
Abstract
The assessment of oppositional defiant disorder, conduct disorder, antisocial personality disorder, and intermittent explosive disorder—the Disruptive, Impulse Control and Conduct Disorders—can be affected by biases in clinical judgment, including overestimating concerns about distinguishing symptoms from normative behavior and stigma associated with diagnosing antisocial behavior. Recent nosological changes call for special attention during assessment to symptom dimensions of limited prosocial emotions and chronic irritability. The present review summarizes best practices for evidence-based assessment of these disorders and discusses tools to identify their symptoms. Despite the focus on disruptive behavior disorders, their high degree of overlap with disruptive mood dysregulation disorder can complicate assessment. Thus, the latter disorder is also included for discussion here. Good practice in the assessment of disruptive behavior disorders involves using several means of information gathering (e.g., clinical interview, standardized rating scales or checklists), ideally via multiple informants (e.g., parent-, teacher-, and self-report). A commitment to providing a full and accurate diagnostic assessment, with careful and attentive reference to diagnostic guidelines, will mitigate concerns regarding biases.
This article summarizes evidence for assessing and diagnosing Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association [APA], 2013) oppositional defiant disorder (ODD), conduct disorder (CD), antisocial personality disorder (APD), intermittent explosive disorder (IED)—collectively referred to as disruptive behavior disorders (DBDs). In addition, because of their relevance for the assessment of DBDs, disruptive mood dysregulation disorder (DMDD) and key dimensions of ODD and CD will be discussed.
In general, DBDs are distinguished from other disorders in the DSM by the centrality of behaviors harmful to others among their core symptoms. There are important distinctions among DBDs, as well as overlapping features that can raise challenges in distinguishing between them. In terms of diagnostic requirements, ODD reflects chronic oppositional behavior and hostile and irritable interpersonal interactions and does not necessarily include aggressive behaviors. The criteria for CD do include aggressive behaviors, as well as property damage, theft, status offenses, and deficiencies in prosocial emotions. Similar to CD, APD is characterized by a persistent disregard for others and for societal norms, but also can include impulsivity, irresponsibility, and frequent physical fights. IED is characterized by intense, reactively aggressive outbursts and by the absence of other DBD symptoms. Finally, DMDD overlaps substantially with ODD in reflecting chronic irritability and outbursts of temper. Each disorder will be described in more detail below.
Valuable prior reviews on the assessment of behavioral disorders have taken a broad focus, including the assessment of common risk factors and co-occurring conditions (e.g., Walker et al., 2020), or a narrower focus, as in the systematic review of screening measures (Lavigne et al., 2016). In the present review, we take a relatively circumscribed focus on evidence guiding the diagnostic assessment of these disorders. There are intriguing approaches to gathering information related to these disorders (e.g., ecological momentary assessment, neuroimaging), although we have not included them here because their diagnostic utility has not been established. Several general, cross-cutting, assessment considerations should be addressed prior to discussing specific DBDs.
Factors Affecting Clinical Judgment in the Assessment of DBDs
Typically, assessment and diagnosis relies on clinician judgment, which may be biased in general practice for a number of reasons (see e.g., Jensen-Doss & Hawley, 2011; Lilienfeld et al., 2014). Some biases are especially prominent for DBDs and may reduce the validity of general clinical judgment in assessment and diagnosis.
Stigma
A concern that is often raised regarding ODD and CD is a belief that assigning a diagnosis will be stigmatizing (e.g., Beltrán et al., 2021; Grimmett et al., 2016), and it is possible to imagine a number of ways in which stigmatizing effects of learning a child’s diagnosis could plausibly occur. However, we have not found any studies showing that in actuality a diagnosis of ODD or CD leads to harm. More fundamentally, this concern could apply to any mental health diagnosis. For example, a meta-analysis of stigma associated with diagnostic labels in academic settings found no significant stigmatizing effects for behavioral disorders alone but did find effects for a combination of behavioral and emotional disorders (Franz et al., 2023). Despite any empirical evidence, assertions about stigma specific to ODD and CD contribute to an overall jaundiced and unfounded bias on the part of clinicians (e.g., Burke et al., 2022) that hinders sound assessment and diagnostic practice.
Empirical evidence is sorely needed to help enhance good clinical practices. Sound studies on stigma would operationalize multiple types of potential stigmatization and would measure the real-world effects following the introduction of a diagnostic label. One concern evident in the existing research (e.g., Franz et al., 2023) is that some studies have characterized stigma to include a participant’s prediction of poor future academic functioning upon learning a diagnosis. In reality, such predictions would accurately reflect the empirical evidence that ODD and CD do predict increased risk for dropping out of school, higher rates of conflict with and rejection from school peers, and other types of impaired academic performance (e.g., Burke et al., in press). Sound research on stigma will need to disentangle the negative effects of the manifest behaviors associated with these conditions from the receipt of a diagnostic label.
This research will ideally characterize how much stigma is created by the diagnostic label. Characterizing the magnitude of the stigmatization is necessary to estimate the cost–benefit ratio, as there are demonstrable benefits to receiving a diagnosis, such as selecting evidence-based treatments, making prognoses, and facilitating formal academic support plans. Receiving a diagnosis of ODD or CD can bring relief to parents (e.g., Johnston et al., 2020), and parents retain privilege in regard to the disclosure of protected health records, including diagnoses. While responses to vignettes provide some information, research on stigma should estimate the real-world costs and benefits of assigning any diagnostic labels, including DBDs. At present, the evidence for clear benefits, along with the lack of evidence for stigmatization due to DBD diagnoses, should compel clinicians to follow appropriate clinical practices and give full and accurate diagnoses.
Trauma
There is a common belief that behavioral disorders are the product of trauma. This belief appears to impair clinical judgment regarding DBDs. In a recent study (Becker-Haimes et al., 2021), 132 clinicians were presented with a vignette of an 11-year-old boy showing symptoms of ODD from birth. Vignettes were experimentally manipulated to vary only in one way: the inclusion of a single potentially traumatic experience (PTE) in the past year. When no PTE was included, 68.0% of clinicians correctly identified ODD, and only 1.6% diagnosed poststraumatic stress disorder (PTSD). In contrast, when the PTE was included, 56.1% diagnosed PTSD and only 28.8% ODD. Rather than being biased by popular misbeliefs about trauma, clinicians should remember that traumatic stressors are risk factors for DBDs, and that DBDs and PTSD can co-occur. The most ethical, clinically appropriate, and likely helpful approach would be to provide a full and accurate diagnostic assessment that does not discount the possibility of DBDs.
Racial Bias in Diagnostic Practice
In practice, children and adolescents of color may be disproportionately misdiagnosed with DBDs (Ballentine, 2019; Fadus et al., 2020), often in cases where a different diagnosis would have been more appropriate, including attention-deficit/hyperactivity disorder (ADHD), autism (Mandell et al., 2007), or a mood disorder (Fadus et al., 2020). For example, white children in a residential facility were significantly less likely to be diagnosed with CD than African American children, despite equivalent or greater levels of aggression or delinquency (Cameron & Guterman, 2007). Effects of bias may be exacerbated when there is discordance between clinician and patient race, although further research is warranted (Van Ryn et al., 2011). Fadus et al. (2020) describe potential strategies to reduce the impact of unconscious racial bias in diagnostic practice, including education, training activities, and other interventions. Ultimately, sound training and mindful application of evidence-based assessment approaches should bolster the reliability and validity of DBD diagnoses. Further knowledge about the causes and consequences of such biases and interventions to reduce racial biases in diagnostic practice, should be a research priority.
Gender Bias in Diagnostic Practice
Prior research has found evidence of a male preponderance of DBDs (Leadbeater et al., 1999) especially with diagnoses of CD (Maughan et al., 2004). A study of youth in residential treatment found evidence that CD was diagnosed more in male than female adolescents, despite higher levels of aggressive symptoms (Cameron & Guterman, 2007). Clinicians must actively attend to the potential for unconscious beliefs about gender and DBDs and ensure adherence to diagnostic criteria (Garb, 1997) while making diagnoses. Improving algorithmic and statistical approaches may help to reduce the impact of gender bias on DBD assessment.
General Assessment Best Practices for DBDs
Any diagnostic assessment should be a multistep process. The current review takes a fairly narrow focus to highlight information specific to the DBDs, but these more general elements of assessment are no less important. First, the purpose of the assessment must be clear and should drive the assessment process. In a treatment context, the presenting problems that motivated service engagement typically define that purpose. The assessment process should then prioritize developing a diagnostic formulation in service of the case conceptualization and treatment planning. A good clinician will be mindful that diagnoses are often, but not always, central to this process, as not all problems are explained by mental health diagnoses and not all diagnoses that a person meets criteria for are pertinent to all presenting problems or associated treatment plans.
Additional important steps include screening out diagnoses and making differential diagnoses. It can be as useful to know if a diagnosis is not present. Likewise, most diagnoses include provisions that they should not be applied if the symptoms are better explained by other mental health disorders, medical conditions, or substance use. Other factors, such as sleep, stress, and other wellness behaviors should be considered as they can impact functioning even outside of the context of a psychological diagnosis. Good assessment practices involve collecting as much potentially relevant information as efficiently as possible.
Standards for Assessment
Despite potential biases, a mental health clinician is still in the best position to integrate all information to provide a sound diagnostic formulation, presuming they follow best practices. Unfortunately, in a worldwide survey of practicing clinicians, 49.8% reported routinely or often making a diagnosis without referring to diagnostic guidelines, and another 32.0% reported doing so only sometimes (First et al., 2018). Another worldwide survey suggests that psychologists in general value diagnoses for guiding clinical decisions and for conveying information to patients and colleagues (Evans et al., 2013). The disconnect between the merit of diagnoses and the infrequency at which diagnostic criteria are referenced should ring alarm bells for clinicians and researchers alike. Clinical values are irrelevant if clinical practice does not allow for reliable diagnoses, as they are a fundamental link between clinical practice and science.
Assessment Methods
Evidence-based best-practices for assessment include the use of behavioral rating scales and structured or semistructured (standardized) diagnostic interview tools. These help to ensure a broad assessment of symptoms and disorders, and in contrast to unstructured clinical interviews, increase the number of identified diagnoses (Matuschek et al., 2016). However, standardized interviews often require extra training and administration time. One practical approach to minimize time and unnecessary effort may involve using rating scales to first rule in (and rule out) areas of concern, and then administering the modules of a diagnostic interview most relevant to the referral issue and associated problems accordingly.
Tables 1 and 2 provide assessment tools, including both clinical interviews and rating scales, related to the measurement of these DSM-5 disorders. Note that these measures have been identified here for their ability to readily determine the presence or absence of DSM-5 symptoms of these disorders. Readers interested in more detailed information about the validation studies for measures of these disorders may be interested in a review by Walker et al. (2020). An evaluation of the relative strengths of some measures of disruptive behavior, broadly construed, can also be found by Becker-Haimes et al. (2021).
Assessment Tools for ODD, CD, & LPE
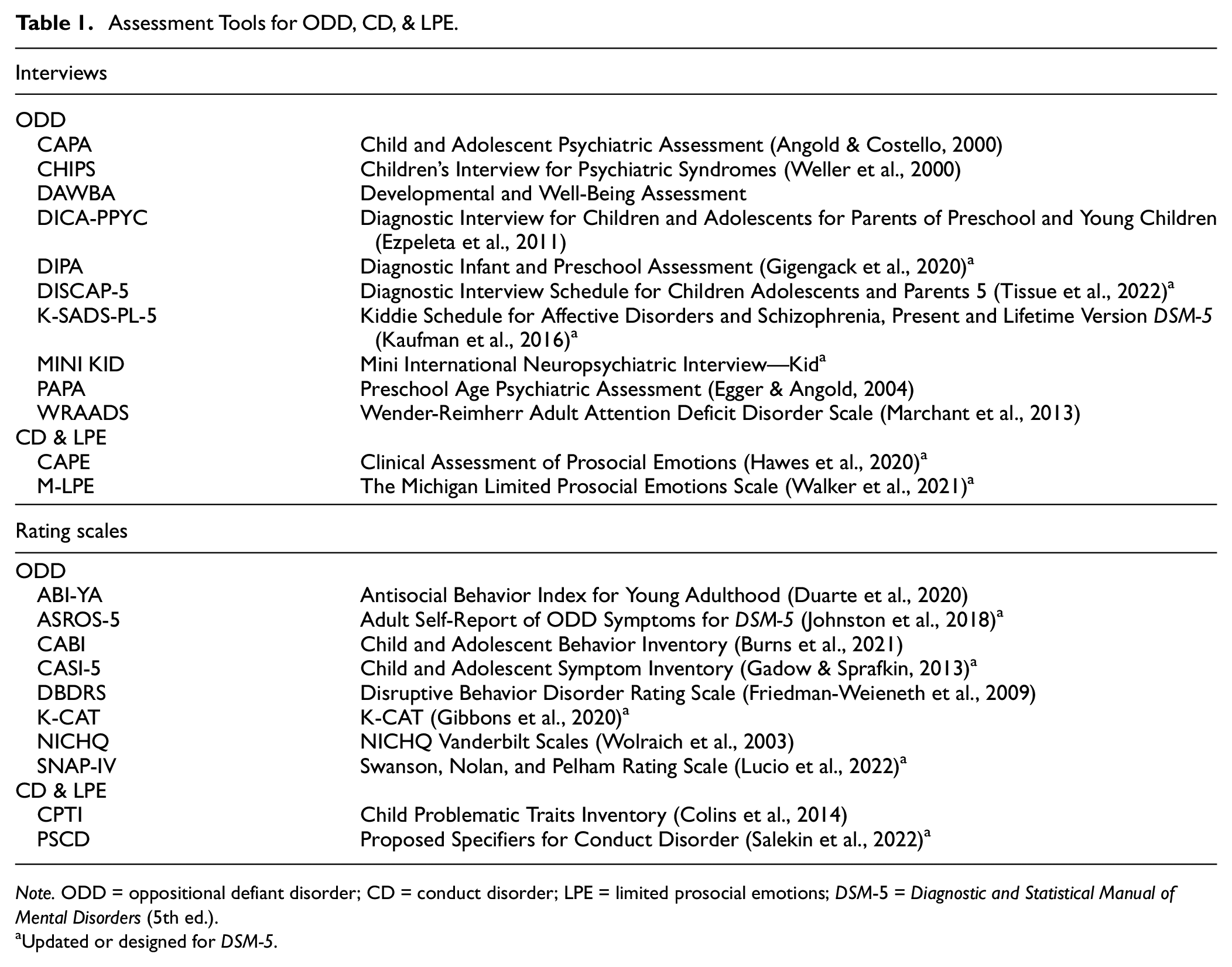
Note. ODD = oppositional defiant disorder; CD = conduct disorder; LPE = limited prosocial emotions; DSM-5 = Diagnostic and Statistical Manual of Mental Disorders (5th ed.).
Updated or designed for DSM-5.
Assessment Tools Related to DMDD, APD, and IED
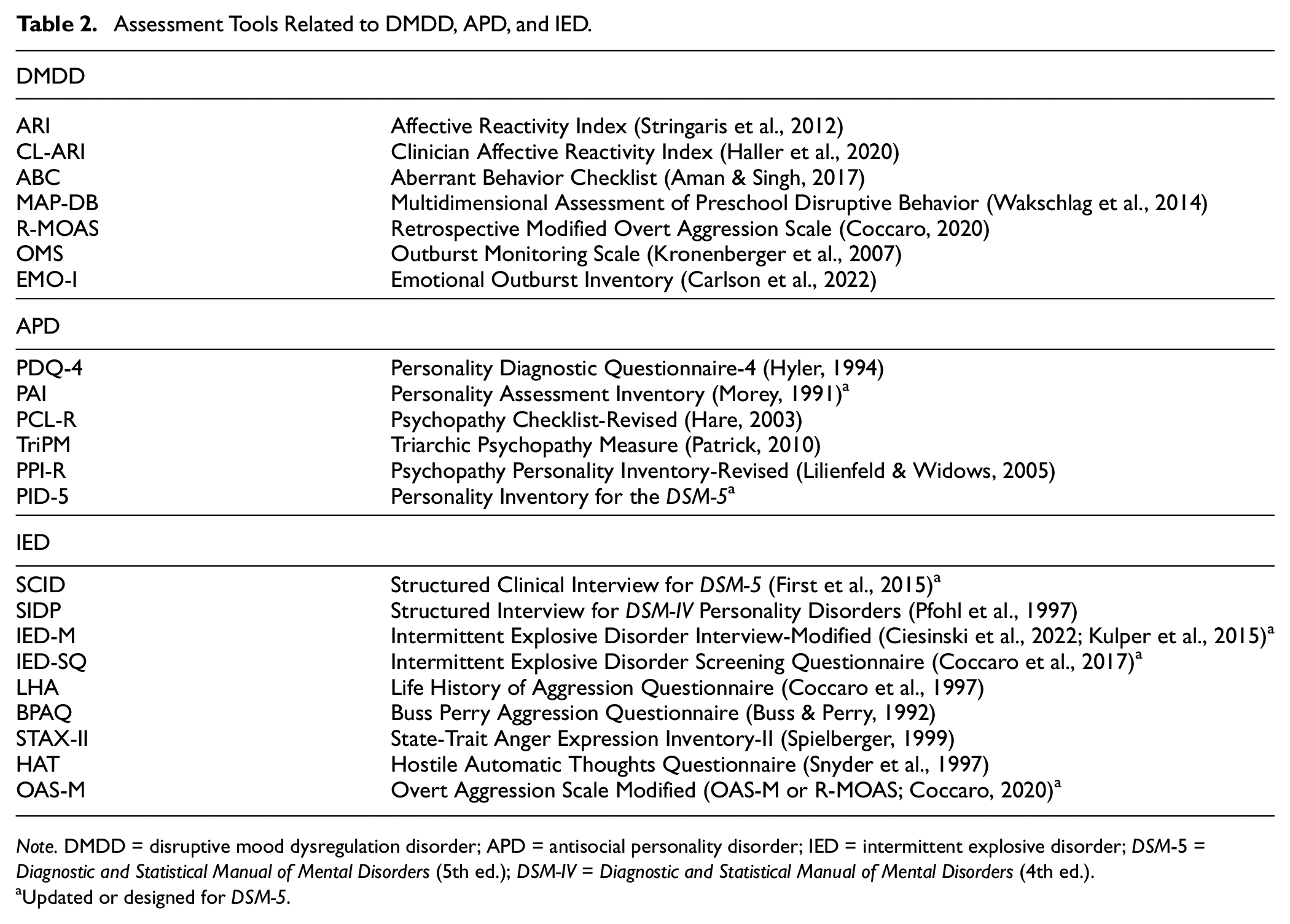
Note. DMDD = disruptive mood dysregulation disorder; APD = antisocial personality disorder; IED = intermittent explosive disorder; DSM-5 = Diagnostic and Statistical Manual of Mental Disorders (5th ed.); DSM-IV = Diagnostic and Statistical Manual of Mental Disorders (4th ed.).
Updated or designed for DSM-5.
Informant Effects
A long-standing challenge in the assessment of DBDs—though not distinct to the DBDs—is that different informants (e.g., parents, teachers, self-report) typically show low interrater agreement when rating the presence or severity of symptoms (e.g., De Los Reyes et al., 2015). Rather than attribute such differences to measurement error, discrepancies should be viewed as potentially related to variations in informant perspective and context. For example, classrooms, homes, neighborhoods, and other social contexts have different rules and expectations for behavior, provide different contingencies, yield varying levels of interactions with peers or siblings, and evoke fluctuations in the child’s emotion regulation, energy level, and intrinsic motivations.
Despite long-standing awareness of the issue, there continues to be a need for evidence and improved methods to help clinicians integrate varying informant reports (De Los Reyes et al., 2022; Martel et al., 2017). Assessments are clearly enhanced by obtaining reports from multiple informants, even though discrepancies between informants are the rule rather than the exception. Children have greater awareness of covert behavior and internal experiences, and teachers and parents observe behaviors in markedly different contexts. Finally, if criteria are met based only on a single informant’s report, this still conveys substantial prognostic risk and should not be discounted. For instance, parent and teacher (McNeilis et al., 2018) and parent and child reports (Evans et al., 2020) of ODD each were roughly equivalently and independently associated with other psychopathology.
Dimensionality Versus Discrete Categories
Categorical diagnoses provide clear utility in regard to clinical decision-making. For example, the presence or absence of a disorder helps to clarify the choice of evidence-based treatments, especially when the evidence base validating those treatments depended on categorizing the presence of that disorder. On the contrary, individual variability in the intensity or nature of symptom demonstration, impairments, and comorbid conditions highlight the limitations of a categorical approach. There is a growing movement toward dimensional classifications of psychological problems (e.g., Lahey, 2021). Pertinent to DBDs, Wakschlag and colleagues (2017) suggested a model involving four key dimensions in young children: noncompliance, irritability, aggression, and callousness. These four dimensions would represent most of the heterogeneous features captured by the symptoms of DBD and could also alleviate some concerns about categorical overlap. For older youth, on the contrary, symptoms pertaining to theft or status offenses, for example, might not coherently fall in the same dimension as noncompliance. Similarly, the reactive and impulsive aspects that may distinguish outbursts within IED might not allow for description within a single dimension of aggression. Empirical evidence regarding the superiority of categorical or dimensional diagnostic approaches is at this point ambiguous (Krueger et al., 2021; Thöne et al., 2022).
Assessment of Specific DBDs and Related Disorders
Oppositional Defiant Disorder
The symptoms that define ODD in DSM-5 (APA, 2013) have not changed much since Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994), when there were only minor changes from Diagnostic and Statistical Manual of Mental Disorders (3rd ed., rev.; DSM-III-R; APA, 1987). Currently, DSM-5 organizes the 8 Criterion A symptoms of ODD under three headings: Angry/Irritable Mood (loses temper; touchy or easily annoyed; angry and resentful); Argumentative and Defiant Behavior (argues with others; actively defies or refuses to comply; deliberately annoys others; blames others), and Vindictiveness, (spiteful or vindictive). These changes are generally consistent with evidence that ODD symptoms of anger and irritability have distinct prognostic utility relative to the behavioral symptoms (e.g., Burke et al., 2005, 2014, 2021; Evans et al., 2017; Waldman et al., 2021). However, DSM-5’s ODD has no subtypes or other meaningful distinctions based on these categories. In contrast, the International Classification of Diseases (ICD-11; World Health Organization [WHO], 2023) included subtypes for ODD with versus without chronic irritability anger (Evans et al., 2021).
Confirmatory factor analyses (CFAs) robustly support the distinction between the irritable and defiant symptom dimensions of ODD (e.g., Burke et al., 2014; Evans et al., 2017; Herzhoff & Tackett, 2016; Rowe et al., 2010; Waldman et al., 2021). Notably, this evidence stretches from preschool age (e.g., Ezpeleta et al., 2012) to adulthood (Gomez & Stavropoulos, 2019; Johnston et al., 2020). However, latent classification and trajectory models have shown mixed findings. Some have supported dimension-based classification (e.g., Burke, 2012; Herzhoff & Tackett, 2016) or trajectories (e.g., Ezpeleta et al., 2020). Others find only distinctions based on overall ODD symptom severity, rather than distinctions between symptom dimensions (Racz et al., 2022; Roetman et al., 2021). Finally, in a community sample of children, a factor mixture modeling approach found evidence for both; ODD symptoms varied over three levels of intensity within three distinct symptom dimensions (Gomez & Stavropolous, 2018).
A fundamental takeaway is that the dimensions of ODD are distinct but not separable. Failing to recognize the chronic irritability dimension within ODD historically led to ignorance regarding increased risks for depression, anxiety, and suicidality among those with ODD. Conversely, if one fails to consider oppositional or defiant behavior while assessing chronic irritability, one may be ignorant of impairments and risks for future antisocial behavior. In terms of assessment methods, no particular changes are required beyond using existing methods or measures of ODD (described below) to sufficiently capture the information needed to identify chronic irritability. One need only attend to the presence and intensity of specific ODD symptoms. There is not yet empirical guidance for categorically identifying the presence of chronic irritability within ODD. The ICD-11 (WHO, 2023) provides guidelines and allows the clinician to determine whether chronic irritability/anger is present, while DSM-5 allows no such determination.
Older measures of irritability typically conflated irritability with aggressive or oppositional behaviors (see e.g., Holtzman et al., 2015), often confounding each within multiple items. Thus for diagnostic purposes, care should be taken in using measures that clearly assess each symptom distinctly. On the contrary, many new measures of chronic irritability based on DSM-5 exclude symptoms of ODD behavioral dimension. This is particularly true for those intended to measure DMDD (see discussion below). As a result, much of the research on DMDD commonly fails to account for effects attributable to oppositional or defiant behavior and not to chronic irritability.
Diagnostic Interviews for ODD
In general, structured diagnostic measures show very good psychometric properties for the assessment of ODD in youth. A recent meta-analysis of standardized diagnostic interviews found that the test–retest reliability for ODD was higher for parent interviews (κ = .59) than for child interviews (κ = .39), underscoring the importance of including parents/caregivers in multi-informant assessments (Duncan et al., 2019). Perhaps the most widely used in research is the Kiddie Schedule for Affective Disorders and Schizophrenia, Present and Lifetime Version DSM-5 (K-SADS-PL-5; Kaufman et al., 2016). Web-based self-administered versions for parent and child report have recently been developed with good initial psychometric evidence (Townsend et al., 2020). Many of the major diagnostic interviews for youth have been slow to update from DSM-IV versions. Given the minimal changes that have been made to the diagnostic formulation for ODD, it is reasonable, when necessary, to use a DSM-IV diagnostic interview to assess for DSM-5 ODD. From this perspective, other diagnostic interviews with good psychometric properties for ODD in youth include the Child and Adolescent Psychiatric Assessment (CAPA; Angold & Costello, 2000) and the Diagnostic Interview Schedule for Children (DISK; Shaffer et al., 2000). Others have been developed for administration that require less training and time to administer, including the Developmental and Well-Being Assessment, the Mini International Neuropsychiatric Interview for Kids, and the Children’s Interview for Psychiatric Syndromes (Weller et al., 2000).
Rating Scales for ODD
Many symptoms of ODD are behaviorally observable and can be reliably assessed, at least partially, through the use of multi-informant rating scales and checklists that map on to the criteria for ODD. The Child and Adolescent Behavior Inventory (CABI; Burns et al., 2021) has been validated in preschool samples. The Swanson, Nolan, and Pelham Rating Scale (Lucio et al., 2022) assesses ODD and has been validated for use in children as young as 3.5 years of age. The Child and Adolescent Symptom Inventory (CASI-5; Gadow & Sprafkin, 2013) includes parent and teacher report versions with items measuring multiple DSM-5 disorders in youth. Finally, a rapid screener called the Kiddie Computerized Adaptive Test (K-CAT) collects dimensional child- and parent-report of ODD via tablet computers in approximately 64 seconds. High concordance with K-SADS generated diagnoses (Gibbons et al., 2020) has been demonstrated, and the entire K-CAT screening of ODD, CD, ADHD, anxiety, depression, mania, and suicidality can be completed in under 8 minutes.
Assessing for ODD Across the Lifespan
Epidemiological research suggests that approximately 10.2% of individuals in the population will experience ODD in their lifetime (Nock et al., 2007). Thus, there is a need for assessments of the disorder across the lifespan. Some clinicians may object to diagnosing ODD in early childhood due to concerns that ODD is hard to distinguish from normative toddler behavior. On the contrary, best-practice assessment approaches with reference to established diagnostic criteria do not pathologize normative behavior in preschool-aged children (Burns et al., 2020; Keenan & Wakschlag, 2004), and can discern both chronic irritability and oppositional behavioral dimensions in preschoolers (Ezpeleta et al., 2020). The validity of diagnosis for pre-verbal children may be consistent with the evidence described above for the equivalent utility (if not agreement) across different informant reports (e.g., Evans et al., 2020; McNeilis et al., 2018).
When working with young children (e.g., toddler to kindergarten age), it is advisable to use interviews that are developmentally appropriate, such as the Diagnostic Interview for Children and Adolescents for Parents of Preschool and Young Children (Ezpeleta et al., 2011). The PAPA is a preschool-age version of the CAPA (noted above), and the Diagnostic Interview Schedule for Children Adolescents and Parents-5 (DISCAP-5; Tissue et al., 2022) has been validated for children as young as 2 years of age and also assesses for CD and LPE. The Diagnostic Infant and Preschool Assessment has been validated for children between 1.5 and 7 years of age in the United States (Scheeringa & Haslett, 2010), Danish (Løkkegaard et al., 2018) and Dutch (Gigengack et al., 2020) samples.
Initial evidence suggests that ODD can be reliably assessed in adulthood (e.g., Barry et al., 2013; Gomez & Stavropoulos, 2019), and early validation of a few measures has been produced. These include the Adult Self-Report of ODD Symptoms, DSM-5 (Johnston et al., 2018), the Wender-Reimherr Adult Attention Deficit Disorder Scale (Marchant et al., 2013). The Antisocial Behavior Index for Young Adulthood consists of items assessing clinician-rated severity of behaviors consistent with ODD, CD, and delinquency and has shown good initial psychometric properties (Duarte et al., 2020). Research continues to build the evidence base for tools for assessing ODD in adults. For now, applying the ODD diagnostic criteria as given in the DSM-5 appears to work reasonably well to identify the disorder in adulthood.
Conduct Disorder
The diagnosis of CD represents a pattern of behaviors that violate the rights of others or of societal rules. To meet criteria in the DSM-5 (APA, 2013), a person must show at least three of 15 symptoms within the past year, including at least one in the past 6 months. These 15 symptoms are organized within four categories: Aggression to People and Animals, Destruction of Property, Deceitfulness, or Theft and Serious Violations of Rules. The estimated lifetime prevalence of CD is around 9.5% (Nock et al., 2006). Multiple subtypes/specifiers are applicable to CD in DSM-5. In addition to severity specifiers (mild, moderate, severe), one important subtype is age of onset, indicating whether the symptoms first emerged prior to around 10 years of age (childhood-onset) or if they began later (adolescent-onset). Earlier onset is linked to more severe and persistent patterns of behavior over the lifespan and has been part of the diagnosis since DSM-IV (Frick & Nigg, 2012).
The most substantial modification to CD in DSM-5 was adding the Limited Prosocial Emotions (LPE) specifier, which has important developmental and prognostic implications (Frick & Nigg, 2012). To meet criteria for CD with LPE, an individual must show at least two of the following four characteristics persistently, in multiple relationships and settings, over at least 12 months: lack of remorse or guilt, callous-lack of empathy, unconcerned about performance, and shallow or deficient affect. Including LPE as a specifier was supported by an expansive literature showing that callous-unemotional features (Frick et al., 2014) identify a meaningful subgroup of youth with severe conduct problems who show clinically distinct presentations, prognostic risks, or poor response to treatment. On the contrary, studies have not always supported the clinical utility of the LPE specifier (e.g., Bansal et al., 2023; Dery et al., 2019). Some argue that a broader multidimensional model of psychopathy would provide greater clinical utility (Lahey, 2014). That is, in addition to the CU/LPE features, other dimensions such as grandiose-manipulative and daring-impulsive behaviors could be included as part of the formulation of CD (Lee, 2018; Salekin, 2016; Salekin et al., 2018).
Diagnostic Interviews for CD
With few exceptions, the interviews and rating scales described above for assessing ODD also include questions for assessing CD. For DSM-5 CD, new measures that include LPE must be used (see Table 1). Some stand-alone interviews for LPE have been developed. The Clinical Assessment of Prosocial Emotions is a semistructured multi-informant clinical interview (Hawes et al., 2020) specific to LPE. Validation studies have included children from ages 3 to 21. The Michigan Limited Prosocial Emotions was developed to be administered as an addendum to the K-SADS (Walker et al., 2021). Spanish language versions of the K-SADS-PL-5 for CD and LPE have been validated for parent and teacher report in a sample of Spanish first graders (Seijas et al., 2018), and for parent- and child-report among youths ages 6 to 18 in Mexico, Chile, Colombia, and Uruguay (de la Pena et al., 2018). The DISCAP-5 (Tissue et al., 2022) assesses for CD and LPE.
Rating Scales for CD
Several rating scales and checklists have been developed to measure CD and LPE. The CASI-5 includes parent and teacher report versions (Gadow & Sprafkin, 2013). The CABI (Burns et al., 2021) measures LPE (but not CD) and has been validated with children as young as 4 years of age. Although existing rating scales of CU are not specific to LPE, studies have shown that it is possible to use CU self-report (Kimonis et al., 2015) or parent and teacher report (Waschbusch et al., 2020) to assess LPE (see also Colins et al., 2020 for a systematic review). The Proposed Specifiers for Conduct Disorder (PSCD) was developed to assess the multidimensional model of psychopathy with scales for CU, grandiose-manipulative and daring-impulsive, along with a limited set of CD items. Validation studies of self-report versions have been conducted in samples adolescents in the United States (Salekin et al., 2022), Iran (Elhami Athar et al., 2022), China (Luo et al., 2021), Italy (Muratori et al., 2021), and Portugal (Ribeiro da Silva et al., 2021) and among detained Belgian youth (Colins et al., 2022). A shortened self-report version has been tested in a sample of Spanish adolescents (Lopez-Romero et al., 2022), and a parent-report version in a sample of Spanish preschoolers between 3 and 6 years of age (Lopez-Romero et al., 2019). It should be noted however that the PSCD does not assess all DSM-5 CD symptoms and does not specifically assess LPE. In particular, it provides little information to assess the LPE characteristic of unconcerned about performance.
Assessing for CD Across the Lifespan
As with ODD, evidence continues to accrue to support the validity and utility of diagnosing CD in early childhood, and measures have been validated for CD and LPE in very early childhood. For example, the DISCAP-5 (Tissue et al., 2022) has demonstrated good concurrent and discriminant validity as well as good interrater reliability among children as young as age 2. While the concept of diagnosing a preschool child with CD with LPE might be challenging, it is important to understand that the diagnosis does not categorize the child, it categorizes a portion of the child’s problematic experiences to provide for accurate conceptualization and treatment planning. CD may also be diagnosed in adulthood, as discussed in the APD section below.
Disruptive Mood Dysregulation Disorder
Classified as a Depressive Disorder in DSM-5, DMDD is covered in this article because it often co-occurs and is part of the differential diagnosis with other disorders characterized by disruptive behavior, temper outbursts, and aggression (APA, 2013; Roy et al., 2014; Stringaris et al., 2018). DMDD is a relatively controversial new diagnosis, introduced for the first time in DSM-5 (APA, 2013). Accordingly, the evidence base for DMDD is new and limited in many respects. For example, DMDD prevalence estimates are typically based on secondary analyses of epidemiological data, and treatment guidelines are extrapolated from knowledge about evidence-based treatments for problems with similar presentations (e.g., ODD, aggression; Baweja et al., 2016; Bruno et al., 2019; Stringaris et al., 2018). Similar limitations extend to assessment and diagnosis. With these caveats in mind, DMDD is nonetheless a major diagnosis, increasingly applied to children and adolescents, and with important clinical implications (Findling et al., 2022; Fristad et al., 2021). Assessment of DMDD can be especially challenging, given high rates of comorbidity and the transdiagnostic character of irritability (Evans et al., 2017). Thus, particular care is warranted in the assessment and diagnosis of DMDD.
Clinically, DMDD is defined by two major symptom components. First, there are severe and recurrent temper outbursts, occurring at least three times per week, including verbal or physical aggression that is developmentally and contextually inappropriate. Second, in between outbursts, individuals with DMDD experience persistently irritable or angry mood, most of the time on most days, and observable to others (e.g., parents, teachers, peers). These symptoms must be largely present for at least 12 months, occurring in at least two of three settings (at home, at school, with peers) and severe in at least one. Finally, symptom onset must occur prior to age 10, and the initial diagnosis cannot be made before age 6 or after age 18 (APA, 2013).
The history of DMDD is beyond the scope of this review and has been detailed elsewhere (e.g., Brotman et al., 2017; Burke et al., 2021; Evans et al., 2017; Leibenluft, 2011; Roy et al., 2014). However, a few pieces are relevant for assessment. DMDD arose from research aimed at testing whether chronic irritability was distinct from pediatric bipolar disorder. A meta-analysis found that chronic irritability predicted future anxiety, depression, and ODD, and found no evidence supporting a prediction to bipolar disorder (e.g., Vidal-Ribas et al., 2016). Accordingly, DSM-5 stipulates that the diagnoses of DMDD and bipolar disorder cannot co-occur (APA, 2013). Much of the relevant evidence for DMDD comes from research on its predecessor, severe mood dysregulation (SMD), a syndrome defined by Leibenluft et al. (2003; see also Leibenluft, 2011). Although roughly similar, DMDD and SMD have key differences with important implications. For example, SMD’s criteria included hyperarousal, dysphoric mood, and IQ ≥ 80. In contrast, DMDD’s criteria do not include any of these features, but they were elaborated and tightened in other ways (e.g., persistence and duration of irritable mood, symptoms, and impairment across settings). In other words, DMDD is designed to be relatively severe and rare. In community data sets, the estimated prevalence of DMDD ranges from less than 1% (0.1%–3.3%; Althoff et al., 2016; Copeland et al., 2013) to as high as 7% (Moore et al., 2019), with irritable mood and temper outbursts being far more common. More recently, Laporte et al. (2021) converged on a prevalence estimate of around 3%.
In addition, DSM-5 stipulates that DMDD cannot be diagnosed alongside ODD or IED. When the full presentation coexists with either of these other conditions, only DMDD should be diagnosed (APA, 2013). Although research on the relationship between DMDD and IED is limited (for exceptions, see Coccaro, 2018; Radwan, & Coccaro, 2020), both are defined by aggressive outbursts, with DMDD additionally having persistent mood features. The relationship between DMDD and ODD symptoms is more complicated. For example, ICD-11(WHO, 2023) rejected DMDD because the evidence base was not sufficient and instead led them to code chronic irritability/anger as a subtype of ODD (Evans et al., 2017, 2021; Lochman et al., 2015). Despite this difference, ICD and DSM formulations both suggest that DMDD is a severe and impairing problem defined by irritable mood and temper outbursts. In fact, DMDD is so closely related to ODD that, were it not for this exclusionary rule in DSM-5, nearly 100% of youths with DMDD would also have ODD (Axelson et al., 2012; Evans et al., 2017; Freeman et al., 2016). To summarize the takeaways relevant to assessment: DMDD is distinct from bipolar disorder, linked to internalizing and externalizing disorders, and empirically overlaps with ODD.
There are few established instruments or guidelines for assessing irritability in youth, and even fewer for DMDD (Baweja et al., 2016; McTate & Leffler, 2017). A recent systematic review (Mürner-Lavanchy et al., 2021) found that, of 110 studies published on DMDD since 2013, more than two-thirds measured the diagnosis using questionable strategies like interviews not designed for DMDD (47%), chart review (7%), diagnoses assigned using no particular instrument (6%), or assessment information not reported (9%). The K-SADS, as noted above (Kaufman et al., 1997, 2016), has been updated for DSM-5 to include DMDD/SMD. It is the most common diagnostic tool, used in ∼25% of recent DMDD studies (Mürner-Lavanchy et al., 2021). Other common DSM-based interviews (e.g., Angold & Costello, 2000; Goodman et al., 2000; Shaffer et al., 2000) were not designed for DMDD. Accordingly, there is a need for clinically oriented approaches with useful, efficient, and established tools (e.g., Sheehan et al., 2010; Weller et al., 2000) to ascertain whether DMDD is present (McTate & Leffler, 2017).
A handful of rating scales and multi-informant instruments are worth noting. The Affective Reactivity Index (ARI; Stringaris et al., 2012) is a brief, general irritability symptom rating scale by parent- and youth-report for research and clinical purposes and has recently been extended with the creation of the Clinician ARI (CL-ARI; Haller et al., 2020). For irritability and aggressive outbursts in DMDD, other empirically supported instruments include the irritability scale of the Aberrant Behavior Checklist (Aman & Singh, 2017), the Multidimensional Assessment of Preschool Disruptive Behavior (Wakschlag et al., 2014), and the Retrospective Modified Overt Aggression Scale (Coccaro, 2020). Although there have been some efforts to develop self- and proxy-report scales that map on to DMDD diagnostic requirements (e.g., Boudjerida et al., 2022), this evidence is still limited and preliminary. However, results are promising for a few brief, free, clinical/research measures relevant to DMDD like the Outburst Monitoring Scale (Kronenberger et al., 2007) and the Emotional Outburst Inventory (Carlson et al., 2022).
All these tools (and their limitations) underscore the need for work on integration of multi-informant and multimethod data (De Los Reyes et al., 2015; Youngstrom et al., 2020), which should include DMDD. Although some research has found no effects of gender in DMDD prevalence (Althoff et al., 2016; Dougherty et al., 2014), the bulk of the evidence suggests a male preponderance for DMDD (APA, 2013; Evans et al., 2017; Hartung & Lefler, 2019). Some evidence suggests DMDD and irritability are applicable internationally (Tiwari et al., 2016; Toohey et al., 2020), but clinicians struggled to accurately and reliably diagnose DMDD in cross-national field studies (Evans et al., 2021; Regier et al., 2013). Looking ahead, there is a need for DMDD assessment research that is both diagnostic and transdiagnostic, both for evaluating existing tools and for advancing new methods. For example, the contextual and time-varying nature of DMDD (e.g., frequency, duration, and triggers of irritable outbursts) lends itself well to ecological momentary assessment approaches (e.g., Naim et al., 2021). Advancing measurement can help clarify phenomenology and treatment of DMDD, including how it relates to other problems of irritable mood and aggressive behavior.
Antisocial Personality Disorder
APD reflects a pervasive pattern of disregard for and the violation of the rights of others, including three or more of the following: failure to conform to social norms with respect to lawful behaviors, deceitfulness, impulsivity, irritability and aggressiveness, reckless disregard for safety of self or others, consistent irresponsibility, and lack of remorse (APA, 2013). For the diagnosis of APD to be made, the individual must be at least 18 years of age, and antisocial behavior must have been evident prior to age 15 (APA, 2013). The DSM has never prohibited giving a diagnosis of CD to someone over the age of 18, as long as the criteria for APD were not met. Since antisocial personality features have been incorporated into the diagnosis of CD with the specifier for LPE, the distinction between APD and CD is less clear. For example, APD is classified in DSM-5 both in the Personality Disorders section and in Disruptive, Impulse-Control, and Conduct Disorders section.
Individuals with APD often have a history of adverse childhood experiences, and frequently have family members with APD or similar difficulties, such as criminal offending (DeLisi et al., 2019). Although estimates vary, evidence suggests that APD occurs in approximately 3% to 5% of adults in the United States. A subset of those with APD also have features of psychopathy, such as callousness and remorselessness (Goldstein et al., 2017; Johnson, 2019). As many as one in four adults exhibit antisocial behavior that may be clinically important and similar to APD but fall short of the meeting the full diagnostic criteria (Goldstein et al., 2017).
Regarding self-report rating scales, measures such as the Personality Diagnostic Questionnaire-4 (Hyler, 1994) and the Personality Assessment Inventory (Morey, 1991) have shown promise in the measurement of APD or overlapping personality traits, with empirically supported clinical cutoffs or t scores. A larger evidence base exists for measures of psychopathy, which overlaps with but is distinct from APD (see more on PSCD in the CD section, above). The Psychopathy Checklist-Revised (PCL-R; Hare, 2003) is one of the most widely used clinical assessment tools for psychopathy and provides another option besides the PSCD. The PCL-R has been primarily used in forensic settings and has shown notably different characteristics when used with male versus female offenders (Dolan & Völlm, 2009). Other measures with good psychometrics for measuring psychopathy in forensic samples include the triarchic psychopathy measure (Patrick, 2010) and the psychopathy personality inventory – revised (Lilienfeld & Widows, 2005). The best practice for assessment includes multiple informants (De Los Reyes & Makol, 2021), although for adult assessments, finding collateral informants (e.g., a partner, friend, or co-worker) can be challenging.
In DSM-5, APD is, like most diagnostic entities, categorical in nature. Consistent with calls for a dimensional approach, the Alternative Model of Personality Disorders (AMPD) has been proposed. It incorporates a multidimensional conceptualization, with two parts: Criterion A, level of personality functioning, including impairments in interpersonal functioning, and Criterion B, a five-domain model of maladaptive dimensional traits (Widiger & McCabe, 2020). When applied to APD, Criterion A impairment includes deficits in prosocial ability, lack of concern for other people, egocentricity, and attempts to control others through dominance. Criterion B traits may include manipulativeness, hostility, deceitfulness, callousness, risk-taking, irresponsibility, and impulsivity (Anderson & Kelley, 2022). In addition, the AMPD includes a psychopathy specifier, characterized by low anxiousness, low withdrawal, and attention seeking (Wygant et al., 2016). In line with the AMPD, the Personality Inventory for the DSM-5 has been developed and implemented as an assessment tool, with promising psychometrics; but questions about discriminant validity and clinical utility remain (Al-Dajani et al., 2016).
APD research has predominantly involved male samples. A systematic review of tools for APD and psychopathy in women found that some measures yield different factor structures for women and men and that evidence of predictive validity for institutional violence and re-offending in is variable in women (e.g., PCL-R; Psychopathy Checklist: Screening Version; Dolan & Völlm, 2009). Evidence also suggests that prevalence rates for APD may vary across racial, ethnic, or sociodemographic lines (Goldstein et al., 2017). Here too, multi-informant and multi-method approaches may prove to be especially variable for assessing antisocial traits across the lifespan.
Intermittent Explosive Disorder
Finally, IED is an impulse control disorder marked by frequent and intense aggressive outbursts (APA, 2013). These outbursts are not premeditated, are out of proportion to preceding stressors, and may result in physical aggression toward property or other individuals. IED is highly comorbid with other psychopathology, including ODD, CD, and substance use disorder (Radwan & Coccaro, 2020; Scott et al., 2016). The features overlap substantially with other disruptive behavior disorders, such as aggressive outbursts within DMDD, temper loss or touchiness within ODD, or the disposition to aggressive behavior of CD. A recent international epidemiological study found that the mean onset for IED was 17 years, with a lifetime prevalence rate of about 0.1% to 2.7% (Scott et al., 2016). However, IED can be diagnosed as young as 6 years old (APA, 2013). In this way, IED explicitly differs from DMDD, which is operationalized as a disorder of childhood and adolescence. IED can occur across lifespan development, but longitudinal evidence regarding its stability over time is limited. Kessler et al. (2011) provide some inferential evidence suggestive of stability of IED, at least in a narrow-band conceptualization indexed primarily by anger attacks. Currently, little guidance for validated intervention for IED is available. One recent clinical trial has found support for the use of cognitive behavioral therapy to decrease IED symptoms and impulsive aggression in adults (McCloskey et al., 2022).
There are few instruments available specifically for the diagnostic assessment of IED. This resource gap may be attributed to the dearth of research on the disorder and the heterogeneity in criteria sets used to diagnose it (McCloskey et al., 2012). Some measures are available that may assist with the diagnosis of IED, including the Structured Clinical Interview for DSM-5 (SCID; First et al., 2015), the Structured Interview for DSM-IV Personality Disorders (SIDP; Pfohl et al., 1997), the Intermittent Explosive Disorder Interview-Modified (IED-M; Ciesinski et al., 2022; Kulper et al., 2015), and the Intermittent Explosive Disorder Screening Questionnaire (IED-SQ; Coccaro et al., 2017). These tools have been found to have good reliability and validity, with differences in whether they ascertain a current or past diagnosis of IED in patients. However, the evidence for the utility of these measurements in clinical settings is mixed. For example, no study has assessed the efficacy of the IED-SQ in clinical settings, it has only been used in research environments. On the contrary, the SCID, SIDP, and IED-M have been used to diagnose patients prior to inclusion in clinical treatment studies for IED (McCloskey et al., 2008, 2022) but not to assess changes throughout treatment. Given relatively high rates of IED in outpatient psychiatric settings (Coccaro et al., 2005), there is a need for instruments that are brief and psychometrically well-supported in this realm.
A variety of measures that might help researchers and clinicians better clarify a patient’s experiences with IED symptoms in the context of related aggressive behaviors are available. Some potentially useful supplementary measures include the Life History of Aggression Questionnaire (Coccaro et al., 1997), the Buss Perry Aggression Questionnaire (Buss & Perry, 1992), the State-Trait Anger Expression Inventory-II (Spielberger, 1999), the Hostile Automatic Thoughts Questionnaire (Snyder et al., 1997), and the Overt Aggression Scale Modified (OAS-M; Coccaro, 2020). These questionnaires provide different insights into the unique aggressive impulses expressed by IED patients and have all been found to have good reliability and validity. The OAS-M is of particular interest as it was developed for use in randomized clinical trials and has shown evidence of change in aggressive symptomatology during these trials (Coccaro, 2020). The OAS-M may be useful for clinical work by assessing changes in symptomatology throughout treatment, but future research is needed to assess its efficacy in these contexts.
Presently, IED remains understudied, especially in children and adolescents. There is a paucity of strong methods for assessing the disorder (McCloskey et al., 2012), particularly for IED in childhood. The majority of IED questionnaires span extensive periods of the lifespan, and to date, only one has been validated for children under 14 years of age (Olvera et al., 2001). Relatedly, there is no IED questionnaire to our knowledge that uses multiple informants, which is critical to understanding the presentation of disruptive behavior disorders in childhood (De Los Reyes et al., 2009; Hart et al., 1994). New and established measures that incorporate multiple informants are needed for adolescents and young adults in particular given the high rates and peak onset of IED in this age range (Scott et al., 2016). Future research also needs to ensure the inclusion of diverse populations in measurement development to help establish the generalization of these assessments across contexts. This is of particular necessity, given the presence of IED across gender, socioeconomic, racial, and ethnic backgrounds (Coccaro, 2012). By integrating these changes and conducting more research on IED, we can advance the assessment of the disorder for the benefit of patients and their families.
Conclusions
Perhaps the most important piece of guidance for the assessment of the Disruptive, Impulse Control, and Conduct Disorders appears the most banal: follow the diagnostic guidelines. Doing so minimizes concerns related to pathologizing normative behavior and allows one to help families understand and change impairing behavior even in very early childhood. To achieve this; however, knowledge of the criteria by themselves is not enough. Evidence-based assessment is enhanced by the use of a broader set of tools and reliance on an empirical knowledge base. Combining careful assessment of symptoms with a mindful awareness and appropriate application of diagnostic criteria may also reduce the impact of racial biases that lead some clinicians to misdiagnose behavioral disorders when they are not present. Combined with up-to-date knowledge of comorbidities and developmental psychopathology, this may reduce misdiagnoses of trauma, anxiety-related or other disorders when disruptive behavior disorder should be identified. Clinicians should remember that diagnoses describe problems, not people, and thus ruling them in or out is fundamental to a well-constructed conceptualization that will best serve treatment planning and maximize good outcomes. Augmenting clinical interviews with rating scales, checklists, and standardized diagnostic interviews is highly recommended. Not only may it improve efficiency of testing, it may also make it more feasible to get the perspective of multiple informants and collect the associated information needed for differential diagnosis, screening out disorders, and identifying factors that could be better explanations for clinical phenomena.
Substantial needs remain in regard to empirical evidence to guide assessment. Research must examine cross-cultural issues related to the valid use of the diagnostic criteria for these disorders, identifying both consistencies and inconsistencies. More widespread good clinical practice will be enhanced by empirical evidence to describe any actual stigma that arises from using these clinical labels. Disruptive behavior problems are highly impairing, and those suffering from it benefit most from careful and straightforward assessment, diagnosis, and treatment. Good practice to these ends is highly achievable.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.