
Abstract
Dysfunctional expectations are a particularly important subset of cognitions that influence the development and maintenance of various mental disorders. This study aimed to develop and validate a scale to assess dysfunctional expectations in posttraumatic stress disorder (PTSD), the “Posttraumatic Expectations Scale” (PTES). In a cross-sectional study, 70 PTSD patients completed the PTES, the Posttraumatic Cognitions Inventory (PTCI), as well as measures of the severity of symptoms of PTSD and depression. The results show that the PTES has excellent internal consistency and correlates significantly with the PTCI and PTSD symptom severity. A regression analysis revealed that the PTES explained variance of PTSD symptom severity above the PTCI, supporting the incremental validity of the PTES. While the original version of the PTES comprises 81 items, short scales were constructed using the BISCUIT (best items scales that are cross-validated, unit-weighted, informative and transparent) method. The current findings provide preliminary psychometric evidence suggesting that the PTES is an internally consistent and valid novel self-report measure in patients with PTSD. However, conclusions about the psychometric properties of the PTES are limited because of the absence of criterion-related validity, factor structure evidence, variability over time/response to intervention, and test–retest reliability. Future research should use the PTES in large-scale longitudinal studies to address these aspects to further validate the scale.
While the psychopathology of posttraumatic stress disorder (PTSD) is multifaceted and complex, the role of dysfunctional cognitions has regained attention in PTSD research in the last decade (Woud et al., 2019). In cognitively focused PTSD research, it is well known that the view of the world changes dramatically after exposure to a traumatic event (Bernardi et al., 2019; Brown et al., 2018; LoSavio et al., 2017). More specifically, research indicates that a traumatic event violates people’s “belief in a just world” (Dalgleish, 2004) and as a result, negative beliefs about the world, other people, and oneself are formed (Woud et al., 2019). Importantly, research found that negative appraisals of the traumatic event and its consequences are strongly associated with PTSD symptom severity; in addition, the persistence of such negative reappraisals predicts later symptom severity (Ehring et al., 2008; Kleim et al., 2013; ter Heide et al., 2017). Accordingly, the Diagnostic and Statistical Manual of Mental Disorders–fifth edition (DSM-5) included cognitive changes after the experience of a traumatic event as part of the new symptom cluster D “negative alterations in cognition and mood”(American Psychiatric Association, 2013), highlighting the importance of further research on the role of dysfunctional cognitions in PTSD.
Several insightful theories have been developed to elucidate how cognitive factors contribute to the development and maintenance of PTSD symptoms, such as the emotional processing theory (Foa & Kozak, 1986; Rauch & Foa, 2006) and the cognitive processing approach by Resick and Schnicke (1992). One of the most influential cognitive approaches to PTSD is the cognitive model of PTSD, developed by Ehlers and Clark (2000). This model assumes that PTSD symptoms persist when people continue to perceive the trauma with a sense of threat, resulting from negative appraisals of the traumatic event and distortions in autobiographic memory. Numerous empirical studies support the assumptions of the model by Ehlers and Clark (2000): they have shown that negative cognitions are associated with PTSD symptom severity and contribute to their exacerbation and maintenance (Dunmore et al., 1999; Ehring et al., 2008; Halligan et al., 2003; Kleim et al., 2013; ter Heide et al., 2017). Drawing on such cognitive accounts, psychological treatments focusing on the modification of dysfunctional cognitive processes have been developed, such as the cognitive processing therapy (CPT; Resick & Schnicke, 1992) and the cognitive therapy for PTSD (CT-PTSD; (Ehlers, 1999; Ehlers & Clark, 2000).
In recent years, expectations have received particular attention in research on aberrant cognitive processes across mental disorders (Rief et al., 2015). Expectations, defined as a subgroup of cognitions, relate to the likelihood of the occurrence of future events or experiences (Kube et al., 2017; Laferton et al., 2017; Olson et al., 1996). Unlike more general negative appraisals and dysfunctional cognitions, expectations offer the advantage of being amenable to a relatively straightforward empirical confirmation versus disconfirmation due to their “if, then” structure (Rief et al., 2015). Thus, dysfunctional expectations might be a promising target in the cognitive-behavioral treatment of PTSD, as they may provide the basis of behavioral experiments in which patients sample new information that helps them revise their initial expectations (Craske et al., 2014; Murray & El-Leithy, 2020; Rief et al., 2015). Neuroscientific and computational approaches that conceive PTSD in terms of hyper-precise prior predictions referring to the anticipation of threat recently spelled out the importance of expectations. Hence, they shape perception toward the continued experience of threat, much like a self-fulfilling prophecy (Kube et al., 2020; Linson & Friston, 2019). Indeed, findings of an empirical study using the trauma film paradigm suggest that expectations might play an important role in the development of intrusive memories (Herzog et al., 2022)—the hallmark symptom of PTSD (Brewin, 2015; Iyadurai et al., 2019; Yehuda et al., 2015).
To systematically investigate how dysfunctional expectations influence the course of PTSD, it is important to be able to assess several types of expectations that are core to PTSD. Although we are cognizant of some assessment tools that aim to examine dysfunctional cognitions in PTSD, such as the Posttraumatic Cognition Inventory (PTCI; Dunmore et al., 1999; Ehlers, 1999) and the Posttraumatic Maladaptive Beliefs Scale (PMBS; Vogt et al., 2012), 1 there is, to our knowledge, no measure available that focuses specifically on expectations in PTSD, in terms of testable future-directed hypotheses that are put in an “if-then” structure—a feature that is often missing in other scales. Existing measures such as the PTCI partly include testable future-directed cognitions. However, not all of PTCI items reflect testable predictions that could be examined in hypothesis-testing interventions, such as behavioral experiments—the backbone of trauma-focused cognitive-behavioral therapy (CBT)—to facilitate cognitive change (Ehlers et al., 2021). In fact, the PTCI also includes a number of more global cognitions about the world that are difficult to be tested in the treatment of PTSD as they are lacking situational specificity (i.e., if–then contingency). Therefore, we sought to develop a measure comprising items with a high situational specificity, thus allowing an empirical test of the validity of patients’ predictions in a straightforward manner. More specifically than other existing instruments assessing posttraumatic cognitions, a new scale would thus allow to assess specific predictions of PTSD patients as highlighted recently by theories on the psychopathology of PTSD (Kube et al., 2020; Linson & Friston, 2019), which consider aberrations in the prediction of future events or experiences as a core feature of PTSD, inspired by neurophysiological evidence (Kimble et al., 2018). When considering a predictive processing perspective, predictions (that are in psychological terms expectations) shape the way how we perceive experiences and thus exert a strong influence on the symptom course. As expectation violation—the discrepancy between patients’ expectations and actual situational outcomes—has been proposed as a crucial treatment process (Craske et al., 2014), it should be a clinical aim to modify dysfunctional expectations. To assist in achieving this goal, a scale with a variety of predictions that can be used for expectation-violating interventions (e.g., exposure, behavioral experiments) is thus also of high practical utility. When aiming to assess relevant types of expectations in PTSD, one may consider symptom-specific expectations referring to the memory of the traumatic event (e.g., “When I am reminded of the traumatic event, I will feel like being at the mercy of these memories.”) and the intense emotions related to the trauma (e.g., “When I experience unpleasant emotions such as fear or guilt, I will feel helpless coping with these emotions.”). Because studies showed that such disorder-specific expectations contribute incrementally to the development of depressive symptoms beyond other types of cognitions (Kube et al., 2019; Kube et al., 2018), we believe that it might be valuable to examine them in PTSD as well. Besides disorder-specific expectations, it might also be worthwhile to consider patients’ treatment expectations (e.g., “If I confront myself with the traumatic event during therapy, I will feel much better in the longer run.”), as studies showed that such outcome expectations predict treatment response for combat veterans suffering from PTSD (Price et al., 2015). However, treatment-specific expectations have not been integrated in other scales so far.
Accordingly, the present study sought to develop a new self-report questionnaire that allows examining both disorder-specific expectations in PTSD and expectations that might be relevant to cognitive-behavioral treatments of PTSD. To this end, we examined a clinical sample of individuals that are treated for their PTSD symptoms, and we aimed to evaluate the psychometric properties of our new scale, the “Posttraumatic Expectations Scale” (PTES). In addition to internal consistency as one reliability aspect, we particularly aimed to assess the incremental validity of our scale by examining whether it is able to predict PTSD symptom severity above the well-established PTCI. Moreover, we aimed to build a short version of the scale to facilitate its use in clinical practice.
Methods
The local ethics committee of the Faculty of Psychology at the Philipps-University of Marburg approved this study (reference number 2018-6k). This study was conducted in accordance with the ethical standards as laid down in the Declaration of Helsinki (1964) and its later amendments.
Patients and Procedure
Data collection took place from May 2018 to July 2019. Participation in this study was voluntary and no financial benefit was offered. Before inclusion in this study, all patients gave their informed consent. To be included, patients had to have the primary diagnosis of PTSD according to International Classification of Diseases–tenth edition (ICD-10), as verified by structured clinical interviews. Also, patients had to be at least 18 years old and fluent in German. Patients were recruited in several local out- and inpatient clinics in the surrounding of the study site. The patients were enrolled for a trauma-focused CBT based on national and international guidelines of psychotherapy for PTSD (National Institute for Clinical Excellence, 2005; Schäfer et al., 2019). In both out- and inpatient settings, patients were enrolled after the diagnosis of PTSD was confirmed, but before treatment began. In addition to the Impact-of-Event-Scale—Revised (IES-R), a trained therapist (i.e., usually a clinical psychologist) assured the reliability of the diagnosis of PTSD using structured clinical interviews. Because some of the expectations assessed in our scale relate to the anticipation of specific aspects of the therapy, it was crucial to complete them prior to the actual therapy. A total of 70 PTSD patients participated in this paper–pencil study. All measures were administered in German.
Measures
Scale Development and Procedure: PTES
First, we did an extensive literature review of dysfunctional cognitions and expectations in PTSD. In doing so, we particularly focused on research on the cognitive model of PTSD (Ehlers & Clark, 2000) and the cognitive processing theory (Resick & Schnicke, 1992) to get a sense of what might be relevant domains where individuals with PTSD hold dysfunctional expectations. Second, we consulted various experts in the field of PTSD research and who frequently work with PTSD patients and asked them for domains of dysfunctional expectations that, in their experience, are core to PTSD. As a result, we defined the following domains for item development: general treatment expectations (subscale A; e.g., “In psychotherapy I will feel supported.”), exposure to the traumatic event during psychotherapy (subscale B; e.g., “If I face the traumatic event in psychotherapy, I will lose control.”), talking about the traumatic event in psychotherapy (subscale C; e.g., “If I tell my psychotherapist about the traumatic event, she or he will blame me for it.”), reexperiencing symptoms (subscale D; e.g., “When I am reminded of the traumatic event, I will feel helpless.”), emotion regulation (subscale E; e.g., “When I experience unpleasant feelings (e.g., blame, anger, sadness, disgust . . .) in relation to the traumatic experience outside of the psychotherapy, there will be nothing I can do to feel better.”), openness to other people (subscale F; e.g., “When I confide in other people (e.g., significant others), they will misuse my trust.”), encounters with strangers (subscale G; e.g., “If I meet strangers, I will be able to make new acquaintances” [inversely scored]), and avoidance behavior (subscale H; e.g., “If I stop avoiding certain things that remind me of the traumatic experience(s) (e.g., places, activities, people), I will reexperience a traumatic event.”). While we developed the first three subscales (i.e., subscales A-C) to refer to expectations regarding the psychological treatment of PTSD, the development of the subscales D-H focused on assessing expectations that relate to various disorder-specific aspects. In terms of domain sampling (Nunnally, 1978), we used these nine categories to derive specific items that were formulated in accordance with the existing expectation literature and theories (Rief et al., 2015; Rief & Glombiewski, 2017); that is, we paid particular attention to the fact that every single item is put in a testable, future-directed manner to enhance falsifiability by the individual. Specifically, when developing each item, we carefully thought about whether it would allow an empirical test of the respective expectation in a behavioral experiment. Furthermore, we used an additional ninth category named “general disorder-specific expectations” (subscale I), where we aimed to assess additional expectations that we considered important but could not clearly be linked to one the aforementioned domains (e.g., “I will be able to live a happy life, despite the traumatic experience I had.”).
After generating the initial item pool, we administered the scale to one PTSD patient who provided feedback on the relevance and comprehensiveness of the items. Based on this feedback, there was an additional review and revision of the items before we administered the 81-item self-report version of the PTES described here in the actual study. The items are rated on a 5-point Likert-type-like scale 2 ranging from 1 (“I don’t agree at all”) to 5 (“I totally agree”). Lower sum scores indicate fewer dysfunctional expectations. As we aimed to balance negative expectations with positive expectations, about half of the items need to be inversely scored. All 81 items of the German version of the PTES are presented in Appendix.
Originally, the scale was developed in German, as the questionnaire was planned to be administered in German in the present validation study; for this article, we translated the scale into English. A research assistant in our lab (German master student with English skills at native level), who was not involved in the item pool generation, translated the German version into English. Subsequently, another person with English skills at native level back-translated and proofread this version, to assure content-related consistency. Readers who are interested in the translated version of this measure that has not been studied empirically can contact directly the corresponding author. However, researchers should be aware that the validation of the German version does not extend to the English version.
Dysfunctional Cognitions in PTSD: PTCI
The PTCI is a 33-item self-report questionnaire measuring maladaptive cognitions in relation to a traumatic event and/or its consequences (Dunmore et al., 1999; Ehlers, 1999). Participants are asked to rate their agreement with the statements on a 7-point Likert-type-like scale ranging from 1 (“totally disagree”) to 7 (“totally agree”). The PTCI consists of three subscales: negative cognitions about the self, the world, and self-blame (Foa et al., 1999). Beyond its use in the original English version, Müller et al. (2010) also used and validated the PTCI in a German sample. Along with the original 33-item version of the PTCI, we used the Interpretation of PTSD Symptoms Inventory (IPSI; Dunmore et al., 1999) in this study. This scale consists of 11 items that measure the distress by intrusions, problems in remembering the traumatic event and the consequences of a traumatic event. Multiple studies showed that the PTCI and IPSI have a sound reliability (Foa et al., 1999; Halligan et al., 2003; Müller et al., 2010). In particular, the internal consistency estimates as indicated by Cronbach’s alpha range from very good (Müller et al., 2010) to excellent (Foa et al., 1999; Halligan et al., 2003), and, to examine the temporal stability, the test–retest reliability as indicated by Spearman’s rho range from satisfactory (Müller et al., 2010) to good (Foa et al., 1999) depending on the retest interval.
Symptom Severity: IES-R
We assessed the severity of PTSD symptoms with the German version of the IES-R. The IES-R is a 22-item self-report questionnaire measuring three areas of PTSD symptoms, namely, intrusion, avoidance, and hyperarousal (Maercker & Schützwohl, 1998). Patients suffering from PTSD are asked to rate the degree of distress of each item during the past week on a 4-point-Likert-type-like scale ranging from 0 (“not at all”) to 3 (“many times”). The IES-R showed a high internal consistency (Creamer et al., 2003) and good psychometric properties in a German adult sample of political prisoners in former East Germany and crime victims (Maercker & Schützwohl, 1998).
Other Measures
PHQ-9
Depressive symptoms were assessed with the German version of the Patient Health Questionnaire-9 (PHQ-9; Gräfe et al., 2004; Kroenke et al., 2001). Previous, extensive validation studies showed excellent psychometric properties for the PHQ-9 (e.g., Kroenke et al., 2010), also for the German version (Gräfe et al., 2004; Löwe et al., 2004). Moreover, a recent cross-cultural validation study of the PHQ-9 showed its favorable psychometric properties in a German sample without migration background and Turkish immigrants in Germany (Reich et al., 2018).
Socio-demographics
Socio-demographic questions were asked in a self-report questionnaire, including age, sex, education level, and marital status.
Statistical Analyses
All analyses were performed using the statistical processing language R (R Core Team, 2021). We used the R package psych (Revelle, 2021).
Preprocessing
In general, we performed data screening according to the recommendations of Tabachnick and Fidell (2013). We systematically inspected outliers, extreme values and missing values, and computed the squared Mahalanobis distance to determine multivariate outliers. This test indicated no significant outliers in our sample (Cohen et al., 1983; Stevens, 2009). To identify whether missing values were missing not at random (MNAR) or missing completely at random (MCAR), respectively, missing at random (MAR), we used the MCAR test (Little, 1988). The MCAR test showed no significant result, χ2 (5675, N = 70) < .0001 p = 1.00, indicating a MCAR distribution of missing values. Since 27% of cases had missing values, random forest imputation (RFI) as implemented in the missForest R package was used (Stekhoven & Buhlmann, 2012). RFI utilizes bootstrapped and aggregated decision trees to predict missing values. A maximum of 10 iterations and 1,000 separate trees were specified. We performed descriptive item and scale analyses and computed bivariate Pearson’s correlations between the scales and p-values. We corrected p-values according to the Holm method for multiple comparisons.
Reliability and Validity Analyses
We determined reliability by computing internal consistency indicated by Cronbach’s α. In addition to Cronbach’s α, McDonald’s ωh, McDonald’s ωt, and the average item correlation should be reported in case of five or more items per scale as recommended by Revelle and Condon (2019). Moreover, we report the average split-half reliability. To determine the incremental validity of the PTES, beyond the PTCI, we performed a multiple hierarchical regression analysis for the complete and the short scale, with symptom severity (IES-R) being the dependent variable. On a subscale level, due to the small sample size, we computed a cross-validated Lasso regression that sets regularized parameters to 0. The coefficients are standardized (beta) and all coefficients not set to 0 predict the respective scale.
Building a Criterion-Keyed Short Scale
We performed BISCUIT (best items scales that are cross-validated, unit-weighted, informative and transparent) analyses (Elleman et al., 2020). From a statistical point of view, BISCUIT builds scales of a predetermined number of items that show the strongest pairwise correlations with a certain criterion and cross-validates or bootstraps these scales. Then, we combined the cross-validated items showing the highest pairwise correlation with the criterion to a scale. For combination, we weighted all retained items equally (i.e., unit weighted). This way, we obtained a realistic estimate of out-of-sample generalizability as recommended by Cohen (1992). BISCUIT is particularly robust to high proportions of missing data and limitations in sample (Elleman et al., 2020). We validated the short scale derived from the complete PTES against the IES-R with an upper bound of a maximum of 15 items. In addition, we developed short scales for the subscales of the IES-R with an upper bound of a maximum of 30 items (10 items for each of the three subscales). We bootstrapped standard deviations of estimated validity coefficients using leave-one-out cross-validation (LOOCV), following the recommendations by Molinaro et al. (2005) and Sammut and Webb (2010).
Results
Patient Characteristics
Of all 70 PTSD patients, 82.6% were female with a mean age of M = 42.06 years (SD = 11.82). 45.7% had children, with a mean number of M = 2.22 (SD = 1.09) children per subject, and 32.9% were married while 30% were single. The educational level was relatively equally distributed; while 61.4% had completed an apprenticeship or vocational training, 1.4% had a higher vocational qualification (e.g., master craftsman), 11.4% had completed a university degree, 4.3% had another vocational training qualification, 20.0% had no vocational training.
The mean age of onset of PTSD was M = 23.70 years (SD = 15.45) with a mean of M = 17.96 years of manifestation (SD = 14.64). According to the Life-event Checklist for DSM-5 (LEC-5), patients reported on average to have experienced five traumatic events (M = 5.31; SD = 2.88), with sexual assaults being the most frequently reported trauma (54%). The average sum score of the IES-R was M = 79.24 (SD = 16.58), indicating that the sample was severely impaired on average (intrusion subscale: M = 26.92 (SD = 6.72); avoidance subscale: M = 24.17 (SD = 7.59); hyperarousal subscale: M = 28.11 (SD = 6.68). The average sum score of the PTCI was M = 155.58 (SD = 35.05) and the mean value of the IPSI was M = 4.03 (SD = 1.34), both speaking to presence of highly dysfunctional cognitions as compared to other PTSD samples (Ehlers, 1999; Müller et al., 2010). In line with these clinical characteristics of the current sample, the mean PHQ-9 sum score was M = 20.70 (SD = 5.52), indicating severe comorbid depressive symptoms. Table 1 portrays the relevant socio-demographic and clinical characteristics of the sample.
Socio-demographic and Clinical Sample Characteristics.
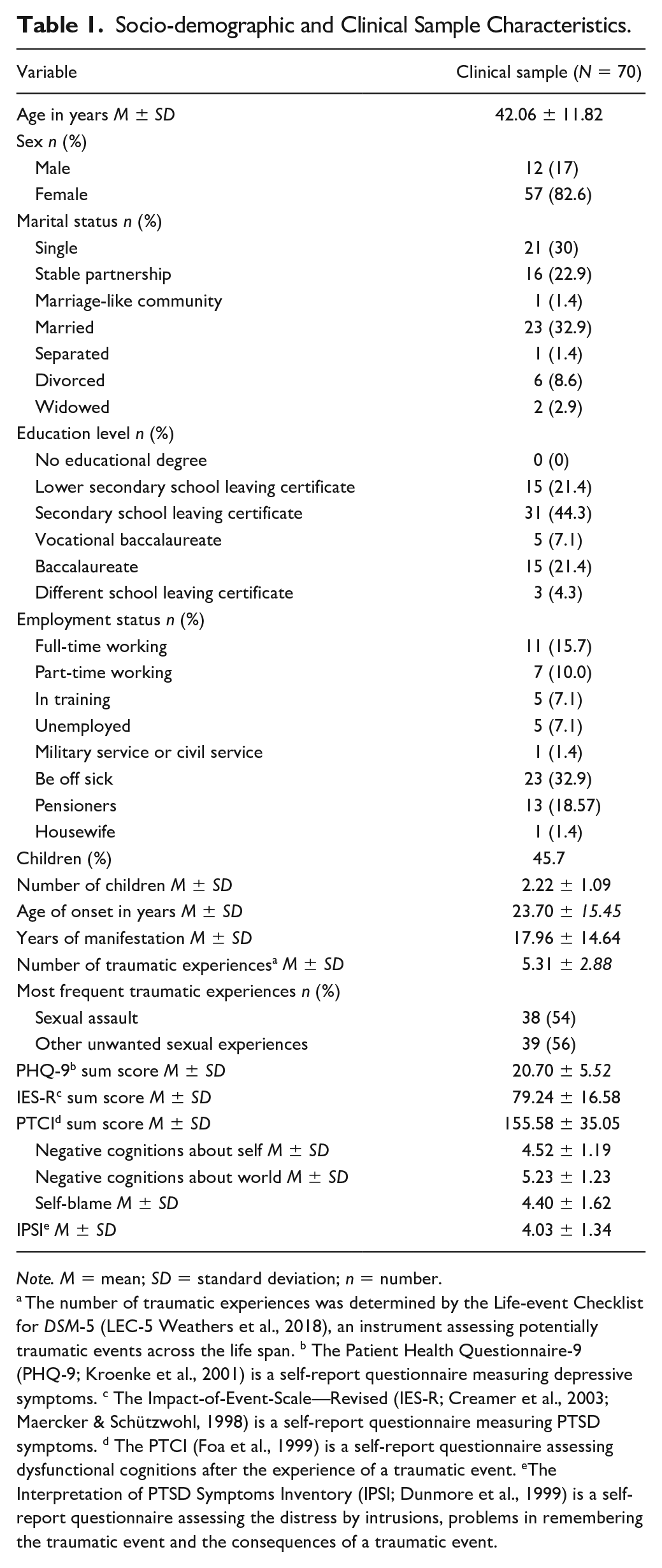
Note. M = mean; SD = standard deviation; n = number.
The number of traumatic experiences was determined by the Life-event Checklist for DSM-5 (LEC-5 Weathers et al., 2018), an instrument assessing potentially traumatic events across the life span. b The Patient Health Questionnaire-9 (PHQ-9; Kroenke et al., 2001) is a self-report questionnaire measuring depressive symptoms. c The Impact-of-Event-Scale—Revised (IES-R; Creamer et al., 2003; Maercker & Schützwohl, 1998) is a self-report questionnaire measuring PTSD symptoms. d The PTCI (Foa et al., 1999) is a self-report questionnaire assessing dysfunctional cognitions after the experience of a traumatic event. eThe Interpretation of PTSD Symptoms Inventory (IPSI; Dunmore et al., 1999) is a self-report questionnaire assessing the distress by intrusions, problems in remembering the traumatic event and the consequences of a traumatic event.
Scale analyses, Construct Validity, and Internal Consistency of the PTES
The items statistics of the PTES and the descriptive statistics of all subscales are depicted in Tables 2 and 3.
Item Statistics (Mean and Standard Deviation) of the PTES Items.
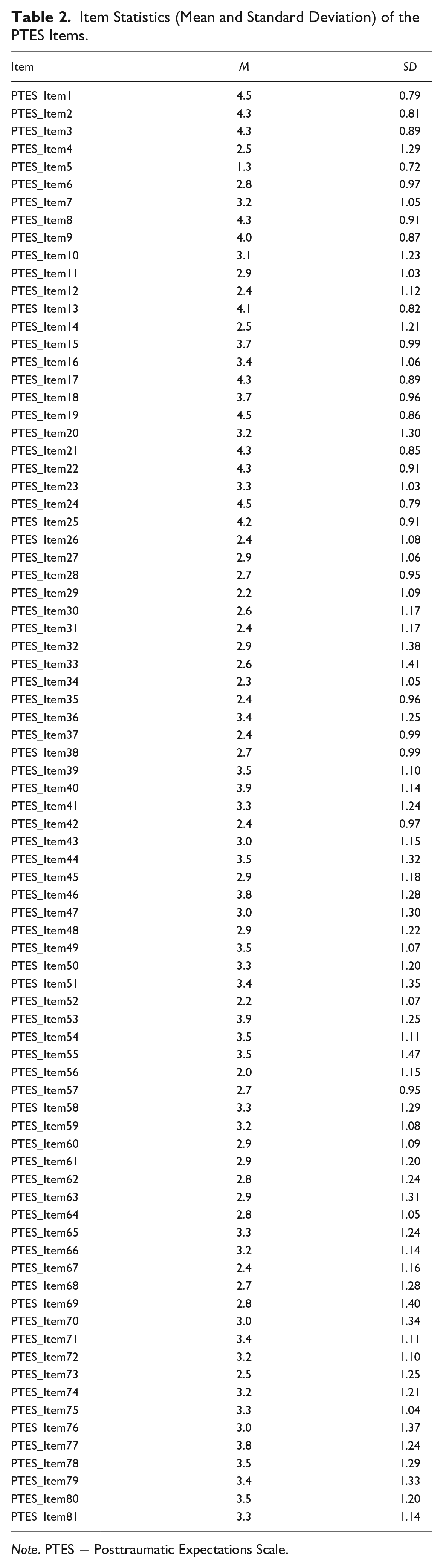
Note. PTES = Posttraumatic Expectations Scale.
Descriptive Statistics of All Scales.
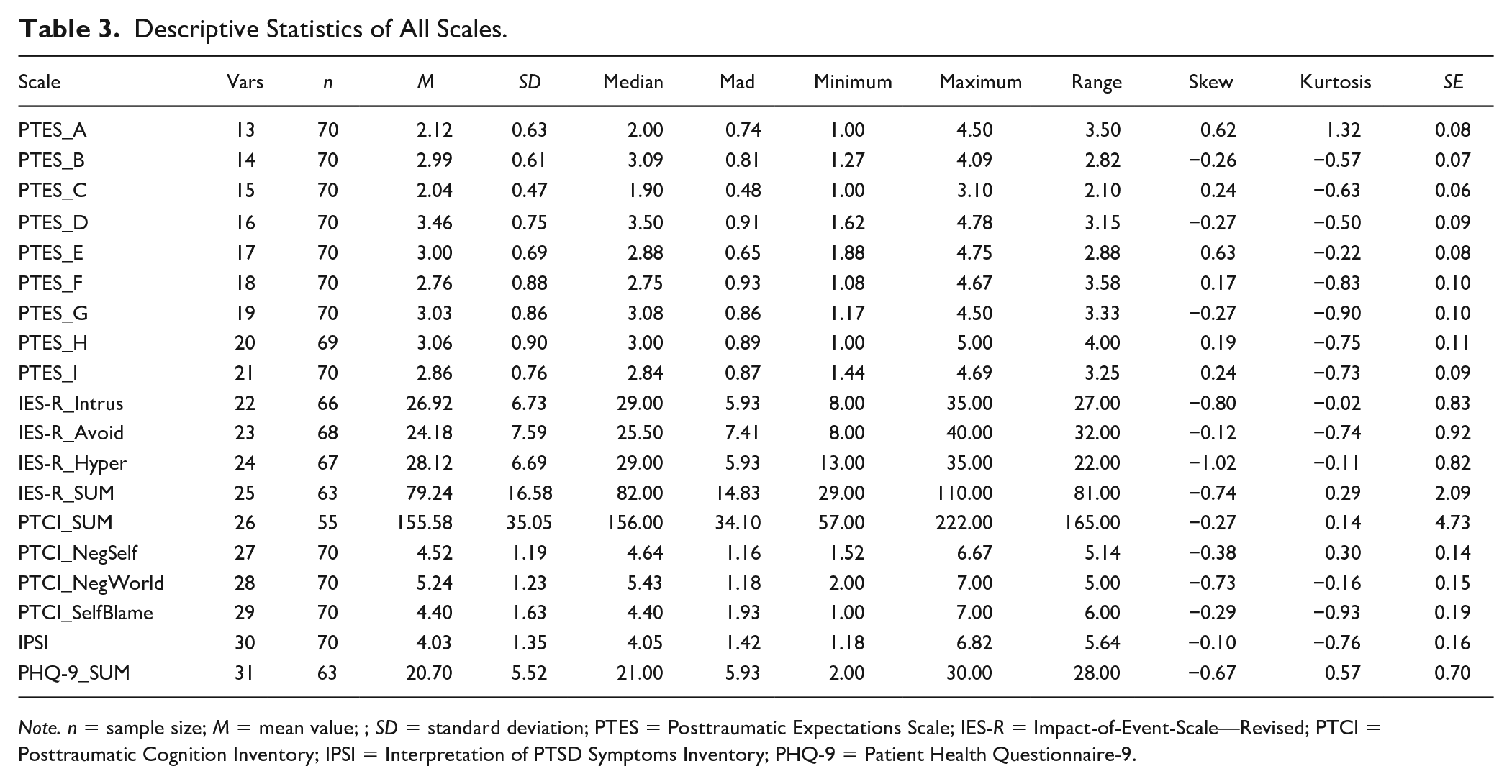
Note. n = sample size; M = mean value; ; SD = standard deviation; PTES = Posttraumatic Expectations Scale; IES-R = Impact-of-Event-Scale—Revised; PTCI = Posttraumatic Cognition Inventory; IPSI = Interpretation of PTSD Symptoms Inventory; PHQ-9 = Patient Health Questionnaire-9.
For the entire PTES and the respective subscales, the reliabilities are displayed in Table 4, along with the inter-correlations of all scales used in the present study.
Results of the Correlational Analyses Between All Scales and Its Reliabilities (N = 70).
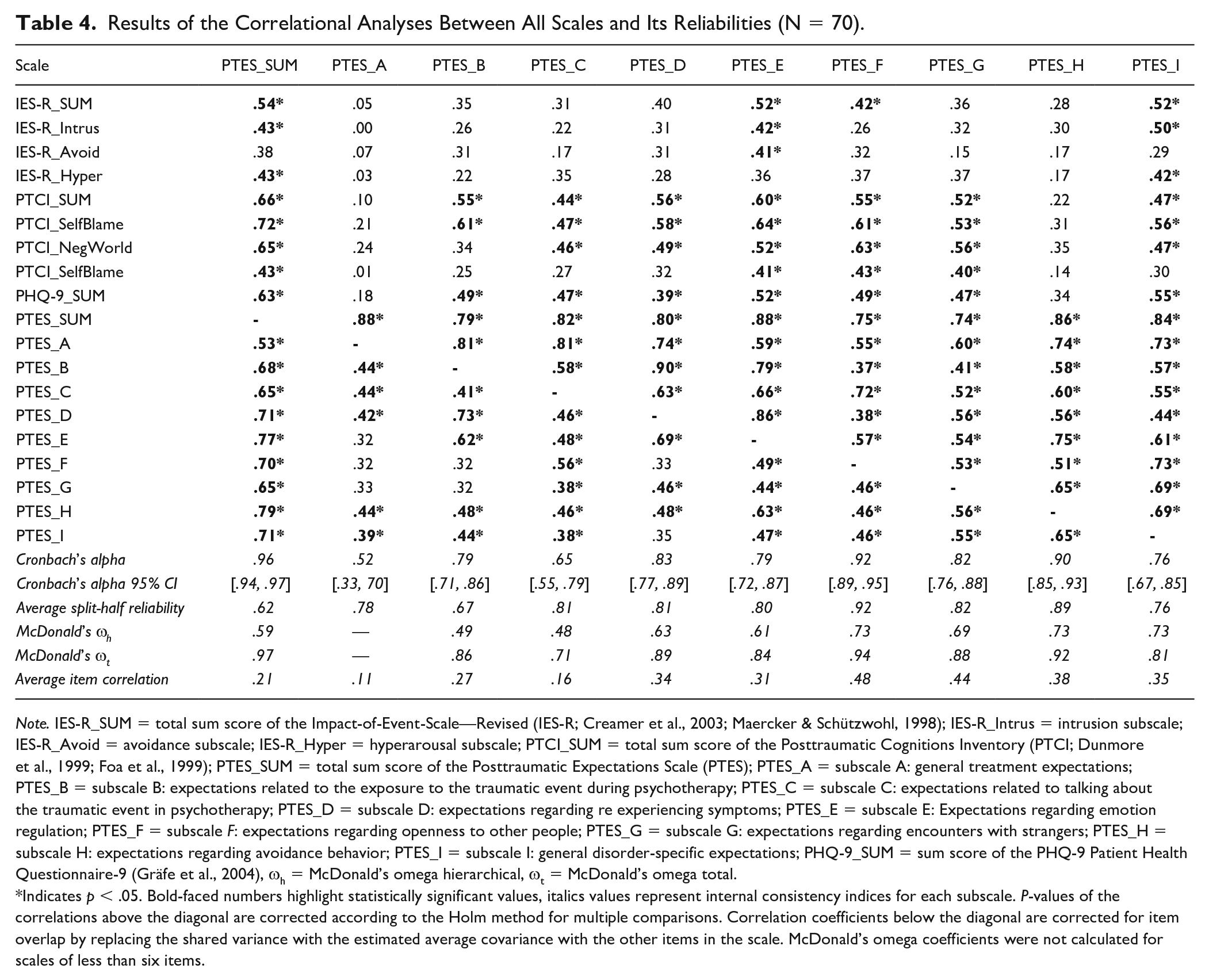
Note. IES-R_SUM = total sum score of the Impact-of-Event-Scale—Revised (IES-R; Creamer et al., 2003; Maercker & Schützwohl, 1998); IES-R_Intrus = intrusion subscale; IES-R_Avoid = avoidance subscale; IES-R_Hyper = hyperarousal subscale; PTCI_SUM = total sum score of the Posttraumatic Cognitions Inventory (PTCI; Dunmore et al., 1999; Foa et al., 1999); PTES_SUM = total sum score of the Posttraumatic Expectations Scale (PTES); PTES_A = subscale A: general treatment expectations; PTES_B = subscale B: expectations related to the exposure to the traumatic event during psychotherapy; PTES_C = subscale C: expectations related to talking about the traumatic event in psychotherapy; PTES_D = subscale D: expectations regarding re experiencing symptoms; PTES_E = subscale E: Expectations regarding emotion regulation; PTES_F = subscale F: expectations regarding openness to other people; PTES_G = subscale G: expectations regarding encounters with strangers; PTES_H = subscale H: expectations regarding avoidance behavior; PTES_I = subscale I: general disorder-specific expectations; PHQ-9_SUM = sum score of the PHQ-9 Patient Health Questionnaire-9 (Gräfe et al., 2004), ωh = McDonald’s omega hierarchical, ωt = McDonald’s omega total.
Indicates p < .05. Bold-faced numbers highlight statistically significant values, italics values represent internal consistency indices for each subscale. P-values of the correlations above the diagonal are corrected according to the Holm method for multiple comparisons. Correlation coefficients below the diagonal are corrected for item overlap by replacing the shared variance with the estimated average covariance with the other items in the scale. McDonald’s omega coefficients were not calculated for scales of less than six items.
Correlational analyses showed that the sum score of the PTES was significantly correlated with all other scales used in the present study. Specifically, the correlation of the PTES with the PTCI was r = .66; its correlation with the IES-R was r = .54; and the correlation with the PHQ-9 was r = .63. The PTCI was also significantly correlated with the IES-R (r = .57) and the PHQ-9 (r = .60), with similar correlation coefficients as the PTES.
The internal consistency of the total scale was high as indicated by α = .96 (95% CI [.94, .97]). The internal consistency of the PTES subscales ranged between α = .52 (95% CI [.34, .70]) for the scale A, assessing general treatment expectations, and α = .92 (95% CI [.89, .95]) for the scale F, assessing openness to other people. Among all subscales, only two subscales did not reach the critical value of α = .70 as an acceptable internal consistency for newly developed scales as proposed by DeVellis (2012); namely, subscale A (general treatment expectations) and subscale C (talking about the traumatic event in therapy). In line with Cronbach’s α, the values for McDonald’s ωt were also high (ωt = .97 for the total PTES with ωt = .71 lowest for the PTES subscale C and ωt = .94 highest for the PTES subscale F). Interestingly, the values for McDonald’s ωh draw a more distinct picture of the reliability and give interesting insights about the saturation of a possibly multidimensional scale with a “general factor”: for example, although we expected that the value for the total PTES would not have been quite so high, as we assumed that the scale is not unidimensional, it seems to be useful to compute a sum score as 59% of the variance could be explained by a “general factor.” Otherwise, the low values of the PTES subscales B and C seem to be critical and multidimensional determined, although we assumed them to be unidimensional. Thus, these scales must be cautiously interpreted. When grouping subscales from a theoretical point of view together, however, the internal consistency estimates for the treatment-specific expectation scale (subscales A–C) are: Cronbach’s α = .82 (95% CI [.76, .88]), McDonald’s ωh = .36, McDonald’s ωt = .86, and the average item correlation r = .16. The internal consistency estimates for the disorder-specific expectation scale (subscales D–H) are: Cronbach’s α = .95 (95% CI [.93, .96]), McDonald’s ωh = .52, McDonald’s ωt = .96, and the average item correlation r = .26.
Incremental Validity Analyses
The results of the regression analyses revealed that the PTCI as the sole predictor explained 36.2% of the variance of the IES-R (Fit R² = .362; R² 95% CI [.20, .53]). When including the PTES sum score as an additional predictor, this model explained a total of 39.3% of the variance (Fit R² = .393; R² 95% CI [.22, .56]). The difference in the explained outcome variance of 3.1% (difference ΔR² = .031; 95% CI [.02, .05]) was significant; thus, the PTES had incremental value over the PTCI. When examining the predictive value of the subscales of the PTES, the results indicated a distinct predictor profile as displayed in Table 5. In both prediction models (IES-R and PHQ-9), the PTCI was the strongest predictor, additionally some PTES subscales were important predictors; for example, the subscale A (general treatment expectations) (β = –.052), subscale E (emotion regulation) (β = .117) and subscale I (general disorder-specific expectations) (β = .211). When considering the subscales of the PTCI in the prediction models as recently suggested (Whiteman et al., 2020), the results remained essentially the same (see Supplemental Material 1).
Lasso Regression Results.
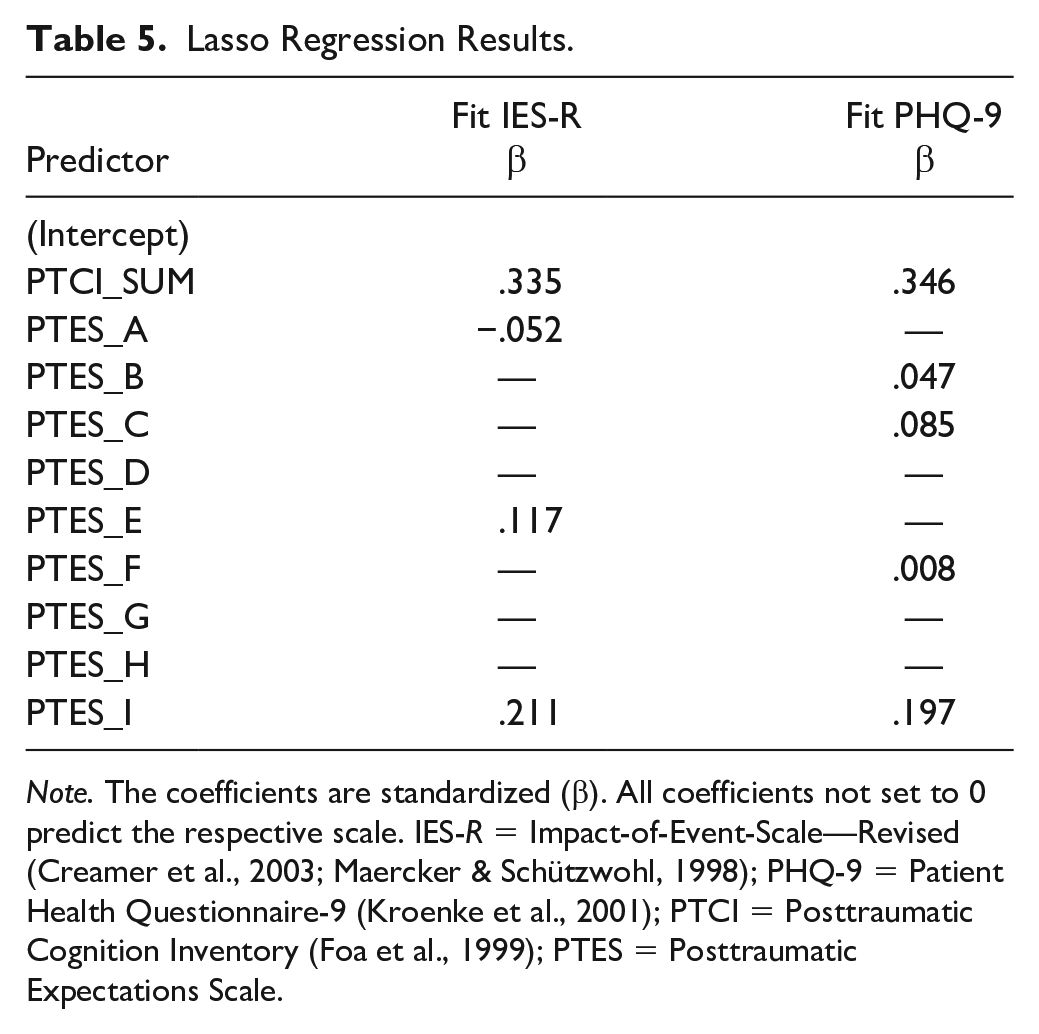
Note. The coefficients are standardized (β). All coefficients not set to 0 predict the respective scale. IES-R = Impact-of-Event-Scale—Revised (Creamer et al., 2003; Maercker & Schützwohl, 1998); PHQ-9 = Patient Health Questionnaire-9 (Kroenke et al., 2001); PTCI = Posttraumatic Cognition Inventory (Foa et al., 1999); PTES = Posttraumatic Expectations Scale.
Building a Short Scale
The BISCUIT method extracted 13 PTES items when validated on the IES-R sum score as the criterion building a 13-items ultra-short scale. We tested the incremental validity over the PTCI total score in a similar way as for the full PTES. When including the PTES sum score as an additional predictor, this model explained a total of 50.6% of the variance (Fit R² = .506; R² 95% CI [.36, .66]). The difference in the explained outcome variance of 14.5% (difference ΔR2 = .145; 95% CI [.12, .16]) was significant, indicating that the ultra-short PTES shows incremental validity. The internal consistency estimates for the ultra-short scale are: Cronbach’s α = .87 (95% CI [.82, .91]), McDonald’s ωh = .65 and McDonald’s ωt = .89. Separately, the BISCUIT method extracted a different number of PTES items when validated on each of the three IES-R subscales (i.e., intrusion: seven items, avoidance: eight items, hyperarousal: seven items) as criteria leading together to a 22-item short scale. These items are displayed in Table 6. Using the IES-R sum score as the criterion, the best symptom-specific items seemed to be Item 48, Item 78, Item 71, Item 58, Item 40, Item 70, Item 77, Item 39, Item 81, Item 5, Item 32, Item 72, and Item 43. These items are part of the 13-item ultra-short scale that yields a more favorable validity. When applying the IES-R subscales as criteria, BISCUIT selected more general expectations as predictors for the intrusion subscale and the hyperarousal subscale, whereas this method selected expectations regarding negative emotions caused by the traumatic event (scale E) and expectations regarding openness to other people (scale F) as predictors for the avoidance subscale in particular. As the subscales are interrelated, this procedure selected some items repeatedly leading to less favorable validity results.
Results of the BISCUIT Analysis for Both the Short Scale of the Total Score and the Short Scales of the Sub Scores of the IES-R.
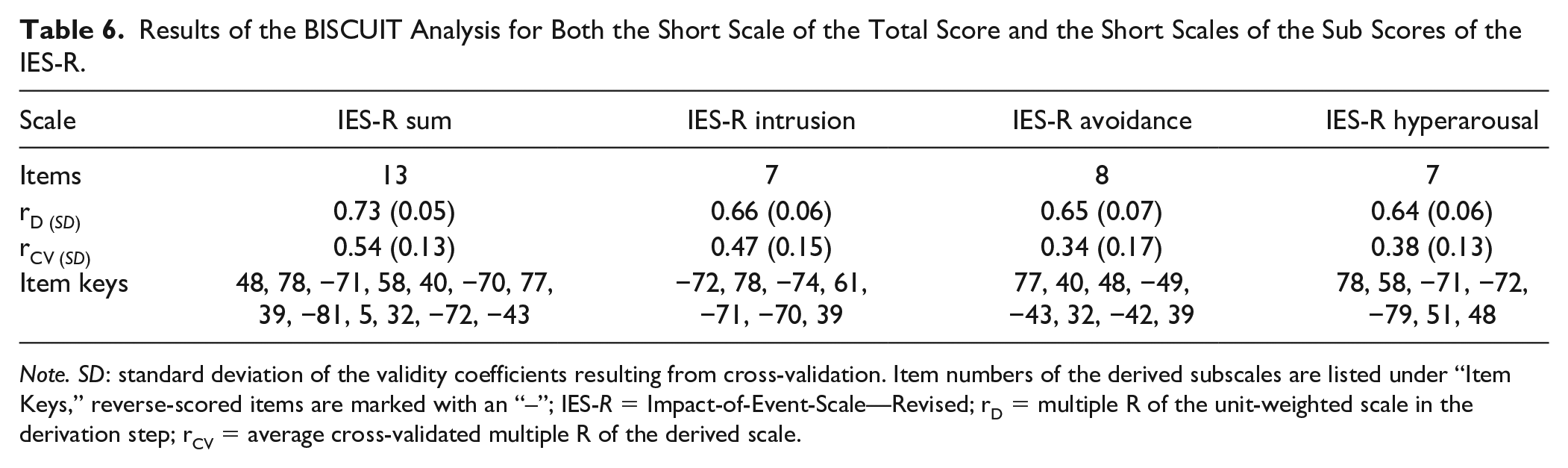
Note. SD: standard deviation of the validity coefficients resulting from cross-validation. Item numbers of the derived subscales are listed under “Item Keys,” reverse-scored items are marked with an “–”; IES-R = Impact-of-Event-Scale—Revised; rD = multiple R of the unit-weighted scale in the derivation step; rCV = average cross-validated multiple R of the derived scale.
Discussion
In this study, we developed the PTES in an iterative and theory-driven process to assess both disorder-specific expectations and treatment expectations in a clinical sample of patients with PTSD. The results of the reliability and validity analyses showed that the PTES is a measure with high internal consistency and its validity appears promising. More specifically, the results of this validation study showed excellent internal consistency of the entire scale and most of the subscales. Moreover, in cross-sectional analyses, the PTES showed significant correlations with the well-established PTCI, as a measure for more general dysfunctional cognitions, as well as the severity of PTSD symptoms, speaking to the concurrent validity of the PTES. With respect to its incremental validity, the results of the regression analyses revealed that the PTES incrementally explained variance of the severity of PTSD symptoms over the PTCI, suggesting that the PTES might be a useful addition to the PTCI. To enhance the applicability for researchers and practitioners, the present study used a state-of-the-art approach (Elleman et al., 2020) to construct short scales that are as valid as possible and also can easily be administered in clinical research and practice, with 13 items for the total symptom-specific criterion and a total of 22 items when using each of the symptom-specific criteria separately (i.e., intrusion: seven items, avoidance: eight items, hyperarousal: seven items). Due to the small sample, we aimed to ensure that our results were nevertheless as robust and generalizable as possible. For BISCUIT, research has shown that it still makes accurate and parsimonious item selections even in small samples with a high rate of missing data (Elleman et al., 2020). The ultra-short scale validated on the full IES-R scale has foremost a practical value as it could be used as a quick screening instrument for dysfunctional expectations in PTSD patients to provide more information on target processes in PTSD treatment. The scales that have been validated on the IES-R subscales allow a more mechanistic understanding (e.g., what specific expectations play a differential role in intrusions as the PTSD hallmark symptom) that might lead to different expectation-violating interventions. Important to highlight, these scales also could be used in research to investigate mechanisms of action where a more accurate presentation is important. However, as this study only provides first evidence in a small sample, we encourage researchers to use the full version—also to replicate our short scales. Collectively, the results of the reliability and validity analyses suggest that the PTES might be a useful tool to assess several types of dysfunctional expectations in PTSD patients reliably. Notwithstanding these promising findings, the preliminary results of our validation study should be interpreted in the light of requiring separate translation and psychometric testing in languages other than German prior to using the measure in those samples. A translation of the PTES into English can be provided by the corresponding author. Before using these scales in clinical practice outside Germany, however, they should be validated in English as well.
Theoretical Implications
While PTSD research thoroughly studied general cognitions, such as negative appraisals of the traumatic event and its consequences (Dunmore et al., 1999; Ehring et al., 2008; Halligan et al., 2003; Kleim et al., 2013; ter Heide et al., 2017; Woud et al., 2019), the present study is the first to systematically focus on expectations as a particularly important subset of cognitions. We acknowledge that there are other existing questionnaires that assess different types of cognitions related to PTSD, such as the PTCI and the PMBS (Vogt et al., 2012). Yet, these existing questionnaires are based on a conception of “cognition” that has recently been criticized as possibly being too broad and unspecific (Rief et al., 2015; Rief & Joormann, 2019). In contrast to these existing measures, the PTES focuses solely on expectations relevant to PTSD, representing the subgroup of cognitions that refer to future events and experiences. The results of this study showed that expectations (as measured by the PTES) indeed explained incremental variance of symptoms of PTSD beyond general cognitions (as measured by the PTCI); therefore, the PTES seems to have value in shifting the focus to patients’ expectations, for example, expectations resulting from core features of the disorder (such as expectations about perceived threat) and expectations concerning psychological treatment. Thus, the present findings might have the potential to extend the cognitive model of PTSD (Ehlers & Clark, 2000) by differentiating between different types of cognitions and therefore refining the association between negative appraisals of the trauma and/or its sequelae and the experience as a current threat (intrusions, arousal symptoms, strong emotions) within the cognitive model. In particular, expectations as assessed with our newly developed scale reflect a person’s prediction of future events and experiences. Recent advances in cognitive neuroscience suggest people’s predictions significantly affect their perception; in other words, people interpret new information in light of their prior predictions (Bastos et al., 2012; Friston, 2009; Kanai et al., 2015). Recent studies suggested that in people with PTSD, predictions are tied to the anticipation of threat (due to the [life-]threatening nature of the traumatic event) that lead to the perception of the world as being insecure and dangerous (Kube et al., 2020; Linson & Friston, 2019). Consistent with these theories from computational psychiatry, the systematic assessment of people’s predictions illustrates the merit of the PTES. Consequently, this might offer insights into how—and why—people with PTSD perceive their world. Drawing on our approach, future research may aim to investigate how patients’ expectations in various domains predict the course of PTSD symptoms in longitudinal designs.
Clinical Implications
Although meta-analyses and systematic reviews of randomized-controlled trials (RCTs; Bisson et al., 2007; Cusack et al., 2016; Ehlers et al., 2010) and practice-based studies (Herzog et al., 2022) indicate the general efficacy of psychotherapy (especially individual trauma-focused CBT in PTSD patients with moderate to large effect sizes across various settings, non-response rates and dropout rates are relatively high (Bradley et al., 2005; Schottenbauer et al., 2008). Therefore, there is space for optimizing the effects of psychotherapy in the treatment of PTSD. Since empirical hypothesis-testing is the backbone of CBT for PTSD in general, and of CT-PTSD (Ehlers, 1999; Ehlers & Clark, 2000) and CPT (Resick & Schnicke, 1992) in particular, the PTES might have the potential to facilitate this approach by allowing a structured assessment of patients’ expectations that can subsequently be tested in interventions such as behavioral experiments. Indeed, changes in posttraumatic cognitions predict changes in CT (Kleim et al., 2013) and CPT (Schumm et al., 2015) for PTSD. Drawing on the work by Kleim et al. (2013) and Schumm et al. (2015), the special focus on dysfunctional expectations in patients with PTSD might offer several advantages for practitioners: Knowledge about situation-specific expectations might be useful in designing effective interventions such as behavioral experiments. When considering dysfunctional expectations instead of more general cognitions, the empirical testing of hypotheses may be more straightforward, for example, dysfunctional beliefs might be easier disconfirmed by new information as gained in a behavioral experiment. From a practical point of view, given that therapist and patient can agree on situation-specific conditions mentioned by the respective item, expectation violation as an important mechanism of change (Craske et al., 2014) could be incorporated more directly and thus facilitated in the treatment of PTSD by the clinically useful items of the PTES. To maximize expectation violation with the help of the PTES, therapists could choose those expectations that the patient endorses most strongly and put effort into creating specific interventions that lead to maximal change in these expectations. This expectation-focused approach might facilitate cognitive restructuring within CBT for PTSD as the experience gained in the specific intervention can be used to modify a person’s global belief of the world or self on a higher-order level (as measured by the PTCI).
To illustrate this argument, we discuss below some examples of how PTES might be used to optimize psychotherapy by the use of behavioral experiments in PTSD. For instance, the dysfunctional expectation as assessed with the PTES, “When I confide in other people (e.g., significant others), they will misuse my trust.,” might be easier to test in behavioral experiment than the more global cognition, “People can’t be trusted,” as assessed with the PTCI. We believe so because the latter is hard to evaluate empirically, whereas the former can be examined in a relatively straight forward manner: The therapist may encourage the patient to talk to a significant other (e.g., a member of the family) and observe whether the other person takes advantage of that situation. Obviously, to be an effective intervention, the therapist and the patient in this example would also have to discuss what “misuse” or “take advantage” could mean exactly, and under which circumstances the behavioral experiment would—in the patients’ perspective—reveal useful and trustworthy information, such that the patient would use it to revise the initial expectation. To give another example, the PTES might also allow an easier disconfirmation of avoidance-related expectations. For instance, while the expectation, “If I stop avoiding certain things that remind me of the traumatic experience(s) (e.g., places, activities, people), I will reexperience a traumatic event.” might be easier to test in behavioral experiment or an exposure session (e.g., by exposure the patient to triggering cues) than the more global cognition, “The world is a dangerous place” from the PTCI.
A structured assessment of patients’ individual dysfunctional expectations with the PTES might help optimizing case conceptualization and, accordingly, developing a treatment plan, at an early treatment stage and targeting these expectations subsequently. Furthermore, patients might complete the PTES repeatedly throughout the therapy to allow an examination of whether the interventions to modify patients’ expectations were actually effective. As an additional advantage, addressing expectation violation through the use of idiosyncratic behavioral experiments could be promising in remotely delivered treatments which recently gained attention in times of Covid-19 and its related challenges in delivering evidence-based practice (Murray & El-Leithy, 2020).
Limitations and Future Research Directions
This study serves as a preliminary validation of the PTES as a newly developed questionnaire assessing dysfunctional expectations of PTSD patients. By interpreting the results of this study, the following limitations must be taken into account:
The major limitation is the sample size, which is closely related to larger confidence intervals and thus a lack of confidence in the estimated effects. Taking this critical aspect into account, we quantified the stability of the effects by applying LOOCV, a procedure that experts have recommended particularly for small sample sizes (Molinaro et al., 2005). Although we presented a subscale structure of the PTES in the introduction (namely, treatment-related expectations and symptom-specific expectations), we were not able to determine if these scales represent distinct underlying constructs as we could not use factor analytic strategies due to sample size. As another substantial limitation, this study used a cross-sectional design and therefore does not allow any conclusions about causality. The cross-sectional nature of our study also limits the conclusions that can be drawn concerning the differential relation to other constructs. Considering this limitation, we could not investigate the test–retest reliability which is an essential next step in further validating this scale. Future studies could therefore incorporate a shortened version of the PTES in longitudinal studies (e.g., in RCTs) using larger samples, which would offer several advantages: first, it can provide information on the causal pathways between expectations change and its relation to symptom severity throughout treatment; second, it can be used to determine test–retest-reliability; and third, it would allow more sophisticated statistical procedures to determine the factor validity (e.g., confirmatory factor analyses) providing stronger evidence for the underlying factor structure, the reliability and the differential relation to other constructs, such as symptom severity. Larger sample sizes could also be used to demonstrate, how much of the explained variance is attributable to a general factor and how much to subfacets, thus, indicating how many factors yield our PTES to determine our theory-driven assumptions. Moreover, criterion-related validity, discriminant validity (beyond PHQ-9), and variability over time/response to intervention could be investigated in future studies to achieve a more nuanced picture of the psychometric properties of the PTES.
Aside of statistical limitations caused by our sample size, idiosyncratic sample features (e.g., recruitment in inpatient and outpatient setting) may have created contextual limitations and impacted results insofar as the results of our study may not generalize to other populations. Particularly, a further drawback of this study is the characteristics of the sample: PTSD patients in the current sample reported relatively high impairment and severe symptoms as compared to previous studies using similar measures (Müller et al., 2010). At least in part, this might be due to the fact that the most frequent traumatic events were sexual assaults and other unwanted or unpleasant sexual experiences as well as other interpersonal traumas, whereas the experience of an accidental trauma was rarely reported. In fact, the experience of an interpersonal trauma caused more dysfunctional cognitions and greater symptom severity than an accidental trauma (Foa et al., 1999; Müller et al., 2010; Shakespeare-Finch & Armstrong, 2010; Startup et al., 2007). The type of trauma exposure might limit generalizability, and thus, the validity results may not be applicable in samples with other types of trauma exposure (e.g., combat). Future studies could therefore focus on other types of trauma exposure to determine its impact on posttraumatic expectations. A further limitation is that we did not collect data on race/ethnicity, which could have been interesting given that PTSD is particularly prevalent among people with a history of migration (Nesterko et al., 2019).
Moreover, this study used only self-rating questionnaires for the assessment of PTSD-specific cognitions and expectations as well as PTSD symptom severity. Regarding the potential risk of common method bias, future studies on the PTES may additionally use an observer-rated instrument, such as the Clinician-Administered PTSD Scale for DSM-5 (CAPS-5; Weathers et al., 2018). In terms of the psychometric properties of the PTES, we note, that while the total scale and most of the subscales of the PTES were internally consistent and valid, the subscale A (i.e., treatment-specific expectations) had lower values of Cronbach’s alpha. Also, this subscale seemed to be relatively unrelated to the total scale; therefore, it might be considered to analyze this scale independent of the other subscales of the PTES. One might argue that the specific treatment provided may at least partly account for the low internal consistency for subscales A and C. However, when grouping treatment-specific expectations together (scales A–C), internal consistency was good (α = .82 (95% CI [.76, .88]), indicating a more homogeneous picture. This suggests that differences between the subscales, rather than differences in the treatment received, may account for some of the low internal inconsistencies when examining the subscales separately. Nevertheless, in view of the fluctuating estimates across different internal consistency indices of the subscales A–C in our sample, future studies should further examine if these subscales should be substantially revised or even dropped.
An additional limitation of the present study is that the English version of the PTES (available upon request) was not tested. The authors encourage other researchers to further validate the PTES in English-speaking countries as the data we used in our study were a German-speaking sample of PTSD patients.
Conclusion
In the present study, we used a sample of 70 patients with PTSD to develop the PTES as a new questionnaire assessing dysfunctional expectations in relation to PTSD. The results suggest that the PTES is a highly internally consistent assessment tool that incrementally explains variance of PTSD symptom severity, above and beyond the well-established PTCI. The PTES might have the potential to further improve cognitive-behavioral treatment of PTSD as it allows a structured assessment of various domains of dysfunctional expectations, which can be used as a starting point for cognitively oriented treatments (such as CPT) and provides a basis for interventions such as behavioral experiments (often used in CT-PTSD) or exposure-based interventions (as used in prolonged exposure therapy), with the aim of disconfirming patients’ expectations and facilitating their modification.
Supplemental Material
sj-docx-1-asm-10.1177_10731911221089038 – Supplemental material for Assessing Dysfunctional Expectations in Posttraumatic Stress Disorder: Development and Validation of the Posttraumatic Expectations Scale (PTES)
Supplemental material, sj-docx-1-asm-10.1177_10731911221089038 for Assessing Dysfunctional Expectations in Posttraumatic Stress Disorder: Development and Validation of the Posttraumatic Expectations Scale (PTES) by Philipp Herzog, Tim Kaiser, Winfried Rief, Eva-Lotta Brakemeier and Tobias Kube in Assessment
Footnotes
Appendix
Acknowledgements
The authors would especially like to thank Dr. Kerstin Kühl for her valuable feedback at generating the item pool, Anna-Lena Eckert for her support in translating the questionnaire into English, and all bachelor and master graduate students as well as practitioners (especially at the Schön Clinic, Parkland-Clinic, and the Outpatient Clinic Marburg) for their support in recruiting patients for our study.
Author Contributions
PH, ToKu, and ELB conceptualized the study. PH collected data and originally drafted and edited the manuscript, ToKu and ELB supervised, reviewed, and edited the manuscript, TiKa computed the statistical analyses, WR revisited the manuscript critically for important intellectual content, and gave substantial feedback for the conception and design of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.