a quick, developmentally appropriate screening tool to identify youth at risk for IGD, warranting further validation in broader samples. More generally, the IVS represents the first attempt to conceptualize inclusion of self with an object or activity (i.e., favorite game) rather than with a group or another person.
Since the inclusion of (Internet) Gaming Disorder (IGD) in the official clinical diagnostic classification systems ICD-11 (World Health Organization [WHO], 2024) and DSM-5 (American Psychiatric Association, 2013), the symptomatology has received increasing interest. IGD describes a pattern of playing digital games that has negative consequences on the individual’s personal, family, social, school, or other life domains and is characterized by a loss of control over gaming activities, increasing prioritization of gaming over other activities and continuing gaming despite these negative consequences (WHO, 2024). Especially children and adolescents represent a vulnerable group for IGD (Fineberg et al., 2022). Thus, it is crucial to identify individuals impacted by the disorder as early as possible.
To date, there is no gold standard in diagnosing IGD, but multiple well-established questionnaires exist (King et al., 2020). Some valid and reliable scales that can be used from adolescence onwards include the Internet Gaming Disorder Scale (IGDS; Lemmens et al., 2015), the Gaming Disorder Scale for Adolescents (GADIS-A; Paschke et al., 2020), the Video Game Dependency Scale (CSAS; Rehbein et al., 2015), or the Internet Gaming Disorder Scale–Short-Form (IGDS9-SF; Pontes & Griffiths, 2015), for example. For children, only very few scales exist: The CSAS (Rehbein et al., 2015) shows promising results via parental report in children aged 8 years and above (Kewitz et al., 2024). In addition, the Video Game Addiction Scale for Children (VASC; Yılmaz et al., 2017) can be used as self-report for 9- to 12-year-olds. An adjusted version of the CSAS in its parental report seems also helpful in identifying hazardous gaming in children (Kewitz et al., 2023). Hazardous gaming is a form of risky gaming behavior defined by different symptoms and a lower diagnostic threshold than IGD (WHO, 2023). Finally, the Digital Addiction Scale for Children (DASC; Hawi et al., 2019) enables assessment of the broader umbrella term Internet Addiction in 9- to 12-year-olds via self-report and the Increased Digital Media Use Questionnaire (IMDUQ; Wartberg et al., 2024) assesses increased digital media use in preschool children.
Despite the existence of valid and reliable scales, individuals at risk for IGD are often overlooked in outpatient clinical contacts (Kewitz et al., 2021) because IGD is often not systematically assessed. Especially in psychotherapy with children and adolescents, routine diagnostics require careful cost–benefit considerations. Developmental differences in language and cognition skills make questionnaire-based assessments more time-consuming than with adults. Thus, a more efficient screening tool could improve detection rates in routine care. For younger populations, simple screening tools using nonverbal cues and intuitive responses may offer a promising alternative.
The present approach is theoretically grounded in the concepts of Other-in-Self (Aron et al., 1992) and identity fusion (Swann et al., 2012). When individuals allow the boundaries of their self to permeate, they may feel their identity merge with another person (Aron et al., 1992) or group (Swann et al., 2012). This can be expressed as varying degrees of self-other overlap or inclusion, up to a complete sense of “being one.” High fusion would promote relational bonds, cooperation, and commitment, sometimes overly so (Aron et al., 1992). Clinical complications may arise when the immersion becomes inflexible (Harrison et al., 2022) or overly devotional (Whitehouse, 2018). To our knowledge, these concepts have never before been linked with behavioral addiction, neither empirically nor theoretically. In fact, to our knowledge, this is the first time that the concept of the Other-in-Self (Aron et al., 1992) has been linked not with another person but with an object or an activity.
Our aim was to capture the cognitive and behavioral preoccupation—core symptoms of IGD (American Psychiatric Association, 2013; WHO, 2024)—as language-independently as possible. In the context of intense gaming, players may develop a sense of identity fusion with their game or components of their games, such as in-game avatars or in-game teams/guilds. As they feel drawn to immerse themselves in the virtual environment and their role in it, gaming becomes an attractor, leading to IGD. Studies have already shown a consistent link between higher avatar identification and IGD—including research on adolescents (Lemenager et al., 2020; You et al., 2017; Zhang et al., 2024). Certain game features, such as complex and unpredictable reward systems, in-game purchases and rewarding in-game social alliances, may contribute further to this immersive effect (Rehbein et al., 2021).
Given this theoretical framework, a nonverbal, pictorial scale that tackles perceived closeness, interconnectedness, or feelings of fusion may be most sensitive to the motivational and affective characteristics underlying IGD. Screening for the disorder may, therefore, be most efficient with the Inclusion of Other-in-Self (IOS) scale (Aron et al., 1992), which has already been successfully applied in younger populations (Vezzali et al., 2016; Vyrastekova, 2021).
The IOS is a single-item scale where participants have to choose which Venn-like diagram best represents their relationship with another individual (see Figure 1). The underlying concept is that the closeness of a relationship can be represented by two circles with varying degrees of overlap. One circle represents oneself, and the second circle represents another person. Studies have shown that the IOS assesses the interconnectedness that one person has with the other (including feeling and behaving close; Aron et al., 1992; Gächter et al., 2015).
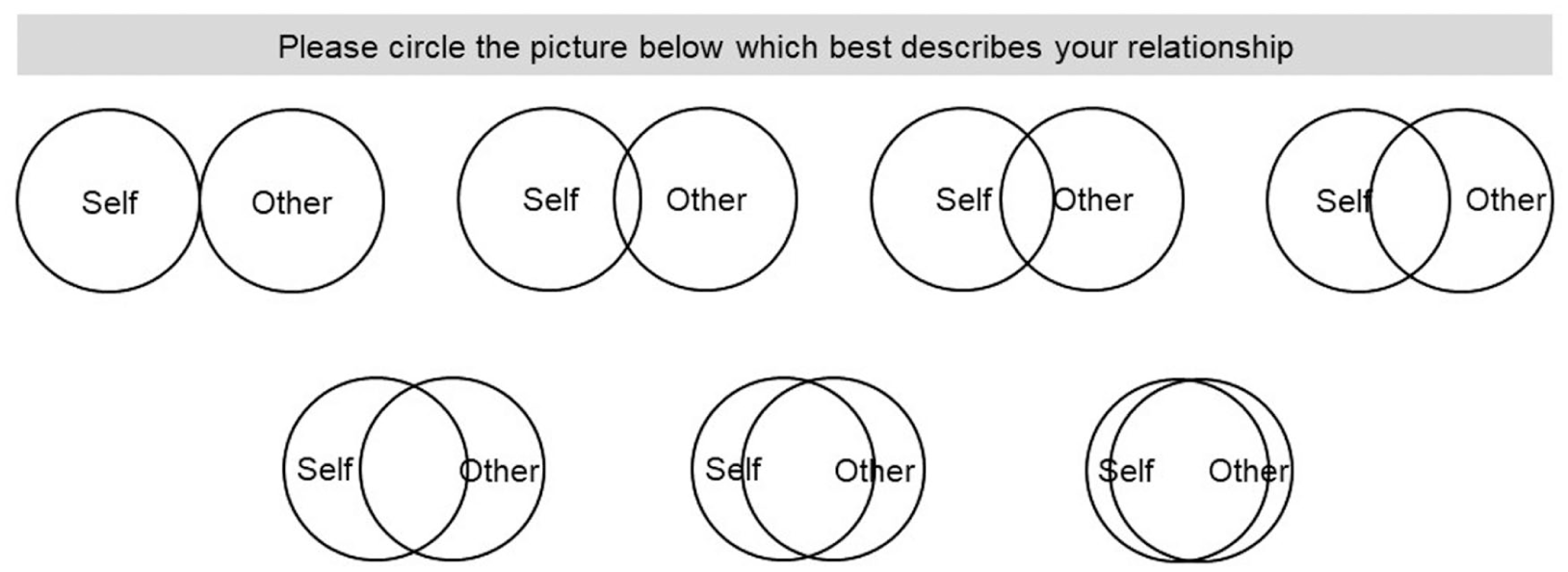
The Inclusion of Other-in-Self (IOS) Scale (Aron et al., 1992).
In addition, the IOS has been associated with mental health and (relational) well-being (Branand et al., 2019). The IOS scale has been applied in research on depression (Frick et al., 2021) and prolonged grief disorder (Harrison et al., 2022). In the context of the latter, it could be shown that patients feel more interconnected with the deceased person compared with healthy control individuals (Harrison et al., 2022). The scale also indicates empathy, altruism, selflessness, and cooperation in relation to (an)other/s (Cialdini et al., 1997; Gächter et al., 2015; Swann et al., 2010; Windmann et al., 2021). Retest reliability has been demonstrated to be r = .83 over a 2-week interval (Aron et al., 1992) while susceptibility to social desirability seems low (Aron et al., 1992; Gächter et al., 2015).
Prior research has demonstrated the applicability of the IOS in child and adolescent populations, supporting its developmental appropriateness. For instance, Vezzali et al. (2016) used the IOS with 7- to 9-year-old children to examine feelings of closeness with peers affected by the same natural disaster. Their findings indicated that children who perceived greater overlap with other affected peers reported stronger group identification and prosocial intentions, consistent with fusion-like processes. Similarly, Vyrastekova (2021) applied a parental version of the IOS in a sample of students aged 4 to 20 years with special educational needs, comparing perceptions of inclusion between regular and special schools; the results supported the IOS as a robust indicator of perceived social connectedness across age groups.
Together, these findings suggest that the IOS can reliably assess the perceived self–other overlap that underlies identity fusion and Other-in-Self dynamics. Consequently, this measure may offer a developmentally appropriate and theoretically grounded tool for screening for IGD-related processes in younger populations.
Here, we developed and evaluated a modified IOS scale called the Inclusion of Videogame in the Self (IVS) scale that tackles the degree of inclusion or fusion of a gamer with their favorite video game. Individuals were asked to indicate their perceived relationship with their favorite video game, as we expected a favorite video game to hold a special place in one’s identity. We focused on the favorite video game because we conceptualize a relationship as one with a specific entity (favorite video game) rather than with a general category (games in general)—analogous to human relationships, it reflects a bond with someone specific rather than with humankind in general. Focusing on a specific avatar (instead of a favorite video game), however, risked excluding players who play games without specific avatar identification.
We investigated whether this adjusted IOS scale can be used to reliably screen children and adolescents at risk of developing an IGD. We hypothesized that the IVS score would correlate positively and strongly with an established IGD scale. Since IGD and Social Media Disorder (SMD) are distinct but correlated constructs (Wartberg et al., 2020), we, in addition, hypothesized that the IVS would correlate positively but only weakly with an established SMD scale. This was done to assess the construct validity of the measure.
Method
Participants
Participants were patients from the child and adolescent psychotherapy outpatient clinic at Goethe University Frankfurt, Germany, who were undergoing outpatient treatment during the data collection period. The outpatient clinic is a general clinic treating all kinds of mental illnesses. Patients who completed the IVS questionnaire as part of their routine diagnostics were included in this study’s analyses. Since research findings suggest that understanding, reliability, and validity of health-related self-assessment increase after age 7 (Riley, 2004), the minimum age was set to 7 years.
IVS data were collected from a total of N = 263 individuals. After removing incomplete data sets and excluding participants outside the age range, N = 189 individuals remained. Thus, the final sample consisted of N = 189 participants aged between 7 and 18 years (M = 13.0, SD = 3.2). Of these, 54.5% were male, 42.3% female, and 1.1% nonbinary. The participants were from various educational backgrounds, including primary schools (11.0%), lower secondary schools (3.5%), intermediate secondary schools (5.2%), comprehensive schools (28.3%), and academic secondary schools (41.0%).
The participants in our study were gaming an average of M = 127 (SD = 134, n = 120) minutes per day, according to self-report and M = 122 (SD = 132, n = 130) minutes per day according to parental report. According to IGDS self-report, 11.4% (n = 12) of the participants in our study met the criteria for IGD. Considering parental report, 22.7% (n = 17) met the IGD criteria.
A detailed description of the participants’ demographic characteristics, divided by age group, is presented in Table 1.
Descriptive Data of Participants by Age Groups.
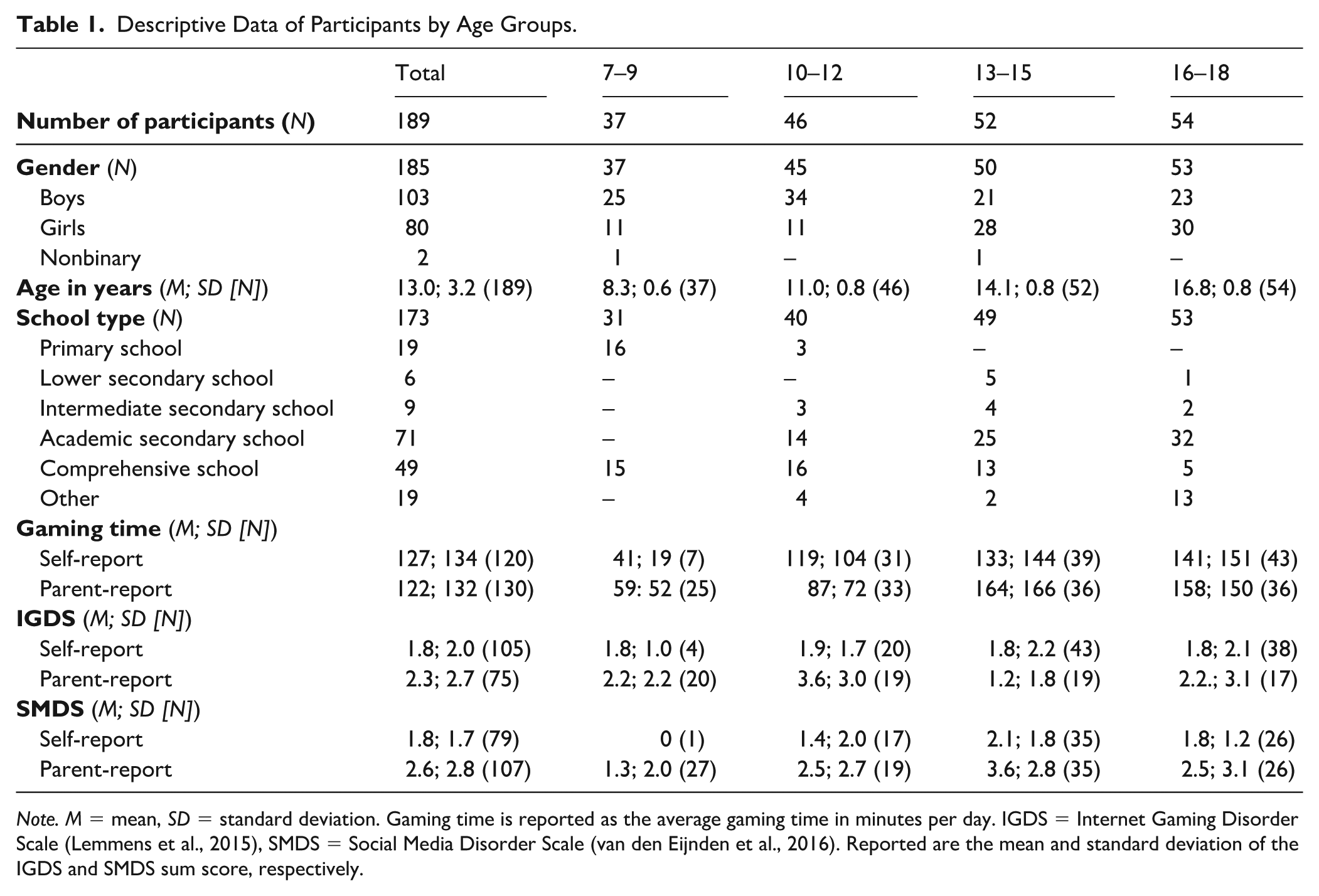
Note. M = mean, SD = standard deviation. Gaming time is reported as the average gaming time in minutes per day. IGDS = Internet Gaming Disorder Scale (Lemmens et al., 2015), SMDS = Social Media Disorder Scale (van den Eijnden et al., 2016). Reported are the mean and standard deviation of the IGDS and SMDS sum score, respectively.
Measures
Inclusion of Videogame in the Self
As the original IOS, the Inclusion of Videogame in the Self (IVS) reflects a 7-point scale (1–7) featuring Venn-like diagrams in which circles representing the “self” and the “video game” overlap to varying degrees. A large overlap of the two circles indicates a high level of game-gamer-inclusion (i.e., the cognitive and behavioral preoccupation; Aron et al., 1992) or fusion of gamer identity with the game (Swann et al., 2012). Figure 2 shows an example of the first item of the scale with the 7-point response scale. The complete questionnaire can be found in Supplemental Appendix A.
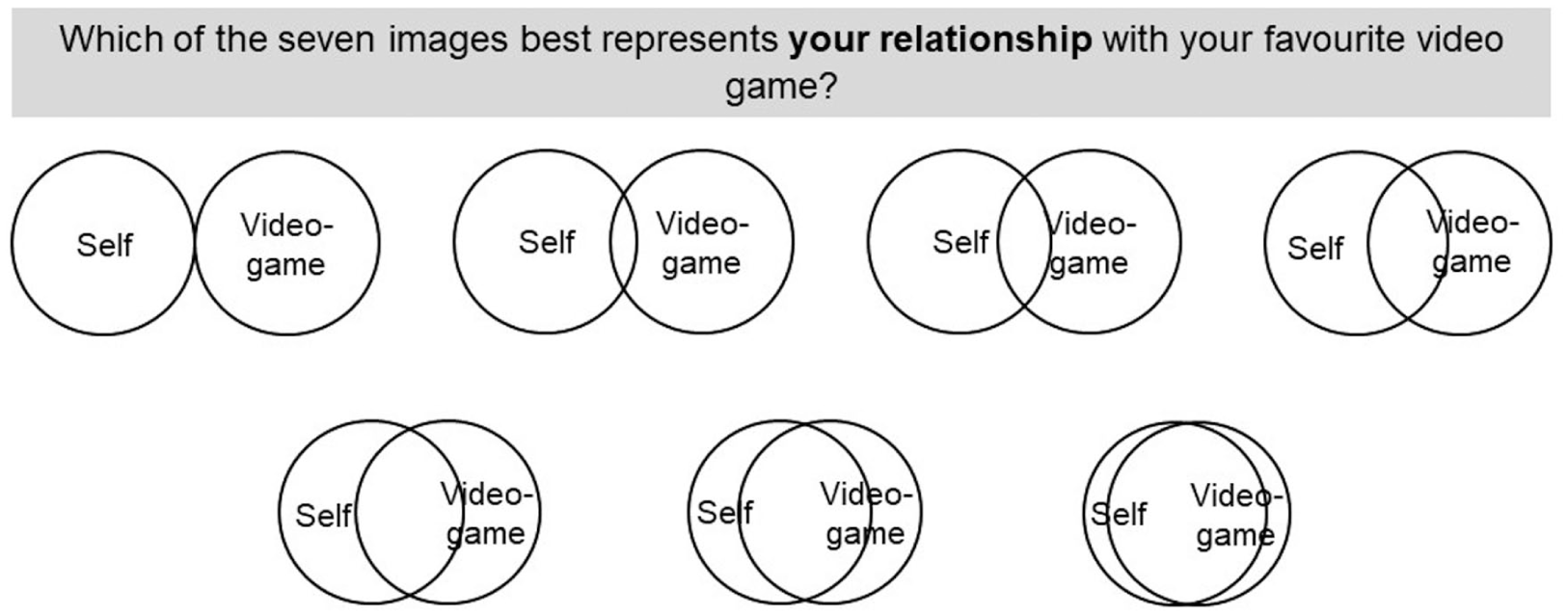
Item 1 of the Inclusion of Videogame in the Self (IVS) Scale.
In contrary to the IOS scale, we first tested five different items assessing the relationship between an individual’s favorite video game and the self at various psychological levels. Specifically, we took a cognitive-behavioral standpoint towards the idea of “fusion,” considering emotion, cognition, and behavior separately (Borg-Laufs, 2022). Hence, the items assessed (a) the individual’s relationship with the video game, (b) the relationship that the individual wishes to have with the video game, (c) the feeling the individual has towards the video game, (d) the thoughts the individual has about the video game, and (e) the time the individual wishes to spend with the video game.
To calculate the total IVS score, the values of all five items were summed up (range: 7–35; for information regarding scale consistency, see below).
Internet Gaming Disorder Scale
The assessment of IGD was conducted using the Internet Gaming Disorder Scale (IGDS) (Lemmens et al., 2015), a psychometric instrument based on the DSM-5 diagnostic criteria for IGD (American Psychiatric Association, 2013). It was administered as self- and parental report (P-IGDS; Wartberg et al., 2019). The self-report IGDS was filled in by n = 105 patients, while the parent-report version was filled in by n = 75. The IGDS consists of nine items, each corresponding to a specific symptom of IGD: preoccupation with gaming, withdrawal symptoms, tolerance, loss of control, diminished interest in other activities, excessive and persistent use despite negative consequences, deceptive behaviors, gaming as an escape from negative emotions, and functional impairment. Each item is rated using a binary response format (0 = no, 1 = yes), allowing for the calculation of a total sum score, with higher scores reflecting greater symptom severity. A cutoff score of 5 or more affirmative responses suggests a potential diagnosis of IGD. The scale has demonstrated strong psychometric properties, including a good internal consistency with Cronbach’s α = .83 (Lemmens et al., 2015) in the self-report version and a good internal consistency with KR20 of .86 in the parent-report version (Wartberg et al., 2019). In this study, the IGDS exhibited acceptable to good internal consistency (IGDS: Cronbach’s α = .76, McDonald’s ω = .74; P-IGDS: Cronbach’s α = .87, McDonald’s ω = .87). The participants’ mean sum scores can be found in Table 1.
Social Media Disorder Scale
SMD symptoms were assessed using the Social Media Disorder Scale (SMDS; van den Eijnden et al., 2016). The scale is constructed similar to the IGDS (Lemmens et al., 2015) and assesses via nine items the abovementioned nine IGD symptoms according to the American Psychiatric Association (2013), applied to social media use instead of gaming. The SMDS also uses the same binary response format and the same cutoff scores as the IGDS. It was also used in its self-report version (van den Eijnden et al., 2016) and in its parent-report version (SMDS-P; Austermann et al., 2021). The self-report version of the SMDS was filled in by n = 79 patients, while the parent-report version (SMDS-P) was filled in by n = 107. The scale shows good internal consistencies with Cronbach’s alpha ranging from α = .76 to α = .82 for the self-report version (van den Eijnden et al., 2016) and a Cronbach’s alpha of α = .85 and a McDonald’s Omega of ω = .88 for the parent-report version (Austermann et al., 2021). In this study, the SMDS exhibited questionable to good internal consistency (SMDS: Cronbach’s α = .63, McDonald’s ω = .59; SMDS-P: Cronbach’s α = .87, McDonald’s ω = .87). The participants’ mean sum scores are presented in Table 1.
Gaming Time
Gaming time was assessed via both self-report and parent-report. Participants were asked to indicate how long they typically played video games on an average weekday and on an average day of the weekend. A composite score of average daily gaming time was computed using the following formula:
(5*average weekday time +2*average weekend time)/7
This was done separately for self-report and parent-report.
Procedure
Data were collected between April 2021 and March 2023 as part of the routine care diagnostics. Pen-and-paper questionnaires were distributed to patients and their legal guardians, mostly their parents, as part of their routine baseline diagnostics via their therapists. Most of the patients filled in the questionnaires at home, others on site (at the clinic). Afterward, the therapists took them to the study coordinators.
Statistical Analysis
Data analysis was performed using IBM SPSS Statistics version 29. Initially, an exploratory factor analysis (EFA) was conducted to determine the underlying factor structure of the IVS questionnaire using a parallel analysis according to Horn (1965). Results were evaluated according to the parallel, scree, and Kaiser’s criterion. Beforehand, the Kaiser–Meyer–Olkin (KMO; Kaiser, 1970) measure of sampling adequacy was determined. The reliability of the scale was assessed using Cronbach’s alpha and McDonald’s omega. On top of that, item total correlations and factor loadings were analyzed. The receiver operating characteristic (ROC) analysis was used to evaluate the diagnostic accuracy of the IVS scores. The ROC analysis was conducted using IGDS self-report data as a reference for IGD diagnosis, as this approach represents a more conservative criterion due to the lower likelihood of child and adolescent patients meeting diagnostic thresholds based on self-evaluation compared with parent ratings (Kewitz et al., 2021). This decision was made to test the diagnostic accuracy of the screening tool more conservatively. Since the ROC analysis showed that the IVS sum score was in need of improvement (see results), the predictive validity of individual items was analyzed using logistic regression analyses. The ROC was redone for items that proved to be a significant predictor of IGD. A proposed cutoff value was identified. Correlation analyses between IGDS, SMDS, gaming time, and the newly proposed IVS score were computed to validate the scale. To examine whether the IVS was differentially related to symptoms of IGD and SMD, Fisher’s Z-test was used. This analysis was conducted separately for self-report and parental report data.
Ethics
Data were collected in a routine care setting. Goethe University Frankfurt granted us permission to collect data according to its ethical guidelines. Both the patients and their legal guardians gave their consent that their data could be used for scientific purposes. The study followed the principles of the Declaration of Helsinki.
Openness and Transparency
The final data set for the study is available at Open Science Framework. The URL for this website is https://osf.io/g869q The permanent DOI pointing to this raw data is 10.17605/OSF.IO/G869Q
Results
Factor Structure and Reliability
The EFA conducted on the IVS questionnaire indicated a single-factor solution. The KMO measure of sampling adequacy was .881, demonstrating the data’s suitability for factor analysis. The factor loadings for the items were high, ranging from λ = .82 to λ = .93, indicating that all items contributed significantly to the underlying construct.
The internal consistency of the IVS was excellent, with a Cronbach’s alpha of α =.93 (McDonald’ ω = .93). Item-total correlations were . 79Item4 < ri < .88Item1.
Diagnostic Accuracy
The diagnostic accuracy of the IVS was evaluated using ROC analysis, using the diagnosis based on the IGDS self-assessment as the criterion. Complete data from n = 105 participants were available for the IGDS. Thus, the following analyses were conducted with that smaller sample size.
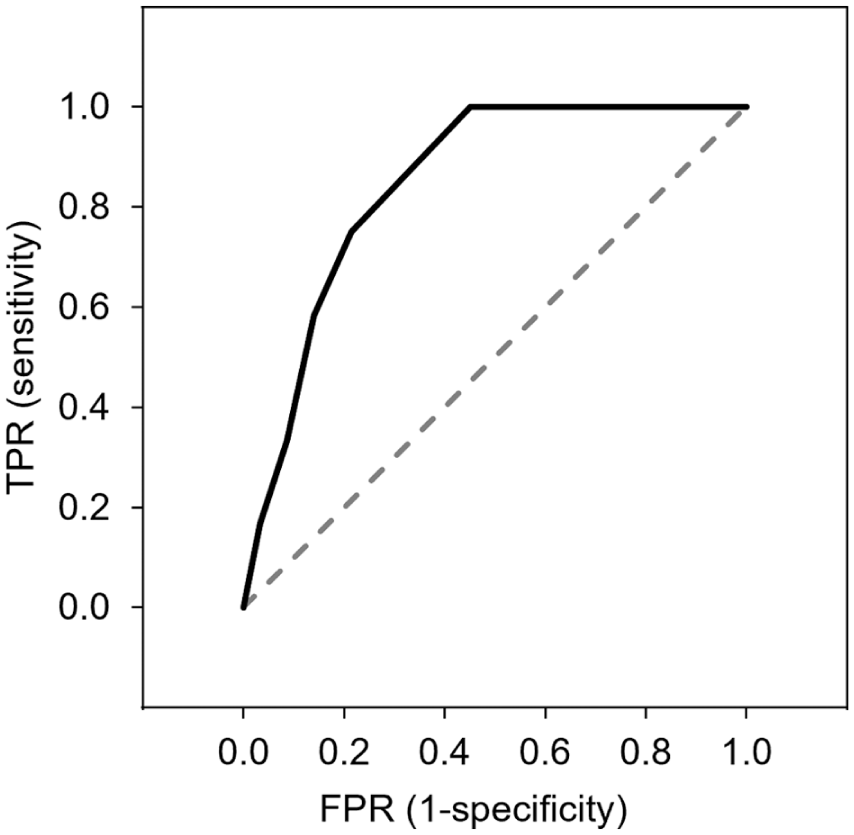
The overall IVS score yielded an area under the curve (AUC) of 0.78 (95% confidence interval [CI] = [0.68, 0.89]), suggesting good discriminatory power. A proposed cutoff score of 12 or higher was identified. Yet, the ROC graph was unsatisfactory (see Figure 3), indicating the need for further refinement.
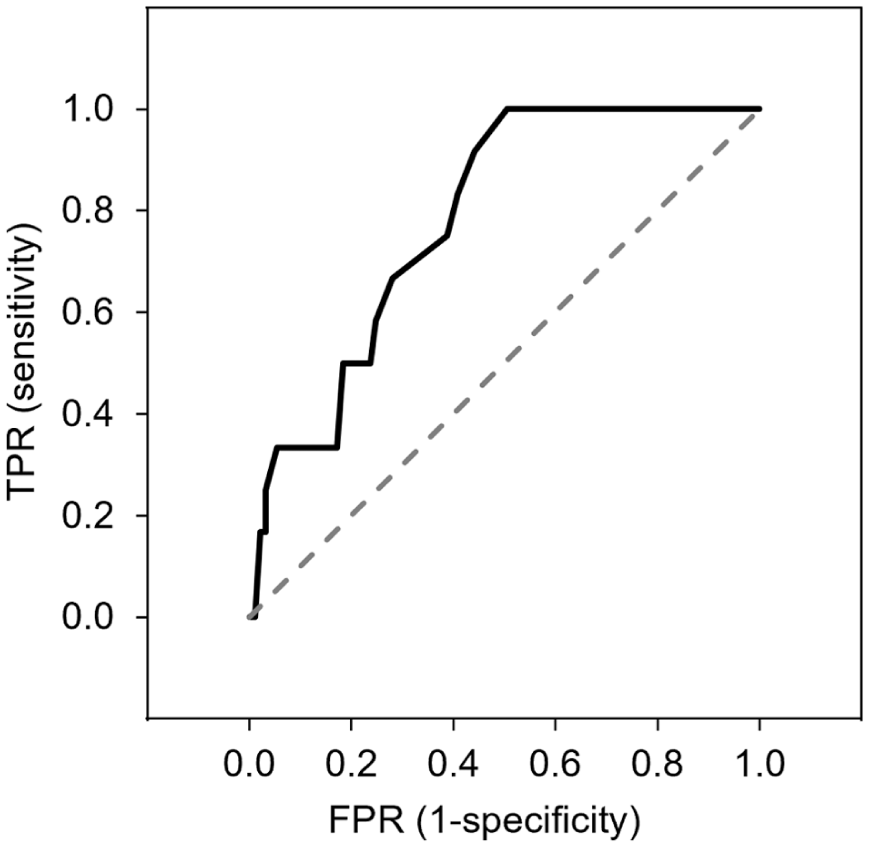
Receiver Operating Characteristic (ROC) Curve for the 5-Item Version of the IVS.
Thus, we performed item-level analyses using logistic regression. These identified only Item 1 as a significant predictor of IGD diagnosis, whereas Items 2 to 5 did not contribute to significantly predicting IGD diagnosis (see Figure 4).
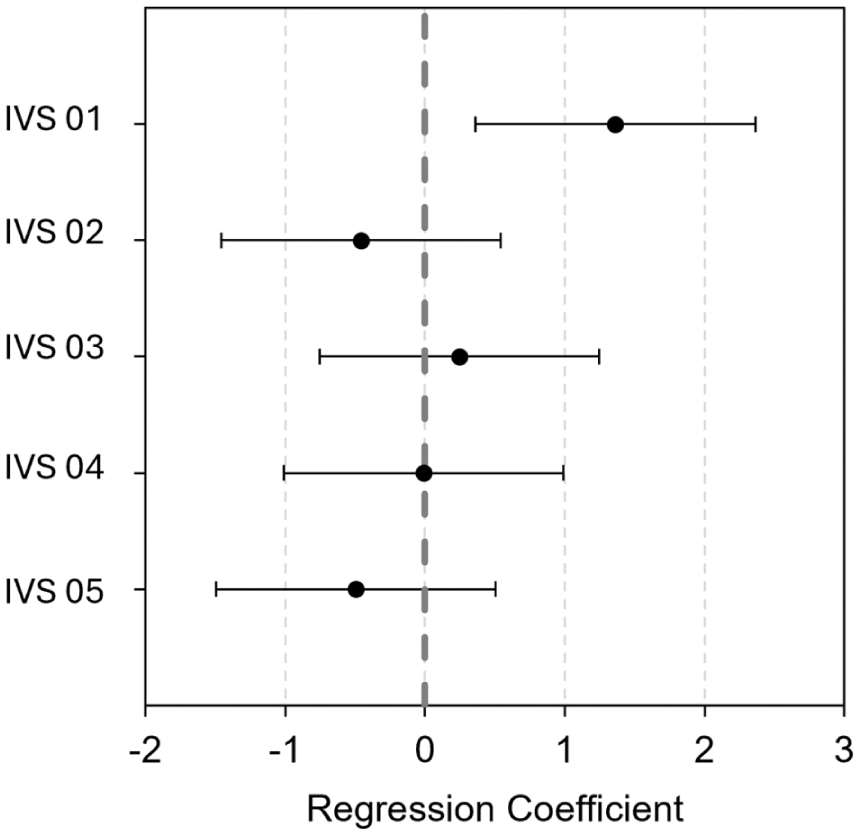
Logistic Regression Coefficients and Confidence Intervals (Without Intercept).
Subsequently, an ROC analysis of Item 1 alone was performed and showed an AUC of 0.85 (95% CI = [0.76, 0.93]), with a suggested cutoff value of 3 or higher (see Figure 5). According to our analysis, Item 1 should effectively identify all participants who met the diagnostic criteria for IGD, though it may also result in a 45% false-positive rate. In the sample with complete IGDS data, the proposed cutoff was reached by n = 54 (51.4%) of the participants (see Table 2). For sensitivity and 1-specificity information at different cutoffs, see the annotation of Figure 5.
Receiver Operating Characteristic (ROC) Curve for the Single-Item Version of the IVS.
Distribution of IVS Classification and IGD Diagnosis According to IGDS (n = 105).

Correlations with Established Measures
Item 1 showed significant positive correlations with established measures of IGD. Specifically, the correlation of the IVS with the IGDS self-report was r(103) = .57, 95% CI = [.43, .69], p < .001, and with the IGDS parent-report was r(73) = .49, 95% CI = [.29, .64], p < .001, indicating moderate to strong associations with these validated instruments. At the same time, the correlation of the IVS with the SMDS self-report was nonsignificant, r(77) = .19, 95% CI = [−.03, .39], p = .094. However, correlation with the SMDS parent-report did reach significance, r(105) = .22, 95% CI = [.03, .39], p = .024. Overall, there were significant differences between IGDS and SMDS self-report correlations, Z = 3.0, p = .001, as well as between IGDS and SMDS parental report correlation, Z = 2.0, p = .021, suggesting differential relationships of the IVS with the constructs of IGD and SMD. Thus, the IVS correlated significantly higher with the IGDS than with the SMDS, which is true for self- and parent-report. Finally, IVS Item 1 showed weak to moderate positive correlations with gaming time (self-report: r(118) = .36, 95% CI = [.19, .50], p < .001; parent-report: r(128) = .27, 95% CI = [.11, .43], p = .002).
Discussion
This study evaluated the psychometric properties of the IVS scale in its five-item version and explored its potential as a single-item screener for IGD. While the full five-item version demonstrated the expected single-factor structure and high internal consistency, diagnostic accuracy was insufficient, leading to a reanalysis focused on single-item performance. The results indicate that Item 1 alone may serve as a proxy for IGD screening, showing moderate to strong correlations with IGD measures, small to moderate correlations with gaming time and no to small correlations with SMD, thereby supporting its construct validity. Item 1 reads: “Which of the seven images best represents your relationship with your favorite video game?.” It is the one item that directly addresses the overall relationship/interconnectedness with the game.
The single-item solution demonstrated promising diagnostic accuracy with an AUC of 0.85 (95% CI = [0.76, 0.93]), indicating its effectiveness in identifying individuals at risk for IGD. The proposed cutoff score of 3 or higher demonstrates perfect sensitivity, successfully identifying 100% of participants who meet the IGD threshold of five or more criteria. Thus, values of 3 or higher on the single-item version of the IVS appear indicative of a higher risk for IGD. We will refer to the measure as the Single-Item IVS. The high sensitivity of the Single-Item IVS is particularly desirable in a screening instrument primarily aimed at effectively ruling out individuals who are with certainty negative and do not need further diagnostics. However, this cutoff is also associated with a high false-positive rate of 45%, indicating that nearly half of the true negatives are misclassified as positive. While the high sensitivity is advantageous, as it ensures that all real cases are included, the high rate of false positives implies that, for scores above the cutoff, further diagnostic assessment is essential before any therapeutic interventions are initiated. The cutoff thus discriminates between those who can be reliably classified as not meeting diagnostic criteria and those who require further assessment, given that approximately every fifth individual above the cutoff is likely to meet the diagnosis. One might question whether this is truly advantageous. However, the Single-Item IVS has the potential to reduce the need for further IGD diagnostics by approximately 50%, as about half of the sample scores below the cutoff. This can result in a significant reduction in diagnostic costs. We believe that such a reduction remains economically viable for routine screenings. Given the scale’s efficiency and low resource demands, its application appears to be highly valuable.
Particularly for children and adolescents, the Single-Item IVS offers practical advantages as a screening instrument for IGD in clinical and educational settings. Its pictorial nature aligns with established child-friendly self-assessment tools, such as the Self-Assessment Manikins (Morris, 1995), which have proven resourceful in evaluating emotional states in young populations (Gouvousis et al., 2010; Hughes & Kendall, 2008). The Venn-like diagrams allow for easy self-reporting, potentially even among children with limited reading or cognitive skills, making it a valuable addition to existing assessment methods. Also, given its rapid administration, the Single-Item IVS is particularly useful for early detection and referral, ensuring that at-risk individuals are not overlooked and can undergo further comprehensive assessment when needed.
Beyond its utility in initial screening, the Single-Item IVS also holds potential for therapy process monitoring. Branand et al. (2019) proposed extending the IOS to state-based assessments rather than solely trait-based measurements. This could provide a more dynamic understanding of how identity fusion fluctuates over time, potentially making the Single-Item IVS useful in tracking changes in IGD severity and, therefore, applicable in therapy process monitoring, helping to track IGD symptom progression during treatment.
Taken together, the main distinction from existing IGD scales is that the IVS is simple, easy to understand, and straightforward to administer, making it suitable for routine diagnostics via self-report even in younger populations. Moreover, its nonverbal format enhances accessibility for individuals with limited language proficiency and facilitates cross-cultural application in research by minimizing the need for translation and adaptation efforts. By lowering practical and linguistic barriers to assessment, the IVS may help promote more routine diagnostic screening and reduce the likelihood that IGD remains undetected.
The effectiveness of the Single-Item IVS as a screening tool for IGD may be related to the underlying psychological mechanisms of identity fusion and immersion in gaming. Prior research suggests that individual’s obsessive passion for gaming and, to a lesser extent, harmonious passion have been linked to problematic gaming behaviors (Infanti et al., 2023). This could be in line with the experience of a permeable sense of self, with blurred boundaries between personal identity and gaming. The item asking about the relationship with the game appears to tap into a psychological mechanism distinct from cognitive engagement (e.g., thinking about the game) or desire (e.g., wishing to play). While all IVS items aim to capture immersion, the “relationship” item may uniquely reflect the internalization of the game into the self-concept, signaling that the game is no longer just an activity but part of who the person is. The other items (e.g., feelings, thoughts, desired relationship, and time spent) introduce additional psychological domains (affect, cognition, motivation, and time investment) that may only partially overlap with the theoretical concept of Other-in-Self (Aron et al., 1992) or Identity Fusion (Swann et al., 2012). On top of that, Item 1 uses straightforward wording and a concrete relational focus, making it easily interpretable across ages and cultural backgrounds. Items like “feelings,” “thoughts,” or “desired relationship” are more abstract and metacognitive, which may be difficult for younger participants to differentiate or report accurately. In younger or less verbally proficient populations, these subtle distinctions may blur, reducing reliability and construct validity. In addition, the Venn-like visual format may not be suited to represent thoughts or feelings. Participants may have struggled to map their “feelings” or “thoughts” onto spatial overlap diagrams, causing measurement noise. Thus, it is plausible that Item 1 as the “relationship” item functions as a more sensitive indicator of problematic gaming because it reflects not just use, but identity-level dependence on the game. However, this is a post hoc hypothesis that warrants further examination.
An additional notable finding was the discrepancy between self-reported and parent-reported IGD scores, with parents reporting higher scores than youth themselves (see Table 1), a pattern observed in previous clinical studies (Kewitz et al., 2021; Lindenberg & Holtmann, 2021; Szász-Janocha et al., 2020). Adolescents may underreport their IGD symptoms, while parents may have stricter perceptions of the severity of symptoms. This reinforces the need for multi-informant assessments, including clinical evaluations, to enhance diagnostic accuracy.
Limitations and Future Research
Several limitations must be considered. First, the study sample consisted exclusively of patients from an outpatient clinic, limiting generalizability to the broader nonclinical population. In addition, the scale was administered in two settings (clinic and home), potentially introducing variability in response conditions. However, in both contexts, participants completed the questionnaires independently, either alone in the clinic waiting room or on their own at home. Future research should validate the IVS in community samples to determine whether the proposed cutoff score remains appropriate. It is possible that a different threshold would be needed in nonclinical settings. In addition, the applicability of the Single-Item IVS to adults or other addictive behaviors warrants examination, and larger sample sizes are needed to confirm the robustness of these findings.
Second, as mentioned above, 45% false positives highlight the need for follow-up assessments. While the Single-Item IVS is useful for preliminary screening, it should not be used as a stand-alone diagnostic tool. Instead, it should serve as a starting point for further evaluation rather than an indicator for immediate intervention, preventing unnecessary resource strain.
Third, the study relied on the IGDS as the validity reference for the IVS. While widely used in research, the IGDS has several limitations that warrant caution. It has been criticized for being overinclusive, potentially classifying individuals as meeting IGD criteria even when gaming behavior may be subclinical or not associated with significant impairment. Moreover, the IGDS focuses on DSM-5 criteria for IGD, which are themselves under discussion in the literature for potential overdiagnosis and lack of alignment with more conservative frameworks, such as the ICD-11 GD criteria (WHO, 2024), which emphasize functional impairment (Castro-Calvo et al., 2021). Critics argue that a DSM-5 diagnosis can be given without the endorsement of any impairment criteria (Colder Carras & Kardefelt-Winther, 2018), inflating estimates of IGD prevalence. In addition, the psychometric properties of the IGDS (Lemmens et al., 2015) appear somewhat less robust in more recent studies on children and adolescents compared with the original validation sample. Nonetheless, it remains a useful instrument for assessing IGD in younger populations (Paschke et al., 2021).
On top of that, in this study, fewer data were available on IGDS than on IVS due to a change in routine assessment during the data collection period. As this study could not include clinical diagnoses for validation and because of the IGDS limitations, future research should compare IVS performance against predominantly used clinical diagnoses and the more conservative ICD-11 criteria.
It is also worth noting that the internal consistency of the SMDS in self-report was questionable in this study, contrary to the good internal consistency reported by van den Eijnden et al. (2016). However, this problem has been reported before (Leo et al., 2023). Accordingly, future studies should test further measures to assess the construct validity of the IVS.
Some additional considerations and directions for future research should be noted. First, the nonverbal, pictorial format of the IVS could be further enhanced by including pictograms to represent the self and the video game. Second, future studies could examine gaming frequency, video game genre and the relationship with a specific avatar or with video games in general, to help further clarify the scale’s construct validity. In this study, we chose to focus on the relationship with a favorite video game for the reasons outlined in the introduction. However, this focus may only partially capture a broader gamer identity that is not tied to a single game. Third, as the IVS relies on self-report, responses may be influenced by participants’ subjective perceptions, social desirability, or limited self-insight. However, given that identity fusion is inherently a subjective construct, self-report remains a valid and essential approach—though future research could benefit from complementary methods (e.g., clinical diagnoses or clinical interviews). In addition, further investigations should explore theoretical mechanisms underlying the IVS, including identity fusion and immersion. A deeper understanding of this phenomenon could improve both the conceptualization of IGD and the development of more precise screening instruments.
Conclusion
The Single-Item IVS appears as a promising, easy-to-use screening tool for IGD, showing high sensitivity and practical advantages, especially for youth. While it can reduce the need for extensive diagnostics, the high false-positive rate means further assessment is necessary before clinical decisions. Future research should validate these findings in larger, diverse samples and explore the underlying psychological mechanisms. Overall, the Single-Item IVS represents a valuable, resource-efficient tool for preliminary IGD screening, with promising implications for clinical practice and research, pending further validation.
Supplemental Material
sj-docx-1-asm-10.1177_10731911261427104 – Supplemental material for Development of a Short Symbol-Based Screening Instrument for Internet Gaming Disorder: The Inclusion of Videogame in the Self (IVS) Scale for Children and Adolescents
Supplemental material, sj-docx-1-asm-10.1177_10731911261427104 for Development of a Short Symbol-Based Screening Instrument for Internet Gaming Disorder: The Inclusion of Videogame in the Self (IVS) Scale for Children and Adolescents by Sonja Kewitz, Sebastian Brand, Sabine Windmann and Katajun Lindenberg in Assessment
Footnotes
Acknowledgements
Data collection took place at the outpatient clinic for child and adolescent psychotherapy of Goethe University Frankfurt. We sincerely thank all patients who participated in the study and the psychotherapists who supported the data collection process. We also extend our gratitude to Jacqueline Salzer for her valuable contributions through her bachelor’s thesis.
Author Contributions
S.K. was involved in conception and design of the study, and data collection and analysis, and wrote the paper. S.B. analyzed the data and was involved in writing. S.W. was involved in the conception and design of the study and writing. K.L. conceived and designed the study and was involved in data collection and writing. All authors have read and agreed to the published version of the article.
Ethics
Data were collected in a routine care setting. Goethe University Frankfurt granted us permission to collect data according to its ethical guidelines. Both the patients and their legal guardians gave their consent that their data could be used for scientific purposes. The study followed the principles of the Declaration of Helsinki.
Consent to Participate
The data were collected as part of routine diagnostic procedures, for which participants and their legal guardians received both written and verbal information.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability
Supplemental Material
Supplemental material for this article is available online.