
Abstract
We examined the operationalization of psychopathy through a multi-method framework in a community sample of 250 participants, who were oversampled for psychopathic traits. Psychopathy was operationalized through clinician-rated measures, including the Psychopathy Checklist: Screening Version and the Comprehensive Assessment of Psychopathic Personality (CAPP): Symptom Rating Scale, as well as the Triarchic Psychopathy Measure and the CAPP-Self Report. Using Exploratory Structural Equation Modeling and controlling for self-report and clinical rating method variances, a four-factor model of psychopathy emerged with factors representing Boldness, Disinhibition, Affective, and Interpersonal traits. We examined the validity of the four-factor model by investigating associations between each factor and conceptually relevant scales, and the results generally supported construct validity. The Interpersonal factor was considered to contribute to the model theoretically in the factor analysis, but the incremental validity of this factor above and beyond the Boldness and Affective factors was not supported by available criterion measures.
Keywords
Researchers have studied psychopathy extensively over the past century, with research intensifying over the past five decades (Patrick, 2018). Yet, it is a multifaceted construct with many complicated nuances that we are still working toward understanding. One way to simplify is to use a factor structure to combine many correlated traits into a broader, higher-order structure. Many theoretical models and measures of psychopathy have been proposed, emphasizing different underlying domains. So, having a robust structure of psychopathic traits that generalizes across models is essential to our understanding and further progress in studying and assessing it. Delving into exhaustive details of all available models and operationalizations of psychopathy is beyond the scope of this article, but we will provide a review of well-established factor structures, including those in our analysis.
Psychopathy Factor Structure
Two-Factors
The Psychopathy Checklist-Revised (PCL-R; Hare, 1991, 2003) has been extensively studied and is widely considered the best-validated method for assessing psychopathy, with other measures more recently gaining popularity to a similar degree. Consequently, much research (especially early research) on the factor structure of psychopathy has come from studies on the PCL-R, and there have been decades of debate about the most appropriate structure. Hare (1991) developed the PCL-R which initially represented a two-factor structure of psychopathy (Harpur et al., 1988, 1989), with Factor 1 portraying affective (lack of remorse or guilt, shallowness of emotions, callousness, and failure to accept responsibility for own actions) and interpersonal traits (grandiose sense of self-worth, superficial charm, pathological lying, and manipulativeness), and Factor 2 outlining behavioral facets of antisocial behavior (early behavioral problems, juvenile delinquency, poor behavioral control, revocation of conditional release, and criminal versatility) and impulsive lifestyle (parasitic, lack of realistic long-term goals, need for stimulation, impulsivity, and irresponsibility). Levenson et al. (1995) even suggested that this structure represents primary (Factor 1) and secondary (Factor 2) subtypes (Karpman, 1941) of psychopathy; though this perspective is not universal (e.g., Hicks & Drislane, 2018).
While researchers have often considered the affective-interpersonal traits of psychopathy as “true” or the “core” of psychopathy, disinhibition-behavioral aspects of the disorder are also significant in the construct and are evident in most psychopathy conceptualizations (see Berg et al., 2017; Sellbom & Drislane, 2021; Sörman et al., 2016). Measures developed subsequent to the early prominence of the PCL-R have often been influenced by it, with some incorporating affective-interpersonal and disinhibition-behavioral traits as two separate factors. However, there have been efforts made to operationalize psychopathy without the influence of the PCL-R to avoid the measure becoming synonymous with the construct (Skeem & Cooke, 2010).
Three Factors
Cooke and Michie (2001) proposed a three-factor structure of psychopathy through research on the PCL-R, including interpersonal, affective, and behavioral facets, which used 13 of the 20 PCL-R items. Their factor structure separated the original Factor 1 into separate interpersonal and affective factors, and Factor 2 was shortened by removing items involving criminal behavior. Research on the Levenson Self-Report Psychopathy Scale (Levenson et al., 1995), which has also been published with an original two-factor structure, has extensive support for a three-factor model that aligns closely with Cooke and Michie’s (2001) model of the PCL-R (see Dickison & Sellbom, 2023 for review). Three conceptual domains have also been evident in contemporary models and operationalizations of psychopathy.
The Triarchic Psychopathy Measure (TriPM; Patrick, 2010) was developed from the triarchic model (Patrick et al., 2009), a theoretical model of psychopathy that involves three domains: Boldness, Meanness, and Disinhibition. However, this conceptual three-domain structure has mostly failed to be represented and confirmed statistically in the TriPM. Other measures operationalizing the triarchic model support factor solutions between 5 and 7 that indicate a better fit in some populations (Collison et al., 2021). Moreover, the Comprehensive Assessment of Psychopathic Personality (CAPP; Cooke et al., 2004) is a theoretical model of psychopathy that incorporates six conceptual domains: Attachment, Behavioral, Cognitive, Dominance, Emotional, and Self. Researchers have found that a three-factor structure best represents the self-report version of the CAPP (Sellbom et al., 2019) that includes Affective (Antagonism/Meanness), Interpersonal (Fearless Grandiosity), and Behavioral (Disinhibition) domains, supported by further research (e.g., Sellbom, Liggins, et al., 2021).
In addition, a three-factor structure of psychopathy has been endorsed in the Psychopathic Personality Inventory-Revised (PPI-R; Lilienfeld & Widows, 2005). The PPI-R is a well-validated operationalization of psychopathy, initially comprising eight subscales that loaded onto two higher-order factors: Fearless Dominance and Self-centered Impulsivity (Benning et al., 2003; Lilienfeld & Widows, 2005), with the orphaned subscale Coldheartedness frequently failing to load onto either of the higher-order factors, indicating that a three-factor model best represents the PPI-R; Fearless Dominance, Self-centered Impulsivity, and Coldheartedness.
Four Factors
Although Cooke and Michie’s (2001) three-factor model of the PCL-R has gained support throughout the literature, it has also been heavily disputed (Hare, 2003; Hare & Neumann, 2008, 2010; Neumann et al., 2005; Vitacco, Rogers, et al., 2005), and a four-factor model has gained extensive traction. Hare and Neumann (2005) proposed a four-factor model of psychopathy from the PCL-R: Interpersonal, Affective, Lifestyle, and Antisocial. Of note, their four-factor model is identical to Cooke and Michie’s (2001) three-factor model, except that the fourth factor consists of the antisocial items that were removed in the latter analysis. The four-factor structure has been confirmed in a variety of populations (e.g., Hare & Neumann, 2005; Hill et al., 2004; Kosson et al., 2002, 2013; Neumann et al., 2006, 2012, 2013; Olver et al., 2013; Vitacco, Neumann, et al., 2005; Vitacco, Rogers, et al., 2005).
Although this research reflects a major debate about which model best represents the PCL-R, this is only one operationalization of psychopathy, and its research literature cannot generalize psychopathy from all perspectives. Furthermore, research on other operationalizations of psychopathy has also suggested a four-factor model of psychopathy. For example, the Elemental Psychopathy Assessment (Lynam et al., 2011) was developed to operationalize psychopathy within the framework of the Five-Factor Model of personality (Lynam & Miller, 2015) and has supported a four-factor structure of Antagonism, Emotional Stability, Disinhibition, and Narcissism (Few et al., 2013; Lee & Sellbom, 2021; Liggins & Sellbom, 2022), though this structure does not fully map onto the four-factor structure of the PCL-R.
Summary
Overall, there is no clear consensus on the most overall appropriate structure of psychopathic personality traits when considering its various conceptualizations and associated operationalizations. It depends on the theoretical and empirical perspective taken in any given study. Although researchers should use multiple measures and consider different perspectives to ensure development in an area (Iliescu et al., 2024), it does increase difficulty in comparing results.
Current Study
To better understand the underlying structure of psychopathy, we used Exploratory Structural Equation Modeling (ESEM) to investigate the factor structure through a multi-trait multi-method design. Specifically, we aimed to elucidate a unified structure of psychopathy based on measures that cover a range of theoretical perspectives. We also aimed to investigate the construct validity of the best model by examining associations with conceptually relevant criterion variables.
We used ESEM to determine the latent factor structure of multiple psychopathy measures administered via numerous assessment modalities (e.g., self-report and clinician-rated). Due to our multi-method approach, we needed to model method factors to control for shared method variance (account for method effects and errors specific to modalities), which can be done within the confirmatory framework of ESEM.
We expected the possible factor structure to range from two to six factors, aligning with common operationalizations and theoretical perspectives of psychopathy. The aforementioned models were derived by investigating psychopathy in the same modality (i.e., self-report or clinician-rated). At the time of this study, only one prior study had, to our knowledge, investigated the factor structure of psychopathy using multimodal approaches. Hare (1985) investigated clinician ratings and self-report inventory scores to determine the agreement between the various measures and modalities and investigated factor loadings onto a two-factor model of psychopathy. The results of a principal-components analysis with varimax rotation indicated that the clinician-rated measures and self-report measures loaded distinctively from each other onto different factors. However, the author did not consider the impact of shared method variance, which made their results noncomparable to the current study. Overall, within the framework of psychopathy, for which there is some indication of the possible factor structure but no firm a priori hypotheses, we considered the ESEM method appropriate to investigate the underlying structure of a multimodal assessment whereby we can control for method variance.
We next investigated the construct validity of the optimal structure identified by examining the factors’ associations with conceptually relevant criterion variables from the Minnesota Multiphasic Personality Inventory-3 (MMPI-3; Ben-Porath & Tellegen, 2020), the Personality Diagnostic Questionnaire-Version 4 (PDQ-4; Hyler, 1994) antisocial personality disorder (ASPD) scale, and the Antisocial Behavior Questionnaire (ABQ; Sellbom et al., 2012). We would expect psychopathy factors reflective of disinhibition/behavioral traits to be positively associated with antisocial personality disorder symptoms and antisocial behavior due to the long-standing association between psychopathy and these constructs (Neumann et al., 2015; Waldman et al., 2018).
We expected the following associations with the MMPI-3 scales: positive associations with externalizing dysfunction (BXD), aggressiveness (AGGR) and aggression (AGG), antisocial behavior (RC4), impulsivity (IMP), substance abuse (SUB), juvenile conduct problems (JCP), disconstraint (DISC), dominance (DOM), self-importance (SFI), cynicism (CYN), hypomanic activation (RC9), and anger proneness (ANP; Wygant & Sellbom, 2024). Psychopathy has also been frequently associated with unemotionality, social boldness, and dominance (see Lilienfeld et al., 2018 for review), therefore, we also expect negative associations with the psychopathy factors and the MMPI-3 scales representing negative emotionality/neuroticism (NEGE), introversion/low positive emotionality (INTR), shyness (SHY), social avoidance (SAV), disaffiliativeness (DSF), emotional/internalizing dysfunction (EID), low positive emotions (RC2), anxiety-related experiences (ARX), fearfulness (behavior-restricting fears; BRF), demoralization (RCd), self-doubt (SFD), inefficacy (NFC), and stress (STR) reactivity (Wygant & Sellbom, 2024). See Table 1 for a summary of hypothesized associations.
Hypothesized Associations Between Psychopathy and Conceptually Relevant MMPI-3 Scales.
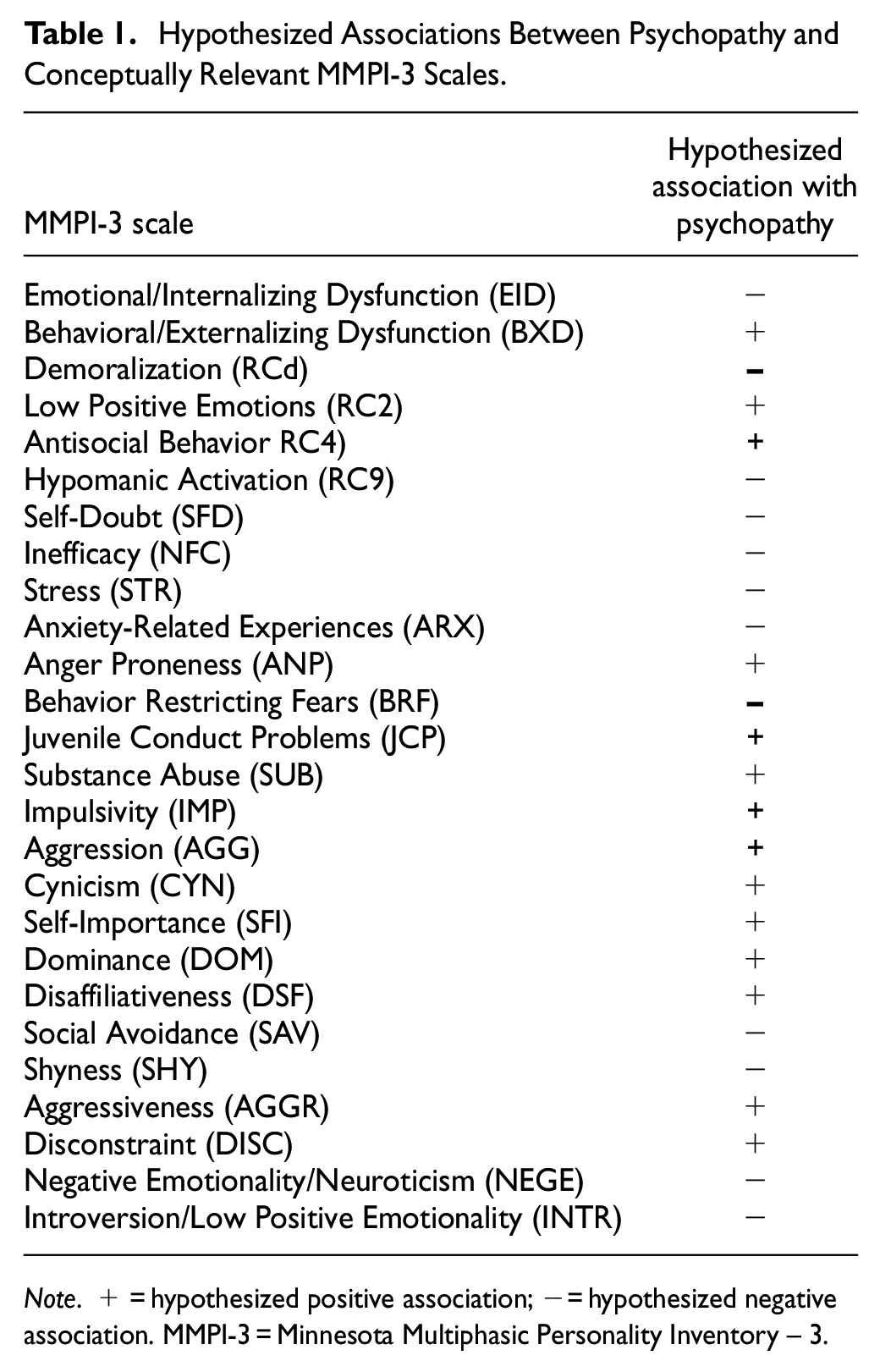
Note. + = hypothesized positive association; − = hypothesized negative association. MMPI-3 = Minnesota Multiphasic Personality Inventory – 3.
Methods
This study was not preregistered. We report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study.
Participants
Participants comprised 250 individuals from a community sample (ages 18–53 years, 54% male, 45% female, 0.9% Nonbinary). Ethnicity represented a generic New Zealand community sample; 65% NZ European, 17% Other European, 14% Māori (the indigenous population of New Zealand), 12% Asian, 8% Pacific Islander, and 7% Other Descent. Recruitment focused on individuals with externalizing traits to increase the likelihood of psychopathic traits as part of a larger project that focused on investigating the association between neural indicators and psychopathy. Of the 250 participants recruited, 19 participants were excluded due to deviant or inconsistent responses on the MMPI-3 (Ben-Porath & Tellegen, 2020) profiles based on scores on Cannot Say ≥15, Combined Response Inconsistency, variable response inconsistency, or true response inconsistency ≥80T, and/or infrequent response (F) or infrequent psychopathology responses (Fp) ≥100T—with the final sample consisting of 231 participants. The University of Otago Ethics Committee (Health) issued ethics approval (approval number: H20/037).
Measures
Descriptive statistics and reliability coefficients for each scale score are reported in Table 2.
Reliability Coefficients for all Scale Scores.
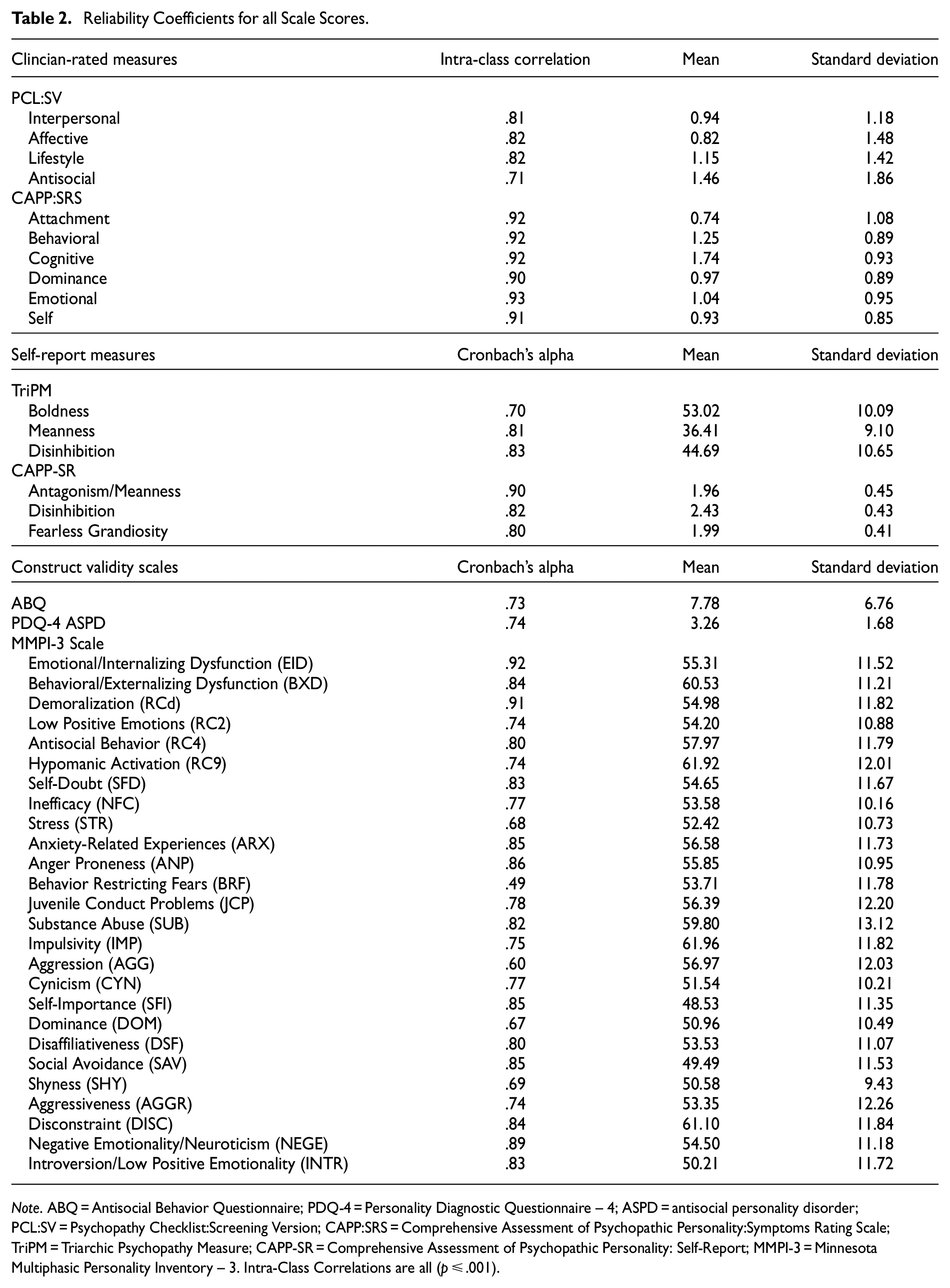
Note. ABQ = Antisocial Behavior Questionnaire; PDQ-4 = Personality Diagnostic Questionnaire – 4; ASPD = antisocial personality disorder; PCL:SV = Psychopathy Checklist:Screening Version; CAPP:SRS = Comprehensive Assessment of Psychopathic Personality:Symptoms Rating Scale; TriPM = Triarchic Psychopathy Measure; CAPP-SR = Comprehensive Assessment of Psychopathic Personality: Self-Report; MMPI-3 = Minnesota Multiphasic Personality Inventory – 3. Intra-Class Correlations are all (p ≤ .001).
Psychopathy Checklist: Screening Version
Hart et al. (1995) developed the Psychopathy Checklist: Screening Version (PCL:SV) for use as a semi-structured interview to provide the basis for clinical ratings of psychopathic traits. The PCL:SV is a 12-item instrument designed to reflect the same factor structure as the PCL:R (Hare, 2003); however, it can be used outside of forensic populations and is more time-effective than the PCL-R. Each item is scored on a 3-point scale, with total scores ranging from zero to 24. For research purposes, a threshold of 18 is often used to indicate a significant presence of psychopathic traits (Hare et al., 2018). The PCL:SV has extensive support for reliability and construct validity and is comparable to the PCL-R (see Higgs et al., 2018 for review). The PCL:SV includes two main parts, which can be divided into the four original PCL factors: Interpersonal, Affective, Lifestyle, and Antisocial. The interpersonal and affective factors load onto a high-order factor akin to primary psychopathy. In contrast, the Lifestyle and Antisocial factors load onto a higher-order factor akin to secondary psychopathy.
Comprehensive Assessment of Psychopathic Personality: Symptom Rating Scale
The Comprehensive Assessment of Psychopathic Personality: Symptom Rating Scale (CAPP-SRS; Cooke et al., 2012) uses a semi-structured clinical interview to allow the administrator to make clinical judgments on each of the 33 CAPP symptoms (Cooke et al., 2004; Cooke & Logan, 2018). The CAPP:SRS traditionally incorporates file information and staff rating forms in symptom ratings. However, the current study used only the CAPP—Clinical Interview to derive ratings of CAPP symptomology due to the research carried out in a community population. The CAPP involves six domains: Attachment, Behavioral, Cognitive, Dominance, Emotional, and Self. The CAPP:SRS has been associated with other psychopathy measures, including the PCL-R (e.g., Cooke et al., 2022).
Triarchic Psychopathy Measure
Patrick (2010) developed the TriPM to assess the triarchic conceptualization of psychopathy: Boldness, Meanness, and Disinhibition (Patrick et al., 2009). The TriPM consists of 58 items rated on a four-point Likert scale where the respondent is required to rate how much each item applies to them. The TriPM has correlated as conceptually expected with psychopathy measures, including the PCL and the CAPP-Self Report (CAPP-SR; Sellbom et al., 2019) (see Sellbom et al., 2018 for review).
CAPP-Self Report
The CAPP-Self Report (CAPP-SR; Sellbom et al., 2019) is a 99-item instrument whereby participants rate how much each item applies to them on a four-point scale. The CAPP-SR was developed to operationalize the CAPP theoretical model of psychopathy, encompassing 33 key symptoms. Therefore, the CAPP-SR allows for measurement of the CAPP in self-report format and permits further research into the factor structure, validity, and reliability of the CAPP as a model of psychopathy. The CAPP-SR is a relatively new measure, however, it has substantial support for reliability and construct validity, including associations against a range of other psychopathy measures (Liggins & Sellbom, 2022; Sellbom et al., 2019; Sellbom, Laurinaitytė, et al., 2021; Sellbom, Liggins, et al., 2021; Shou et al., 2021). A three-factor model best represents the underlying symptom structure and was used in the current study: Antagonism/Meanness, Disinhibition, and Fearless Grandiosity (Sellbom, Liggins, et al., 2021). The CAPP-SR factor scales are the average scores of the individual symptom scales that load meaningfully on each factor (see Sellbom, Liggins, et al., 2021).
Minnesota Multiphasic Personality Inventory-3
The MMPI-3 (Ben-Porath & Tellegen, 2020) is a 335-item, self-report broadband measure of personality and psychopathology. The MMPI series of instruments is extensively validated, with normative data from a general community sample, and validated to map onto contemporary theories of psychopathology and maladaptive personality (Ben-Porath & Sellbom, 2023). The 335 items of the MMPI-3 aggregate onto ten validity scales and 42 substantive scales that are organized hierarchically. Participants rate the MMPI-3 statements as true or false as applied to them. The current study used the following conceptually relevant scales of the MMPI-3 to determine validity: EID, BXD, RCd, RC2, RC4, RC9, SFD, NFC, STR, ARX, ANP, BRF, JCP, SUB, IMP, AGG, CYN, SFI, DOM, DSF, SAV, SHY, AGGR, DISC, NEGE, INTR; see Table 1 for full scale names.
Antisocial Behavior Questionnaire
The ABQ (Sellbom et al., 2012) is a 16-item self-report inventory whereby the participant is required to rate whether they have engaged in behaviors that are considered to be criminal (e.g., drug-related offenses, theft, assault, and vandalism) on a 3-point scale (no, yes—but only once, yes—more than once). The ABQ is a version of a self-report measure of delinquency (Hirschi et al., 1980; Lynam et al., 1999) modified by Sellbom et al. (2012) to sample antisocial behavior in community and prison populations.
Personality Diagnostic Questionnaire-Version 4
The PDQ-4 (Hyler, 1994) is a 99-item true/false self-report measure outlining the Diagnostic and Statistical Manual-Fourth Edition (American Psychiatric Association, 1994) criteria for personality disorders. The current study used only the 22-item ASPD scale of the PDQ-4. The items (1 = true, 0 = false) were added to calculate total scores.
Procedure
This study was part of a larger project investigating the relationship between psychopathy and neural indicators. Participants were asked to complete a battery of self-report measures (which included two psychopathy measures) while an experimenter fitted an electroencephalogram (EEG) cap before completing a series of EEG tasks delivered via the computer. Participants were then administered a semi-structured interview (which included two clinician-rated psychopathy measures) by a highly trained research assistant enrolled in (or completed) a clinical psychology program under the supervision of a registered clinical psychologist. There were four separate research assistants responsible for clinical ratings. Therefore, we investigated the consistency of agreement between raters to ensure that ratings were sufficiently reliable. Inter-rater reliability was calculated from a small subsample (n = 25) where two clinical research assistants independently rated participants based on the available interview information. Intra-class correlations were then calculated for each clinician-rated measure (see Table 2) through a two-way random model (absolute agreement). Participants received a NZD $75 supermarket voucher, and up to NZD $10 in cash in winnings from the EEG tasks that were part of the broader project (measures not used in this study).
Data Analysis
Data Preparation and Model Specification
ESEM in Mplus Version 8 (Muthén & Muthén, 1998/2017) was used for model evaluation using the maximum likelihood with a robust scaling estimator. Missing data were estimated via full-information maximum likelihood. We specified models with one, two, three, four, five, and six latent factors, respectively, representing distinct facets of psychopathy in each analysis. Because we used ESEM, all indicators loaded on each substantive factor were rotated to a simple structure through the default oblique geomin method. Latent factors were permitted to correlate to estimate associations between resulting psychopathy domains. For each model, we also specified two method factors representing the shared self-report and clinical rating variances, respectively, which were orthogonal to the trait factors.
Fit Indices, Model Evaluation, and Factor Loadings
The most appropriate model was determined by considering model fit indices, focusing on the Comparative Fit Index (CFI), Tucker-Lewis Index (TLI), Root Mean Square Error of Approximation (RMSEA), and Standardized Root Mean Square Residual (SRMR). CFI and TLI compare the model fit to a null model, with values close to 1.0 indicating a good fit (Hu & Bentler, 1999; Kline, 2023). RMSEA considers the difference between the model prediction and what is observed in the data while accounting for degrees of freedom and sample size. A lower RMSEA, closer to zero, indicates a better fit (Hu & Bentler, 1999; Kline, 2023). SRMR assesses the standardized overall difference between predicted and observed covariances, with lower values indicating a better fit (Hu & Bentler, 1999; Kline, 2023). Although we used conventional thresholds to evaluate model fit (CFI, TLI ≥0.90; RMSEA, SRMR ≤0.08), we also placed a high premium on theoretical considerations in model evaluations (Sellbom & Tellegen, 2019). For this study, we considered factor loadings of
Construct Validity
First, the final scores of the four-factor model were extracted from Mplus Version 8 and entered into IBM SPSS (IBM Corp, 2021) for further study. Next, we calculated zero-order correlations between the four factors and all conceptually relevant measures. We interpreted correlations as effect sizes based on Cohen’s (1992) recommendations and considered a medium effect size (r ≥ |.30|) as meaningful. Because resulting factors were expected to be correlated, we also conducted separate latent regression analyses in cases where more than one psychopathy factor was meaningfully correlated with a conceptually relevant scale to determine which psychopathy factor uniquely contributed to each prediction.
Results
Factor Analysis
Correlations between all variables included in the factor analysis are available in Table S1. We estimated models with one to six factors. Table 3 shows the model fit indices. Models with five or six factors did not properly converge because of Heywood cases (i.e., implausible parameter values), causing non-positive definitive matrices possibly owing to multicollinearity (10/120 [8.33%] correlation pairs > .70; see Table S1) or sample size. Attempts at resolving these implausible values (e.g., setting indicator residual variances to zero) were unsuccessful. Although the RMSEA value was imperfect for the four-factor model, it was the only model with an otherwise acceptable fit, and it was theoretically congruent (i.e., classic three-factor model plus boldness), so it was retained for further construct validity analysis. See Table 4 for all factor loadings and correlations between latent factors.
Fit Indices for Psychopathy Models.

Factor Loadings and Factor Correlations.
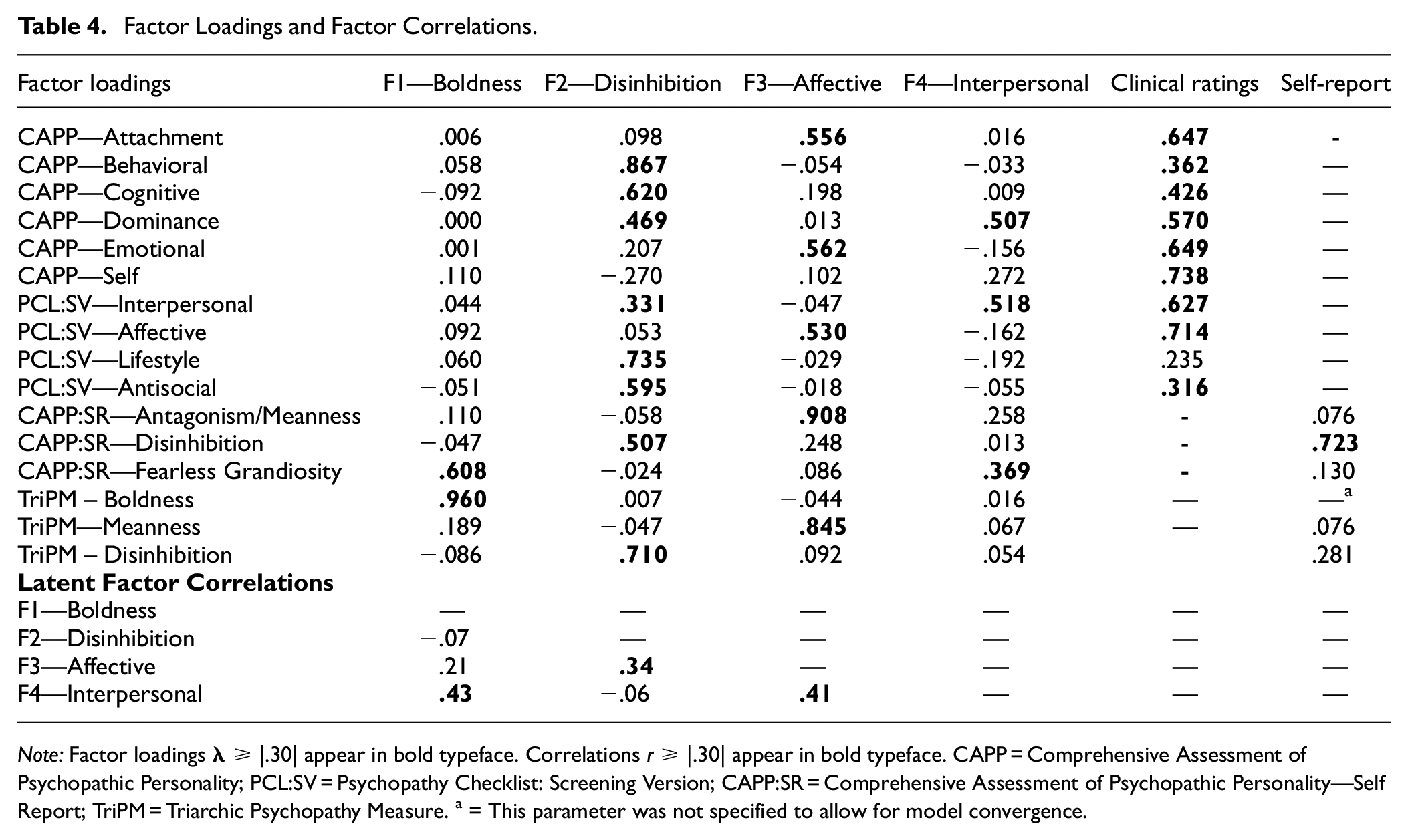
Note: Factor loadings
Factor 1 was labeled Boldness due to high loadings of CAPP-SR Fearless Grandiosity and TriPM Boldness. Factor 2 was labeled Disinhibition as CAPP Behavioral, Cognitive, and Dominance, PCL:SV Lifestyle and Antisocial, CAPP:SR Disinhibition and TriPM Disinhbition loaded preferentially. Factor 3 was labeled Affective due to the highest loadings being CAPP Attachment and Emotional, PCL:SV Affective, CAPP:SR Antagonism/Meanness, and TriPM Meanness. Factor 4 was labeled Interpersonal due to high loadings of CAPP Dominance, PCL:SV Interpersonal and also CAPP:SR Fearless Grandiosity. The method factor loadings are also represented in Table 4. It is important to note that the loadings are substantially larger for the clinical ratings compared to the self-report.
Construct Validity
Table 5 shows the correlations between the four factors and the conceptually relevant criterion measures. The Boldness factor was negatively and meaningfully correlated with MMPI-3 EID, RCd, RC2, SFD, NFC, STR, ARX, BRF, NEGE, INTR, SAV, and SHY, as expected. The Boldness factor was also positively associated with the MMPI-3 scales of AGGR, SFI, and DOM.
Correlations Between Psychopathy Factors and Conceptually Relevant Measures.
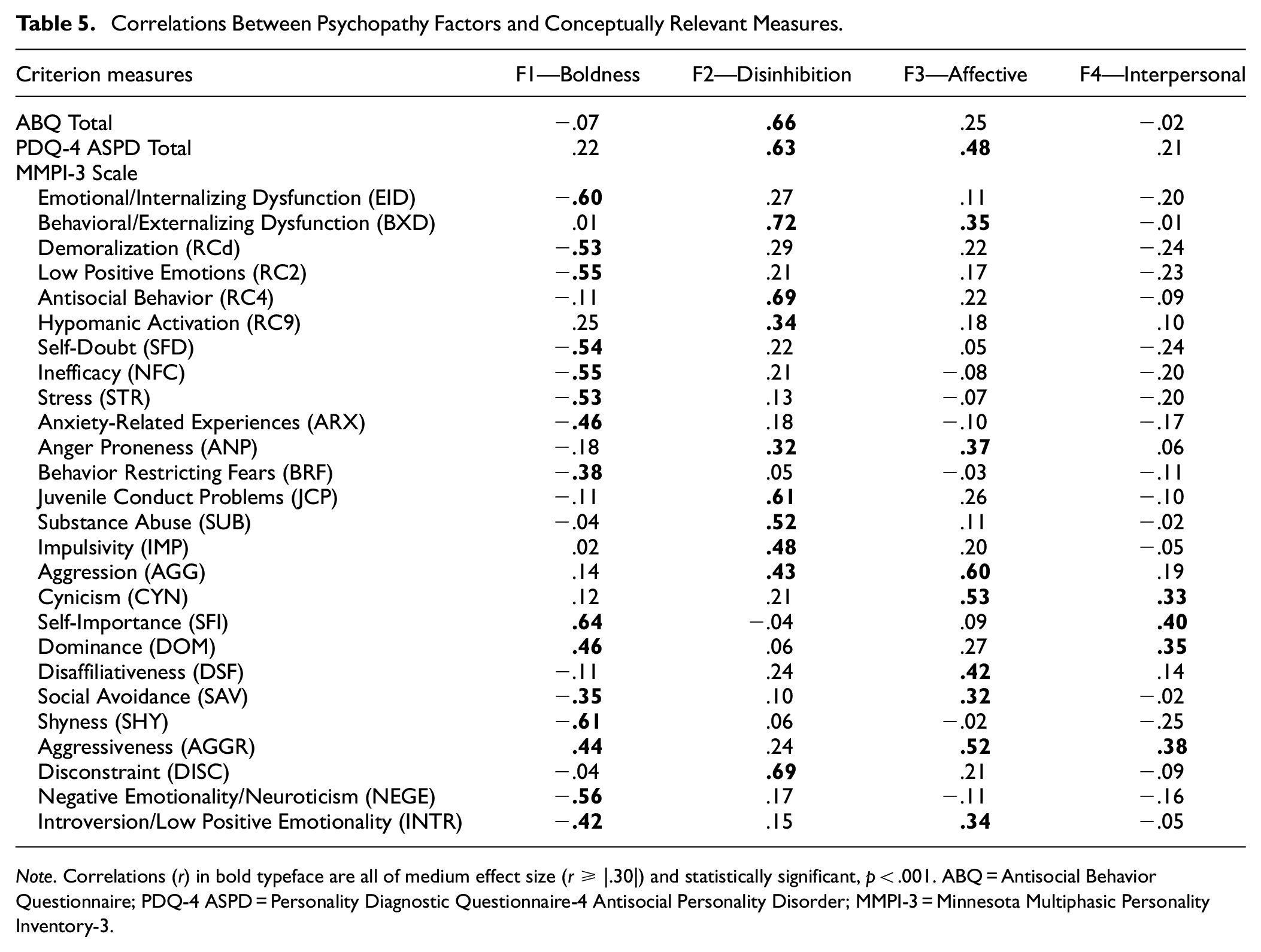
Note. Correlations (r) in bold typeface are all of medium effect size (r ≥ |.30|) and statistically significant, p < .001. ABQ = Antisocial Behavior Questionnaire; PDQ-4 ASPD = Personality Diagnostic Questionnaire-4 Antisocial Personality Disorder; MMPI-3 = Minnesota Multiphasic Personality Inventory-3.
The Disinhibition factor was positively associated with ABQ and PDQ-4 ASPD total scores, MMPI-3 BXD, RC4, RC9, ANP, DISC, JCP, SUB, IMP, and AGG.
The Affective factor was positively correlated with PDQ-4 ASPD total score, and MMPI-3 AGGR, INTR, CYN, DSF, SAV, BXD, and ANP. Finally, the Interpersonal factor was positively associated with the MMPI-3 AGGR, CYN, SFI, and DOM. These findings are consistent with previous literature and theoretical knowledge of psychopathy as discussed later.
Table 6 reports the results of linear regression analyses for latent psychopathy factors and their associations with relevant criterion measures for which there were at least two meaningful predictors in the bivariate analysis. Low Boldness uniquely predicted higher scores of INTR and EID. Conversely, high Boldness was the best predictor of MMPI-3 SFI and DOM. Disinhibition scores were the best predictor of PDQ-4 ASPD and MMPI-3 BXD. High Affective scores predicted MMPI-3 ANP, AGGR, AGG, and CYN. Moreover, Boldness and Affective factors were equally important in predicting SAV, but in opposite directions, with lower Boldness and higher Affective scores predicting this variable. It is important to note that the Interpersonal factor associations with MMPI-3 SFI and DOM appear to be due to shared variance with boldness, which had significant unique components in the prediction. In addition, the associations between the interpersonal factor and MMPI-3 AGGR and CYN appear to be due to shared variance with the Affective factor.
Linear Regression Analyses with Psychopathy Factors Predicting Scores on Criterion Measures.
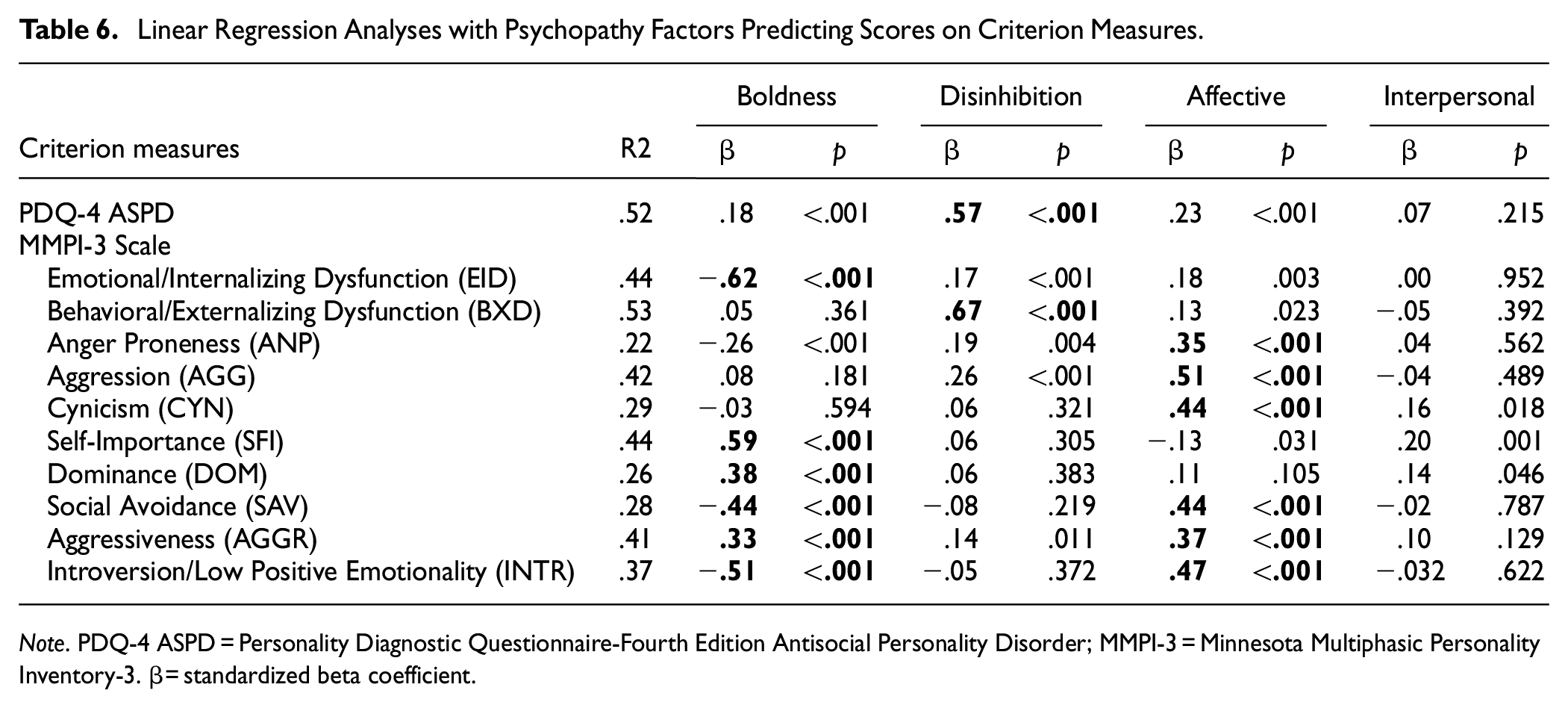
Note. PDQ-4 ASPD = Personality Diagnostic Questionnaire-Fourth Edition Antisocial Personality Disorder; MMPI-3 = Minnesota Multiphasic Personality Inventory-3. β = standardized beta coefficient.
Discussion
We aimed to investigate the underlying structure of psychopathy across a range of common measurement approaches in a community population to elaborate on the already extensive discussion in the literature about the underlying factor structure of the psychopathy construct and its associated ambiguity. Using ESEM, community sample findings indicated best model fit for a four-factor structure underlying the data. Construct validity analyses revealed that the latent factors were associated with conceptually relevant criterion variables with a pattern that made sound theoretical and intuitive sense regarding psychopathy as described in the broader literature.
Boldness
The first factor was labeled Boldness due to the predominant factor loadings and the existing literature on this psychopathy construct; these were CAPP:SR Fearless Grandiosity and TriPM Boldness. Boldness, in the scope of psychopathy, has been referred to or described as part of the psychopathy construct since the early works of Cleckley (1941) and thereafter. However, there is debate on whether boldness is central to the psychopathy construct, with some research indicating that boldness is less relevant to the broader psychopathy construct (e.g., Gatner et al., 2016; Marcus et al., 2013; Miller & Lynam, 2012; Vize et al., 2016), whereas others disagree (e.g., Berg et al., 2017; Lilienfeld et al., 2012, 2016, 2018). It should be noted that some scholars consider boldness as a differentiating factor between psychopathy subtypes, for example, higher levels of boldness constitute more “adaptive” subtypes such as primary psychopathy, noncriminal psychopathy, and subclinical psychopathy (Lilienfeld et al., 2018; Sellbom & Drislane, 2021). Thus, there is some ambiguity in findings and perspectives on the central relevance of boldness to the psychopathy construct may be due to the populations assessed and the psychopathy variants present.
The pattern of associations between the boldness factor in the current study and conceptually relevant scales revealed associations with scales articulating limited internalizing dysfunction, anxiety, and fear, coupled with emotional stability and extraversion. In addition, a sense of self importance, interpersonal dominance, and social confidence; these are quite consistent with the general construct validity evidence for boldness measures (e.g., Sellbom, 2019; Sellbom et al., 2018). Therefore, the boldness factor comprises symptoms of fearlessness, social dominance, and self-assurance, perhaps entailing the more “adaptive” features of psychopathic personality and supporting notions that this construct, at least in isolation, is not representing a pathological phenotype. However, the boldness factor was also associated with MMPI-3 Aggressiveness, which represents instrumental aggression, grandiosity, and dominance, indicating a link between boldness and interpersonal externalizing tendencies.
There will likely be continued debate on the relevance of boldness to the psychopathy construct to psychopathy, which this study will not necessarily resolve. It is noteworthy, however, that this construct does emerge as an independent domain when multiple theories and measurements of psychopathy are considered conjointly, which is consistent with past research that has also conducted conjoint analyses with different models (e.g., Liggins & Sellbom, 2022).
Disinhibition
The second factor was labeled Disinhibition, as it reflects the antisocial, impulsive, and lifestyle attributes of psychopathy. CAPP-SRS Behavioral and Cognitive domains, PCL:SV Lifestyle and Antisocial, and TriPM Disinhbition loaded preferentially onto this factor. Unsurprisingly, the Disinhibition factor in the current study correlated significantly with external criteria scales measuring antisocial and criminal behavior and externalizing scales pertaining to aggressiveness, impulsivity, and substance use. This pattern of associations is consistent with those of a range of disinhibition/behavior psychopathy scales (see Sellbom et al., 2018 for review). Moreover, the disinhibition factor in the current study aligns closely with Cooke and Michie’s (2001) behavioral style factor of psychopathy as well as the traditional Factor 2 of the PCL-R which has long-standing associations with aggression (Porter et al., 2018), antisocial behavior (Nelson & Foell, 2018), and substance use (Ellingson et al., 2018). The emergence of a disinhibition factor within a broader multi-perspective model of psychopathy is not controversial, as this domain can be located within every established theory of the disorder (e.g., Patrick et al., 2009).
Affective
The third factor was labeled Affective as it aligned with long-standing descriptions of callous-unemotional traits (in youth) and affective deficiencies of psychopathy or “meanness” (in adults) evident in the literature. CAPP Attachment and Emotional, PCL:SV Affective, CAPP:SR Antagonism/Meanness, and TriPM Meanness loaded preferentially onto this factor. Affective traits of psychopathy have long been referred to as relevant to psychopathy; indeed, there is substantial research that indicates that these traits can be considered a “core” of the psychopathy pathology (see Sellbom & Drislane, 2021 for review).
As conceptually and empirically expected, the Affective factor in the current study was influential in predicting external criteria articulating aggression, cynicism, social detachment, and antisocial behavior. Therefore, our Affective factor describes someone who is emotionally shallow, socially contemptuous, detached, exploitative, cruel, and lacking in guilt, remorse, and empathy. Such a constellation of traits is referred to as “callous-unemotional traits” in childhood (Viding & Kimonis, 2018), describes features of the classic “Factor 1” of the PCL instruments (Harpur et al., 1988, 1989), as well as primary psychopathy in the psychopathy subtype literature (Hicks & Drislane, 2018). There is little debate that affective traits are a central component of the construct of psychopathy (e.g., Sellbom & Drislane, 2021). Callous-unemotional traits present in children indicate more severe conduct and behavioral problems and indicate the development of psychopathy later in life (Frick & Marsee, 2018). Research has demonstrated associations between affective and behavioral traits of psychopathy, “callous aggression” and disinhibition in the context of broader externalizing psychopathology (Krueger et al., 2007; Patrick et al., 2013), and our Affective and Disinhibition factors were significantly correlated in our analyses.
Interpersonal
The fourth factor was labeled Interpersonal, as it describes someone who is dominant, manipulative, and deceitful in their interactions with others. CAPP Dominance and PCL:SV Interpersonal loaded preferentially onto this factor. The Interpersonal factor was correlated with conceptually relevant scales describing instrumental aggressiveness, cynicism, self importance, and dominance. However, results from linear regression analysis indicated that the interpersonal factor did not augment the other factors in associations with external criteria, which raises questions about the incremental validity of this factor; this finding could, of course, be a reflection of available criterion measures. The conflation between interpersonal and affective factors is not surprising given that operationalizations of psychopathy often refer to two-factor models: affective-interpersonal and disinhibition-behavioral (Hare, 2003; Hare et al., 2018; Harpur et al., 1988, 1989) Other external criteria may be required for further elucidation of construct validity. However, separating Affective and Interpersonal factors is indicated within the broader literature and aligns closely with Cooke and Michie’s (2001) three-factor model of psychopathy, as well as Hare and Neumann’s (2005) four-factor model.
Interpersonal deviance is often perceived as key to psychopathy (Draycott et al., 2011), with empirical operationalizations supporting this contention. For example, three- and four-factor models of psychopathy include an interpersonal factor (Cooke & Michie, 2001; Hare, 2003; Hare & Neumann, 2005), and cluster analysis studies have indicated that interpersonal traits of psychopathy assist in differentiating primary from secondary psychopathy (Swogger & Kosson, 2007; Vassileva et al., 2005). Moreover, psychopathy is associated with external factors indicative of interpersonal distress, such as failed intimate relationships (Ullrich et al., 2008), toxic work environments and violation of public trust (Gao & Raine, 2010; Mathieu et al., 2020; Neo et al., 2018), poor attachment (Blanchard & Lyons, 2016; Christian et al., 2019), and a limited number of positive relationships (Mooney et al., 2019). Therefore, we consider the interpersonal factor to be an important component of the construct of psychopathic personality.
Overall, the current factor analysis supports a four-factor structure underlying the construct of psychopathy over multimodal assessment of psychopathy. Although the incremental validity of the interpersonal factor in the current study is questionable, the four-factor model fits the data favorably and makes more conceptual sense in the scope of the overall literature. Moreover, our four-factor model aligns with Cooke and Michie’s (2001) three-factor model of psychopathy, with the addition of a separate boldness factor.
Implications
The findings of this research have important theoretical and practical implications. From a theoretical perspective, it is useful that traditional psychopathy models emerge when these are considered in conjunction. The traditional three-factor model of psychopathy elaborated via the PCL-R and its variants emerged (affective, interpersonal, and behavioral/lifestyle) along with the boldness domain. A comprehensive model of psychopathy for scientific purposes, therefore, ideally considers these four domains in the operationalization of this construct.
From a practical perspective, multi-method assessments of psychological constructs are consistent with best practices within evidence-based psychological assessments (e.g., Bornstein, 2017). In applied forensic settings, the PCL-R is predominantly used to assess the construct of psychopathy (see Hare, 2016). Although this instrument does often include multiple sources of information in ratings, thereby adhering somewhat to best practice with multimodal assessments, research on psychopathy has evolved tremendously since the initial development of the PCL-R to include multiple modes of assessments, as this study has articulated. The current study, therefore, offers unique information regarding the convergence of multimodal assessment of psychopathic personality disorder and the relation between measures. For instance, it provides some guidance in the integration of information on clinician ratings and self-report inventories. In addition, the current study relates psychopathy factors to one of the most widely used broadband self-report instruments of psychopathology and personality, the MMPI-3, adding to already growing literature regarding assessing psychopathy through the MMPI-3 (Wygant & Sellbom, 2024). Clinicians who use the MMPI-3 can take guidance from this and other literature in terms of what scale scores align with different domains of psychopathic personality based on a comprehensive perspective.
Limitations and Future Directions
The current study was the first to our knowledge to investigate the underlying factor structure of psychopathy using a multimodal, multi-trait approach while controlling for method variance, which is a strength. However, limitations must also be acknowledged. First and foremost, the sample size was relatively small for what is typically observed for large, complex models, and it is possible that this issue might have contributed to the non-convergence of the larger factor solutions (i.e., 5+). This limitation notwithstanding, the use of ESEM and hierarchical ESEM are unlikely to be heavily impacted by sample size issues (e.g., Swami et al., 2023), particularly as sample sizes below 50 participants can be appropriate for standard exploratory factor analysis (EFA) models under certain conditions (de Winter et al., 2009). Nevertheless, future research should replicate these findings with larger sample sizes.
Moreover, the current study investigated psychopathy in a community population representative of New Zealand, and while recruited for externalizing and psychopathic tendencies, the degree to which these results apply to institutionalized and other ethnic populations remains unclear. Future research must replicate these findings in various populations to determine the robustness and generalisability of the current findings. In addition, it is questionable whether our Interpersonal factor incrementally adds to the overall model above and beyond the other factors, particularly the Affective factor. Therefore, future research should use better-suited external criteria to determine any further distinction between factors. Our analysis also did not include extensive interpersonal manipulation criteria, which are key to the psychopathy construct. Future research should investigate whether the inclusion of such adds to the incremental validity of the Interpersonal factor. In addition, for construct validity analysis, the current study was constrained to measures investigating externalizing traits specific to psychopathy and related constructs. Although this meant we could investigate convergent validity effectively, it has resulted in a lack of discriminant validity analysis.
Conclusion
By considering multiple perspectives and operationalizations of psychopathy, we can better understand the construct broadly rather than through the lens of one operationalization. Importantly, this multimodal factor analysis is the first of its kind; therefore, this factor structure is tentatively proposed. Future research must consider how psychopathy presents from a multimodal approach to align with best practice, better understand psychopathy without any biases that may be associated with particular operationalizations, and work toward the resolution of the ever-going debate about the construct that is psychopathy. In light of this, this research supports the notion that it is important that psychopathy assessments include different modalities to supplement diagnosis to better inform research into a range of broader topics, including underlying mechanisms and interventions. The construct of psychopathy is ever evolving with more research, and multimodal research can be useful to capture the construct comprehensively without mono-method bias.
Supplemental Material
sj-docx-1-asm-10.1177_10731911251333315 – Supplemental material for Operationalizing Psychopathy Through a Multi-Method Approach
Supplemental material, sj-docx-1-asm-10.1177_10731911251333315 for Operationalizing Psychopathy Through a Multi-Method Approach by Ella M. Dickison and Martin Sellbom in Assessment
Footnotes
Acknowledgements
The authors acknowledge Emeritus Professor Neil McNaughton and Dr Phoebe Neo for their contributions to the overall project and Emma Veltman, Claire Liggins, and Dr Simon Wallace for serving as Research Assistants.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Professor Martin Sellbom is a paid consultant to the University of Minnesota Press, publisher of the MMPI-3, which was included in this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a research grant from the Royal Society of New Zealand Marsden Fund (19-UOO-249).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.