
Abstract
Stigma experienced and/or conveyed by family members of individuals with mental health conditions may impact on their health and wellbeing, and on the quality of care and health outcomes of people with lived experience of mental illness. However, most of the research on stigma and mental illness has been on public attitudes and behaviors of patients rather than what is expressed by or experienced within families. We aimed to identify scales that assess stigma in the context of family life, and to evaluate their psychometric properties. A literature search across Web of Science, PsycINFO, Medline, Scopus, and ProQuest Social Science (up to August 2025) yielded 14 eligible studies, reported via PRISMA. None of the 14 scales directly or solely assesses family-context stigma, but includes dimensions of self or public stigma, especially related to schizophrenia, possibly neglecting other forms of severe mental illness (SMI). In addition, existing tools often overlook the full range of family relationships and diverse caregiving experiences. There is a need for measures that more adequately and comprehensively capture the often complex and nuanced experience of mental illness stigma within families.
Stigma refers to negative beliefs, attitudes, or stereotypes directed at a person or group due to a characteristic considered different or undesirable. As such stigma encompasses facets such as labeling, stereotyping, exclusion, status loss, and discrimination (Link & Phelan, 2001) and has been used in a wide range of health and social contexts such as AIDS, race, and disability (Jackson-Bets & Edwards, 2018). Thus, while socially stigmatizing attitudes and behaviors may be differently expressed, perceived, or experienced, they generally involve relationships of asymmetrical power (Stangl et al., 2019). Stigma may be anticipated by such individuals, provoking avoidant or defensive behaviors, such as social withdrawal, self-criticism, overgeneration, and self-stigmatization (Rüsch, 2023; Thornicroft et al., 2009). Thus, such individuals internalize much of the negative beliefs and attitudes of others including attributes of violence, unpredictability, untrustworthiness, and so on. In this way, self-stigma is highly correlated with low self-esteem (Corrigan & Rao, 2012). Over time, one’s identity may be replaced by a dominating negative self-view, an “illness identity” that overshadows all other aspects of the individual (Yanos et al., 2008).
Anticipated stigma, referring to an expectation of rejection, contributes to the reinforcement of internalized stigma (Bos et al., 2013; Parcesepe & Cabassa, 2013; Pescosolido & Martin, 2015; Rüsch et al., 2005). Relatedly, affiliate stigma (stigma vicariously experienced by family members or caregivers) and associative stigma (stigma directed toward individuals through their broader social ties) have been distinguished in the literature (Mak & Cheung, 2008; van der Sanden et al., 2016). Clarifying this distinction is important, as inconsistent use of these terms can obscure differences in how stigma affects families versus wider networks.
As social beings, individual family members, whether immediate or extended, receive, and reproduce cultural knowledge, beliefs, behaviors, and attitudes including those pertaining to stigma. Thus, while families are potential recipients of stigma (vicarious or affiliate stigma), they may also, wittingly or unwittingly, reproduce beliefs and behaviors that are discriminatory and harmful toward a family member with a mental illness. Within many cultural narratives, mental illnesses are believed to be the result of poor genes, malevolent parenting, lack of care, spiritual problems, or adverse environmental conditions, beliefs often compounded by awareness of the hereditary nature of such conditions (Magliano et al., 2001; Phillips et al., 2000; Yildiz et al., 2010). In this context, families become sites of attribution, not only regarded as causal agents but also as carriers of genetic or moral responsibility (Leavey et al., 2007, 2016). Consequently, family members frequently experience a deep sense of responsibility for their loved one’s mental illness and its uncertain prognosis, while also confronting a complex emotional terrain marked by guilt, self-blame, and internalized shame. Such responses are not simply personal but are shaped and reinforced by the family’s broader social and cultural milieu, which may stigmatize them both explicitly and implicitly (Goldberg et al., 2023; Yin et al., 2020). Studies, both qualitative and quantitative, have illuminated these psychosocial challenges, particularly among families of individuals diagnosed with schizophrenia, bipolar disorder, major depression, and complex post-traumatic stress disorder. In contrast, these dynamics appear less explored in relation to chronic anxiety conditions and personality disorders, where stigma may manifest in more diffuse or nuanced forms (Chang & Horrocks, 2006; González-Torres et al., 2007; Krupchanka et al., 2016; Lerner et al., 2018). For some, the emotional toll of this stigma results in social withdrawal, as family members retreat from their communities, perceiving their connection to mental illness (affiliate stigma) as a source of disgrace, exposure, or humiliation (Ahmedani et al., 2013; Dolezal, 2022).
Families may therefore play a significant role in either mitigating or exacerbating the process of stigmatization. Understanding the root causes and the complex, often contradictory issues related to stigma within families may provide the basis for psychoeducational family interventions that reduce the risk of their families contributing to stigma. A systematic review of scale measurement properties (Mokkink et al., 2009) may identify the most appropriate scale for assessing a particular phenomenon, select appropriate scales, and identify gaps in knowledge on measurement properties (Sultan et al., 2021).
In the present study, family-context stigma is operationally defined as stigma-related beliefs, emotions, and behaviors that are experienced, enacted, or negotiated specifically within family systems as a result of a family member’s stigmatized identity, condition, or circumstance. This includes the ways in which stigma is expressed between family members (e.g., blame, distancing, shame, or concealment), the internalization of stigmatizing attitudes that arise through family interactions, and the structural or relational consequences that emerge within the family unit (e.g., altered roles, secrecy, disrupted communication, or avoidance of external support). Importantly, family-context stigma is not limited to the perceptions of external observers but is embedded in ongoing relational dynamics, shared meanings, and reciprocal influence processes among family members. Thus, the construct captures both interpersonal manifestations of stigma within families and the unique psychosocial burden that arises from being part of a stigmatized family system.
While family-context stigma is related to existing forms of stigma described in the literature, such as self-stigma, public stigma, affiliate stigma, and associative stigma, it is conceptually distinct in both its level of analysis and its primary locus of action. Self-stigma refers to the internalization of negative societal beliefs by the stigmatized individual, whereas public stigma reflects societal attitudes toward a group, and associative or affiliate stigma captures the stigma experienced by individuals because of their relationship to a person who is stigmatized (Ritsher et al., 2003). In contrast, family-context stigma focuses specifically on the family as a relational environment in which stigma is produced, reinforced, contested, and transmitted across members and over time. It therefore encompasses but is not reducible to individual-level internalization or externally imposed devaluation. Rather than focusing only on individual psychological reactions or generalized societal attitudes, family-context stigma emphasizes relational processes, such as triangulation, protective secrecy, intergenerational transmission of shame, and stigma-management strategies negotiated among family members. This relational focus positions the construct at the meso-level, bridging individual and societal perspectives on stigma.
Conceptually, family-context stigma is positioned as an intermediate, relational construct situated between individual and societal forms of stigma. Public stigma shapes broader beliefs about a stigmatized condition; these beliefs may be internalized as self-stigma by the individual and as affiliate or associative stigma by close others (Brohan et al., 2010). Within families, however, these broader attitudes take on relational meaning and are shaped by family-specific processes such as communication patterns, power dynamics, shared narratives, and cultural values (Van Brakel, 2006). Family-context stigma is therefore theorized to (a) be influenced by public and structural stigma, (b) affect both individual and collective family well-being, and (c) mediate outcomes such as family cohesion, help-seeking behavior, and psychosocial adjustment. In this model, the family is not merely the setting in which stigma is experienced, but an active social system that shapes how stigma is interpreted, managed, and reproduced.
Although stigma-related instruments have been reviewed previously, no systematic review has focused specifically on scales measuring mental illness stigma within family contexts. This review addresses that gap by critically evaluating 14 commonly used measures for their psychometric properties, content, and applicability to family settings. While several tools include interpersonal references, most assess individual internal processes (self-stigma), perceptions of public attitudes (public stigma), or stigma via association (affiliate/associative stigma). Even when family is mentioned, it is typically treated as part of the broader social environment rather than as a distinct, emotionally and structurally defined system with unique roles, norms, and histories. Accordingly, existing measures do not operationalize stigma as embedded in family functioning or relational processes, nor do they position the family as the primary unit of analysis. We therefore provide a comparative overview to guide scale selection and highlight the need for instruments that more comprehensively capture cognitive, emotional, and behavioral dimensions of stigma in family contexts.
Aim
To examine scales used to assess various forms of stigma among families caring for individuals with severe mental illness (SMI) through a systematic review.
Method
This study was registered under PROSPERO (CRD42024495217) and was conducted in accordance with the PRISMA guidelines for systematic reviews (Moher et al., 2009; Page et al., 2021).
Search Strategy
To avoid possible replication, we searched prominent databases (including Cochrane Library, Open Gray, PsyArXiv, PROSPERO, Ethos, ProQuest Dissertations and Theses, JBI Database of Systematic Reviews and Implementation Reports, and the University of York Center for Reviews and Dissemination Database) using key terms such as “stigma,” “stigma in family,” “stigma scales,” “systematic review stigma scales,” and “systematic review stigma quantitative measures.” No registered systematic reviews have been conducted in this specific area to date.
A systematic search of the following reputable electronic databases was undertaken: Ovid databases (Medline, PsycINFO) Scopus (Elsevier), Web of Science (Clarivate), Pro-Quest Social Science. Google scholar and ScienceDirect were also utilized for the search. Gray literature sources were accessed through Pro-Quest Dissertations and Thesis (PQDT), multiple websites and organizational sites. The search terms included synonyms and derivatives of “Family Stigma” and “Mental illnesses.” MESH terms for titles, abstracts, and key phrases, terms and keywords were employed. The structure of each database utilized dictated how searches were conducted. Terms were joined using Boolean operators (“AND” and “OR”), and searches were enlarged using truncations (*). The following four groups of main search terms were used in general in combination: (stigma, family/familial/family-based stigma, stigma in family, courtesy stigma, secondary stigma, stigma by association, associative stigma, affiliate stigma) and (family members, carers, parents, spouses, siblings, children, primary care givers, relatives) and (mental illness, severe mental illness, mental health conditions, mental health difficulties) and (measure, scales, psychometric scales, inventory, index). Complete details of the search strategy can be found in File a. The researchers conducted a thorough exploration of databases, employing filtering criteria such as “maximum cited” and “relevance” to refine the search results. This search was carried out up to August 15, 2025, and publication year was not kept under restricted criteria. The reference lists of the included studies were additionally cross-checked, and relevant citations were manually sought and included if they satisfied the eligibility requirements.
Study Selection and Eligibility Criteria
After systematically screening all papers from the databases by reviewing their titles and abstracts, all duplicates were eliminated. We then obtained full texts of potentially relevant articles and screened them for inclusion in the review. PRISMA flow diagram was used to identify and record the selection process for all the articles (Figure 1).
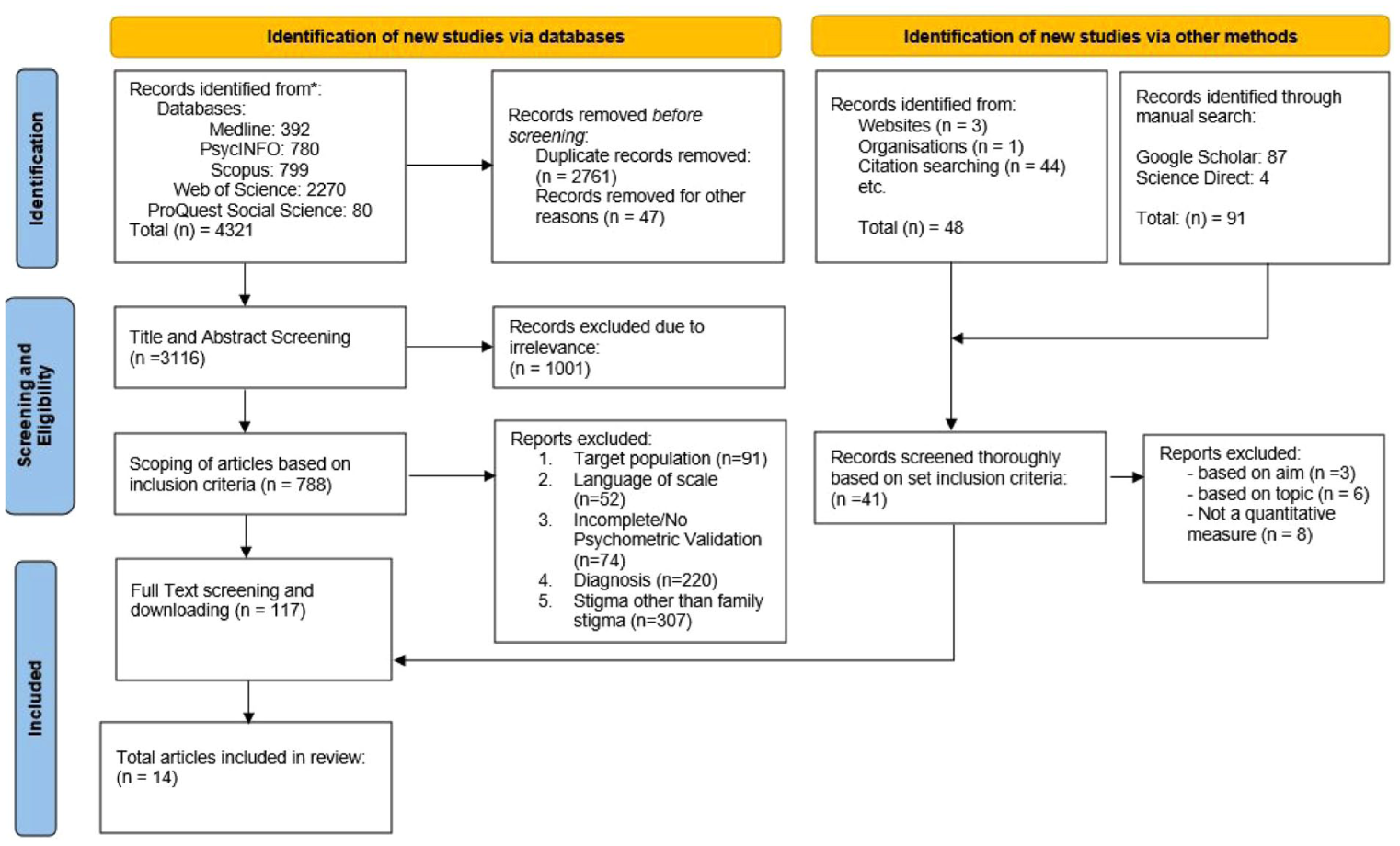
Prisma Flowchart.
In cases of reviewer discrepancies, resolution was pursued through collaborative discussion where a third reviewer was consulted for consensus in areas needed to ensure robustness and reliability of the study selection and extraction process (Nawijn et al., 2019) (Table 1).
Inclusion-Exclusion Criteria.
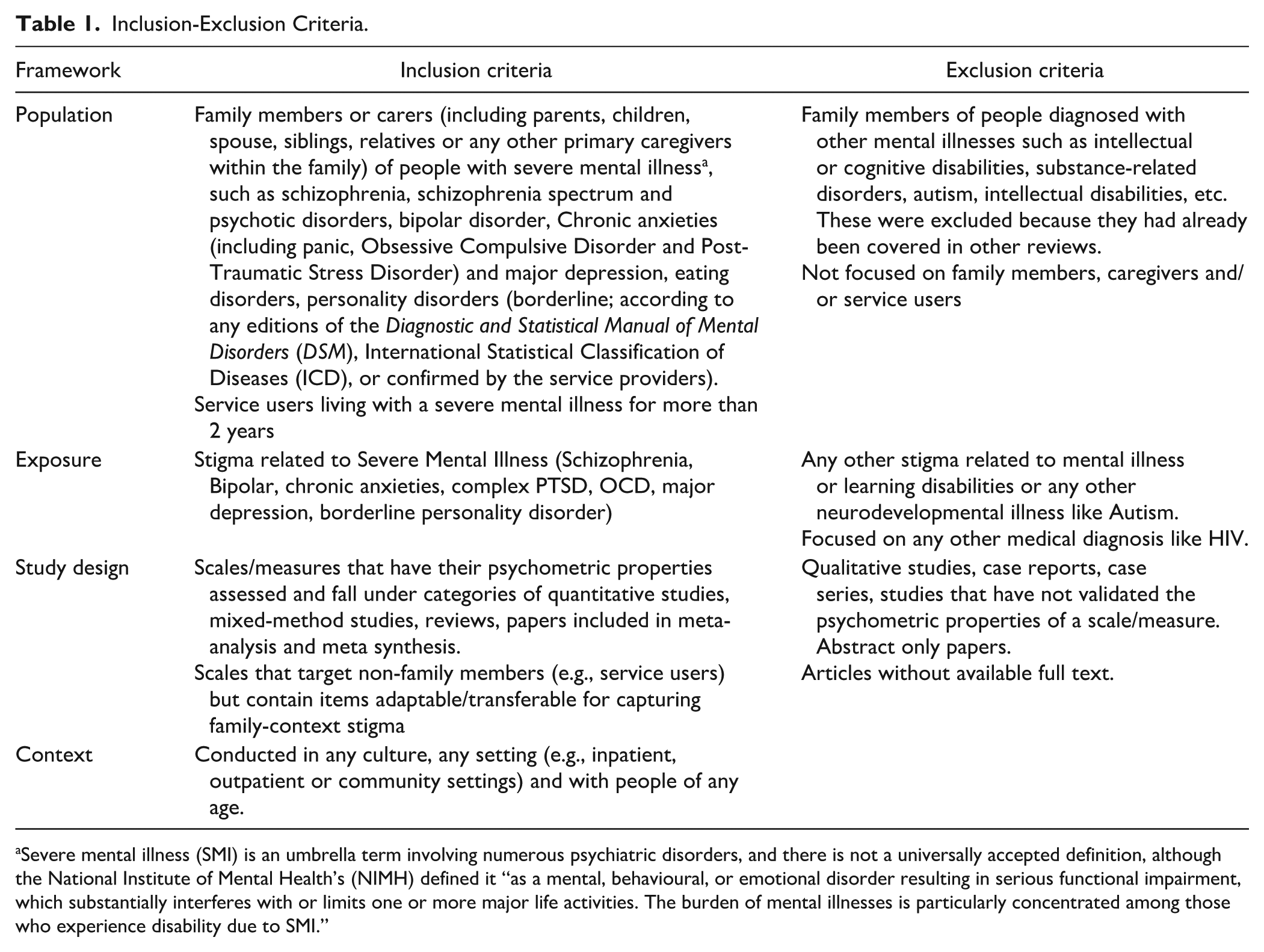
Severe mental illness (SMI) is an umbrella term involving numerous psychiatric disorders, and there is not a universally accepted definition, although the National Institute of Mental Health’s (NIMH) defined it “as a mental, behavioural, or emotional disorder resulting in serious functional impairment, which substantially interferes with or limits one or more major life activities. The burden of mental illnesses is particularly concentrated among those who experience disability due to SMI.”
Data Synthesis
We integrated findings from the selected studies to derive insights into the research question. Employing a content analysis approach, we identified similar, overlapping and emphasized contents and patterns across the literature, allowing for a better understanding of the subject matter, to facilitate building of the new measure emphasizing on the elements that require addressal and assessment.
After data extraction, we collated outcomes to facilitate a thorough analysis of the effectiveness of the measures. We used a narrative approach to analyze the content, examining questions like who the scale worked for, how it worked, and why. We also used a quantitative method to combine relevant data, grouping the studies based on the type of stigma each scale measured, such as self-stigma, public stigma, or stigma by association. The certainty of the evidence was addressed individually for each included study through the GRADE approach, which included five domains addressing risk of bias, inconsistency, indirectness, imprecision, and publication bias, with four levels of rating: high, moderate, low, and very low (Schwingshackl et al., 2021).
Data were presented in both table and written formats, allowing us to identify scales that focused on types of stigma relevant to our research goals, such as the effects of self-stigma versus public stigma within family contexts. This information was intended to support the better visual understanding for the development of a comprehensive stigma scale tailored to family settings, which could aid future research effort.
Results
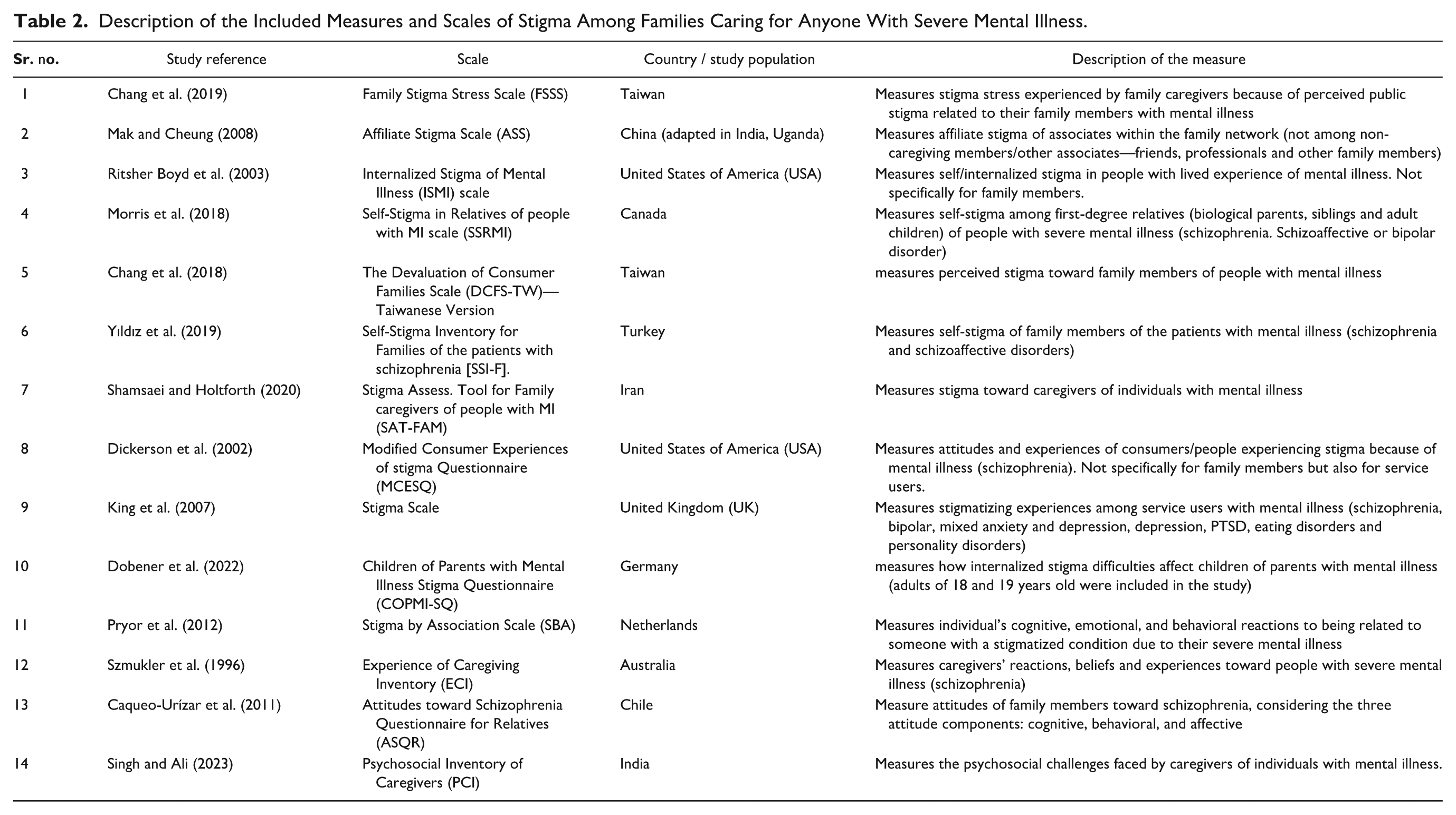
This review scrutinized survey measures of all categories of stigma among families caring for individuals with SMI, focusing on how public, self, and affiliate stigma impact both family members and those with SMI. The goal was to evaluate how well current tools measure the experiences of families dealing with stigma. By doing this, the review aimed to enhance future research on stigma in mental illness by highlighting the need to consider family members in future interventions and design stigma scales that address their experiences, especially when their family members struggle with mental health conditions. The review identified 14 studies that created scales/tools to measure stigma in families to some extent (Table 2). Table 3 gives detailed information about each tool. Some criteria, like comparing results to a “gold standard” measure, were left out because no such standard exists for stigma. To make the evaluation clearer, certain aspects like agreement, measurement error, and responsiveness were adjusted. The quality of the tools were rated based on available information, though not all measures provided complete details (Tables 2 and 3).
Description of the Included Measures and Scales of Stigma Among Families Caring for Anyone With Severe Mental Illness.
Quality Criteria Check.
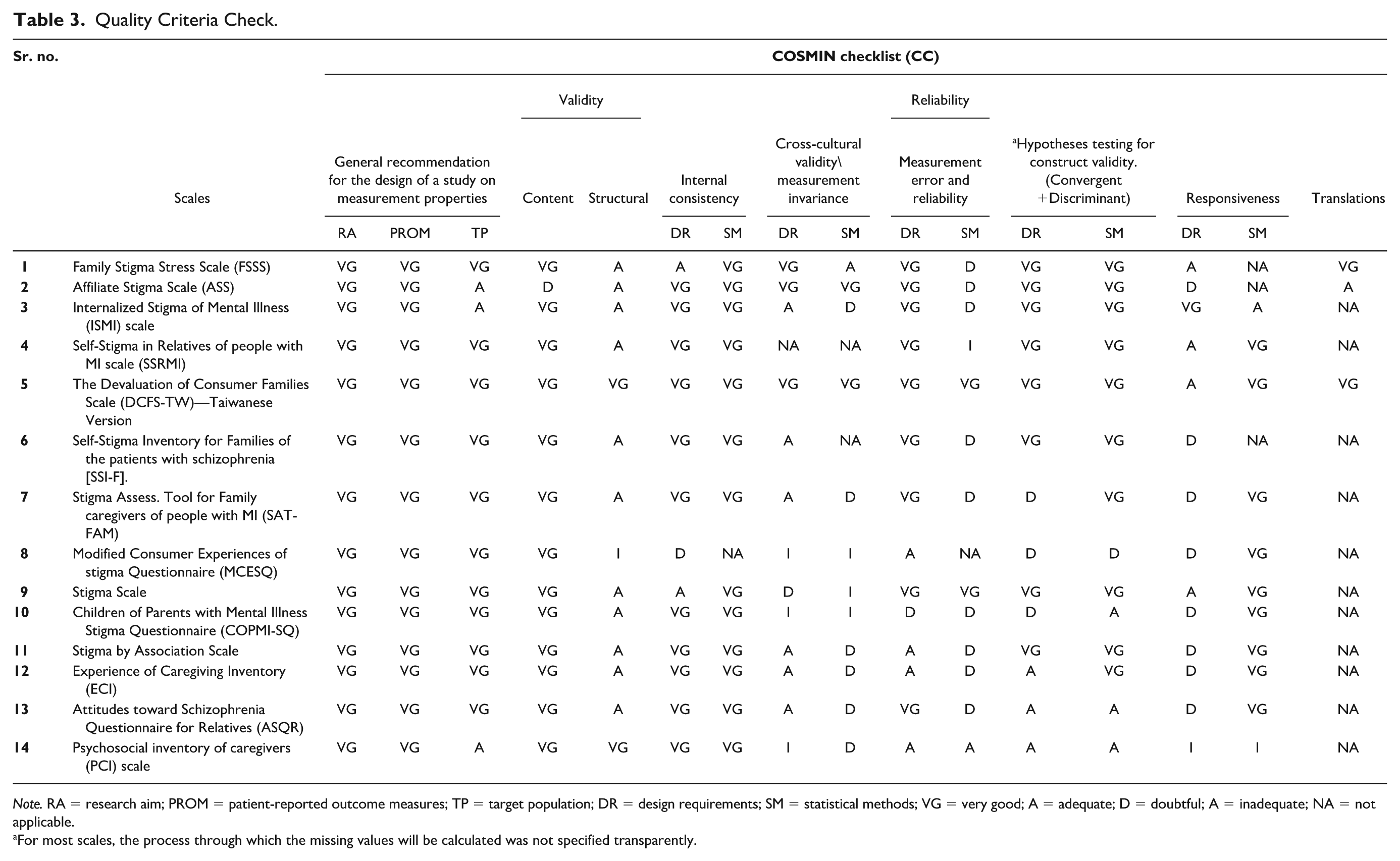
Note. RA = research aim; PROM = patient-reported outcome measures; TP = target population; DR = design requirements; SM = statistical methods; VG = very good; A = adequate; D = doubtful; A = inadequate; NA = not applicable.
For most scales, the process through which the missing values will be calculated was not specified transparently.
Data Extraction
After screening and the removal of duplicate entries, a total of 14 papers underwent a comprehensive full text examination as shown in Figure 1. We followed expert guidelines for paper extraction (Higgins & Green, 2011). Comprehensive documentation was maintained for excluded articles, including the corresponding reasons for their exclusion. Information such as author details, publication year, country of origin, name of scale, type of stigma being assessed, aim of the study, type of scale, language of the scale, response options (binary, Likert-type scale, etc.), number of items, scale development process, piloting and validation processes, reliability tests and results, administration, sampling strategy and sample size, participant percentage variation in gender, ethnicity, etc., age range, question/item themes, and limitation themes elicited through the contents, research objectives, study design, target population, sample size, type of illness, psychometric properties of the scale, and key outcomes of the associated measures was systematically extracted.
A custom critical reading and assessment form facilitated detailed extraction of relevant study information. A Population, Exposure, Outcome (PEO) framework was utilized to conduct in-depth analysis of included papers.
Quality Appraisal and Assessment of Bias
An individual evaluation of the quality and risk of bias profile was conducted for each of the included studies (refer to Tables 3 and 4). The assessment involved rating the level of evidence from all scales using the COSMIN checklist (Mokkink et al., 2019) and collating it with Terwee et al.’s (2007) health status questionnaires, to avoid any gaps and conduct a comprehensive quality check of each measure. The COSMIN checklist encompasses 10 specific criteria, with few subdividing categories under each section. Each category criteria are rated on a 4-point rating scale ranging from “very good,” ‘adequate,’ or “doubtful,” and “inadequate.” The inclusion of a 4-point rating scale serves as an illustrative tool aimed at enhancing comprehension regarding the implications of decisions made in the design of a study, particularly in relation to its methodological quality. The primary objective of the checklist was to facilitate a thorough examination, ensuring that all crucial aspects are duly addressed in the process of designing a study focused on measurement properties. A comprehensive evaluation of each article was determined, categorizing it under the criteria. This checklist rating is also inclusive of the COSMIN Risk of Bias assessment (Prinsen et al., 2018).
Criteria for Adequacy of Psychometric Properties and Scoring System of Stigma Measures.
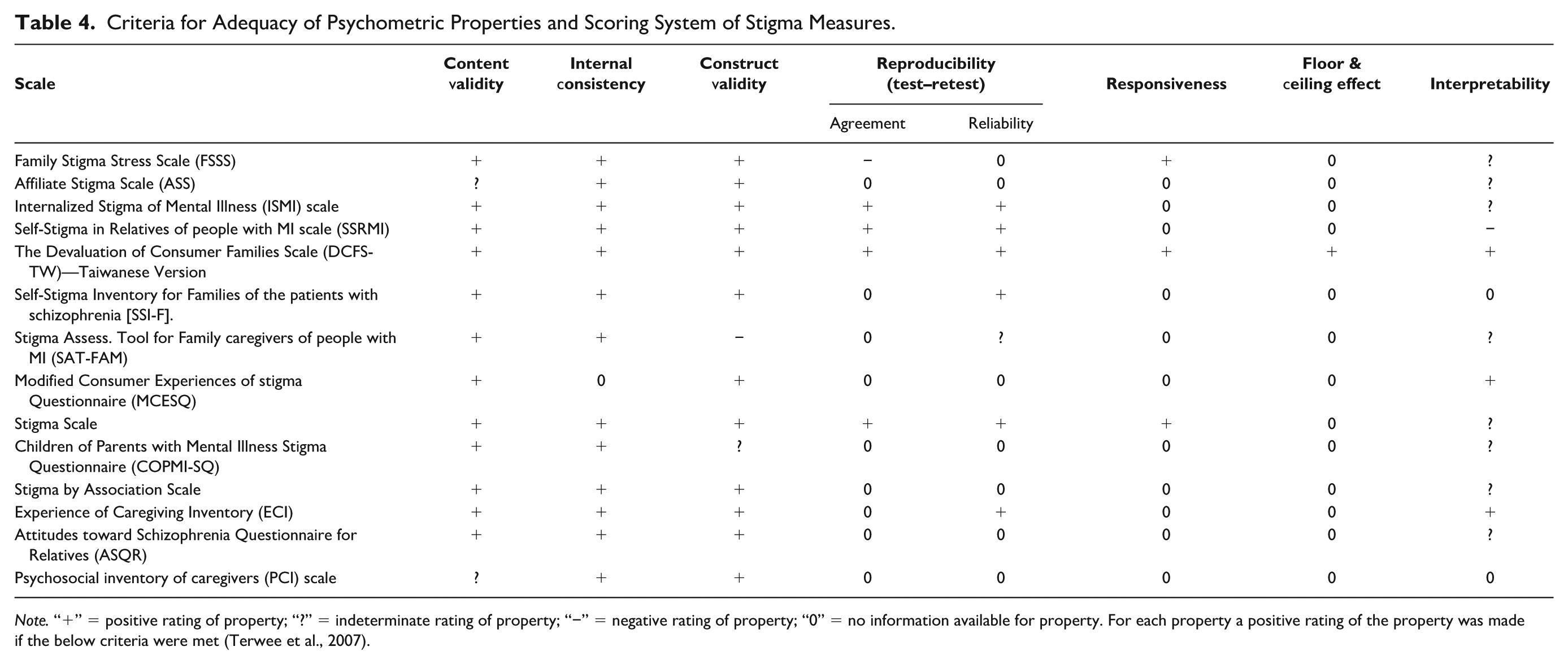
Note. “+” = positive rating of property; “?” = indeterminate rating of property; “−” = negative rating of property; “0” = no information available for property. For each property a positive rating of the property was made if the below criteria were met (Terwee et al., 2007).
In instances where a determination regarding the risk of bias was inconclusive, resolution was achieved through deliberation between GL and FF. Furthermore, for each research study, we explicitly denoted whether at least one outcome measure had undergone validation, its prior publication status, origin (developed by the author or utilizing pre-existing items). The assessment of scales entailed identifying evidence of psychometric adequacy, whereby a scale was deemed acceptable if it met one or more of the subsequent criteria: the authors documented a Cronbach’s α of 0.7 or higher, the authors explicitly affirmed the measure’s reliability or validity, or there existed demonstrable indications of validity or reliability as evaluated by the reviewing team.
The evaluation of nine measurement properties, namely content validity, internal consistency, construct validity, reproducibility (agreement and reliability), responsiveness, floor or ceiling effects, and interpretability, forms an integral part of this framework. Tables 2 and 3 provides a display of the definitions and criteria of adequacy for each psychometric property. Notably, specific criteria from the original framework were selectively applied to certain studies, as evidenced in Table 4. For instance, while Terwee et al. (2007) categorize item selection as a relevant criterion for content validity, this review restricted its consideration of item selection to being a mandatory and applicable criterion solely for studies related to the original scale development (Table 4).
Measures for Families
Eleven measures/scales in Table 2 assess different aspect of stigma, specifically among family members or caregivers of individuals with SMI: Family Stigma Stress Scale (FSSS), Affiliate Stigma Scale (ASS), Self-Stigma in Relatives of people with Mental Illness scale (SSRMI), The Devaluation of Consumer Families Scale—Taiwanese Version (DCFS-TW), Self-Stigma Inventory for Families of the patients with schizophrenia (SSI-F), Stigma Assess. Tool for Family caregivers of people with Mental Illness (SAT-FAM), Children of Parents with Mental Illness Stigma Questionnaire (COPMI-SQ), Stigma by Associate Scale (SBA), Experience of Caregiving Inventory (ECI), Attitudes toward Schizophrenia Questionnaire for Relatives (ASQR) and Psychosocial Inventory of Caregivers (PCI) scale. Among these, ASS is one of the most popular scales employed by researchers to understand associative or courtesy stigma among family members (Chen et al., 2020; Mak & Cheung, 2008).
Self/Internalized Stigma
Two measures assessed self/internalized stigma: SSRMI (schizophrenia, schizoaffective or bipolar disorder—first-degree relatives like biological parents, siblings, and adult children) and SSI-F (schizophrenia and schizoaffective disorder—family relatives like mother, father, sibling, resident spouse).
SSRMI utilizes a mixed-methods approach using both inductive and deductive procedures across four phases: interviews with first-degree biological family members, item finalization, item reduction based on participant feedback, and psychometric validation for both a 30-item and a 10-item scale. The 30-item measure had an internal consistency of .90, with five subscales. However, only three subscales met the adequate reliability criterion (α ≥ 0.70): separation (α = 0.76), culpability (α = 0.77), and devaluation (α = 0.77). Stereotyping (α = 0.62) and status loss/discrimination (α = 0.41) did not meet this criterion. Psychometric analyses suggested that the scale is better conceptualized as a single construct rather than five distinct subscales. To simplify administration, a 10-item version was developed, retaining the broad content and demonstrating similar psychometric properties (internal reliability = .82; test–retest reliability, r = 0.86, p < .001). Given the comparable psychometric features, the 10-item version may be preferable in many settings. The study focused on stigmatized experiences related to three specific severe mental illnesses (SMI), excluding other SMI clusters and the applicability of the scale to second-degree or non-biological family members. In addition, it did not explore the potential differences in self-stigmatization between a family member’s diagnosis and a personal diagnosis.
The SSI-F employs a mixed-method approach to assess self/internalized stigma among relatives of individuals with SMI (Turkish sample). The original 19-item inventory shows strong internal consistency (.88) and test–retest reliability (.93, p < .001). Subscales for withdrawal, concealment of illness, and perceived devaluation have factor scores of .84, .82, and .84, respectively. A 14-item version identifies three factors: fear of others’ reactions leading to social withdrawal, illness concealment, and reduced self-confidence with perceived devaluation. However, the scale is specific to schizophrenia, limiting its broader applicability. The study’s small, single-center sample and lack of comparative analysis with other Turkish self-stigma scales, along with reliance on self-report measures, limit the generalizability and accuracy of the findings.
Perceived/Public Stigma
Among the assessment scales, the FSSS (schizophrenia, bipolar disorder, or major depressive disorder—primary caregiver who devotes maximum time and effort of care) and DCFS-TW (schizophrenia, bipolar affective disorder, or major depressive disorder—family caregivers, identified by the participant as a family member who spent the maximum time and effort in caring for the patient) captured the stigmatized experiences of family members dealing with SMI. These scales adeptly gauge the perceived stigma from the broader public.
The FSSS is an adaptation of an instrument proposed by Rüsch et al. (2009a, 2009b), based on Kaiser et al. (2004). The FSSS, like the original scale, is an 8-item measure with two 4-item subscales: a perceived stigma-related harm subscale and a subscale measuring perceived resources to cope with stigma. Stigma stress occurs if perceived harm exceeds perceived coping resources. The scale has an internal consistency of .85 and showed better test–retest reliability over 4 to 8 weeks than over shorter or longer intervals
DCFS-TW is a modified version of the DCFS by Struening et al. (2001), which assesses perceived stigma toward family members of patients with mental illness (PWMI). Items were also taken from the revised DCFS by Mak and Kwok (2010), both of which have acceptable internal consistency (α = .71 to .86). DCFS-TW is a 9-item scale measuring stigma experienced by family caregivers of PWMI. Confirmatory factor analysis showed satisfactory fit indices, but its applicability is limited to a Taiwanese sample, affecting generalizability. The psychometric properties differ slightly from the original DCFS, and while its briefness and efficiency make it effective in clinical settings, it was only administered to primary caregivers, limiting its ability to distinguish stigma levels between primary and non-primary caregivers.
Affiliate Stigma
Seven different measures assess stigma somewhat in connection with individuals associated with SMI, commonly referred to as either affiliate, associative or courtesy stigma in these scales. Among studies focusing on this cluster of SMI, researchers predominantly employed one of these scales, a modified version of them, or a combination of selected items to conduct their research. Notably, the assessment of affiliate stigma among family members is grounded in the recognition that these measures possess components capable of encompassing the diverse elements of stigmatized experiences among the families of individuals with SMI.
The ASS and SBA are widely used measures with strong psychometric properties, demonstrating internal consistency of .94 and .90, respectively. The ASS is a 22-item self-report scale assessing stigma among caregivers, particularly focusing on the self-stigmatization of Caregivers of People with Mental Illness (CPMI) and Caregivers of People with Intellectual Disabilities (CPID). It evaluates three interrelated dimensions—(a) cognitive, (b) affective, and (c) behavioral, based on the cognitive perspective of stigma (Link et al., 2004), distinguishing it from other scales. The ASS has been validated in multiple contexts, including China, Uganda, and India, alongside being translated to multiple languages. While these studies demonstrate good reliability and validity, limited sample diversity and cultural variation restrict the Generalizability of their findings. The ASS shows robust psychometric properties in caregiver populations but has conceptual limitations for assessing family-context stigma. It measures the internalization of stigma by individual caregivers without accounting for how stigma operates within the broader family system. The scale does not capture how stigma is experienced, transmitted, or negotiated among multiple family members, nor does it assess relational consequences such as role strain, disrupted communication, or changes in family cohesion. Although valuable for evaluating caregiver-level stigma, the ASS does not fully address the relational and systemic processes central to family-context stigma, highlighting the need for measures that explicitly assess stigma within family interactions and functioning.
Recent developments have introduced new scales that broaden the assessment of caregiver stigma. For example, the Psychosocial Inventory for Caregivers (PIC) in India evaluates a wide range of psychosocial challenges with strong internal consistency, and the Family Stigma Stress Scale (FSSS), translated into English, focuses on stressors associated with family-related stigma. Unlike the ASS, which primarily targets self-stigmatization within the family, these newer scales capture a broader spectrum of caregiver experiences, providing a more holistic understanding of the psychosocial and familial impacts of stigma.
Alternatively, SBA presents a notable limitation in its documentation, specifically in the lack of information regarding the psychometric validation of the scale, its reliability and validity. The scale is designed around three core elements: cognition, emotional responses, and behavioral reactions. The cognitive aspect is assessed through 12 items that gauge the emotional impact of having a family member with SMI, such as sentiments like “I feel ashamed of it.” In addition, the scale includes seven items focused on beliefs related to having a family member with a severe mental illness, for instance, “People might treat me in a negative way if they find out about my family member’s condition.” Finally, nine items are dedicated to measuring behavioral reactions associated with having a family member with severe mental illness. While the scale’s content is available, the inaccessibility to the whole research article and absence of a robust psychometric foundation leaves gaps in our ability to critically evaluate its validity and reliability. The full scale is not available online, and upon contacting the author, only the scale’s items were provided, not the entire research paper. Since the primary author is retired, he could only share a copy of the scale via email. This limitation underscores the importance of further research and validation efforts to enhance the scale’s utility in assessing the complex interplay of emotions, beliefs, and behaviors in individuals with family members facing severe mental illness.
SAT-FAM, a 30-item stigma assessment tool, has been developed for family members of individuals with mental illness using a phased study approach. The three phases involved conceptualization and analysis of stigma toward family caregivers in Phase I, development of the preliminary version of the scale in Phase II and testing the psychometric properties of the final version in Phase III (4 themes emerged: shame and discrimination—7 items, α = .92; social interaction—9 items; α = .89; emotional reaction—8 items; α = .88; avoidant behaviors—6 items; α = .87). Administered among an Iranian sample, this tool serves the crucial purpose of identifying specific problems, needs, resources, and strengths of family caregivers, facilitating a targeted approach to address stigma. While SAT-FAM is valuable in understanding stigmatized experiences, it is essential to note certain limitations. Notably, the scale does not specifically target associative stigma and maintains an exploratory nature. This limitation restricts its ability to achieve full validation. Furthermore, the tool did not explore how stigma varied based on demographic and clinical characteristics of participants, making the findings less representative of the broader population. Although SAT-FAM holds potential implications for stigma reduction strategies, its efficacy remains questionable due to the lack of final validation (overall internal consistency was satisfactory being >.89).
ECI is a 66-item self-report questionnaire designed to assess caregivers’ positive and negative beliefs related to the caregiving process. Unlike other scales, the ECI is not exclusive to primary family members; rather, it encompasses anyone involved in the various stages of caregiving like relatives for individuals with Serious Mental Illness (SMI), such as schizophrenia. The ECI comprises eight negative appraisal subscales, each demonstrating strong internal consistency (overall α of the scale > .70). These subscales including (a) difficult behaviors, (b) negative symptoms, (c) stigma, (d) problems with services, (e) effects on family, (f) need to back up, (g) dependency, and (h) loss. Within these subscales, ten relatively independent dimensions were identified, with eight being negative (“difficult behaviors,” “negative symptoms,” “stigma,” “problems with services,” “effects on family,” “need to back up,” “dependency,” and “loss”) and two positive dimensions (“positive personal experiences” and “good relationship with the patient”). It is important to note that the ECI does not operate in isolation from coping mechanisms and psychological morbidity. It also challenges the traditional notion of caregiver burden, neglecting the complex interplay of factors that shape the experiences of those caring for individuals with SMI. It is crucial to acknowledge that the ECI may not fully encompass the diverse elements of stigma. This limitation can impact our understanding of how different types of stigmas contribute to the exhibited behaviors and expressions of caregivers toward their family members with SMI.
ASQR is a 9-item scale that considers caregiving burden and measures attitudes of family members toward schizophrenia, considering the three attitude components (subscales): cognitive, behavioral, and affective. It assesses the emotional reaction of relatives and caregivers who are not necessarily primary family members. It has an adequate construct validity with good internal consistency of .90, .89, and .79, respectively, for all three subscales. However, due to its administration on a small sample from Chile, the validity of the scale is weakened.
The COPMI-SQ, a 67-item scale, has four distinct subscales: experienced stigma by association, anticipated stigma by association, affiliate stigma, and structural discrimination. The internal consistency for these subscales ranges between .86 and .97. Notably, this scale is tailored for children of parents dealing with various mental disorders, including but not limited to personality disorders, PTSD, OCD, schizophrenia, pain disorders, phobias, and mood disorders. The relevance of including the COPMI-SQ in this review lies in its specific focus on the age group of 12 to 19 years. Although our review primarily focuses on psychometric properties of scales with participants aged over 18, the inclusion of this scale is justified as its target sample includes older adolescents, specifically carers aged 18 and 19 years. The uniqueness of the COPMI-SQ extends beyond its age specificity; it also delves into aspects of attached stigma experiences, particularly in cases where parents are struggling with mental health conditions. The items within the COPMI-SQ may be helpful in comprehending affiliate, experienced, structural, and anticipated stigma. While the scale responses may be influenced by the children’s own experiences of stigma, the content of the items remains pertinent.
The PIC is a 62-item scale designed to assess the psychosocial challenges faced by caregivers of individuals with mental illness. The scale was developed and tested among 340 caregivers in Assam, India. The PIC demonstrated strong psychometric properties, including an internal consistency (Cronbach’s α) of 0.88. Confirmatory factor analysis (CFA) supported the scale’s structural validity, with the average variance extracted (AVE) exceeding 0.50, indicating acceptable convergent validity. Discriminant validity was established as the square root of the AVE was greater than the inter-factor correlations. However, it may have limited generalizability to other cultural or geographic contexts and lacks a test–retest reliability or changes in psychosocial challenges over time. Moreover, it does not explicitly assess family context or associative stigma. Finally, demographic and clinical characteristics of participants were not fully analyzed in relation to scale scores, limiting understanding of how psychosocial challenges may vary across subgroups of caregivers.
Measures for Service Users (Considered Service Users as Members Embedded Within Families)
ISMI, MCESQ, and Stigma scale are for measuring stigmatized experiences among service users having mental illness, but not their family members. These scales have been included here in this review as the items can be modified and adapted into ones appropriate for family members. For example, item like “I feel comfortable being seen in public with an obviously mentally ill person” under the stigma resistance section of ISMI can also be used in reference to address family member. Similarly, question like “people have been understanding of my mental health problems” can be modified into “People have been understanding of my family member‘s mental health problem” and “People have avoided me because of my family members” mental health problems,’ etc.
The ISMI is a 29-item questionnaire that evaluates the subjective experience of stigma among psychiatric outpatients, covering alienation, stereotype endorsement, perceived discrimination, social withdrawal, and stigma resistance. It has high internal consistency, with a reliability coefficient of .90. The term “mental illness” is used throughout, but respondents are encouraged to interpret it personally. Due to reliability issues with the stigma resistance subscale, a 24-item version was created, showing improved psychometric properties with an internal consistency of .91 and a test–retest correlation of .73. However, concerns exist about the scale’s generalizability due to the skewed sample, predominantly women, and a lack of diversity in ethnicity, race, and socioeconomic status. Further refinement is needed to enhance its applicability across a more diverse population, ensuring a more balanced representation and improving the scale’s robustness in assessing self-stigma.
MCESQ is a 26-item measure assessing attitudes and experiences of consumers (service users having schizophrenia) themselves with two subscales (stigma and discrimination). This is the modified version of the original scale introduced by Wahl (1999). Terms like “consumers” have been replaced with “persons with mental illness” and “persons who use psychiatric services” to make it more appropriate to the context. Internal consistency of the scale was .88, but the scale lacked thorough validation that may limit the interpretation of findings acquired through this scale.
Finally, the stigma scale is a 28-item questionnaire assessing stigmatized experiences and views of service users of mental illness with three subscales (discrimination, disclosure, and positive aspects). The psychometric properties of the scale indicate a good internal consistency of .87 but lack further psychometric validation through CFA or other appropriate statistical validation tools. While most of the scales have undergone assessment within clinical settings and have been limited to exploratory factor analysis, rather than the confirmatory stage.
Co-Design
Among the available stigma scales used with families, few were developed with clear, documented involvement of caregivers, relatives, or lived-experience groups. The strongest examples are the Self-Stigma in Relatives of people with Mental Illness (SSRMI), which was developed directly from interviews and cognitive testing with first-degree relatives, and the Stigma Assessment Tool for Family Caregivers (SAT-FAM), which similarly drew its initial item pool from qualitative interviews with caregivers of people with mental illness. The Children of Parents with Mental Illness Stigma Questionnaire (COPMI-SQ) also incorporated participatory methods, including comprehensibility testing with children and adolescents who have a parent with mental illness, and the Internalized Stigma of Mental Illness (ISMI) scale involved service-user input during development, although it is not caregiver-focused.
For a substantial group of widely used scales, we have no evidence that caregivers, family members, or lived-experience representatives contributed to their design. This includes instruments such as the Affiliate Stigma Scale (ASS), Self-Stigma Inventory for Families (SSI-F), Family Stigma Stress Scale (FSSS), Devaluation of Consumer Families Scale (DCFS/DCFS-TW), Stigma by Association Scale (SBA), Modified Consumer Experiences of Stigma Questionnaire (MCESQ), Stigma Scale, Experience of Caregiving Inventory (ECI), Attitudes toward Schizophrenia Questionnaire for Relatives (ASQR), and the Psychosocial Inventory of Caregivers (PCI).
Discussion
We examined the psychometric properties of scales that tap into the construct of stigma experienced by carers/family members. The term “stigma” was used broadly, covering various types except for professional and institutional stigma. We sought to identify measures of mental illness-related stigma in the context of family life. We found that current scales have limited applicability in this area for the following reasons: (a) in most scales, the few family-related items tend to be peripheral rather than the focus of investigation; (b) mental illness is considered as a undifferentiated generic concept rather than recognizing that disorders are accompanied by different symptoms, behaviors and levels of severity, which may impact on others and influence their responses.
For most measures used for family-context stigma, the development papers do not record stakeholder involvement, focusing solely on psychometric testing without detailing any co-design or participatory processes. Consequently, few scales in this domain were created with explicit family involvement. Without an emic understanding of the lived experience of stigma in families, confidence that such scales capture the full dimensional range of caregiving in SMI tends to be undermined. Most of the scales reviewed here fall into a conventional perspective of families as “victims” of public attitudes and beliefs, generally responding to social stigma through shame and concealment, but neglecting the more challenging aspects of living with SMI in the family milieu. Not only can family members be hurt by social responses to mental illness, but they also translate and reinforce these attitudes and beliefs into negative behavior in the family.
While evidence on health and social benefits of appropriate family support for people with a mental disorder can be traced back to the 1950s, concepts such as Expressed Emotion only started being fully explored in the 1980s. As a construct, EE comprises criticism, hostility, and emotional over-involvement by caregivers in the families of people with psychosis and is observed to predict symptom relapse and poor outcomes (Leff & Vaughn, 1985). Once acknowledged, research on psychoeducational interventions for families emerged in a range of contexts (Claxton et al., 2017; Leavey et al., 2004). Moreover, it is seldom acknowledged that families may hold stigmatizing social beliefs and attitudes about mental illness prior to diagnosis. Our own research on families and suicide noted that some families held stigmatizing views on psychiatry and services, which prevented appropriate help-seeking prior to suicide (Leavey et al., 2017). In addition, families may also respond negatively to a mentally ill family member due to emotional or financial strain and the lack of adequate medical, educational, and social support. Thus, many families with depleted resources use maladaptive coping mechanisms, which may easily be interpreted as stigmatizing.
Highlighting the challenges that can occur within families should not be perceived as blaming families or undermining the extraordinary support that most provide; rather, we argue that research on stigma in families often ignores the complexity found within families that develop within different social, cultural and educational backgrounds, the various knowledge, skills and experiences that influence dispositions and responses toward mental illness and the treatment of family members who become ill.
In recent years, qualitative approaches have increasingly informed the development of multi-method assessment toolkits, incorporating self-report measures, behavioral assessments, and psychological indicators (Blascovich et al., 2001; Greenwald et al., 1998). This development is important given that stigma operates through both automatic, implicit responses and more deliberate, controlled reactions (Pryor et al., 2004).
There is a need therefore for a multi-dimensional scale capable of assessing the various types of stigma experienced within the familial context, for both service users and their family members. This should be developed in consultation with carers, service users with lived experience, researchers, and clinicians, combining newly created items with adapted items from existing scales to capture the full spectrum of stigma experienced by family members and carers.
Limitations
Despite the expanded search strategy, it remains possible that some relevant gray literature was not captured due to the substantial inconsistency and evolution of terminology used to describe stigma experienced by family members (e.g., courtesy stigma, secondary stigma, associative stigma). This lack of definitional consensus is a recognized issue in stigma research and presents an inherent challenge for systematic searching. While considerable effort was made to mitigate this through the inclusion of a broad range of search terms, the possibility of omission cannot be fully eliminated and should be considered when interpreting the findings.
Our inclusion criterion requiring a lived experience of a SMI for more than 2 years may have excluded early-stage caregiving experiences, including stigma emerging at the point of first symptoms or pre-diagnosis. This timeframe was selected to ensure diagnostic stability and to allow sufficient time for stigma manifestations to unfold and become observable within family relationships, which is often a gradual, cumulative process. While this criterion reduced heterogeneity in the sample, it may nevertheless have limited our ability to capture the initial development and early evolution of stigma within families. Future research would benefit from examining stigma trajectories from the prodromal phase through to longer-term caregiving.
Including anxiety and eating disorders while excluding substance use disorders and autism spectrum conditions may appear inconsistent with some broader definitions of SMI. However, in most clinical and research contexts, SMI refers to psychiatric conditions marked by significant emotional, cognitive, and behavioral disturbance with substantial functional impairment, including major mood disorders, psychotic disorders, and, in some classifications, severe anxiety and eating disorders (American Psychiatric Association [APA], 2013; National Institute of Mental Health [NIMH], 2022). Autism spectrum disorder is classified as a neurodevelopmental condition, characterized by lifelong differences rather than an episodic or deteriorating course, and the stigma associated with it therefore operates in qualitatively different ways (Lai et al., 2014). Substance use disorders, while also highly stigmatized and burdensome for families, are grouped within a separate category of addictive disorders with distinct mechanisms and treatment pathways (APA, 2013; Livingston et al., 2012). The exclusion of autism spectrum and substance use disorders was therefore based on these diagnostic and conceptual distinctions, not on any judgment of their importance.
Conclusion and Recommendations
Future instruments assessing family-context stigma should address interrelated domains, including internalized family beliefs, enacted stigma within interactions (e.g., criticism and overprotection), anticipated judgment and social withdrawal, relational strain and role changes, and protective processes such as advocacy and coping. A combination of item formats, such as self-report, multi-informant or dyadic, and scenario-based, may best capture both explicit and implicit responses. To date, there are no well-validated scales that have been (a) developed with families and people with lived experience and (b) capture the complexity of family circumstances and responses to mental illness. In the interim, existing measures may be used cautiously, while future scale development should be grounded in family systems theory and co-produced with family members.
Footnotes
Acknowledgements
The authors acknowledge support from the Challenging Health Outcomes/Integrating Care Environments (CHOICE) project and from UK Research and Innovation (UKRI), whose support contributed to the development of this research.
Author Contributions
Study conception, material preparation, data collection, data extraction, analysis, and drafting of the manuscript were performed by OG. Study conception, design, critical revision, and contributions to drafting were performed by GL and FF. Critical revisions and review were performed by NR, SEL, and PCG. All authors read and approved the final manuscript.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This review was conducted as part of the first author’s PhD project, for which Ulster University has awarded a Vice-Chancellor's Research Scholarship.