
Abstract
Eating disorders are severe and often chronic mental illnesses that are associated with high impairment and mortality rates. Recent estimates suggest that eating disorder prevalence rates are on the rise, indicating an increased need for accurate assessment and detection. The current review provides an overview of transdiagnostic eating disorder assessments, including interview, self-report, health and primary care screeners, and technology-based and objective assessments. We focused on assessments that are transdiagnostic in nature and exhibit high impact in the field. We provide recommendations for how these assessments should be used in research and clinical settings. We also discuss considerations that are crucial for assessment, including the use of a categorical versus dimensional diagnostic framework, assessment of eating disorders in related fields (i.e., anxiety and depression), and measurement-based care for eating disorders. Finally, we provide suggestions for future research, including the need for more research on short transdiagnostic screeners for use in health care settings, standardized assessments for ecological momentary assessment, development of state-based assessment of eating disorder symptoms, and consideration of assessment across multiple timescales.
Introduction
Eating disorders (EDs) are serious psychiatric illnesses with high mortality, morbidity, and societal cost (Deloitte Access Economics, 2020). EDs are characterized by disturbances in eating behaviors, changes in weight, and impaired physical, emotional, and social functioning. Due to physiological complications and high suicide rates, EDs have the second-highest mortality rate of any psychiatric disorder, after opioid use disorder (Chesney et al., 2014). Lifetime prevalence of EDs is 14.3% in males and 19.7% in females (Ward et al., 2019). However, these rates likely underestimate the actual prevalence of EDs due to low rates of recognition, treatment-seeking, and lack of psychometrically strong assessment and screening in minorities, males, and older adults (Grillot & Keel, 2018), signifying the need for strong assessments of EDs that can accurately detect EDs in all populations.
ED Diagnoses
The three primary ED diagnoses include anorexia nervosa (AN), bulimia nervosa (BN), and binge-eating disorder (BED; American Psychiatric Association [APA], 2013). However, about 50% of those with EDs fall into the category of other specified feeding and eating disorder (OSFED), such as atypical AN (AAN), which is a clinically significant and impairing ED that does not neatly fit into one of the primary diagnostic categories (Dalle Grave, 2011). Regardless of diagnosis, EDs are highly heterogeneous with high diagnostic overlap (i.e., restriction and binge eating are transdiagnostic behaviors, regardless of diagnosis), which complicates assessment and treatment (Keel et al., 2012). The Transdiagnostic Theory of EDs posits that common mechanisms and symptoms (e.g., overvaluation of eating, shape, and weight) are shared among all EDs such as AN, BN, and AAN (Fairburn et al., 2003). As such, this review focuses on transdiagnostic assessment of behaviors and cognitions that span across ED diagnoses (AN, BN, BED, and OSFED). Timely and accurate assessment of EDs can aid in early recognition and treatment of EDs and therefore reduce mortality rates and societal burden of these disorders.
Broad Overview of Current Assessment in EDs
Assessment is the foundation of both treatment of and research on EDs (Poston & Hanson, 2010). To date, ED assessments are used for several purposes, including determination of presence of an ED diagnosis, progress in treatment, and intensity of ED symptoms (including the following important domains: behaviors [e.g., restriction], cognitions [e.g., body dissatisfaction], and affect [e.g., fear of weight gain], and physiology [e.g., feeling full]). Currently, four types of assessments exist for EDs: Semi-structured interviews generally administered by a trained professional, self-report measures, task-based assessments, and technology-based assessments. In general, interviews (discussed in more depth below) are considered to be the most accurate type of assessment, but these can be lengthy and costly because they require a large amount of training to administer. Self-report assessments, including brief screening instruments, are easier to administer, but may be less reliable due to participant or client potentially misinterpreting the questions or desire to answer in a particular way (i.e., minimize symptoms). Task-based assessments (e.g., modified stroop task; Jones-Chesters et al., 1998) have the potential to eliminate these biases, but can be difficult to administer because they often require special equipment and laboratory environment. Finally, assessments using technologies such as ecological momentary assessment (EMA) and sensor technology are emerging, such as wearable watch or a ring that passively (i.e., without any effort from a participant) collects physiological data (e.g., heart rate), geolocation data, and so on (K. E. Smith et al., 2019). These tools have the potential to provide low-burden and low-bias assessments of ED behavior (i.e., gym attendance and exercise intensity) but are still in the nascent stages. We will review each of these areas below and provide recommendations on their usage for both clinical and research purposes.
Importantly, a recent systematic review of the literature found close to 100 different assessments related to ED pathology (Piotrowski, 2018; Schaefer et al., 2021). Inclusion of all 100 assessments is beyond the scope of this review paper. Our overall aim of this article is to provide new, cutting-edge evidence-based assessment guidelines and raise issues in need of current research. As such, we focused this review on high impact transdiagnostic, and dimensional assessments of ED cognitions and behaviors (symptoms) that are common across all EDs. We had two primary selection criteria for assessments we review. First, we only included measures (interview and self-report) that assess EDs transdiagnostically and focus on dimensions rather than diagnoses. In other words, we did not include assessments of specific disordered eating behaviors. Instead, we focused only on assessments that measure core ED behaviors (e.g., restriction and binge eating) AND cognitions (e.g., overvaluation of weight and shape), given that research suggests that transdiagnostic EDs are characterized by behaviors and cognitions (e.g., Fairburn et al., 2003). Second, we focused on assessments that demonstrated high impact in the field (>20 cites standardized by years in existence). The only exceptions to this rule were inclusion of the relatively new Eating Pathology Symptoms Inventory–Clinician-Rated Version (EPSI-CRV; Forbush et al., 2020) and the Screen for Disordered Eating Scale (SDE; Maguen et al., 2018). We included the EPSI-CRV because we think it has great promise and expect it to garner high impact in the future, and we included the SDE to compare with the SCOFF (Morgan et al., 1999) in primary care settings. Notably, we only included assessments that have strong psychometric properties for the assessment of EDs: We did not include any highly cited measures with poor measurement. Finally, we included task-based measures and technology measures as areas in need of additional research. Of note, we focus our review on measures primarily on adults but also note when assessments are supported in adolescent populations. Please see Tables 1 and 2 for a list of included and excluded measures, along with a justification for inclusion/exclusion.
Included Measures.
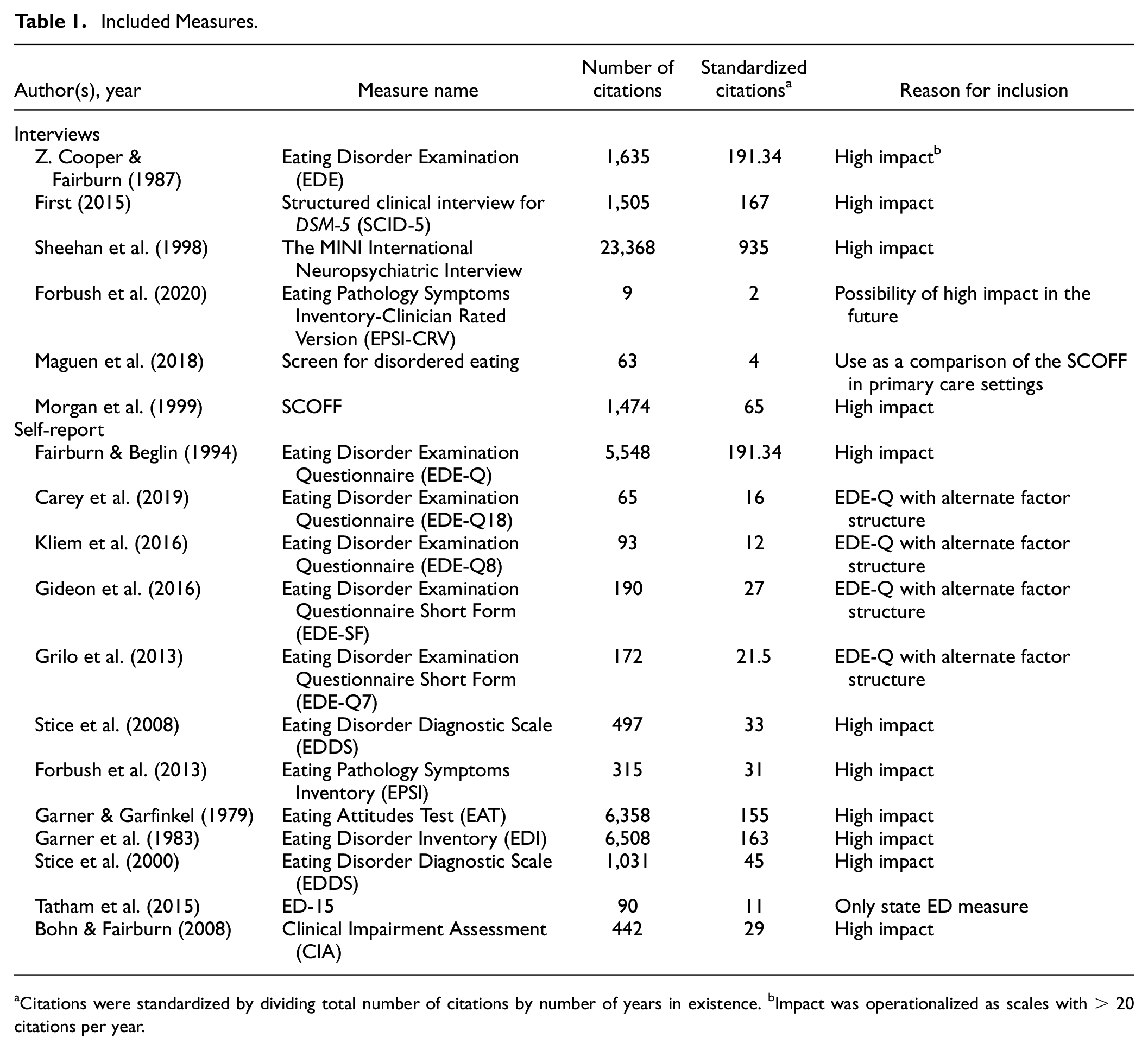
Citations were standardized by dividing total number of citations by number of years in existence. bImpact was operationalized as scales with > 20 citations per year.
Excluded Measures.
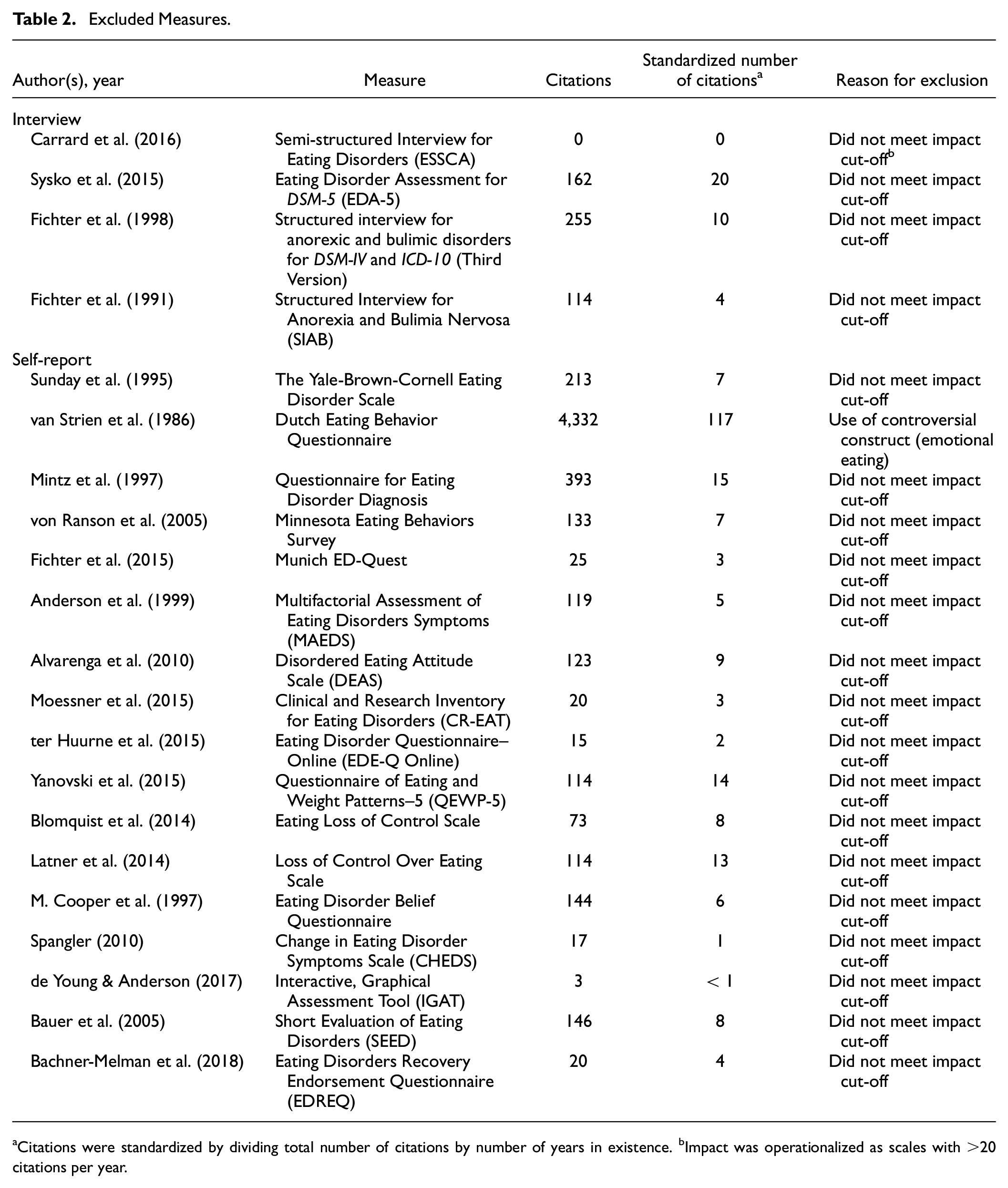
Citations were standardized by dividing total number of citations by number of years in existence. bImpact was operationalized as scales with >20 citations per year.
Current Eating Disorder Assessments
Structured and Semi-Structured Clinical Interviews
The Eating Disorder Examination (EDE; Z. Cooper & Fairburn, 1987) is a semi-structured interview designed to assess the full range of current ED psychopathology (cognitions and behaviors). The EDE is widely used and often considered the “gold standard for ED assessment” (Walsh et al., 2015). The EDE, 17th edition (EDE-17.0D; Fairburn et al., 2014) consists of 62 items that mainly focus on the previous 4 weeks (e.g., 28 days or 1 month). Each item includes at least one mandatory probe question, as well as optional supplementary questions designed to elicit sufficient information for the interviewer to make an informed rating. The EDE yields frequency data on key ED behaviors in terms of the number of episodes of a specific behavior or the number of days on which the behavior occurred, and subscale scores reflecting cognitive features of EDs, including the following four subscales: Dietary Restraint, Eating Concern, Weight Concern, and Shape Concern (Fairburn et al., 2014). In addition, there is an overall global score that is derived by taking the average of the four subscale scores. The EDE takes approximately 45 minutes to 1.25 hours to administer, generally by a highly trained professional, and is appropriate for ages 14 years and older (Fairburn et al., 2014; Walsh et al., 2015). It is important to note that administration of the EDE requires clinical expertise and specialized training to administer (Fairburn et al., 2014; Walsh et al., 2015). While psychometric data for the EDE-17.0D are not available in the primary publication, the psychometric properties of earlier versions support the reliability and validity of EDE scores (Berg, Peterson, Frazier, & Crow, 2012; Schaefer et al., 2021). Prior studies have also found that the EDE is able to capture clinically significant change across treatments (Fairburn et al., 2009; Le Grange et al., 2007).
Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013) Eating Disorder Modules (SCID-5; APA, 2013) is a semi-structured interview for making standardized DSM-5 (APA, 2013) diagnoses in adults. The SCID-5 Research Version (SCID-5-RV; First et al., 2015) contains a module for assessing diagnostic criteria for feeding and eating disorders (i.e., AN-R, AN-B/P, BN, BED, OSFED, and avoidant–restrictive food intake disorder [ARFID]) that include transdiagnostic ED symptoms. The SCID assesses both current and lifetime diagnoses and includes criteria for partial or full remission, which may be important to assess for clinical treatment and research purposes. The assessor is also prompted to obtain age at illness onset and to rate current illness severity. Administration time of the full SCID ranges from 1 to 2 hours; however, implementation and scoring of the ED module only can be completed in about 10 minutes (Walsh et al., 2015). Ideally, the SCID should be administered by an assessor who has sufficient clinical experience and knowledge of ED psychopathology and DSM diagnostic criteria to make informed clinical judgments about the interviewee’s responses. However, those with less knowledge or clinical experience can administer the SCID if they receive appropriate training under the supervision of an experienced assessor (Walsh et al., 2015).
There are currently no reliability and validity data available for SCID-5 eating and feeding disorder diagnoses, however, prior research provides support for the psychometric properties of earlier versions of the SCID (Lobbestael et al., 2011; Schaefer et al., 2021; Thomas et al., 2010; Walsh et al., 2015; Zanarini et al., 2000). For example, one study found evidence of fair interrater reliability (κ = 0.61) for SCID-IV diagnoses of EDs, while another found evidence of excellent interrater reliability (κ = 0.70; Lobbestael et al., 2011; Thomas et al., 2010). Similarly, another study reported excellent interrater reliability (κ = 0.77) and good test–retest reliability (κ = 0.64) for SCID-IV diagnoses of EDs (Zanarini et al., 2000). Our recommendation for usage of the SCID-5 ED modules is to use them in conjunction with another more specific assessment of ED pathology. Our team generally implements the SCID-5 in conjunction with the Eating Disorders Diagnostic Interview (EDDI; see below) to arrive at a clear ED diagnosis, as there is limited psychometric data on the ED modules administered on their own.
The EDDI (Stice et al., 2008) is a semi-structured interview that was adapted from the EDE by capturing the presence of each ED symptom (cognitions and behaviors) over the past month. Nondiagnostic items from the Weight Concern, Shape Concern, Eating Concern, and Dietary Restraint subscales of the EDE were omitted from the EDDI (Rohde et al., 2015). Items assessing ED symptoms in the past month are summed to create an overall ED symptom composite (Stice et al., 2008). Prior studies have shown that the symptom composite exhibits good internal consistency, test–retest reliability, interrater agreement, sensitivity to detect effects of ED prevention and intervention programs, and predictive validity for onset of depression (Rohde et al., 2015; Stice et al., 2008, 2011, 2013).
Eating Pathology Symptoms Inventory–Clinician Rated Version (EPSI-CRV; Forbush et al., 2020). The EPSI-CRV is a semi-structured interview for assessment of ED symptoms pathology in adults that is based on the self-report version of the EPSI (Forbush et al., 2013). This assessment is novel, but is included in this review because of its strong psychometrics, transdiagnostic assessment, and potential for high impact. The EPSI-CRV measures both dimensional nature of ED symptoms and generates a current DSM-5 ED diagnoses. The EPSI-CRV consists of 13 modules. Eight modules mimic self-report version of the EPSI and include Body Dissatisfaction, Binge Eating, Cognitive Restraint, Excessive Exercise, Restricting, Purging, Muscle Building, and Negative Attitudes Toward Obesity. Five additional modules are used to determine DSM-5 diagnoses: Subjective Binge Episodes, Binge Eating Disorder, Low Weight, Overvaluation of Weight and Shape, and Fear of Weight Gain. Items within each dimensional module are rated on a 5-point scale, ranging from 0 (not at all) to 4 (very often) based on the frequency of behaviors or cognitions. The module is then scored by adding up item responses to derive a total score. Modules that are used to determine ED diagnosis also include a categorical rating that is coded as absent, subthreshold, or present. The EPSI-CRV demonstrated good interrater reliability, convergent and discriminant validity, strong construct validity, and a good factor structure (Forbush et al., 2020). The EPSI-CRV takes approximately 40 minutes to administer and can be used in both clinical and research settings. The recommended training for administering EPSI-CRV includes knowledge of DSM-5 diagnostic criteria, competency in interviewing skills, and some basic knowledge of ED psychopathology. One benefit of EPSI-CRV is it was designed for the use in the community settings and specialty training in EDs is not required. EPSI-CRV may also be better at capturing ED pathology in diverse populations than other interviews (e.g., presence of muscle building subscale). Finally, the EPSI-CRV is highly structured and desired to minimize clinician or researcher interpretation and therefore bias.
The MINI International Neuropsychiatric Interview (M.I.N.I.; Sheehan et al., 1998) is a brief diagnostic structured interview designed to assess for the presence of Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994) and International Classification of Diseases, 10th Revision (ICD-10) psychiatric disorders. Sheehan et al. (1998) identified a need for a structured interview that could simultaneously meet the needs of academic research–oriented settings, clinical settings in psychiatry and psychology, and primary care settings that require brief and accurate screening measures (Sheehan et al., 1998). Early in the development of the M.I.N.I., Sheehan et al. (1998) recognized the implicit tradeoff between brevity and accuracy and ultimately decided to design each module to be slightly overinclusive to accept more false positives rather than miss true cases (Sheehan et al., 1998). The current version of the M.I.N.I. (English Version 7.0.2) consists of modules for the following DSM-5 and ICD-10 diagnostic categories, including AN, BN, and BED. Most of the modules include one or two screening questions to rule out the diagnosis when answered negatively (Lecrubier et al., 1997). Administration of the M.I.N.I. takes approximately 15 minutes and requires limited training; however, lay interviewers may require more extensive training relative to experienced clinicians (Sheehan et al., 1998).
The initial validation of the M.I.N.I. evaluated the diagnostic concordance among the M.I.N.I., the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders (3rd ed., rev.; DSM-III-R; APA, 1987; SCID-III), and the Composite International Diagnostic Interview (CIDI; Sheehan et al., 1998). The comparison of the M.I.N.I. and the SCID-III provided evidence of good to excellent diagnostic concordance, with kappa values of 0.90 and 0.78 for AN and BN, respectively (Sheehan et al., 1998). The comparison of the M.I.N.I. and the CIDI also showed good to very good diagnostic concordance, with a kappa value of 0.53 for lifetime BN (Sheehan et al., 1998). The M.I.N.I. also showed excellent interrater reliability for AN and BN, and good to excellent test–retest reliability for AN and BN, respectively (Sheehan et al., 1998).
Based on the available literature, we recommend using either the EDE or a combination of the SCID-V ED modules with another assessment (either EDE or EDDI) to capture accurate ED diagnoses. This combination allows for characterization of transdiagnostic EDs and includes all relevant cognitions and behaviors. In addition, although psychometric data are limited, the EPSI-CRV demonstrates strong promise as an interview assessment for EDs.
Self-Report in Clinical Practice and Research
Although clinical interviews are considered the “gold standard” for the assessment of EDs, they are often time-intensive and require extensive training to administer properly (Berg, Peterson, & Frazier, 2012). As an alternative, researchers have developed various self-report assessments that quickly and efficiently assess ED symptoms. Self-report assessments are particularly useful in settings that do not specialize in the diagnosis and treatment of EDs, as self-report instruments often require significantly less training and time to administer. Unsurprisingly, self-report ED assessments are frequently used among clinicians and researchers alike (Fitzsimmons-Craft et al., 2019; U.S. Preventive Services Task Force [USPSTF], 2022). Commonly used transdiagnostic ED self-report assessments that capture both cognitions and behaviors include the Eating Disorder Examination Questionnaire (EDE-Q; Fairburn & Beglin, 2008), the Eating Pathology Symptom Inventory (EPSI; Forbush et al., 2013), the Eating Attitudes Test (EAT; Garner & Garfinkel, 1979), the Eating Disorder Inventory (EDI; Garner et al., 1983), and the Eating Disorder Diagnostic Scale (EDDS; Stice et al., 2000).
Eating Disorder Examination Questionnaire Version 6
The EDE-Q is a self-report measure commonly used for diagnostic and screening and for assessment of ED severity (cognitions and behaviors) either in terms of treatment outcome or in terms of research purposes (Ayala et al., 2022; Mond et al., 2004). As a self-report alternative to the EDE, the 28-item questionnaire is similarly composed of four subscales measuring dietary restraint and eating, weight, and shape concerns, and utilizes the same 28-day time frame as the EDE. Instead of an interview, the 28-item EDE-Q uses 6-point Likert-type scales ranging from 0 days to everyday for each item (Mond et al., 2008). The convergent validity between the EDE and the EDE-Q is considered acceptable (Mond et al., 2004; Reas et al., 2011); however, individuals tend to score higher on the EDE-Q compared with the EDE (Mond et al., 2004). Research also suggests the EDE-Q sufficiently differentiates people with EDs from those without EDs, although the questionnaire is less adept at detecting the presence of binge-eating disorder (BED) and subjective binge-eating episodes (Aardoom et al., 2012; Berg, Peterson, Frazier, & Crow, 2012; Reas et al., 2006). Overall, data on the EDE-Q suggest that the factor validity is strongest for use of an overall subscale of ED symptom severity (Calugi et al., 2017; Peterson et al., 2007). Furthermore, a cut-off score of 2.3 is commonly used to indicate likelihood of clinically elevated ED symptoms (Mond et al., 2004). In addition to the full version of the EDE-Q, several shorter versions exist when time is a consideration for assessment, including the EDE-Q7, EDE-Q18, EDE-Q8, and EDE-SF.
Short Versions of the EDE-Q
The EDE-Q7 was developed by Grilo and colleagues (2013) and includes seven items with three subscales: dietary restraint, overvaluation of shape/weight, and body dissatisfaction. While the EDE-Q18 is also composed of three subscales, the subscales are restriction, weight/shape concern, and preoccupation/eating concerns (Carey et al., 2019). Alternatively, the EDE-Q8 (Kliem et al., 2016), comprised of eight items, provided support for the original four subscale model of the EDE-Q. Finally, Gideon and colleagues (2016) developed the Eating Disorder Examination Questionnaire Short Form (EDE-SF), which includes 12 items loading onto five factors. Because the EDE-SF evaluates the prior 7 days rather than the typical 28-day timeframe, it has been used by clinicians and researchers to measure treatment progress and research outcomes (Piya et al., 2021; Rom et al., 2022). Overall, the identified brief versions of the EDE-Q show acceptable psychometric properties, although some, such as the EDE-SF and the EDE-Q7, currently have greater evidence of strong validity and are used more frequently than others (Jenkins & Rienecke, 2019; Machado et al., 2020). Future research is needed from the field for consensus on which short form is ideal for usage in research and clinical work, although in general the EDE-SF and EDE-Q7 appear to have the best evidence of validity.
The Eating Pathology Symptom Inventory (Forbush et al., 2013) is a 45-item multidimensional measure developed to assess ED pathology (cognitions and behaviors) across a variety of populations. EPSI has six subscales: Body Dissatisfaction, Binge Eating, Cognitive Restraint, Excessive Exercise, Restricting, Purging, Muscle Building and Negative Attitudes toward Obesity. The items are rated on the Likert-type scale from 0 (never) to 4 (very often). The EPSI has demonstrated strong evidence for test–retest reliability, internal consistency, and convergent and discriminant validity across a range of samples in men and women (Forbush et al., 2014). The EPSI was designed to minimize gender and weight-related bias (Forbush et al., 2013, 2020). The EPSI has a strong factor structure and is able to differentiate between ED diagnoses (Forbush et al., 2013, 2014). Advantages of EPSI include separation of cognitive restraint and restriction constructs, inclusion of excessive exercise subscale, and muscle building subscale, which allows for more effective assessment of EDs in males. Overall, the EPSI is a very strong assessment of ED pathology, especially when implementing research from a latent variable perspective (i.e., use of subscales).
Eating Attitudes Test 26
Originally comprised of 40 items evaluating eating attitudes and behaviors (Garner & Garfinkel, 1979), the EAT was quickly shortened to its current version, the Eating Attitudes Test 26 (EAT-26), which includes 26 items with responses ranging from 0 (never) to 6 (always; Garner & Garfinkel, 1979). The EAT-26 is composed of three transdiagnostic subscales (dieting behavior, preoccupation with food and “bulimic behaviors” [p. 873], and self-control and external pressure regarding weight). As with the EDE-Q, researchers have identified differences in the factor structure during subsequent confirmatory factor analyses, although most studies demonstrate items loading onto either three or five factors (Rivas et al., 2010; Spivak-Lavi et al., 2021).
Although the EAT-26 has performed well in some cross-cultural replication studies (Asl et al., 2021; Kang et al., 2017), some research suggests the EAT-26 may not translate well across cultures and racial groups (Kelly et al., 2012; Spivak-Lavi et al., 2021). In addition, the EAT-26 demonstrates appropriate sensitivity to change, making it a useful tool for clinical trials or with health care settings (Hepworth et al., 2010). Although the EAT-26 has frequently been used as an assessment tool, Garfinkel and Newman (2001) advised caution for use as a screening tool in community samples due to evidence suggesting its relatively low sensitivity with nonclinical populations. This continues to be a concern among some researchers (McEnery et al., 2016).
Eating Disorder Inventory Version 3
The EDI was first developed to assess cognitions and behaviors of AN and BN but has since been adapted to include additional transdiagnostic EDs. The first edition of the EDI included 64 items with responses ranging from 0 (never) to 6 (always). The most recent version, the 91-item Eating Disorder Inventory Version 3 (EDI-3; Garner, 2004), was developed by Garner in 2004 and is composed of three ED-specific subscales (drive for thinness, bulimic behaviors, and body dissatisfaction) in addition to nine subscales measuring associated mental health symptoms (“low self-esteem, personal alienation, interpersonal insecurity, interpersonal alienation, interoceptive deficits, emotional dysregulation, perfectionism, asceticism and maturity fear” [Clausen et al., 2011, p. 102]). Clausen et al. (2011) tested the psychometric properties of the EDI-3 using confirmatory factor analysis, and results aligned with Garner’s original factor structure. In addition, the EDI-3 demonstrates acceptable detection of positive ED cases and non-ED cases as well as good internal consistency and construct validity (Clausen et al., 2011; Cumella, 2006). Unlike other ED diagnostic tools, the EDI-3’s assessment of ED adjacent subscales could provide additional context about participant responses to the ED subscales. However, research suggests the EDI-3 may be less appropriate to use with men (Stanford & Lemberg, 2012). A final consideration is that the EDI-3 is copyrighted, and researchers and clinicians must pay for its use, limiting its ability to be a widely inclusive assessment.
Eating Disorder Diagnostic Scale (EDDS) is a 22-item self-report tool that assesses a variety of cognitions and behaviors associated with AN, BN, and BED within the past 3 to 6 months. The scale utilizes a variety of response options, including items that are dichotomous, multiple-choice, and based on frequency of ED behaviors, all of which are summed to create the total score. Higher scores likely indicate more severe ED pathology. Because the EDDS is based on the diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders (APA, 2013), it is frequently used as a tool to diagnose EDs and can be used as a self-report assessment to determine diagnoses (Bankoff et al., 2016). However, limitations of the EDDS include its relatively high identification of false-positive cases and suboptimal psychometric properties across gender and racial/ethnic groups (Kelly et al., 2012). Notable advantages of the EDDS include the assessment of BED behaviors and ability to detect BED as well as its sensitivity to change, which makes it a useful tool for monitoring treatment progress.
Eating Disorder–15 is a brief 10-item assessment that measures ED cognitions and behaviors over the prior 7 days (Tatham et al., 2015). It consists of two subscales, namely, the Weight/Shape concern subscale and the Eating Concerns subscale, which measure “near identical constructs” to the EDE-Q (Tatham et al., 2015, p. 1005). Similar to the EDE-Q, the ED-15 has high internal consistency, sensitivity, and test–retest reliability, making it a useful tool for measuring rapid changes in ED symptomology in both clinical and research settings (Rodrigues et al., 2019; Tatham et al., 2015). Tatham and colleagues (2015) note, however, that although the ED-15 is useful for session-by-session monitoring, it should be used in conjunction with longer measurement tools to assess change in overall symptoms over extended periods of time.
State ED Assessments
State assessments measure psychological phenomena that are unstable across time and can be affected by a variety of internal and external factors (Cole et al., 2005; Hertzog & Nesselroade, 1987). Despite evidence demonstrating differing physiological and emotional states can impact disordered eating behaviors (Dingemans et al., 2017; Leehr et al., 2015), the ED literature is currently lacking state assessments of transdiagnostic ED cognitions and behaviors (i.e., symptoms). In recent years, however, two brief measures have been developed to measure changes in ED symptoms across a brief period of time (7 days): EDE-SF and the ED-15. In contrast to most ED assessments that assess symptoms over extended periods of time, usually a month or longer, the ED-15 (Tatham et al., 2015) evaluates symptoms within the past 7 days, making it better suited to track session by session changes in ED symptoms (Tatham et al., 2015). In addition, the brevity and efficiency of the ED-15 make it more conducive for consistent use and monitoring of rapid changes in symptoms throughout treatment. Similarly, the EDE-SF mentioned previously is used to measure rapid changes in treatment by evaluating the prior 7 days of treatment (Piya et al., 2021; Rom et al., 2022). Development of an ED state measure is a crucial need for the ED field, as such a measure could be used in experimental, prospective, and momentary study designs to assess current levels of ED symptoms.
Recommendations for Self-Report Assessments
Usage of self-report assessments depends heavily on the intended function of the assessment. In general, the EPSI has the strongest psychometric reports for use in research populations when research is centered from a traditional disease model and drawing from latent variable theory (Forbush et al., 2016). The EDE-Q is a strong measure in terms of symptom report and can be used either in its original or in its short form in both research and clinical work to determine symptom severity, and when research is drawing from a network perspective (i.e., symptom reports; Mond et al., 2004). The EDDS is advantageous for diagnosis when an interview is too timely or costly. In general, self-report assessment should consider the function, purpose, and feasibility of their assessment when selection is made. Notably, additional self-report measures that measure either specific ED behaviors only or eating styles (rather than symptoms; for example, emotional eating) not discussed, but also warranting consideration dependent upon the construct/symptom of interest are the Dutch Eating Behavior Scale (Van Strien et al., 1986), the Binge Eating Scale (Gormally et al., 1982), and the Yale-Brown-Cornell Eating Disorder Scale (Sunday et al., 1995). For a full systematic review of self-report assessments, see Schaefer et al. (2021).
Screening Assessments for Use in Primary Care and Other Health Care Settings
Research suggests early detection and treatment of ED cognitions and behaviors (i.e., symptoms) is associated with better health and psychological outcomes, including shorter duration of illness, decreased symptom severity, and increased ED recovery rates (Austin et al., 2021; Treasure et al., 2015). In addition, some research suggests that simply screening for EDs may not significantly facilitate increased treatment-seeking behavior among people at risk of an ED, indicating a possible need for the simultaneous provision of screening and treatment interventions (Shah et al., 2022). Furthermore, EDs are most often detected and diagnosed by a primary care provider (PCP; Striegel-Moore et al., 2008), signifying the need for accurate and comprehensive ED screening assessments that can be used within primary and other health care settings. Unfortunately, researchers have observed inconsistent and insufficient use of ED assessments among many PCPs, who often report feeling ill-equipped to assess and treat EDs (Currin et al., 2009; Linville et al., 2013; Thompson-Brenner et al., 2012). However, there is evidence suggesting that when PCPs are provided appropriate ED-specific training and support, they are more likely to assess and identify patients with EDs, and subsequently, provide a higher number of referrals to specialized ED services (Linville et al., 2013; Wade et al., 2022). When PCPs do conduct ED assessments, they frequently use brief self-report screening tools such as the SCOFF or the Screen for Disordered Eating (SDE), rather than more time-intensive diagnostic assessments such as the EDE-Q (Johnston et al., 2007). Below we review assessments that can be used in primary care settings.
SCOFF
Morgan and colleagues (1999) created the five-item SCOFF questionnaire, which is the most frequently used transdiagnostic ED screening tool in primary care settings, possibly due to its brevity and satisfactory ability to discriminate between individuals with and without EDs (Hay et al., 2022). SCOFF is an acronym based on the first letter of the five questions assessing for ED symptoms: Sick (self-Induced vomiting), control (feeling out of control around food), One (weight loss of one or more European Stones), Fat (belief that oneself is larger than others claim), and Food (feeling that food dominates one’s life). The five dichotomously scored items assess the presence of cognitive or behavioral symptoms of AN and BN, and endorsement of two or more items indicates clinically significant ED symptoms. Although the SCOFF demonstrates an adequate ability to identify people with AN and BN, research indicates it is less sensitive in detecting other EDs, including BED and OSFED (Kutz et al., 2020; Solmi et al., 2015). In addition, the USPSTF (2022) indicates there is currently a lack of evidence regarding its use with adolescents, men and gender-diverse individuals, and among racial and ethnic minorities.
Screening for Disordered Eating
Maguen and colleagues (2018) combined select items from previous ED assessments to develop the SDE in an attempt to increase identification of BED and other transdiagnostic disordered eating behaviors in primary care settings. Like the SCOFF, the SDE is composed of five items that assess common ED symptoms. Also similar to the SCOFF, the SDE uses a cutoff score of two or more affirmative responses. Unlike the SCOFF, however, the SDE assesses for episodes of binge eating, making it a promising tool for identifying BED in primary care settings. In a comparison between the two measures, the SDE demonstrated greater detection of AN, BN, and BED compared with the SCOFF (Maguen et al., 2018). However, more research is needed as there is not yet sufficient evidence to make definitive claims about the superiority of either screening tool.
Recommendations for Screenings in Primary Care
Our recommendation for screenings in primary care is to use the SDE to ensure comprehensive assessment of all EDs. However, use of either the SCOFF or SDE is encouraged. Finally, clearly given the lack of evidence on screening tools for EDs and high prevalence of treatment seeking in these settings, this area is a high priority area for future research.
We will now briefly review additional areas of assessment that are needed to broadly assess ED symptoms, including an emphasis on areas that are in need of future research.
Assessment of Comorbidities
EDs are highly comorbid with multiple additional mental disorders, including, but not limited to, depression, social anxiety disorder, obsessive compulsive disorder, post-traumatic stress disorder, generalized anxiety disorder, and substance use disorders (Pallister & Waller, 2008; Pearlstein, 2002; Vagg et al., 1980; Van Alsten & Duncan, 2020). While a review of the assessments for each of these conditions is beyond the scope of this article, we highly recommend assessment of these disorders, in addition to ED symptoms to gain a full picture of ED pathology. We also highly recommend that researchers and clinicians who specialize in anxiety and depression include assessments of EDs, given that EDs are significantly elevated in these populations (Garcia et al., 2020). Furthermore, recent research has shown, in particular, that social appearance anxiety (i.e., fear of evaluation of one’s appearance), shame, perfectionism, and self-criticism are core aspects of ED pathology (Bardone-Cone et al., 2007; Levinson et al., 2021), indicating that these constructs are also extremely relevant for assessment.
Ecological Momentary Assessment
A major limitation of interview, self-report, and screening assessments is that most require individuals to report on cognitions, behaviors, and emotions that occurred prior, which introduces recall biases (Berg, Peterson, & Frazier, 2012; Ebner-Priemer et al., 2006) and that these assessments are generally focused on one time point, which limits the ability to explore symptom dynamics (Stone & Shiffman, 1994). In response to concerns with response bias and in an effort to increase the ability to capture processes across time, new types of assessments have been developed. EMA, also called experience sampling or time-series methodologies (Trull & Ebner-Priemer, 2009; Walz et al., 2014), is an assessment method that uses repeated real-time sampling of a person’s current behavior, emotions, and cognitions in their natural environment. EMA generally involves prompted (time-contingent) or participant-initiated (event-contingent) self-report ratings focused on how participant feels “in the moment” and any behaviors they have engaged in since last check-in. In general, EMA typically measures state versus trait psychological constructs (e.g., body dissatisfaction experienced in the moment rather than in general). For more information on EMA, see Stone and Shiffman (1994) for a review. We will concentrate our discussion on EMA for the assessment of EDs.
Current EMA Assessments for ED
Research
EMA assessments can capture antecedents and consequences of ED behaviors (e.g., how an emotion may lead to a behavior or vice-versa) and can provide insight on the frequency and patterns of ED symptoms (e.g., change in symptoms at different times of the day; Engel et al., 2016), both of which are important for clinical work and research-focused investigations. To date, EMA assessment items have typically been developed for each study by modifying questions from existing self-report measures. For example, Engel et al. (2013) asked participants whether they engaged in a variety of ED behaviors since last check-in, such as binge eating, loss of control eating, and vomiting. Other measures include ED-related cognitions such as analog scale asking participants to rate how dissatisfied they were with their body since last check-in (Fitzsimmons-Craft et al., 2015). Another EMA measure included items to assess behaviors, cognitions, and emotions both in general and around mealtimes in individuals with EDs (e.g., I felt guilty during the most recent meal; Levinson et al., 2022). The most comprehensive ED EMA measure to date consists of 56 items assessing common behavioral, cognitive, and emotional symptoms of EDs as well as related transdiagnostic constructs and comorbidities (Levinson et al., 2021). One major limitation of EMA measures is lack of evaluation of psychometric properties, although past studies found convergence of EMA assessments with retrospective measures (Engel et al., 2016).
Clinical
Finally, Recovery Record is a clinical tool that adapted self-monitoring (a primary intervention in gold-standard treatments for EDs; Fairburn & Beglin, 2008) to an easy-to-use mobile application format that is used with clinician–patient pairs (Tregarthen et al., 2015). Recovery Record assesses daily ED symptoms, food intake, and current cognitions. In addition to Recovery Record, there are three additional commercialized applications with evidence-based assessment elements (Wasil et al., 2021). However, only Recovery Record was reported to have feasibility and acceptability compared with paper–pencil methods (Keshen et al., 2020; Lindgreen et al., 2018). This technology has strong support for its utility and shows how assessment methodologies can be integrated into clinical use (Goodwin et al., 2019; Peis et al., 2020).
Recommendations for EMA
EMA is a rapidly burgeoning area of assessment in the EDs, which has primarily been used for research purposes. There are many existing EMA assessments that have been used; however, few (if any) have had their psychometric properties tested. This area is also an area of high priority for additional research. Research is needed to establish comprehensive and uniform use of EMA in research that captures relevant aspects of EDs and related comorbidities. Finally, there is some research showing the utility of EMA-like tools for use in clinical treatment. Again, more research is needed to expand upon the best ways to use EMA in clinical settings. For example, EMA could be used to track progress across treatment or could be integrated into electronic medical records to help establish and guide evidence-based treatment.
Behavioral Tasks
Laboratory Tasks
Another area of growing interest for assessment is the use of objective assessments of behavior. For example, behavioral tasks such as modified stroop, modified dot-probe (MacLeod et al., 1986), Go/No-Go, visual search task, word association, and anagrams as well as psychophysiological methodologies such as eye-tracking, startle eye-blink modulation and facial electromyography, event-related potentials, positron emission tomography, and functional magnetic resonance imaging have been shown to identify ED symptoms, cognitions, and behaviors more implicitly (see systematic and methodological review for more details on these methods; Ralph-Nearman, Achee, et al., 2019). An examination of literature with implicit processing, and automatic approach and avoidance responses to ED-related stimuli (e.g., food, body, and perfectionism) demonstrated that while behavioral responses were typically similar across ED diagnoses transdiagnostically, that diagnostic differences immersed with those studies that also included psychophysiological assessments (Ralph-Nearman, Achee, et al., 2019).
Assessment in the Natural Environment
Outside the laboratory, behavioral tasks, smartphone applications, and wearable sensor technologies are being developed to assess EDs and related symptoms. These tools may include self-assessment and passive monitoring (see review of digital psychiatry tools: Torous et al., 2021) as well as more implicit and visual assessments in individuals’ everyday life. Both behavioral avoidance of ED stimuli (such as high-fat body size or food) and body image disturbance (such as overestimation of body size, or body dissatisfaction) increase risk of relapse in EDs and are therefore crucial behaviors to assess (e.g., Carter et al., 2012; Keel et al., 2005).
Behavioral Avoidance Assessments
Behavioral avoidance of ED stimuli, such as high-fat food and high body mass index (BMI), is predictive of ED relapse and related to ED pathology. One such multi-platform assessment, the Approach-Avoidance task (AAT), has recently been developed (Ciotti et al., 2022). This tool assesses the implicit processing of visual body- and food-related stimuli. See Brockmeyer et al. (2020), Lender et al. (2019), and Neimeijer et al. (2019) for more information. The advantage of this assessment is the objective measurement of implicit cognitive biases toward food and body present in EDs.
Visual Body Image Disturbance and Concerns Assessments
Body-related disturbance are made up of perceptual (e.g., body size distortion) and attitudinal (e.g., body dissatisfaction) aspects and are a key cognitive symptom that drives ED pathology (e.g., Metral et al., 2014; Stice, 2002) and a criterion for diagnosing EDs (e.g., AN; APA, 2013). A new digital multi-platform to assess multidimensional aspects of body-related disturbance, called Somatomap (Ralph-Nearman, Arevian, et al., 2019; Ralph-Nearman et al., 2021), has demonstrated high reliability as a perceptual marker of visual body image disturbance in AN (Ralph-Nearman, et al., 2023). See Ralph-Nearman, Arevian, et al. (2019) for more information on this tool.
The Affect Misattribution Procedure (AMP; Payne et al., 2005) is a computer-based measure to assess automatic affective reactions or implicit affect by indexing reactions to stimuli such as larger bodies and high-calorie food pictures (Spring & Bulik, 2014). The AMP has been adapted for use in remote settings to detect negative implicit evaluations of eating and food-related stimuli. The AMP was shown to predict ED symptoms and behaviors overtime (A. R. Smith et al., 2018) and represents an additional behavioral assessment that can be used to assess ED pathology.
Physiological Indices
Another area of potential promise in terms of objective assessment is psychophysiological assessment. Wearable physiological sensors have shown some promise in passively detecting the pre-onset of problematic behavioral episodes in other illnesses such as predicting epileptic seizures (Meritam et al., 2018), autistic outbursts (Goodwin et al., 2019), and discharge timing for hospitalized patients with severe depression (Peis et al., 2020). Recent research has begun to explore passive sensor technology in relation to ED symptoms and prediction of relapse. For example, recent research has found that global positioning system can predict binge eating (Juarascio et al., 2015) and that passively collected physiological data combined with machine learning analytics can predict purging behaviors (Ralph-Nearman, et al., in press 2023). This type of assessment may provide a new methodology for easy to collect, low-burden assessment of ED psychopathology (see K. E. Smith et al., 2019, for a review).
Recommendations for Objective Assessments
To date, there are few objective assessments of ED symptoms and related pathology, although some newer measures, including measures of body and food avoidance, perceptual body disturbances, and implicit attitudes toward food and body, are in existence. This area is one with great promise and more research is needed to both develop objective assessments and test how to best implement these assessments into research and clinical settings.
Summary of Existing Assessments
Overall, there are data suggesting that the EDE, SCID-V, EPSI-CRV, and EDDI are strong interview assessments. There is support for several self-report assessments, including the EPSI, EDE-Q, and EDDS, although consideration for the perspective and function of assessment should be considered when selecting assessments. There are two current short assessments that can be used in primary care/health care settings, the SCOFF and SDE. The SCOFF’s primary limitation is that it does not assess for binge eating, which may limit detection of many binge-spectrum EDs. Assessment of comorbidities should be prioritized and researchers and clinicians working with anxiety and depression should strongly consider inclusion of ED assessments. There are currently no assessments of state ED in existence. EMA is a promising area for dynamic assessment and integration into clinical practice, but more research is needed specifically to develop psychometrically strong assessments. Finally, behavioral assessments such as the AAT, Somatomap, and physiological indices hold promise for more objective measurement of EDs.
We want to note that our inclusion criteria for assessments in the current view is limited to measures that captured cognitive-behavioral dimensional, transdiagnostic, and had citations >20 a year. This definition is somewhat arbitrary and it is possible that some strong assessments with high utility may not meet this criteria.
Next, we will review considerations for use of the assessments we have discussed above. In particular, we will discuss assessment use in research versus clinical practice, assessment setting (specialty clinic vs. general health care), assessments for diagnostic and treatment planning, use of categorical assessment, and measurement-based care.
ED Assessments in Research and Clinical Practice
In addition to their clinical utility, ED assessments are often imperative for ED and non-ED researchers alike. They are frequently used in research settings to screen prospective participants, identify categorical or dimensional illness characteristics between participants or groups, and evaluate the effectiveness of clinical interventions and treatments (Catalan-Matamoros et al., 2011; Kristeller et al., 2014; Wagner et al., 2016). For example, many randomized controlled trials on clinical treatments for EDs use the EDE and/or the EDE-Q as an outcome variable to identify changes in ED symptomatology over time, either within a single individual or between distinct groups, which can be used to illustrate the possible efficacy and impact of a particular treatment or intervention (Le Grange et al., 2007; Linardon et al., 2022; Wagner et al., 2016). Given the current recommendations by the USPSTF (2022), researchers should analyze the disadvantages and benefits of using a particular assessment, especially when used in populations where sufficient empirical support is still lacking (adolescents, gender-diverse individuals, gender and ethnic minorities, etc.).
Assessment Goals Based on Setting (e.g., Emergency Room vs. Specialized ED Services)
Current guidelines on the management of EDs emphasize the importance of early detection and its potential to improve outcomes, including likelihood of recovery (Johns et al., 2019; Peat & Feltner, 2022; Raffoul et al., 2022). Primary care and emergency department settings are well suited for the screening and early detection of EDs, as they are often the first point of contact for any health-related complaints (Dooley-Hash et al., 2012; Peat & Feltner, 2022; Redekopp et al., 2022; Striegel-Moore et al., 2008). However, the USPSTF (2022) was unable to recommend the routine screening of EDs in adolescents and adults in primary care settings due to a lack of direct evidence on the benefits and harms associated with such screenings (Feltner et al., 2022; Peat & Feltner, 2022). This decision is undoubtedly disappointing for ED clinicians and researchers, and it is in direct conflict with guidelines and recommendations from several professional organizations who advocate for routine screening for EDs, including the American Academy of Pediatrics, the Academy for Eating Disorders, and the American Association of Family Physicians (Academy for Eating Disorders, 2021; Harrington et al., 2015; Hornberger et al., 2021; Peat & Feltner, 2022). In light of these seemingly conflicting recommendations, it is important to consider that the definitions and goals of “screening” and “diagnosis” differ across treatment settings (i.e., primary care and emergency departments vs. ED-specific services; for example, Peat & Feltner, 2022).
In the primary care and emergency department settings, screening refers to the possible identification of an unknown disease using rapid tests, examinations, or other procedures in seemingly well individuals who present for routine care (Hill et al., 2010; Peat & Feltner, 2022; Wilson & Jungner, 1968). Importantly, screening is not meant to be diagnostic and is not intended to be implemented in patients presenting with obvious signs or symptoms of EDs (e.g., underweight as defined by BMI) or seeking ED-specific care (Peat & Feltner, 2022). As such, the goal of screening in primary care and emergency department settings is to differentiate between patients who likely do not have an ED from those who likely have an ED and may benefit from additional, more in-depth assessment and treatment (Peat & Feltner, 2022).
In contrast, the definition of “screening” in specialized treatment settings and research trials is broader and includes the identification of a specific clinically significant ED and ongoing monitoring of symptom severity (Peat & Feltner, 2022). In addition, patients seeking care at ED-specific treatment settings and research trials typically present with obvious signs and symptoms of EDs (e.g., underweight, restriction, and inappropriate compensatory behaviors). Notably, the USPSTF (2022) excluded studies that focused on underweight populations because patients presenting for care with obvious signs and symptoms of a disorder fall outside the scope of routine screening in primary care settings (Peat & Feltner, 2022). Furthermore, assessment tools commonly used by ED specialists, such as the EDE, the SCID-V ED modules, or the EDDI, are long, difficult to interpret, and require extensive clinical experience and knowledge regarding ED psychopathology and DSM-5 diagnostic criteria. However, to be useful within the context of a primary care or emergency department visit where time is limited, screening measures must be accurate, brief, and require little to no training prior to implementation in routine practice (Peat & Feltner, 2022). Taken together, measures routinely used by ED clinicians and researchers are neither appropriate nor practical for routine use in primary care and emergency department settings, and the implementation of these measures in individuals presenting with obvious signs and symptoms of EDs deviates from the notion of screening as a preventive service (Hill et al., 2010; Peat & Feltner, 2022).
While the USPSTF (2022) concluded that the evidence was insufficient to assess the balance of benefits and harms of screening for EDs in adolescent and adults, they identified several screening questionnaires that could be used in primary care settings for individuals without obvious signs and symptoms of EDs, including the SCOFF (Hill et al., 2010; Morgan et al., 1999; Peat & Feltner, 2022). The SCOFF questionnaire is a brief, validated five-item tool designed to address core features of AN and BN, and has been the dominant screening tool used in primary care settings over the past three decades (Hay et al., 2022; Hill et al., 2010; Morgan et al., 1999). The USPSTF found adequate evidence on the accuracy of the SCOFF for screening EDs in adult females; however, the evidence is insufficient for other populations, including adolescents and males (USPSTF, 2022).
Overall, there is a strong need for the additional studies on the benefits and harms of screening in diverse populations to better reflect the demographics of patients presenting to primary care and emergency department settings (Feltner et al., 2022; Hay et al., 2022; Peat & Feltner, 2022). In addition, most of the existing screening tools were designed to detect AN and BN, but not EDs that were introduced in the DSM-5, including ARFID and atypical anorexia, or EDs in diverse populations, such as racial minorities, males, individuals in larger bodies, and transgender youth (Feltner et al., 2022; Hay et al., 2022; House et al., 2022; Nagata & Golden, 2022).
Assessments for ED Diagnosis and Treatment Planning
Diagnoses and Implications for Treatment Planning
There are two main frameworks to conceptualize and assess ED diagnosis for treatment planning, which are (a) categorical assessment or (b) dimensional and transdiagnostic assessment. Categorical assessment follows the most current Diagnostic and Statistical Manual of Mental Disorders (DSM-5; APA, 2013) and views EDs as several distinct and separate mental illnesses (i.e., AN, BN, BED, and OSFED). This viewpoint is based on the medical model and is often used by insurance companies for reimbursement purposes, for inclusion into certain clinically based ED programs, and in research for inclusion into clinical trials (Mond et al., 2004). Alternatively, the dimensional and transdiagnostic approach, following the Transdiagnostic Theory for EDs (Fairburn et al., 2003), is in line with more recent viewpoints on psychopathology, such as the network perspective (Cramer et al., 2010); conceptualizes EDs as having shared underlying mechanisms and symptoms; and conceptualizes pathology on a continuum of severity. Conceptualization of EDs as either categorical or continuous has implications for the assessments of corresponding pathology.
Limitations of Categorical Diagnosis for Assessment
In some instances, categorical diagnoses may prove to be problematic for accurate assessment. For example, the primary difference via assessment between AN and OSFED AAN is if the individual is over or under 18.5 body mass index (BMI). However, most research points to these illnesses as being more similar than different behaviorally and cognitively. One area of assessment that is particularly problematic with this distinction is in the ability to capture AN versus atypical AN versus AN in partial remission. For example, when an individual is weight restored above 18.5 BMI, they would technically be considered as meeting criteria for atypical AN if assessment is not done on prior weight loss. In this example, a diagnosis of AN in partial remission may be more appropriate. An additional limitation of current categorical conceptualizations is that individuals diagnosed with a specific ED, such as AN, will often migrate to a different ED category (e.g., Fichter et al., 2017). These examples point to (a) the limitations of relying on categorical markers (BMI categories) and (b) the need for detailed information on both current and prior indicators of pathology. These issues point to the need for both categorical (e.g., structured clinical interviews) assessments that provide diagnostic information and dimensional (e.g., EDE-Q and EPSI) assessments that provide more detailed dimensional assessment of ED pathology.
Inclusion of ED Measures in Anxiety and Depression Assessments
As discussed above, EDs are highly comorbid with additional psychological disorders, most notably anxiety and depression. Despite this fact, few anxiety and depression researchers routinely include ED assessments both in research and in clinical practice (Mond et al., 2004). We highly recommend that any researcher or clinician working with anxiety and depression include routine questions to screen for EDs. If a short screening measure is needed, we recommend using the SCOFF or SDE. If there is room or need for additional assessment, we recommend using the EDE-Q or EPSI as self-report assessments of ED symptoms. More work is needed to implement ED assessment routinely in these settings, including work on how ED researchers can work with depression and anxiety researchers and clinicians to implement existing or develop new assessments that can easily be integrated into routine depression and anxiety assessment settings.
Measurement-Based Care for EDs
Measurement-based care is the systematic evaluation of patient symptoms before or during a psychotherapy session to inform treatment that has been utilized in the treatment of depression and anxiety disorders (Lewis et al., 2019). Measurement-based care includes administering symptom, outcome, or process measure at each session, clinician review of data, sharing data with patient, and collaborative reevaluation of the treatment plan informed by data. Measurement-based care helps detect failure to respond to treatment, worsening of symptoms, or symptom improvement as well as helps engage patients in treatment (Simon et al., 2013).
Measurement-based care for EDs has used the EDE-QS, which is a 12-item 7-day recall measure of ED symptoms to assess weekly changes in ED symptoms (Gideon et al., 2016). A measurement-based care model is used by the National Health Service in the United Kingdom and is referred to as patient-reported outcome measures (PROMs; Austin et al., 2021). Initially, PROMs included the EDE-Q (Fairburn & Beglin, 1994) and the Clinical Impairment Assessment Questionnaire (CIA; Bohn & Fairburn, 2008). However, more recently individualized i-PROMs have been piloted, where patients write in their symptoms and rate them on a severity scale (Austin et al., 2021). In the United States, outcome measurements at admission and discharge are becoming a common practice in ED treatment (Attia et al., 2017), although measurement-based care has not been widely implemented and is not standard. More research on the use of measurement-based care in countries outside of the United Kingdom is needed.
Future Directions for ED Assessment Research
Ecological Momentary Assessment
One area in need of more research is on the development of psychometrically strong EMA measures that capture (a) ED symptoms, (b) co-occurring conditions, and (c) mechanisms that maintain ED (e.g., perfectionism and self-criticism: Bardone-Cone et al., 2007; Levinson et al., 2021). The development of comprehensive and standard measures in momentary can be used in both research and clinical settings. For example, in research this type of assessment could better capture momentary dynamics among ED symptoms in daily life, which can lead to the development of personalized treatments and better conceptualization of the cyclical nature of ED symptoms. In clinical settings, these types of EMA assessments could be integrated into electronic health records or given throughout treatment for measurement-based care. This type of integration could provide feedback to clinicians on how to tailor treatments.
Network Theory
Given the emphasis in this review on transdiagnostic assessment, we will discuss network theory, given its emphasis on symptom dimensions as underlying pathology. Notably, we do not review other dimensional systems such as HITOP but instead refer the reader to other sources for this information (e.g., Kotov et al., 2022). To date, most assessments have been developed based on latent variable theory and use factor analysis to distinguish which constructs underlie assessments (Fitzsimmons-Craft et al., 2019). For example, the EPSI is a strong measure of ED pathology that was developed with several factors mapping onto subscales of binge eating, purging, dietary restraint, and so on (see description of EPSI above; Forbush et al., 2013). However, as additional perspectives on how psychopathology arises and maintains itself become more mainstream, new types of assessments may be needed. Specifically, network theory proposes that psychopathology arises and maintains itself through dynamic relationships among symptoms (for more information see Cramer et al., 2010). Notably, because most assessments were not developed for network theory, these assessments may not be the best way to capture psychopathology through a network perspective. Instead, measures that comprehensively assess the entire scope of psychopathology symptoms may be needed. For an example, please see work by Cusack et al. (2022), who developed a measurement of interoceptive sensations in EDs based on a network perspective. More research is needed to develop and test assessments developed stemming from a network theory perspective.
Timescale
As mentioned above, there are currently no assessments of state ED symptoms. More research is needed to develop ED assessments across a variety of timescales. For example, the EDE-Q has been developed into multiple versions that assess timescales ranging from 7 to 28 days. However, given the fact that ED symptoms have high variability, even within moments, more research is needed to develop ED assessments on multiple time scales ranging from seconds to months.
Summary
There are several strong assessments of ED psychopathology, including structured clinical interviews, self-report assessments, and behavioral assessments. We provide recommendations on how to best use these assessments for clinical and research purposes, including recommendations for screening in health care settings and in clinical and research settings focused on anxiety and depression. We also discuss several considerations for integration into clinical practice and treatment outcome research, including the limits of a categorical diagnostic system and need for more dimensional or symptom-based assessment. Finally, we provide recommendations for future research, including the need to develop strong EMA measures, capture objective measures possibly through passive sensing, and consider development of assessments that capture psychopathology from a network perspective. Overall, there is much work left to do in the area of ED assessment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.