
Abstract
No tools quantify the experience, psychological, and practical impact of receiving a diagnosis from a non-deficit perspective. Autism is increasingly late diagnosed in adulthood. The Impact of Diagnosis Scale (IODS) was initially developed for borderline personality disorder. We aimed to develop a revised version suitable for autistic adults and potentially other diagnostic groups. Following a trial of a preliminary revision, the researchers and autistic research advisors co-produced an expanded pool of 46 items, scored on 7-point Likert-type scale, within 6 hypothesized domains. Scale reduction processes were applied to data from 125 formally diagnosed autistic adults. Following iterative rounds of factor analysis using maximum likelihood estimation with Promax rotation, 22 items were retained across 4 domains to comprise the IODS-R. The IODS-R adds new understanding to the experience of receiving an autism diagnosis in adulthood. It may be useful for evaluating diagnostic services and other diagnostic groups.
Psychologists and other health professionals frequently communicate potentially life-changing diagnoses. Although qualitative researchers have theorized the impact of autism or other mental or physical health diagnosis on self-concept and everyday life (Bury, 1982), no measurement tool quantifies this phenomenon from a neutral, non-deficit perspective (e.g., Asif et al., 2016; Mcbride et al., 2000). This is particularly relevant to the situation of late-diagnosed autistic adults 1 who have lived the majority of their lives without an explanation for their experiences of significant differences and difficulties (Huang et al., 2020).
A number of quantitative and qualitative studies have examined the experiences of receiving medical diagnoses. Studies of physical health diagnoses tend to use quantitative methods and mainly report negative outcomes such as psychological distress, social isolation, and lowered quality of life (e.g., Amano et al., 2021; Feng & Astell-Burt, 2017; Sharpley & Christie, 2007). In contrast, a qualitative study of people diagnosed with nonepileptic seizures identified positive emotional reactions in some participants who view the diagnosis as offering an explanation and hope for the future (Thompson et al., 2009). A smaller number of mostly qualitative studies exploring the impact of mental health diagnoses identified both positive and negative responses (Perkins et al., 2018). For example, Pitt et al. (2009) interviewed eight participants diagnosed with psychosis, identifying that although diagnosis has positive effects on service access and understanding the problem, the labeling also causes disempowerment and social exclusion. In their review of qualitative literature, Perkins et al. (2018) highlight that transparent and timely disclosure of diagnosis offers relief, validation of experiences, self-understanding, and empowerment for service users, despite clinicians’ fears that disclosure might expose service users to stigma or damage the therapeutic relationship. Provision of information was empowering and normalizing (Perkins et al., 2018), a valued task also highlighted in the diagnosis of autism in adults (Jones et al., 2014), although clinicians in Perkins et al. (2018) report a lack of time and resources to do this.
Autism Diagnosis in Adulthood
Autism spectrum disorder (ASD) is characterized in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) as persistent deficits in social communication and interaction and restricted, repetitive patterns of behavior, interests, or activities. The diagnostic criteria have expanded over past decades to include people with less noticeable autistic traits (Whitehouse et al., 2017). The changing criteria, coupled with increasing awareness of autism, particularly in females (Jensen et al., 2014), have led to a “lost generation” (Lai & Baron-Cohen, 2015) whose autism is only identified in adulthood. An increasing number of both quantitative and qualitative studies have provided a deep understanding of the experience of receiving an autism diagnosis in adulthood. Adults report awareness of both specific difficulties and a general sense of being different before diagnosis but do not always have enough knowledge to recognize autism as a possibility (Huang et al., 2020; Jones et al., 2014; Lewis, 2016). Although the DSM-(5th ed.; DSM-V; APA, 2013) definition of autism focuses on deficits, autistic adults report varied but mostly positive emotional reactions to diagnosis as they re-interpreted their past experiences through the lens of autism (Huang et al., 2020; Lewis, 2016; Powell & Acker, 2016). In some studies, the diagnosis gives autistic adults a new sense of belonging as it allows them to connect with other autistic people and identify as part of a wider autistic community (Huang et al., 2020; Tan, 2018). Some autistic adults express that autism is a positive part of their identity that comes with unique strengths (Lewis, 2016; Tan, 2018). These views are aligned with the neurodiversity movement, which asserts that neurodevelopmental conditions including autism are natural human variations that should be accepted and supported rather than minimized or cured (den Houting, 2019; Kapp et al., 2013). Despite their opposition to deficit-based conceptualizations of autism, neurodiversity proponents recognize the necessity of autism as a medical diagnosis as it enables access to support services (Kapp, 2020).
Measuring the Psychological Impact of Diagnosis
A number of quantitative studies focused on physical health diagnoses used the Impact of Events Scale (Horowitz et al., 1979; Zilberg et al., 1982) or its revised version (IES; Weiss & Marmar, 1997) to assess impact of diagnosis (e.g., Asif et al., 2016; Bleiker et al., 2000; Einsle et al., 2012; Mcbride et al., 2000). The IES was developed to assess the impact of stressful events or trauma, with the revised version assessing frequency of negative experiences in Intrusion, Avoidance, and Hyperarousal domains. Einsle et al. (2012) reports a high prevalence (range 4.8%–29.2%) of post-traumatic stress disorder (PTSD) following cardiac or cancer related diagnosis, highlighting the emotional impact of diagnosis. Feng and Astell-Burt (2017) assess the impact of diabetes diagnosis longitudinally using measures of distress, quality of life and social support. Although they found reduced quality of life, mental health and social contacts, evidence for psychological distress was not particularly strong. Interestingly, Feng and Astell-Burt (2017) argue the need to examine potential positive aspects of receiving a diagnosis using tools such as the Warwick-Edinburgh Mental Well-being Scale.
Of direct relevance, Casey et al. (2012) used the IES-R to identify post-traumatic stress symptoms in parents of children diagnosed with autism, framing autism diagnosis as a potentially traumatic event. Using the IES in the context of autism is problematic as it only measures negative experiences related to diagnosis and does not consider possible positive outcomes such as improved access to supports, a revised self-identity or revised life goals. Further critique of the IES suggested scores are biased by factors other than stress, including mental accessibility and recall of events, with Lees-Haley et al. (2001) demonstrating IES scores within the PTSD range for students reporting on the worst movie they had seen recently. Together, these findings point to the necessity of developing specialized tools that assess both the positive and the negative impacts of diagnosis.
The Impact of Diagnosis Scale and Preliminary Revision
As part of the Australian Longitudinal Study of Autism in Adulthood (ALSAA; Arnold et al., 2019), we sought to explore the positive and negative impacts of receiving an autism diagnosis from autistic adults’ perspectives. To our knowledge, the recently developed Impact of Diagnosis Scale (IODS; Courtney & Makinen, 2016) was the only tool closely related to this construct. The IODS was originally developed to explore the impact of diagnosis of borderline personality disorder (BPD). The original publication included preliminary data of adolescents diagnosed with BPD and some suggestions for future development. There are some similarities between the experiences of receiving BPD or autism diagnoses that led us to consider this tool, including diagnostic complexity, effects on self-understanding, and exposure to stigma (Lester et al., 2020). With permission of the original authors, we developed a preliminary revision of the IODS for use in autism research with a particular focus on use of non-pathologising language, as described elsewhere (IODS-PR; Arnold et al., 2020). Our preliminary revision resulted in a 12-item tool across three domains of Service Access, Being Understood, and Self-Acceptance and Understanding. Results showed a generally positive impact of diagnosis on the Self-Acceptance and Understanding domain, with neutral impact in the other two domains. This successful piloting within the ALSAA data collection, together with interest from our participants and our autistic and carer research advisory group, led our team to consider developing an expanded tool to capture the experience of receiving a diagnosis more broadly. In particular, in addition to a more detailed understanding of psychological impact, having separate domains to identify the impact of clinician practices would be of benefit to the evaluation of clinical services, and domains to identify the impact on service access of benefit to the evaluation of the broader service systems. Hence, we were interested if individual domains or combinations of domains could be constructed suited to these purposes.
The Current Study
This article describes the inclusive research processes used to develop the IODS-R and reports findings in relation to the diagnosis of autism in adulthood. Quantitative measurement can allow for the future investigation of protective and risk factors associated with psychological adjustment to diagnosis in adulthood. We aimed to develop a tool that measures the experiential, psychological, and practical impact of receiving an autism diagnosis in a way that closely aligns with autistic adults’ experiences. In terms of concurrent validity, we hypothesized that the IODS-R, and in particular, the mental well-being domain would show a positive moderate relationship with an existing measure of well-being, with other domains showing a weaker or nonsignificant relationship.
Method
Participants
The ALSAA (Arnold et al., 2019) is a questionnaire-based, prospective, longitudinal cohort study of Australian autistic adults (25+ years) and a non-autistic comparison group, with ethics approval from the the UNSW Sydney Human Research Ethics Committee, approval number HC15001. Participants were recruited through advertisement and contact with autism, disability or education-related organizations, peak bodies, and clinicians. Snowball sampling was also employed in the Time 2 data gathering. The IODS-R was included during the latter part of Time 2 data collection. Participants completed online or hardcopy surveys with a large battery of measures including the IODS-R expanded item pool. To improve the accuracy of self-reported autism diagnosis, the survey asked autistic participants to provide details of diagnosing clinicians and complete the Autism-spectrum Quotient-Short (AQ-Short; Hoekstra et al., 2011). Only participants who reported a formal diagnosis of autism and agreed to at least one screening item (see Instruments) were included in this analysis. Full details of the ALSAA sample and procedures are described elsewhere (Arnold et al., 2019).
Following encouraging results from the IODS-PR, the item pool used to develop the IODS-R was expanded part-way through the data gathering of the ALSAA at Time 2. Hence, the total number of formally diagnosed autistic participants available for this study who had completed the expanded item pool was limited to N = 125 (28 males, 89 females, 8 non-binary/other; Mage = 40.98 years, SD = 11.39, range 25–80 years). Participants had all been formally diagnosed as autistic, and 95.12% (n = 117) scored above the screening cut-off of 65 (M = 88.45, SD = 10.67, n = 2 missing) on the AQ-Short (Hoekstra et al., 2011), which has a sensitivity of .97. The average age of receiving an autism diagnosis was 37.43 years (SD = 12.02, range 9–79, n = 1 missing) and average years since being diagnosed was 3.94 years (SD = 5.29, range 0–28, n = 1 missing). Co-occurring mental health conditions were common (e.g., depression n = 52, 43%; anxiety n = 70, 58%). Just more than half of the participants were employed (n = 70, 56%, n = 6 missing) and about a quarter were studying (n = 34, 27%, n = 6 missing). Most participants reported having higher education (certificate/diploma n = 30, 24%; undergraduate degree n = 45, 36%; postgraduate degree/PhD n = 29, 23%). Roughly half were married or in de facto relationships (single n = 61, 49%; married/de facto n = 58; 46%; other n = 5, 4%; n = 1 missing).
Instruments
IODS-R was further developed from the IODS-PR (Arnold et al., 2020) with significant collaboration with the ALSAA Research Advisory Network (RAN) of autistic and carer advisors. The process used to develop the IODS-R is outlined throughout this manuscript. The final tool (see Supplementary material) consists of 22 items, containing two screening item and four domains: Mental Well-being (MWB), Clinician Support (CS), Self-understanding (SU) and Service Access (SA). The two screening items pertain to participants’ memories of being diagnosed and living with the diagnosis. Each item is scored on a 7-point Likert-type scale (Strongly Disagree—Strongly Agree), with a Not Applicable (NA) option. Two items (10 and 11) are reverse scored. Higher scores indicate a more positive impact of diagnosis.
The Autism-spectrum Quotient-Short (AQ-Short) (Hoekstra et al., 2011) is a self-report measure of autistic traits in adolescents and adults adapted from the 50-item Autism-spectrum Quotient (Baron-Cohen et al., 2001). It was used here to describe our sample and to support self-reported autism diagnosis. It contains 28 Likert-type scale items rated from 1 (definitely agree) to 4 (definitely disagree) across five domains of Social skills, Routine, Switching, Imagination, and Numbers and patterns. Higher total scores indicate greater autistic traits, with a recommended cut-off of >65 for screening purposes. The AQ-28 showed a sensitivity of .97 and specificity of .82 for distinguishing autistic people from a general population sample (Hoekstra et al., 2011). It showed a coefficient α of .83 in our sample, within the range (α between .77 and .86) found by Hoekstra et al. (2011).
The Warwick-Edinburgh Mental Well-being Scale (WEMWBS; Tennant et al., 2007) is a self-report measure of positive well-being, used in this study as a measure of concurrent validity of the IODS-R subscales. The WEMWBS contains 14 items scored on 5-point Likert-type scales ranging from 1 (none of the time) to 5 (all of the time). It has shown concurrent validity with several other measures of well-being, and strong coefficient α (.89–.91) and test–retest reliability (.83). It showed a coefficient α = .93 in our sample.
Procedure and Data Analysis
Based on findings from the IODS-PR, and in unison with conducting a systematic scoping review of the literature (Huang et al., 2020), the authors (SRCA, YH, YIH, JH) collaborated with the RAN advisors (n = 7) to propose six ideal domain targets for the final revision on the tool: Service access (ability to receive appropriate health and community services), Well-being (a positive feeling of wellness), Self-acceptance, and understanding, Diagnostic process, Relating with others, and Accuracy of diagnosis. The RAN advisors requested for some domains to have descriptors for added clarity. Potential new items based on these domains were iteratively brainstormed and prioritized. The resultant expanded item set consisted of 48 items including two screening items. All 12 IODS-PR items remained in the expanded item set.
Stata 15 was used for all analyses. We first conducted exploratory factor analysis using the principal factors method with promax rotation on the 46 scored items to determine factor structure and items to retain. For this analysis, items indicating more negative reactions to diagnosis were reverse scored and NA responses were converted to a neutral score of 4 to maximize the small sample size as opposed to assigning them to missing data, taking a conservative approach to reducing overall variance as opposed to missing imputation, and as NA would have similar impact as a neutral response to the calculation of average domain scores. Item 15 (“. . . has improved my relationships with my work colleagues, supervisor and employer”) and Item 16 (“. . . has improved my relationships with my fellow students and teachers/lecturers”) were combined into a single item due to similarity and large number of NA responses. Across the entire item pool, although excluding Items 15 and 16, the majority (82%) of participants had 2 or fewer NA responses. Multiple criteria were considered in factor retention decisions (Izquierdo et al., 2014), including visual inspection of eigenvalues, review of the scree plot, parallel analysis with 1,000 repetitions using 95th percentile eigenvalues, Veli’er’s minimum average partial, and clinical judgment of resulting structure, with four, five, and six-factor solutions tested to identify the best-fitting structure for potential domains.
After determining the ideal number of factors to retain, the steps below were used to reduce the total number of items, repeating the factor analysis to update loadings and confirm factor structure after each removal:
Items were deleted if loadings on all factors were <.3.
Items with close cross-loadings (<.2 difference between two highest-loaded factors) were removed to ensure the distinctiveness of subdomains.
Items with weakest loadings and/or closest cross-loadings were removed from factors with the highest number of items, considering thematic relevance, until all factors had a similar number of items.
Descriptive statistics and correlation analysis were conducted on the resultant scale and scale domains. Concurrent validity was tested using a correlation of total and domain scores against other measures gathered in both the total sample and a sample restricted to those who had received their diagnosis within the last 2 years, as the impact of diagnosis is likely to change to some extent over time.
This study was not preregistered. Data and study materials access requires approval, please contact the corresponding author.
Inclusive Research Process
The ALSAA study from which these data were drawn had an established group of autistic and carer research advisors and followed an Inclusive Research Protocol as described by Arnold et al. (2019). We used a mixture of detailed consultation and peer research in developing the IODS-R. The autistic and carer research advisors consulted included a mixture of those diagnosed in childhood and adulthood. Some advisors were alumni of the Autism CRC Autistic Researcher Academy program (now known as the Sylvia Rodgers Academy; Rodger et al., 2016). This program aimed to upskill autistic adults with an interest in research to work as co-producers of research and as peer researchers.
The ALSAA research advisors were invited to engage in an intensive process of iterative rounds of consultation to brainstorm target domains and potential items. A lay summary was developed to facilitate this process and revised over iterative rounds based on feedback received. The lay summary included an introduction and background, a list of target domains and potential items, and instructions for providing feedback. Feedback was received via email, video conferencing and pre-recorded video responses. Feedback highlighted the potential for some items to be misinterpreted by some autistic respondents, which were revised using more precise language. For example, the draft item “. . . gives me hope for the future” was changed to “. . . gives me more hope for my future life and happiness.” Advisors also requested expanded descriptions be provided for some hypothesized domain descriptors, for example, “Well-being, a positive sense of wellness.”
Peer research involves academic researchers working directly with people with lived experience of the topic area as co-researchers. Ideally, co-researchers should be involved in all stages of the research, from applying for funding, designing the study, recruitment, data gathering, analyzing, and interpreting data as well as developing and promoting outputs (den Houting et al., 2021). Peer research requires a more intensive level of community stakeholder involvement than consultation, with greater power-sharing, community engagement, and the overarching aim of doing research with rather than on the population group (den Houting et al., 2021). Autistic peer researcher JH, who was also an ALSAA research advisor, was involved in analysis of the qualitative data during the preliminary revision of the tool, helping to inform the development of the expanded domains and item set. JH reviewed both the preliminary and final versions of the tool including naming of domains, as well as co-authoring this manuscript.
Results
For the 125 available participants and excluding screening items, the Kaiser–Meyer–Olkin (KMO) test (KMO = 0.77) and Bartlett’s test of sphericity, χ2(1,081) = 3,497.63, p < .001, indicated that the data were acceptable for factor analysis. Although the expanded item set was developed based on six hypothesized domains, exploratory factor analysis, and scale reduction showed a 4-factor model to be the best solution. The resultant IODS-R thus consisted of four domains each containing five items (see Table 1), plus two screening items (22 items in total). The first factor Self-Understanding (SU) refers to the extent to which the diagnosis enhanced the person’s view of their characteristics and experiences. The second factor Mental Well-being (MWB) consists of items related to emotions and self-esteem after diagnosis. The third factor Clinician Support (CS) contains items measuring the perceptions of the diagnosing clinician. The fourth factor Service Access (SA) refers to the availability of relevant support services after diagnosis.
Factor Loadings of Items 3 to 22 in the IODS-R.
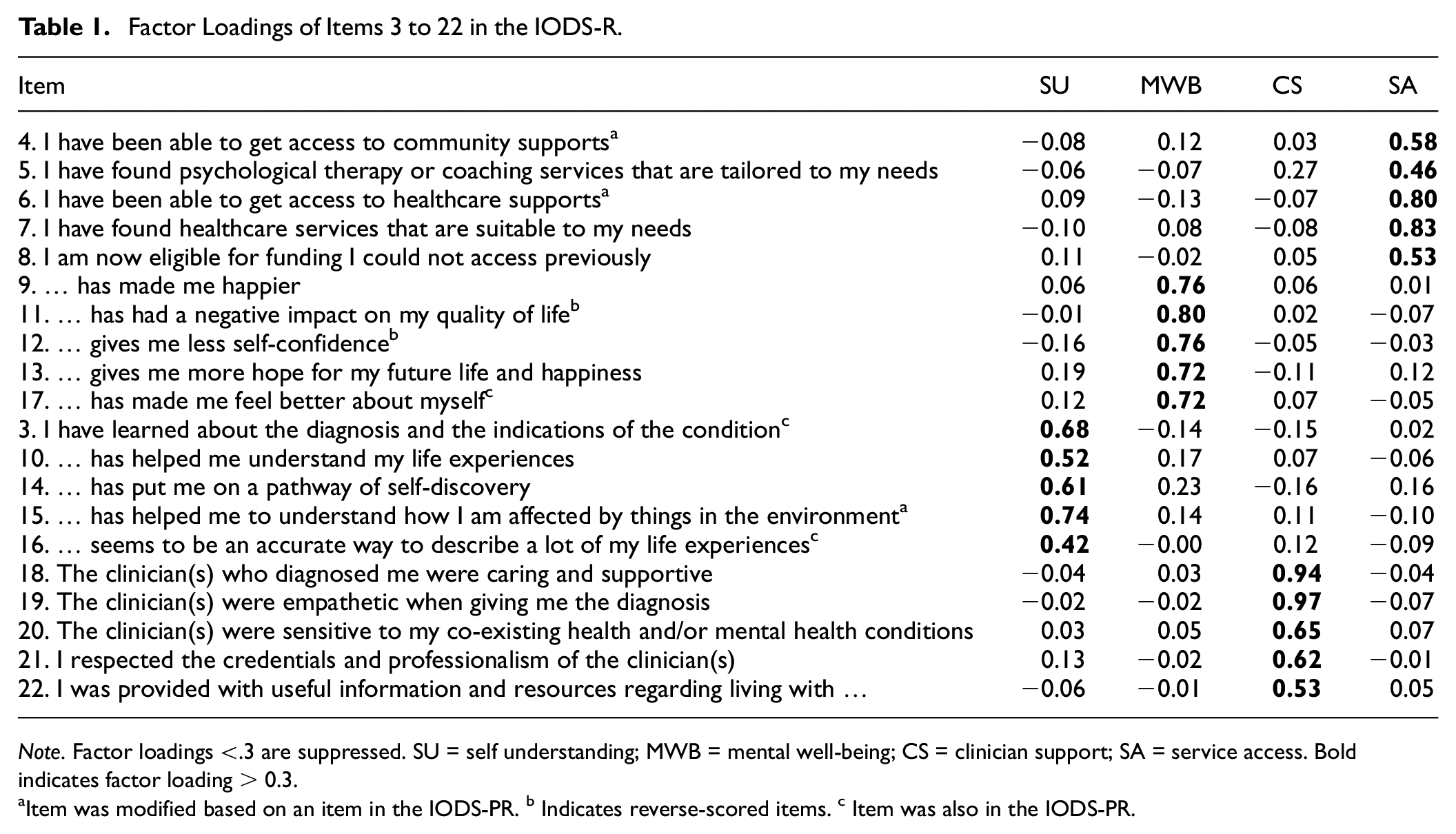
Note. Factor loadings <.3 are suppressed. SU = self understanding; MWB = mental well-being; CS = clinician support; SA = service access. Bold indicates factor loading > 0.3
Item was modified based on an item in the IODS-PR. b Indicates reverse-scored items. c Item was also in the IODS-PR.
To probe configurational invariance we also ran the EFA limited to females (see Supplementary Table 1), finding that most items again fell within the same factor, although one slightly cross-loaded (item 5) and one item was below .3 factor loading (item 16).
Domains and Coefficient α
The 20 scored items overall (α = .80) and four factors of SU (α = .73), MWB (α = .87), CS (α = .83), and SA (α = .74) all showed good coefficient α. Correlational analysis (see Table 2) showed SU was moderately positively correlated with MWB, SA was moderately correlated with CS and MWB was weakly correlated with CS.
Correlations Between IODS-R Subdomains.
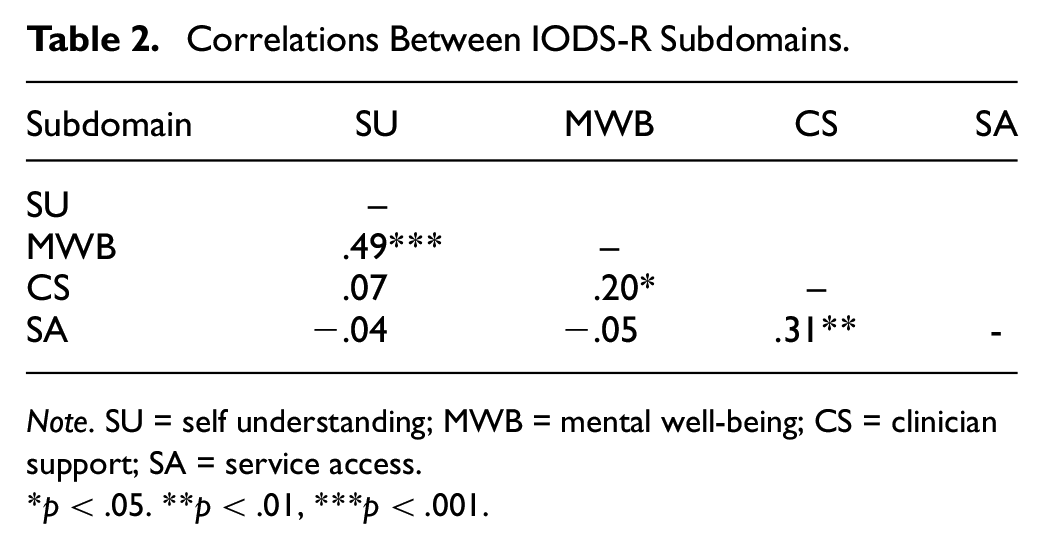
Note. SU = self understanding; MWB = mental well-being; CS = clinician support; SA = service access.
p < .05. **p < .01, ***p < .001.
Domain scores were calculated from item means. Participants were removed from domain score or total score analysis if more than two items in a domain were missing. SA, due to the nature of the items, was the only domain significantly affected, with observations reducing to n = 101, and CS losing only one observation. Participants’ average domain scores were generally positive for SU (M = 6.37, SD = 0.75), MWB (M = 5.28, SD = 1.41), and CS (M = 5.79, SD = 1.18) but more neutral for SA (M = 3.09, SD = 1.49) (see Table 3). Rerunning the analysis with the sample restricted to those who were diagnosed within the last two years, all mean scores were largely unchanged remaining within 0.2 points difference for all domains.
Domains and Combined Scores Summary.
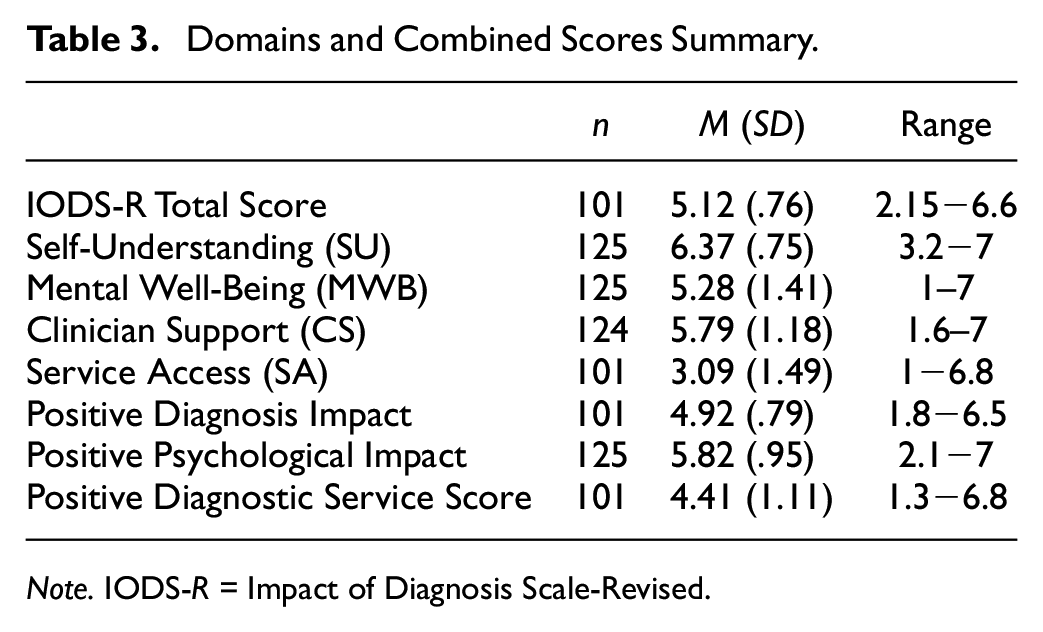
Note. IODS-R = Impact of Diagnosis Scale-Revised.
Given potential practical applications, we also tested potential combinations of domain scores. The Positive Diagnosis Impact (MWB + SU + SA) score had a good coefficient α (.71) as did the Positive Psychological Impact (MWB + SU) combined score (α = .85) and the Positive Diagnostic Service Score (CS + SA) combined score (α = .79).
Correlations With WEMWBS
Limiting the sample to those who received a diagnosis within the last 2 years, expected correlations were found between IODS-R scores and the WEBWBS total score (see Table 4). There was a strong correlation between the MWB domain and the WEMWBS, with significant moderate relationships with SU and the IODS-R total score. In the full sample, the MWB and total score relationships remained, although SU become non-significant and CS showed a weak significant relationship with the WEMWBS.
Correlation of Subdomains With the WEMWBS.
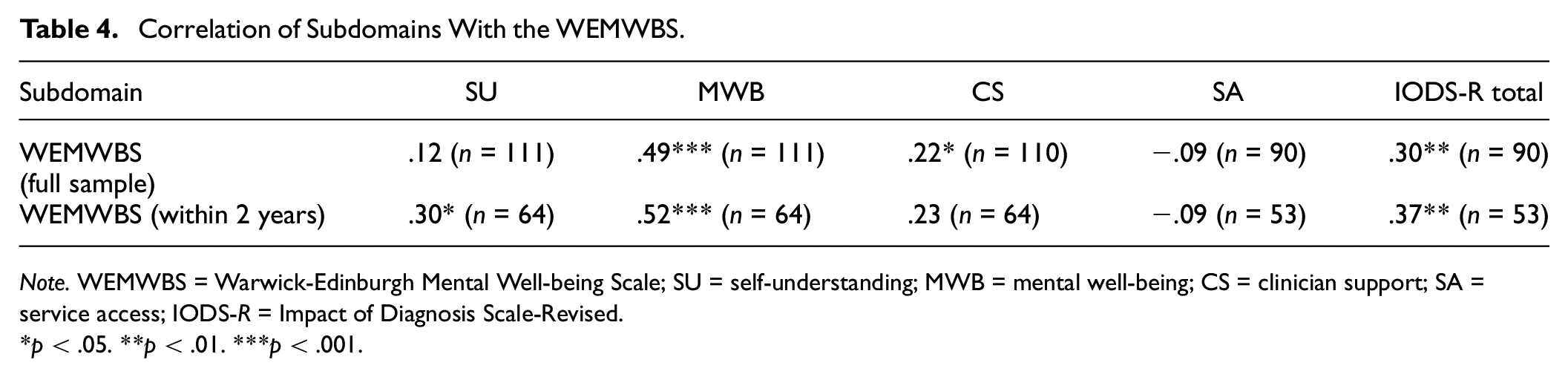
Note. WEMWBS = Warwick-Edinburgh Mental Well-being Scale; SU = self-understanding; MWB = mental well-being; CS = clinician support; SA = service access; IODS-R = Impact of Diagnosis Scale-Revised.
p < .05. **p < .01. ***p < .001.
Discussion
Using inclusive research approaches, EFA and scale reduction, we developed a further revision of the IODS-PR for application with autistic adults, termed the IODS-R. The tool has been significantly modified from the original version of IODS (Courtney & Makinen, 2016) and the preliminary revision (Arnold et al., 2020), with the new design potentially allowing for diagnoses other than autism to also be examined. Compared to the original version of the tool, our revision showed good coefficient α overall and in single and combined domain scores. Although further validation is needed, our data demonstrated good convergent validity for the MWB domain and the WEMWBS, and moderate associations between the WEMWBS and the SU domain and total scores when the sample was limited to those more recently diagnosed. Further validation is needed to support the use of total and/or composite domain scores, although individual domain scores are likely to be of utility in clinical practice. Particularly, an exploratory bifactor analysis in a substantially larger sample is needed (Bader et al., 2022) to support the validity of total or combined domain scores. If validity can be established, the content of combined domain scores may be of particular application for service and system evaluation purposes. Autistic adults in this sample reported a generally positive psychological impact of autism diagnosis in terms of mental well-being and self-understanding, and generally positive experiences with diagnosticians, though service access following diagnosis was less satisfactory. These quantitative findings aligned with past qualitative research on responses to diagnosis of autism in adulthood (Lewis, 2016; Powell & Acker, 2016; Punshon et al., 2009; Tan, 2018), providing further support for this new tool. The provision of diagnosis is a frequent and fundamental activity of many health professionals. The IODS-R is the first measure of its kind and shows promise for the evaluation of diagnostic services, clinician practices, and the client experience of diagnosis for other diagnoses as well as autism.
Receiving a diagnosis of autism in adulthood has been described as “an emotional roller coaster” (Lewis, 2016, p. 436). Despite potential negative consequences of stigma and misunderstanding, existing research found receiving an autism diagnosis to be positive for most autistic adults, providing relief and clarification for a lifetime of differences and often difficulties (Huang et al., 2020; Jones et al., 2014). Our quantitative findings, where most participants reported increased well-being and self-understanding, are in alignment with past qualitative research, which suggests the content validity of the IODS-R. Based on these findings, we encourage diagnosticians to change “the story” (Brown et al., 2021, p. 1171) of autism by reframing deficit narratives. Instead, clinicians should highlight strengths and challenges from a neurodiversity perspective when disclosing the diagnosis (den Houting, 2019; Kapp et al., 2013). Previous studies have mentioned the “service cliff” (Laxman et al., 2019), referring to a lack of services available for autistic individuals once they reach adulthood, as well as a paucity of services available for newly diagnosed autistic adults (Evans et al., 2022; Huang et al., 2020). This literature aligns with the results from the SA domain and indicates the need for policy, funding, and service development for this significant population group.
There is little literature on autistic adults’ experiences and rapport with their diagnostic clinician or diagnostic team (Evans et al., 2022; Jones et al., 2014). Evans et al. (2022) reported on late diagnosed autistic adults in New Zealand, where two-thirds of participants expressed satisfaction with the diagnostic assessment stage. Of interest, Jones et al. (2014) surveyed 128 autistic adults in the United Kingdom and found 71.1% of participants to be quite or very satisfied with the “manner of disclosing professional” (p. 3039). Satisfaction with the manner of the professional did not make an independent contribution to overall satisfaction with the diagnostic process, though they argued the finding was due to collinearity with satisfaction with the quality of information received at diagnosis. Overall, this emphasizes the importance of information provision at the point of disclosure. Despite poor service access, our results from the CS domain suggest that most Australian autistic adults in our sample had positive experiences of support from their diagnosing clinicians. The CS domain will be of use in future work to determine the impact of clinicians on overall response to diagnosis, and to identify best practice in disclosure of diagnosis to clients.
Good practice in scale development highlights the importance of a strong conceptualization of the construct to be measured (Clark & Watson, 2019). A strength of our scale development was the conduct of a systematic scoping literature review, alongside the use of inclusive research practices including an advisory group and an autistic peer researcher, which helped to ensure the item pool development was grounded in lived experience. Inclusive or participatory research practice can improve the quality and relevance of studies (den Houting et al., 2021; Forsythe et al., 2019) although difficulties can emerge regarding power dynamics and management of relationships, greater financial costs and need for extended project timelines (den Houting et al., 2021). Using inclusive processes in this study greatly enhanced the quality and accessibility of the tool developed, highlighting that draft items may not have been accessible or could have been misinterpreted by respondents.
There is a dearth of quantitative research on clients’ responses to diagnosis, with no other tool focused on the measurement of the impact of diagnosis. This presents some problems in terms of establishing concurrent validity in comparison to a gold standard. We were able to partially demonstrate expected convergent (total score, MWB and SU domains) and divergent (SA and CS domains) validity of the IODS-R with reference to the WEMWBS when the sample was limited to those more recently diagnosed, although in the full sample, the CS domain showed a significant weak correlation with WEMWBS and the SU correlation became nonsignificant. Nevertheless, this still suggests overall that impact of diagnosis is related to mental well-being, with some separation of the SU, CS, and SA domains from the MWB domain of the IODS-R. As the ALSAA study involved a limited set of instruments, more research is needed to establish convergent validity of other domains and total score using a broader range of measures. Here, we suggest several measures that may be of interest to future researchers. The Self-Reflection and Insight Scale (Grant et al., 2002) might be a useful measure to compare with SU. Validation of the SU domain is especially important as existing research has highlighted relief and self-understanding as common consequences of adulthood autism diagnosis. The SA domain appears more difficult to identify a potential convergent measure. Although the ALSAA study gathered data using the Barriers to Health Care Checklist (Arnold, Bruce, et al., 2023; Raymaker et al., 2016), this is a different construct to fulfillment of specific post-diagnosis support needs. To validate the CS domain, tools focused on clinician-patient communication (Street & Mazor, 2017) might be appropriate. Future research in larger samples should also explore relationships between participant characteristics, particularly cognitive ability, indicators of social capital and income, and IODS-R domain scores.
Although findings to date are promising, more work is needed to establish the validity and reliability of the IODS-R, including practical utility. Test–retest reliability may be subject to the time frame between measurements. We would hypothesize there may be a response curve following diagnosis, as people may adapt to this new self-knowledge and return to a homeostasis of subjective well-being over time (Cummins et al., 2002). Future research could also use the IODS-R to explore differences in diagnostic experiences based on life stage when the diagnosis was received. Service availability is likely to vary over time and jurisdiction. In addition to potential utility identifying determinants of positive adaptation to diagnosis, the IODS-R may also have practical utility when applied to service evaluation. Although our revision was focused on autism, future researchers may seek to adapt and validate this tool for use across different diagnostic groups. Application to other diagnostic groups should also employ a cautious inclusive research approach to ensure that aspects specific to the lived experience of the target condition are included.
Limitations
Our sample may have limited generalizability given the female majority, as typical estimates of autism prevalence suggest a 1:3 or 1:4 female to male ratio (Loomes et al., 2017). Although a small sample, re-running the EFA limited to females reproduced a similar although not identical factor loading pattern. Ideally, larger samples could be used to test factors and measurement invariance. Females are known to have higher rates of self-selection into online research (Guo et al., 2017), with numerous recent online autism studies having now recruited female majority samples (e.g., Arnold et al., 2019; Arnold, Higgins, et al., 2023; Gilmour et al., 2012; Howard & Sedgewick, 2021; Nicolaidis et al., 2013; Scheeren et al., 2022). Female gender has also been associated with an increased age of autism diagnosis (Huang et al., 2021) with a trend toward decreased gender ratios in older cohorts (Idring et al., 2015; May & Williams, 2018; Rutherford et al., 2016). Although we did not have data on IQ, the majority of our sample were autistic adults who had higher education qualifications, with half employed and half in relationships, highlighting the importance of investigating the impact of autism diagnosis in autistic adults with intellectual disability or higher levels of support needs. Given resource constraints and the geographic spread of Australia, we were unable to verify self-reported formal diagnosis of autism, although potential participants who indicated poor memory of diagnosis were excluded based on screening items in the IODS-R. Furthermore, participants were required to provide detailed info about their diagnosis and complete the extensive ALSAA survey (1–3 hr) with no pay, which minimized incentives to give false responses. To obtain the maximum sample size for scale development, the sample was not restricted to those recently diagnosed except for the convergent validity analysis. Also, to maximize sample size in the EFA, we assumed that in most circumstances, a NA response has a similar meaning to a neutral response. Thus, NA was treated as a neutral response in our EFA. Although still a small sample for factor analysis, Bartlett’s test and the KMO suggested the sample was adequate for EFA. Given the limited sample size, we also included 7 participants who received their diagnosis more than 15 years ago, although they did pass the two screening questions checking for memory of the diagnostic event.
As data collection occurred within the context of a larger longitudinal study, the total item pool size was limited to manage the respondent burden. Although an extensive item pool is ideal in scale development (Clark & Watson, 2019), our limitation was partly offset by having autistic research advisors prioritize the potential items prior to data gathering.
Although we demonstrated good convergent validity of the MWB domain with the WEMWBS, further validation of the IODS-R is required. Limited sample size precluded the use of a twofold validation approach, with further replications of the proposed four-factor model needed. Particularly, bifactor analysis in a larger sample (Bader et al., 2022) could determine if the proposed combinations of domains and the use of a total score have validity. As discussed, identifying measures to determine convergent validity will be difficult given the lack of scales developed that focus on the domains associated with impact of diagnosis. Although clinical judgment was also used in determining factors and items, it is possible that using a quantitative approach to scale reduction could have artificially narrowed some domains or that some redundant items still remain. Application and testing with population groups other than autistic adults is also required.
Conclusion
The IODS-R is the first tool co-produced with autistic adults to measure the impact of receiving an autism diagnosis, with the potential to be used with other diagnostic groups. With further validation, it can support research determining factors that influence positive adjustment to the receipt of a life-changing diagnosis. Despite a dearth of diagnostic and support services available to autistic adults, adults who do receive an autism diagnosis found it beneficial in terms of deepened self-understanding and improved well-being. Policies and practices that lead to improved service provision are needed to increase the quality and availability of supports post-diagnosis. Parties interested in using the IODS-R are requested to contact the author so a database of usage can be maintained to support further development of the tool, and to avoid usage of the preliminary revision version that, although slightly shorter (12 vs. 22 items), did not have the same level of co-production or refinement in its development.
Supplemental Material
sj-docx-1-asm-10.1177_10731911231196486 – Supplemental material for Development of the Impact of Diagnosis Scale–Revised (IODS-R)
Supplemental material, sj-docx-1-asm-10.1177_10731911231196486 for Development of the Impact of Diagnosis Scale–Revised (IODS-R) by Samuel R. C. Arnold, Yunhe Huang, Lauren P. Lawson, Julianne M. Higgins, Ye In (Jane) Hwang, Amanda Richdale and Julian N. Trollor in Assessment
Supplemental Material
sj-docx-2-asm-10.1177_10731911231196486 – Supplemental material for Development of the Impact of Diagnosis Scale–Revised (IODS-R)
Supplemental material, sj-docx-2-asm-10.1177_10731911231196486 for Development of the Impact of Diagnosis Scale–Revised (IODS-R) by Samuel R. C. Arnold, Yunhe Huang, Lauren P. Lawson, Julianne M. Higgins, Ye In (Jane) Hwang, Amanda Richdale and Julian N. Trollor in Assessment
Footnotes
Acknowledgements
The authors acknowledge the valuable contribution of the ALSAA Research Advisory Network members Dr Matthew Bennet, Jen Harland, Julianne Higgins, Michael Knight, Gabriel Nakhel, Joanne Mahony, Cheryl Strangio, and Chris Tanner whose insight and recommendations shaped the IODS-R. We also gratefully acknowledge the cooperation and participation of all participants on the autism spectrum involved in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge the financial support of the Cooperative Research Center for Living with Autism (Autism CRC), established and supported under the Australian Government’s Cooperative Research Centers Program. JT is supported by an NHMRC Leadership Fellowship GNT2009771
Data Availability Statement
This study was not preregistered. Data and study materials access requires approval, please contact the corresponding author.
Supplemental Material
Supplemental material for this article is available online.