
Abstract
The Minnesota Multiphasic Personality Inventory-3 (MMPI-3) scales that are designed to assess various forms of externalizing psychopathology have received relatively little research attention to date. The goal of this investigation was therefore to examine the validity of these MMPI-3 scales in the measurement of the externalizing spectrum. A community sample (n = 206) with high levels of externalizing psychopathology and a university sample (n = 645) were used. The former sample was administered structured clinical interviews for various forms of externalizing psychopathology, whereas the student sample completed the Externalizing Spectrum Inventory-160. Confirmatory factor analysis was used to operationalize the externalizing spectrum using each set of measures. The results indicated that the externalizing MMPI-3 scales were associated with a general externalizing factor and an expected pattern of associations, while systematic residuals of individual disorder symptoms also emerged. Moreover, in the university sample, specific MMPI-3 scales hypothesized to assess antagonistic-externalizing (Aggressiveness, Aggression, and Cynicism) emerged as key predictors of a callous-aggression residual group factor. The Substance Abuse scale was unsurprisingly the best predictor of such dysfunction. These findings provide guidance for mental health practitioners who use the MMPI-3 for the assessment of externalizing psychopathology symptoms.
Keywords
Externalizing is a well-established psychopathology spectrum that has consistently emerged in structural models of mental disorders for the past several decades (see Krueger et al., 2021, for a review) and is featured as a major super-spectrum in contemporary psychopathology perspectives, such as the Hierarchical Taxonomy of Psychopathology (Kotov et al., 2017) and the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013; see Wright et al., 2012). The externalizing spectrum was initially conceived in research with children and adolescents (e.g., Achenbach, 1966) and tends to encompass attention-deficit/hyperactivity disorder [ADHD], oppositional defiant disorder, conduct disorder, and intermittent explosive disorder in childhood. The adult framework extends to antisocial personality disorder/psychopathy and substance use disorders as well (e.g., Beauchaine & McNulty, 2013; Krueger et al.,2002, 2005; Patrick, 2022; Young et al., 2000). The externalizing commonality across these disorders is clearly heritable, as evidenced from genetic studies in both children (e.g., Burt et al., 2001; Dick et al., 2005; Tuvblad et al., 2009) and adults (e.g., Kendler et al., 2003; Krueger et al., 2002; Young et al., 2000), with over 80% of this latent commonality being attributable to genetic effects in adulthood (e.g., Krueger et al., 2002; see Dhamija et al., 2016, for a review). A more elaborated model of externalizing psychopathology was proposed by Krueger et al. (2007) which included separate liability factors for substance misuse and callous aggression in a bifactor model framework. This elaborated model has received substantial validity support across samples and methods (e.g., Patrick et al., 2013; Sellbom, 2016; Venables & Patrick, 2012).
Externalizing disorders are a major public health problem for society due to their links to criminal behavior, including violence, that impacts other people (e.g., Kendler et al., 2013; Krueger et al., 2021). The financial costs to society related to crime, violence, and substance use is enormous (e.g., Darke, 2010; Gatner et al., 2023; Miller et al., 2006). Advancing scientific knowledge concerning the assessment of externalizing psychopathology can help facilitate accurate risk identification and provide sound evidence for targeted prevention, with the ultimate consequence of substantially reducing this financial and emotional burden on society. The current project sought to examine the validity of the Minnesota Multiphasic Personality Inventory-3 (MMPI-3; Ben-Porath & Tellegen, 2020a) for this purpose.
The MMPI instruments have always included a range of scales relevant to various forms and manifestations of externalizing psychopathology, but the MMPI-2-RF and MMPI-3 have more direct links to contemporary psychopathology structure than their older counterparts (Sellbom, 2019b). The MMPI-3 has a range of scales that have been assigned to a behavioral/externalizing domain of interpretation (Ben-Porath & Sellbom, 2023). These scales can be organized hierarchically, with the Behavioral/Externalizing Dysfunction (BXD) scale at the highest level, Antisocial Behavior (RC4) and Hypomanic Activation (RC9) at the mid-tier level, and seven Specific Problem (SP) scales (Family Problems [FML], Juvenile Conduct Problems [JCP], Substance Abuse [SUB], Impulsivity [IMP], Activation [ACT], Aggression [AGG], and Cynicism [CYN]) at the lowest level. In parallel to this hierarchy, the MMPI-3 Personality Psychopathology Five (PSY-5) scale Disconstraint (DISC) measures a dispositional proclivity toward externalizing behavior. Sellbom (2020) has also argued that the PSY-5 Aggressiveness (AGGR) scale and the Self-Importance (SFI), Dominance (DOM), and Disaffiliativeness (DSF) SP scales should be considered markers of the antagonism dimension of externalizing and therefore be considered in a broader assessment of this super-spectrum. Sellbom (2020) also presented some preliminary results from both community and university samples that these scales were associated with some markers of externalizing, although SFI, DOM, and DSF to a much lesser degree than the other scales.
Sellbom et al. (2021) found support for an MMPI-3 scale structure that they mapped onto the HiTOP model in two large mental health and prison samples. The externalizing super-spectrum was specified as part of this much larger structure with two lower-order factors representing antagonism and disinhibition, respectively. In addition to the aforementioned SP scales, Anger Proneness (ANP) also loaded on the antagonistic-externalizing factor, whereas DSF had marginal factor loadings across both samples. In a sequential hierarchical analysis, DSF loaded preferentially on a detachment factor in both samples and SFI also loaded negatively on an internalizing/distress factor. J.R. Brown and colleagues (2023) generally replicated the latter findings in primary care and student samples. Thus, the DSF scale is less likely to be an important marker of externalizing psychopathology, whereas ANP, SFI, and DOM remain potential candidates in addition to the standard externalizing MMPI-3 scales. However, it is important to consider that the analyses across these studies were focused on internal structure of MMPI-3 scales, and they were not evaluated against any external criterion representing the externalizing psychopathology spectrum.
Thus, although research linking the MMPI-3 scales to psychopathology spectra is emerging (e.g., J.R Brown et al., 2023; Sellbom et al., 2021), no study to date has examined explicit associations with a more comprehensive approach to modeling the externalizing psychopathology spectrum per the extant psychopathology literature (e.g., Krueger et al., 2005, 2007). As mentioned earlier, in the MMPI-3 Technical Manual (Ben-Porath & Tellegen, 2020b), Sellbom (2020) presented associations between the externalizing MMPI-3 scales as well as AGGR, SFI, DOM, and DSF against a series of externalizing disorder symptom counts in a community sample and self-reported maladaptive externalizing personality traits from a university sample. The externalizing scales in particular exhibited large associations with the extra-test criterion measures with SFI, DOM, and DSF showing more specific circumscribed associations with conceptually relevant variables. Although these results are informative, only a pattern of bivariate associations with individual disorder and trait constructs were considered, and the externalizing spectrum was not modeled from these data. Sellbom’s (2020) results were also confined to the test manual and thus not peer-reviewed.
Two additional studies have also provided evidence that particular MMPI-3 scales have promising validity with respect to the assessment of externalizing tendencies. T.A. Brown and Sellbom (2021, 2023) also examined correlations between MMPI-3 scale scores and traditional personality disorder symptom counts and dimensional personality traits in a large university sample from New Zealand. The MMPI-3 externalizing scales were associated with antisocial personality disorder (BXD, RC4, RC9, JCP, SUB, IMP, AGG, CYN, and DISC) as well as other personality disorders that have been linked to externalizing spectrum (e.g., Krueger et al., 2021; Sellbom, 2019a), such as paranoid (BXD, ANP, FML, IMP, AGG, CYN, and DSF), borderline (BXD, RC4, RC9, ANP, FML, IMP, AGG, CYN, and DISC), histrionic (BXD, RC4, RC9, ANP, FML, IMP, ACT, AGG, CYN, and DISC), and narcissistic (BXD, RC9, ANP, IMP, AGG, and CYN). A similar pattern of results emerged with the antagonism and disinhibition domains of the Comprehensive Assessment of Traits relevant to Personality Disorder (CAT-PD; Simms et al., 2011) in the university sample, with SFI only being specifically associated with Grandiosity and Exhibitionism, and DOM with Domineering and Exhibitionism. Furthermore, Maccarone et al. (2023) recently showed that BXD, RC4, SUB, and DISC were also related to a range of alcohol and drug use history variables in a large clinical neuropsychology sample. Although promising for identifying the most relevant MMPI-3 scales, neither study considered externalizing from a hierarchical spectrum perspective.
The goal of the current study was to examine associations between a broad range of MMPI-3 scales most relevant to the externalizing super-spectrum and a latent factor representing this spectrum in two separate samples. In addition, it was examined whether the selected MMPI-3 scales were associated with unique aspects of different types of externalizing psychopathology while controlling for general factor variance, both in terms of externalizing disorder symptom counts and liability factors for callous-aggression and substance use problems (Krueger et al., 2007). It was expected, based on the literature just reviewed, that the MMPI-3 scales that formally belong to the behavioral domain would be associated with externalizing psychopathology, with broader scales (BXD, RC4, RC9, AGGR, DISC) as the best predictors of the externalizing super-spectrum. Furthermore, it was conceptually expected that JCP would be a particularly potent predictor of conduct disorder history, SUB of substance misuse, IMP of ADHD, ANP and AGG of intermittent explosive disorder as well as callous aggression and CYN of callous aggression (Maccarone et al., 2023; Sellbom, 2020; Wygant & Sellbom, 2024). Although FML, SFI and DOM were expected to be associated with externalizing, they were not expected to be prominent markers of either the general factor or any specific systematic residual variances given their more specific foci of measurement and the findings in the broader literature just reviewed.
Method
This study was not pre-registered. Two archival samples were used and all data analyses were pre-planned unless otherwise explicitly stated. All data exclusions, manipulations, and measures used in this study are reported. The data used in this study are considered proprietary by the University of Minnesota Press, who can be contacted for permissions. The corresponding author can be contacted for assistance with this process. Furthermore, these samples have been used in previous studies (Dickison et al., 2024; Neo et al.,2021, 2024a, 2024b) but the research questions and all analyses presented in the current study are novel.
Participants
Community Sample
Participants were recruited from the general community via paid Facebook advertisements and flyers distributed across the community, including at community corrections offices, targeting a range of externalizing disorders and behaviors (e.g., history of criminal convictions, drug use, anger management problems, impulsivity, and/or ADHD) for a broader study on personality and brain processes (e.g., Neo et al., 2021, 2024) with an aim to obtain diverse representation of externalizing psychopathology. 1 A total of 242 participants completed the experimental protocol. Participants who produced invalid MMPI-3 profiles (i.e., Cannos Say ≥ 18, Combined Response Inconsistency, Variable Response Inconsistency or True Response Inconsistency ≥ 80T, Infrequent Responses or Infrequent Psychopathology Responses ≥ 100T) were excluded, which resulted in a final sample of 206 individuals. Their ages ranged from 18 to 56 years old (M = 36.2; SD = 9.57). There were 87 participants who identified as male, 118 who identified as female, one who identified as transgender, and one who elected not to respond. The most commonly self-reported ethnicities were New Zealand European (71.4%), Māori (13.6%), Asian (12.1%), and Other European (10.7%). An additional 8.7% reported belonging to “other” ethnic groups. The percentages add up to more than 100% as participants were not limited to the number of ethnicities they could select. Almost 39% self-reported that they had been convicted of a criminal offense in the past, with 18% of the sample currently being on probation or parole. Based on structured clinical interviews, 120 (58%) met diagnostic criteria for at least one DSM-5 externalizing disorder, including ADHD (any type, 28%), antisocial personality disorder (22%), history of conduct disorder (22%), alcohol use disorder (20%), cannabis use disorder (15%), and intermittent explosive disorder (5%). As intended, these rates are substantially higher than a typical community sample (Kessler et al., 2011).
In terms of differences between included and excluded participants, there were no differences in age (t [241] = 1.23, p =.221), gender (χ2 [2, N=245] = 3.98, p = .136), minority ethnicity status (χ2 [1, N=242] = 0.11, p = .740), or history of criminal convictions (χ2 [1, N=242] = 1.81, p = .178); however, those excluded were more likely to have been diagnosed with an externalizing disorder compared to those who were included (χ2 [1, N=242] = 20.38, p <.001, Cramer’s V = 0.29).
University Sample
This sample consisted of 707 psychology students at the University of Otago recruited through a research participation program. After exclusion based on MMPI-3 validity scales, 151 men (23%) and 494 (77%) women, who ranged in age from 18 to 57 (M = 19.61; SD = 2.96), remained. Most participants reported their ethnicity as New Zealand European (70%), with 17% Other European, 8% Chinese, 7% Māori, 3% Pacific Islander, and 3% Indian, and 14% selecting “other.” Again, these values sum to greater than 100% because some selected more than one option.
In terms of differences between included and excluded participants, there were no differences in age (t [700] = 0.34, p =.973) or biological sex (χ2 [1, N=703] = 0.51, p = .474). However, those excluded were more likely to be of minority ethnicity status compared to those who were included (χ2 [1, N=645] = 9.98, p =.002, Cramer’s V = 0.12), although the effect size estimate associated with this difference was small.
Measures
MMPI-3
The MMPI-3 (Ben-Porath & Tellegen, 2020a) is a 335-item self-report inventory on which participants responded true or false to each statement about themselves. The items aggregate onto 10 validity scales and 42 scales that measure substantive clinical content. The MMPI-3 externalizing scales along with SFI, DOM, and AGGR were used in this study.
Structured Clinical Interview for DSM-5 Disorders–Research Version
The modules for ADHD, substance use disorders, and intermittent explosive disorder from the Structured Clinical Interview for DSM-5 Disorders–Research Version (SCID-5-RV; First et al., 2015) were used. Each disorder symptom count was scored according to the number of criteria met for that disorder. Inter-rater reliability (intra-class correlation, two-way random model, absolute agreement) was good to excellent for all symptom counts, ranging from .87 (intermittent explosive disorder) to .99 (alcohol use disorder). The SCID-5-RV modules were only administered to the community sample.
Structured Clinical Interview for DSM-5 Personality Disorders
The Structured Clinical Interview for DSM-5 Personality Disorders (SCID-5-PD; First et al., 2016) modules for antisocial personality disorder and conduct disorder (history) were used. Each disorder symptom count was scored according to the number of criteria met for each disorder. The inter-rater reliability for the conduct disorder ratings were fair (intra-class correlation coefficient [ICC] = .67) and excellent for antisocial personality disorder symptom ratings (ICC = .95). This SCID-5-PD module was only administered to the community sample.
Externalizing Spectrum Inventory-160
The Externalizing Spectrum Inventory-160 (ESI-160; Patrick et al., 2013) is a short form of the full-length ESI, which is a self-report inventory that measures a range of externalizing behaviors. The ESI-160 contains 23 scales in total that measure various forms of impulsivity, dishonesty, (low) empathy, theft, fraud, physical, destructive, and relational aggression, and marijuana, alcohol, and other drug use and problems. Item responses are based on a four-point Likert-type scale (“True,” “Somewhat true,” “Somewhat false,” or “False.”). Research has shown that, within prisoner and student samples, the ESI-160 yields reliability results similar to the longer measure (Patrick et al., 2013) that has acceptable construct validity (Venables & Patrick, 2012). The 23 scales were used to estimate Krueger et al.’s (2007) bifactor model for the externalizing spectrum. The ESI-160 was only administered to the participants in the university sample.
Procedure
The University of Otago Human Ethics Committee (Health) approved both data collections.
Community Sample
Participants first completed a battery of questionnaires for a separate study before undergoing electroencephalogram (EEG) testing for that project. After completing the EEG recordings, the participants were interviewed in a private room in the corresponding author’s research lab by a trained research assistant under the supervision of a registered clinical psychologist. The research assistants were clinical psychology students with extensive practical experience who had undergone substantial training in these structured interviews by the corresponding author. For a small random subset (n = 20), a second research assistant observed the interview and independently rated the participant on the SCID-RV and SCID-5-PD for purposes of inter-rater reliability. The participants also completed a battery of self-report questionnaires, including the MMPI-3. The participants received $50 of petrol or supermarket vouchers for reimbursement of their inconvenience.
University Sample
All participants across both samples completed a series of self-report questionnaires (including the ESI-160) in groups of up to 12, while monitored by a trained research assistant. They were recruited from the psychology department research participation program, which includes all students enrolled in first- and second-year psychology courses, and they received course credit for their participation.
Data Analyses
First, in the community sample, it was examined whether individuals who met diagnostic threshold for any externalizing disorder scored higher on the selected MMPI-3 scales than those who did not meet criteria for any of those diagnoses. For this purpose, a series of independent samples t-tests were used with Cohen’s d to characterize effect size magnitudes. The a priori alpha level was set to .05, but the focus was on evaluating effect sizes.
Next, confirmatory factor analysis was used to estimate a latent variable model in each of the samples using Mplus 8.8. Because several indicators were not normally distributed, the maximum likelihood estimator with robust scaling (MLR) was used. Global model fit indices (Chi-square test, Confirmatory Fit Index [CFI], Tucker–Lewis Index [TLI], Root Mean Squared Error of Approximation [RMSEA]) were used to determine the plausibility of the models given observed data. The models in each sample were different, given the differences in measurement. In the community sample, a one-factor latent variable with the six externalizing disorder symptom counts as indicators was estimated. Specifically, antisocial PD, conduct disorder, ADHD, intermittent explosive disorder symptoms, alcohol use disorder, and cannabis use disorder 2 were used as manifest indicators. A correlated residual was also specified a priori between the two substance use disorder variables as additional liability factors have been identified for such psychopathology (e.g., Kendler et al., 2003; Krueger et al., 2007). In the university sample, Krueger et al.’s (2007) bifactor model was estimated in which all 23 ESI-160 scales loaded on a general externalizing factor, whereas some of the indicators also loaded on one of two residual group factors of substance misuse and callous aggression based on the factor loadings (i.e., > .|30|) presented in Patrick et al. (2013) (for more information, see the “Results” section). For both models, modification indices were consulted post hoc for possible re-specification in the event that the a priori model would evince poor fit to the observed data. Only modification indices that could be theoretically supported (e.g., the systematic variances would be theoretically associated above and beyond what would be accounted for by the latent variable) were considered.
To examine the MMPI-3 scales, a series of Multiple Indicators and Multiple Causes (MIMIC) models in which each of the individual MMPI-3 scales served as predictors to determine their bivariate associations with the general externalizing factor were estimated and evaluated. A medium effect size (i.e., β≥ .|30|) was set to indicate a meaningful association. Next, MIMIC models in which multiple MMPI-3 scales were entered simultaneously to evaluate the relative incremental predictions were also estimated and evaluated; however, because scales within scales sets have item overlap, all such regression models were estimated separately for each MMPI-3 scale set given item overlap across levels of the scale hierarchy. Only scales with a meaningful bivariate association were entered into a regression model to reduce the likelihood of negative suppressor effects and because there were no theoretical reasons to expect cooperative suppression.
Finally, to determine whether the MMPI-3 externalizing scales showed a pattern of specific associations with the individual disorder constructs (in the community sample) or callous aggression and substance misuse (in the university sample) beyond general externalizing, zero-order prediction models were also estimated in which the residual variances were (in separate models) regressed onto each of the MMPI-3 scales. In other words, these would indicate associations between MMPI-3 scales and the systematic residual variances of the individual disorder constructs or group factors.
Results
Tables S1–S6 in the online supplemental materials show correlation matrices across all study variables in each sample.
Group Differences
First, the externalizing MMPI-3 scale scores were examined for differences across participants diagnosed with at least one externalizing disorder and those who did not meet diagnostic threshold for any such disorder in the community sample. The results of the independent samples t-tests are shown in Table 1. All scales with the exception of SFI were significantly higher in the externalizing disorder group compared to those without such disorders. Although DOM scores were significantly higher in the externalizing disorder group, the difference was associated with a small effect size and also would likely not have survived any correction to the alpha level for multiple tests. The remainder were associated with large effect size differences, with BXD, RC4, and DISC being the best scales at differentiating between the groups. This finding is unsurprising as these three scales are the ones most broadly related to externalizing problems, with DISC reflecting a broadband dispositional proclivity toward externalizing.
Independent Samples t-tests for MMPI-3 Scales across Externalizing Disorder Conditions.

Note. BXD = Behavioral/Externalizing Dysfunction, RC4 = Antisocial Behavior, RC9 = Hypomanic Activation, ANP = Anger Proneness, FML = Family Problems, JCP = Juvenile Conduct problems, SUB = Substance Abuse, IMP = Impulsivity, ACT = Activation, AGG = Aggression, CYN = Cynicism, SFI = Self-Importance, DOM = Dominance, AGGR = Aggressiveness, DISC = Disconstraint.
p < .001. *p < .01.
Externalizing Spectrum Models
In the community sample, the one-factor EXT model converged appropriately. The model fit was very close, with a non-significant chi-square test (χ2 = 9.72, df = 8, p = .29) and excellent model fit indices (CFI = .99, TLI = .99, RMSEA = .032, Standardized Root Mean Square Residual [SRMR] = .027). Factor loadings appear in Table 2; these were all of acceptable magnitude. Overall, the EXT model was deemed acceptable for the primary analyses.
Factor Loadings for CFA Model in Community Sample
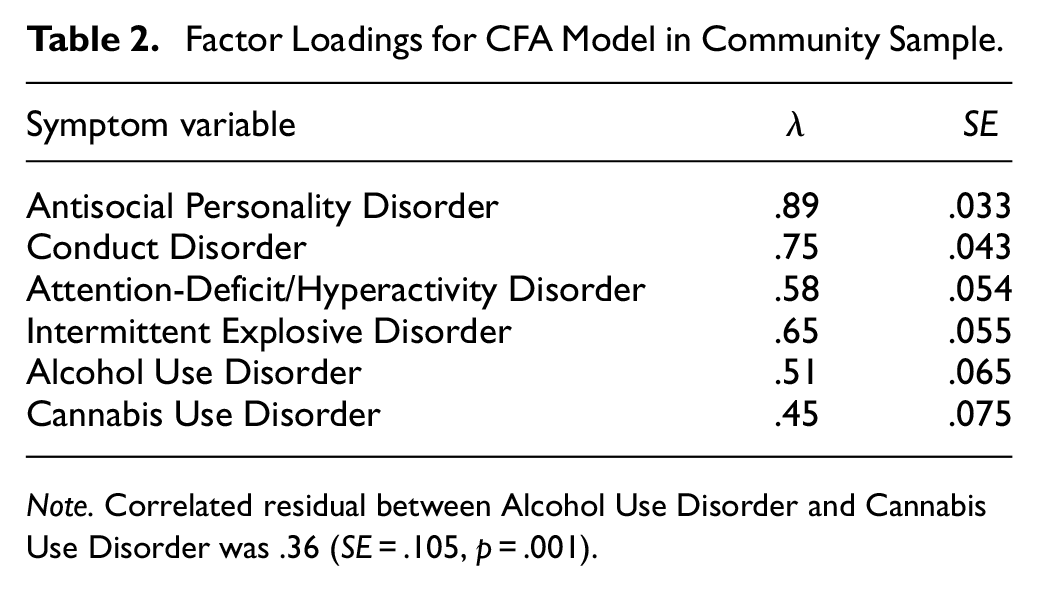
Note. Correlated residual between Alcohol Use Disorder and Cannabis Use Disorder was .36 (SE = .105, p = .001).
In the university sample, the initial bifactor model had mediocre to poor model fit based on conventional thresholds (χ2 = 1370.84, df = 217, p <.001, CFI = .77, TLI = .73, RMSEA = .091, SRMR = .076). In a post hoc re-specification, two correlated residuals were added (blame externalizing and alienation; alcohol use and alcohol problems) based on conceptually defensible overlap of systematic residual variances. These same correlated residuals were also necessary in Patrick et al.’s (2013) modeling of the ESI-160 scales, indicating replicability. This model was associated with improved model fit (χ2 =1057.24, df = 215, p <.001, CFI = .83, TLI = .80, RMSEA = .078, SRMR = .069), albeit still poor with respect to the incremental model fit indices. However, such indices tend to perform less well with complex models and large sample sizes (e.g., Lai & Green, 2016; Rigdon, 1996) and the intercorrelations among the ESI-160 scales were not large (see Supplemental Table S5), which further contributes to lower incremental fit. Therefore, because the pattern of factor loadings generally supported the theoretical structure and the modifications were consistent with previous research, this model was retained for further analyses rather than applying additional modifications. Table 3 shows the factor loadings for the final model; all loadings were at least .30 or larger, with most exceeding .40. For the callous-aggression factor, Excitement Seeking (.12) and Rebelliousness (.05) had very weak loadings, and while inconsistent with Patrick et al. (2013), this finding is not surprising given the conceptual nature of the construct (Patrick et al., 2013; Sellbom, 2016; Venables & Patrick, 2012).
Factor Loadings for Final Bifactor Model in University Sample

ESI-160 scale was reversed prior to analysis. Correlated residuals between Alcohol Use and Alcohol Problems was .58 (SE = .023, p < .001) and between Alienation and Blame Externalizing was .45 (SE = .036, p < .001). ESI = Externalizing Spectrum Inventory.
MMPI-3 Scale Associations
The primary analyses concerned the evaluation of the broad set of potential MMPI-3 markers of externalizing. First, in a series of MIMIC models using the latent general externalizing factor as a criterion, each of the MMPI-3 scales was entered as predictors in individual models. These results are shown in Table 4 (community sample) and Table 5 (university sample). The pattern of bivariate associations across samples was highly robust; indeed, a post hoc intra-class correlation analysis indicated excellent agreement (ICC = .94; two-way random model, absolute agreement). With the exception of SFI and DOM, all MMPI-3 scales were associated with a meaningful effect size, although AGGR technically fell below the a priori threshold in the university sample (β = .29). BXD and DISC had bivariate associations of β > .70 across both samples.
MIMIC Models for MMPI-3 Scales Predicting the Externalizing Latent Factor in the Community Sample

Note. BXD = Behavioral/Externalizing Dysfunction, RC4 = Antisocial Behavior, RC9 = Hypomanic Activation, ANP = Anger Proneness, FML = Family Problems, JCP = Juvenile Conduct problems, SUB = Substance Abuse, IMP = Impulsivity, ACT = Activation, AGG = Aggression, CYN = Cynicism, SFI = Self-Importance, DOM = Dominance, AGGR = Aggressiveness, DISC = Disconstraint.
MIMIC Models for MMPI-3 Scales Predicting the General Externalizing Factor in the University Sample

Note. BXD = Behavioral/Externalizing Dysfunction, RC4 = Antisocial Behavior, RC9 = Hypomanic Activation, ANP = Anger Proneness, FML = Family Problems, JCP = Juvenile Conduct problems, SUB = Substance Abuse, IMP = Impulsivity, ACT = Activation, AGG = Aggression, CYN = Cynicism, SFI = Self-Importance, DOM = Dominance, AGGR = Aggressiveness, DISC = Disconstraint.
The latent regression models, which were conducted within each scale set using only MMPI-3 scales with a priori meaningful associations as predictors, are also presented in Tables 3 and 4. The RC scale models accounted for 67% and 56% of the variance in the general factor in the community and university samples, respectively. Although RC4 was the primary predictor in the community sample, both RC4 and RC9 contributed about equally to this prediction in the university sample. The SP scale models accounted for 75% and 68% of the variance in the general factor in the community and university samples. Although most scales (except FML) significantly contributed to the prediction in the university sample, four scales (JCP, SUB, IMP, and AGG) were significant predictors in the community sample. Finally, the PSY-5 scale model accounted for 60% of the variance in the externalizing factor in the community sample, with DISC being the sole significant predictor. This model was not estimated in the university sample as only DISC met the threshold for a meaningful association.
Finally, the associations for MMPI-3 scales with residual systematic variances were considered; these are reported in Table 6. For the residual symptom counts in the community sample, there was a general positive manifold with respect to predictions, and the broader scales (in particular, BXD, RC4, and DISC) were generally associated with externalizing disorders. Among the SP scales, as expected, JCP had the largest association with history of conduct disorder, IMP was the best predictor of residual ADHD symptoms, ANP and AGG had the only large associations with intermittent explosive disorder, and SUB was the most robust predictor of residual alcohol use disorder and cannabis use disorder, although the pattern was less clear for the latter variable. In terms of the associations with the callous aggression and substance misuse group factors in the university sample, the pattern was clearer. BXD, JCP, AGG, CYN, and AGGR had meaningful associations with the callous aggression factor, as generally expected, whereas BXD, RC4, DISC, and SUB had meaningful associations with the substance misuse factor.
Fully Standardized Regression Coefficients From MIMIC Models for MMPI-3 Scales Predicting Symptom Count Residuals and Latent Group Factors in the Community and University Samples, respectively
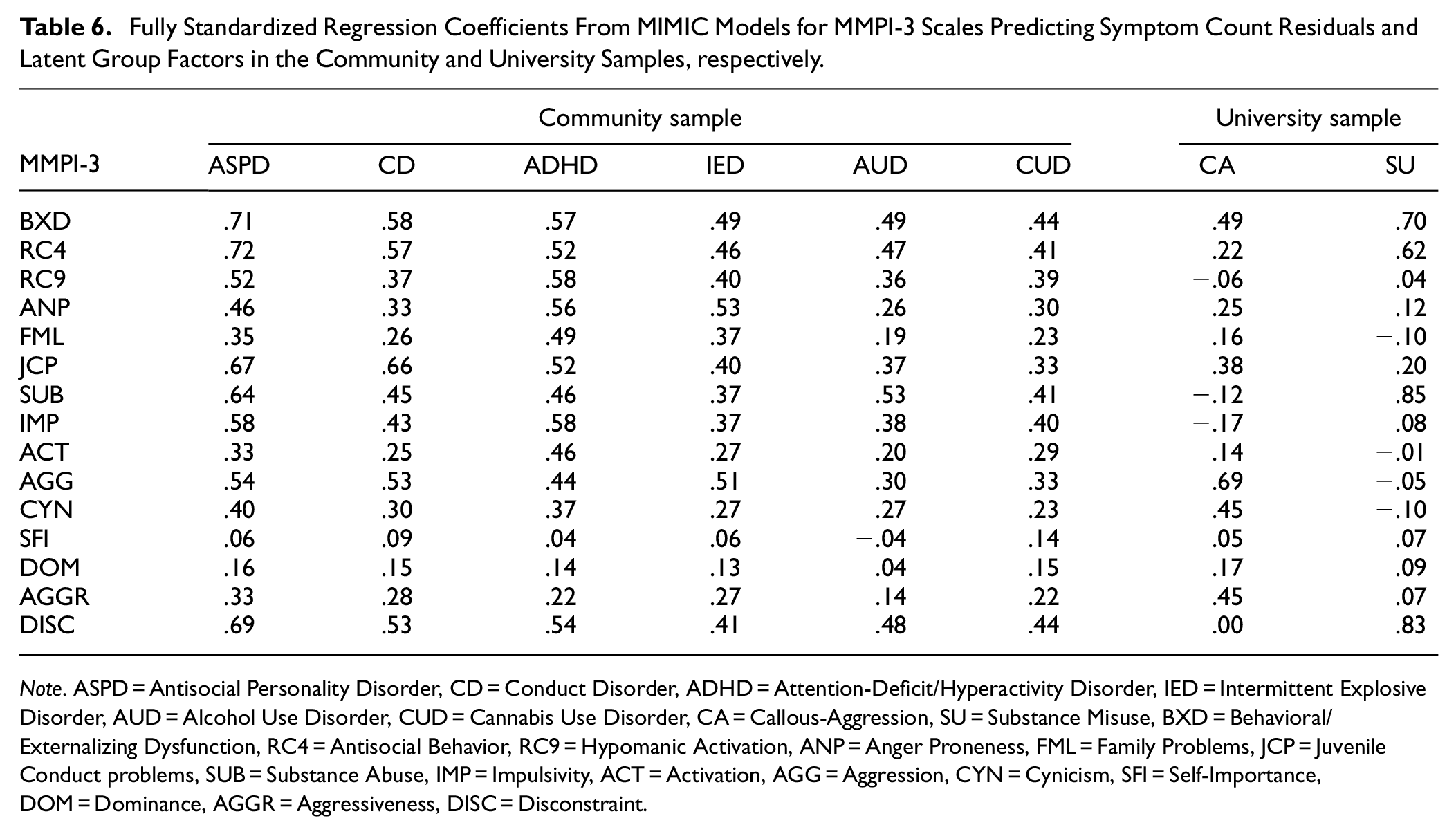
Note. ASPD = Antisocial Personality Disorder, CD = Conduct Disorder, ADHD = Attention-Deficit/Hyperactivity Disorder, IED = Intermittent Explosive Disorder, AUD = Alcohol Use Disorder, CUD = Cannabis Use Disorder, CA = Callous-Aggression, SU = Substance Misuse, BXD = Behavioral/Externalizing Dysfunction, RC4 = Antisocial Behavior, RC9 = Hypomanic Activation, ANP = Anger Proneness, FML = Family Problems, JCP = Juvenile Conduct problems, SUB = Substance Abuse, IMP = Impulsivity, ACT = Activation, AGG = Aggression, CYN = Cynicism, SFI = Self-Importance, DOM = Dominance, AGGR = Aggressiveness, DISC = Disconstraint.
Discussion
The current study aimed to examine the associations between a range of MMPI-3 scales conceptually relevant to the externalizing super-spectrum with latent variable models representing this structure in two separate samples. The results generally indicated that scales designated as being part of the behavioral domain for MMPI-3 interpretation (along with ANP) were all meaningful predictors of general externalizing in the bivariate analyses, whereas two scales from the interpersonal domain, but with relevant content (SFI and DOM), did not contribute to any of the predictions in a meaningful manner. In the university sample, there was also a clear pattern of associations with residual group factors reflecting callous aggression and substance misuse. These general findings will be discussed in more detail.
Two scales in particular, BXD and DISC, along with RC4 in the community sample are clearly the best overall MMPI-3 indicators of the externalizing spectrum. These scales were also associated with the largest effect sizes in differentiating between those with externalizing disorders and those without such disorders in the community sample. BXD and RC4 both reflect a general tendency toward a range of externalizing proclivities, including nonadherence to social norms and standards, rejection of authority, impulsivity, and substance use, with BXD at a broader level also including elements of antagonism (e.g., Ben-Porath & Sellbom, 2023). DISC, specifically, represents a dispositional proclivity toward externalizing, and the construct it operationalizes (also known as disinhibition) is included in every major personality model (e.g., DSM-5 Alternative Model for Personality Disorder [AMPD], ICD-11 Personality Disorder). Trait disinhibition is considered as the core personality liability factor for externalizing (Beauchaine & McNulty, 2013; Patrick et al., 2013; Venables & Patrick, 2012; see also Patrick, 2022), and it is therefore unsurprising that the MMPI-3 DISC scale emerged as an important predictor.
Contemporary psychopathology models consider externalizing as a super-spectrum at a level above the antagonistic-externalizing and disinhibited-externalizing spectra (in HiTOP; see e.g., Kotov et al.,2017, 2021; and in AMPD, e.g., Wright et al., 2012). The antagonism domain usually emerges in structural studies with a sufficient range of indicators of such maladaptive personality traits (e.g., Krueger et al., 2021). In the community sample, traditional psychopathology markers of externalizing were used, but it is important to consider that some key mental disorders that are typically represented through antagonism were not included (e.g., narcissistic and paranoid personality disorder; interpersonal and affective psychopathic personality traits), and as such, the best predictors were generally scales that are primarily measures of disinhibited-externalizing (i.e., RC4, RC9, JCP, SUB, IMP; see Sellbom, 2020). Indeed, scales like AGGR, CYN, and to some degree, AGG, which are hypothesized to be the best MMPI-3 markers of antagonistic-externalizing (Sellbom, 2020; Sellbom et al., 2021), did not emerge as key predictors of externalizing in the community sample. In the university sample, however, the elaborated externalizing spectrum model proposed by Krueger et al. (2007) was operationalized, with the callous aggression factor conceptually representing a liability factor for antagonistic-externalizing that is separate from general externalizing (Patrick, 2022; Patrick et al., 2013); this factor is also akin to meanness in the triarchic psychopathy model (Patrick, 2022). The MMPI-3 scales that emerged as the best predictors of this factor were AGGR, AGG, and CYN (along with BXD as a broader super-spectrum scale), which is consistent with previous MMPI-3 research into these externalizing manifestations (Sellbom, 2020; Sellbom et al., 2021). Indeed, these are also scales that emerge as prominent predictors of interpersonal and affective psychopathic personality traits across samples (e.g., Wygant & Sellbom, 2024).
The residual substance misuse variance (including the group factor in the ESI model) was best predicted by broader markers of disinhibited-externalizing (BXD, RC4, DISC) and, unsurprisingly, the SUB scale. These findings are consistent with the available MMPI-3 literature. For instance, Maccarone et al. (2023) recently showed that these scales in particular were the best predictors of a range of substance-related history variables in a clinical neuropsychology sample. It is also noteworthy that these predictions were of systematic variances that is non-overlapping with general externalizing. Some research has indicated that substance use disorders, while sharing genetic liability with general externalizing, also have a genetic vulnerability that is separate from this spectrum (e.g., Kendler et al., 2003). Patrick et al. (2013) hypothesized that this liability factor might reflect proclivities toward sensation and novelty seeking or nonconformity to traditional values rather than outright disinhibition and impulsivity, which could be consistent with the current findings.
Two MMPI-3 scales that were included did not emerge as meaningful predictors of externalizing. SFI and DOM were included because both are conceptually linked to grandiosity, domineering, and exhibitionism which are part of interpersonal antagonism (e.g., Crowe et al., 2018), they have been empirically linked to such maladaptive traits (T.A. Brown & Sellbom, 2023), and owing to recent structural evidence that these MMPI-3 scales load among other relevant scales on an antagonism spectrum factor across samples (J.R. Brown et al., 2023; Sellbom et al., 2021). Neither scale was meaningfully associated with any form of externalizing across the two samples. However, as noted earlier, some of these personality manifestations of antagonism (grandiosity, domineering, and exhibitionism) were not featured among the indicators used in the current models, including the 23 ESI-160 scales. Consequently, whereas SFI and DOM might be relevant to these specific interpersonal facets of antagonism, they cannot be considered key markers of the externalizing spectrum, which is consistent with their inclusion among the MMPI-3 Interpersonal Specific Problems scales rather than the externalizing ones.
The current findings have applied implications for MMPI-3 assessment. The findings further confirm that the BXD scale can be used as a broad-based marker of externalizing dysfunction, reflecting a severity dimension of this general super-spectrum. Clinicians who interpret the test can therefore have confidence that this scale will reflect substantial impairment in this domain although more narrow scales will need to be considered to provide more nuanced interpretation of externalizing symptoms and traits. Moreover, the DISC scale should be considered a core dispositional marker of this spectrum (e.g., Krueger et al., 2002), particularly of disinhibited-externalizing, and those with elevated scores have likely exhibited prolonged tendencies toward a range of externalizing problems. Clinicians can benefit from this information to also determine whether impairment in externalizing (as indicated by BXD, and to slightly lesser degree, RC4) is likely influenced by long-standing dispositional proclivities (i.e., elevated DISC), including antisocial personality traits (e.g., Brown & Sellbom, 2021), or perhaps more contextual or situational factors. Such information would also be important for forensic mental health professionals making risk determinations for future re-offending.
MMPI-3 scales that appear at lower levels of the interpretive hierarchy can also add further nuance. For instance, elevations on AGGR, AGG, and CYN scales, in particular, can serve as useful indicators of the potential presence of antagonistic-externalizing symptoms and traits, which could include traditional psychopathic personality traits (i.e., affective-interpersonal or meanness; Patrick, 2022). The presence of such traits would have both diagnostic implications and be informative with respect to risk formulation. Other SP scales can further delineate the specific manifestations of externalizing. For instance, JCP can alert to the presence of past conduct problems, IMP measures a transdiagnostic construct that is relevant to multiple externalizing manifestations, including ADHD, and SUB unsurprisingly is the best marker of substance use problems. Thus, the pattern of elevations of these SP scale scores can allow clinicians to generate a more specific formulation of the externalizing psychopathology dysfunction that is indicated by high BXD and/or RC4 scores.
The current study is not without limitations that merit careful consideration. First, although the use of multiple samples should be considered a strength, the samples themselves have limited generalizability. The community sample is not necessarily representative of any natural population and the university sample is quite homogeneous with respect to age, gender, and education. Second, no systematic diagnostic information beyond externalizing was collected, which means that the impact of other comorbidities on the findings could not be examined. Third, the operationalization of externalizing in both samples was mono-method, which means that the latent factors were also influenced by shared method variance among their indicators. However, the type of method was different across the two samples. Moreover, all measurement in the university sample was via self-report, which results in shared method variance with the MMPI-3 scale scores, and possible inflation of effect sizes to an unknown degree. On the other hand, the sample is likely range restricted with respect to externalizing dysfunction which might serve to attenuate effect sizes to an unknown degree. Finally, individuals in the community sample who were excluded due to invalid MMPI-3 profiles were more likely to have an externalizing disorder diagnosis than those who were not, which might have impacted the generalizability of the findings. However, it is also not surprising that higher rates of externalizing would be associated with higher rates of profile invalidity as individuals with such psychopathology likely have less capacity for sustained attention and might also be less cooperative. These various limitations notwithstanding, it is encouraging that the findings replicated well across the two samples and different measurement modalities.
Future research should replicate these findings in other relevant clinical, forensic, and correctional samples. It would be ideal if such studies also took a multimethod approach to the examination of MMPI-3 scale associations with externalizing psychopathology. Moreover, studies should also consider the full externalizing super-spectrum and include comprehensive measurement of antagonistic-externalizing given that the current study placed a stronger emphasis on the disinhibited-externalizing spectrum. Given the available range of MMPI-3 scales to cover externalizing, researchers should also consider their utility in modeling the externalizing spectrum to address novel questions about such dysfunction.
Supplemental Material
sj-docx-1-asm-10.1177_10731911241293939 – Supplemental material for MMPI-3 Assessment of Externalizing Psychopathology in Targeted Community and University Samples
Supplemental material, sj-docx-1-asm-10.1177_10731911241293939 for MMPI-3 Assessment of Externalizing Psychopathology in Targeted Community and University Samples by Martin Sellbom in Assessment
Footnotes
Author’s Note
The author is grateful to Yossef Ben-Porath and Ella Dickison for their comments on an earlier version of this article. The author also acknowledges Neil McNaughton for his contributions to this project more broadly.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.S. is a paid consultant to the University of Minnesota Press, publisher of the MMPI-3.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A grant from the University of Minnesota Press funded this project.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.