
Abstract
Recently developed mindfulness scales have integrated aspects of the body in measuring mindfulness unlike other established scales. However, these scales focused solely on body awareness and did not embrace all aspects of mindfulness and the body. Specifically, they did not integrate embodiment in mindfulness. The proposed Embodied Mindfulness Questionnaire (EMQ) aims to operationalize the proposed notion of “embodied mindfulness” by grounding it into five dimensions, each representing a set of skills that can be cultivated through training and practice: (a) Detachment from Automatic Thinking, (b) Attention and Awareness of Feelings and Bodily Sensations, (c) Connection with the Body, (d) Awareness of the Mind-Body Connection, and (e) Acceptance of Feelings and Bodily Sensations. The EMQ items were developed through consultations with a panel of eight graduate students and a group of 10 experts in the field. Results from a series of three studies supported the proposed five subscales of EMQ and suggested that these subscales are independent and supported by convergent and discriminant evidence. In addition, results suggested that scores of EMQ subscales are different in terms of sensitivity to mindfulness training or meditation practice and experience. Limitations, as well as theoretical and practical implications of the EMQ subscales, are thoroughly discussed.
The interest in mindfulness as a concept continues to grow, as shown by the increase in the number of publications pertaining to mindfulness during the last four decades (Google Scholar, 2021). This increase is also a reflection of the fact that the term “mindfulness” is currently used as an umbrella for a variety of approaches that assign different meanings to the same word. Although differences among varying conceptualizations and definitions of “mindfulness” have been previously highlighted (see e.g., Hart et al., 2013), few efforts have attempted to reconcile or integrate these differing conceptual approaches. To address the current gap, we used the theory of embodiment as a common denominator among the various conceptualizations of “mindfulness.”
The theory of “embodiment” expresses the idea that knowledge and experience are grounded in bodily states and specifically in the brain’s modality-specific systems (Lakoff & Johnson, 1999; Niedenthal et al., 2005). Those systems include the sensory systems that underlie the perception of a current situation, the motor systems that underlie action, and the introspective systems that underlie conscious experiences of emotion, motivation, and cognitive operations. According to an embodied perspective on cognitions, physical body position and movement can change the way people think, the conclusions they draw, and the decisions they reach (Lakoff & Johnson, 1999; for a review see, Niedenthal et al., 2005).
In addition, several theories of emotion emphasize the idea of embodiment (see, for example, Damasio, 1994; Niedenthal, 2007; Niedenthal et al., 2005; Teasdale & Barnard, 1993). These theories propose a complex reciprocal relationship between the bodily expression of emotion and the way in which emotional information is processed in the body. Therefore, the conceptualization of embodiment encompasses a bidirectional link among cognition, emotions, behaviors, and bodily states. In line with this conceptualization, Varela et al. (1991) and Thompson & Varela (2001) proposed that consciousness itself is embodied, thus involving a two-way reciprocal relationship between the brain and the body. Furthermore, they suggest that consciousness is embedded in an environmental context. Consciousness, therefore, cuts across the brain–body–world divisions rather than being simply located in the head.
Based on the theory of embodiment, specifically from the work of Varela et al. (1991) and Thompson & Varela (2001), we introduced the notion of “embodied mindfulness” (Khoury et al., 2017, 2019). This new notion is grounded in neurobiology, namely in the integration of top-down and bottom-up processes (Taylor et al., 2010). According to this definition, “embodied mindfulness” is a skill/ability that includes elements of attention, awareness, and acceptance involving the mind, body, and mind-body associations. “Embodied mindfulness” comprises the following five dimensions, and each represents a set of skills that can be cultivated through training and practice: (a) Detachment from Automatic Thinking, (b) Attention and Awareness of Feelings and Bodily Sensations, (c) Connection with the Body, (d) Awareness of the Mind-Body (i.e., cognition-emotion) Connection, and (e) Acceptance (i.e., non-avoidance) of Feelings and Bodily Sensations. This definition shares common elements with previous, standard mindfulness definitions (e.g., Attention and Awareness of Feelings and Sensations), but extends it by integrating skills trained through mindfulness meditation practice (namely, Detachment from Automatic Thinking and Acceptance of Feelings and Bodily Sensations) and skills related to embodiment (namely, Connection with the Body and Awareness of the Mind-Body Connection). This definition, therefore, moves from a traditional trait (disposition)-based conceptualization of mindfulness that normally includes one or multiple dimensions that are supposed to be equally present or absent in an individual by theorizing “embodied mindfulness” as a set of embodied skills/abilities that can be trained sequentially (i.e., build on each other) throughout time using multiple and incremental behavioral practices. These skills might, therefore, require a different level of effort to cultivate. Although some might require less practice and be more sensitive to a low level of meditation practice or mindfulness training, others might require longer and more sustained training and practice. In the following, we present these skills (dimensions/subscales) starting with the more traditional ones (i.e., the one partially present in other mindfulness scales), which we hypothesize being easier to cultivate, and then we move toward the skills that are novel and related to embodiment, which we hypothesize may require longer and more sustained training and practice. In addition, the latter skills might build upon the previous ones in such way that the earlier skills may be prerequisites to develop the more advanced skills. Therefore, our conceptualization of the notion of “embodied mindfulness” may not yield to a singular global latent variable. This hypothesis will be tested through confirmatory factor analyses.
Detachment from Automatic Thinking
Many cognitive theorists have focused on the role mindfulness practices (namely, meditation) may play in controlled (i.e., intentional, deliberate, effortful, and conscious) versus automatic (i.e., habitual, non-deliberate, effortless, and non-conscious) thinking (see e.g., Breslin et al., 2002; Craske & Hazlett-Stevens, 2002; Teasdale et al., 2002; Wells, 2002). It has been suggested that the inability to inhibit automatic thinking is related to a constellation of emotional disorders, including excessive worry, anxiety, and depression (see e.g., Mathews & MacLeod, 2005). The notion of “embodied mindfulness” involves the ability to decenter, or detach, from automatic thoughts (i.e., thoughts that are not intentional or grounded in the body). Decentering (or detachment from automatic thoughts) is also emphasized as a mechanism of Mindfulness-Based Cognitive Therapy (MBCT; Segal et al., 2013), in which participants learn to view thoughts as events in the mind rather than necessarily being reflections of reality, accurate self-view, or indications of internal bodily states. Decentering emphasizes changing one’s relationship with one’s thoughts and adopting a more distanced perspective, rather than trying to alter the content or nature of the thoughts (Fresco, Moore, et al., 2007; Fresco, Segal, et al., 2007; Teasdale et al., 2002). In a randomized controlled trial (RCT), mindful breathing (a type of body-focused meditation) was related to a significant increase in decentering and decrease in automatic thinking, in comparison with progressive muscle relaxation (Feldman et al., 2010).
Many prominent authors in the field of mindfulness have pointed to the theoretical link between decentering and mindfulness (see, for example, Carmody et al., 2009). Kabat-Zinn (1994) suggested that mindfulness allows one to observe the workings of the mind moment-by-moment, to see thoughts as “just thoughts, and allow the thoughts to come and go without getting caught in the stories they relate.” Bishop (2002) defined mindfulness as “a state in which one is highly aware and focused on the reality of the present moment, accepting and acknowledging it, without getting caught up in thoughts that are about the situation or in emotional reactions to the situation” (p. 71). Kostanski and Hassed (2008), wrote, “living mindfully means being in the moment, connected with the senses, not caught up with mental chatter” (p. 17). In the same line of thought, Groves (2016) suggests that the practice of meditation involves “stepping out of being caught up in mental distractions, and returning back to the body” (p. 290). In summary, the ability to detach from (or inhibit) automatic thinking is the first building block of the notion of “embodied mindfulness” by unstrapping attentional mechanisms, allowing therefore for flexible attention that can be directed toward the body or external stimuli.
Attention and Awareness of Feelings and Bodily Sensations
Unstrapping the attention from the mind and its continuous stream of thoughts as taught in the first skill can allow directing attention to the body and awareness of bodily sensations in the present. In fact, body awareness can be defined as the dynamic and interactive process through which the body’s psychological states, processes, actions, and functions are perceived, at both interoceptive and proprioceptive levels (Mehling et al., 2009). Body awareness is a central element of all Mindfulness-Based Programs (MBPs) and the majority of meditation practices. In fact, analysis of clinical, behavioral, and neuroscientific findings strongly suggest that brain regions related to both interoceptive (e.g., insula) and exteroceptive (e.g., somatosensory cortex) body awareness are highly activated among meditators and individuals who participate in Mindfulness-Based Stress Reduction (MBSR) training, compared with waitlist controls or non-meditators (see e.g., Chiesa et al., 2013; Hölzel et al., 2011; Lutz et al., 2008). In addition, participating in MBCT increased body awareness, which was found to be a mediator of the positive effects of MBCT on depression severity (de Jong et al., 2016). Multiple studies have furthermore shown a link between increased body awareness and improved regulation of negative affect (Füstös et al., 2012), subjective well-being (Brani et al., 2014), empathic responses (Singer et al., 2004), and mindfulness (Cebolla et al., 2016). Body awareness is a core component in the notion of “embodied mindfulness,” as it is an integral part of the bidirectional mind-body link proposed by the theory of embodiment.
Connection With the Body
Most mindfulness meditation practices involve using the body as an anchor, and therefore require sustaining a connection with the body. In fact, most of the current Western MBPs, for example, MBSR (Kabat-Zinn, 1982, 1990), MBCT (Segal et al., 2013), Mindfulness-Based Relapse Prevention (MBRP, Bowen et al., 2009), and Mindfulness-Based Eating Awareness Training (MB-EAT, Kristeller et al., 2014; Kristeller & Hallett, 1999), emphasize sustaining attention and awareness of the body through different exercises (e.g., through body scans, walking/eating meditations, or gentle yoga stretching). The duration of maintaining the attention will vary among the practices as some such as mindful eating might require just a few minutes, while other practices such as body scans can last for 45 minutes or more. Briefly, in every formal mindfulness exercise taught in MBPs, the body is the anchor of the practice. Although related to the attention and awareness of body sensations, this ability to sustain attention and awareness of the body is qualitatively distinct. It requires not only noticing or being aware of sensations but also sustaining attention and awareness to foster a natural feeling of connection with the body. Therefore, we hypothesize that Connection with the Body, although different from Attention and Awareness of Feelings and Bodily Sensations, builds sequentially on it and, therefore, is fundamental to the notion of “embodied mindfulness.”
Awareness of the Mind-Body Connection
Thich Nhat Hanh writes, “When body and mind are one, the wounds in our hearts, minds, and bodies begin to heal” (Nhat Hanh, 2006). This statement shows the importance of the mind-body connection in Buddhism. Similarly, Langer’s work on mindfulness (Langer, 1989, 1997; Langer et al., 1978) empirically demonstrates the central role of the mind-body interaction in inducing and cultivating mindfulness (see, for example, Crum & Langer, 2007; Langer et al., 2010; Pagnini & Philips, 2015). For instance, in her landmark “Counterclockwise” study conducted in 1979 (Langer, 2009), Langer asked participants to embed their mind in the past (20 years ago) which led to measurable changes in their bodies (e.g., in terms of strength, vision, hearing, and physical appearance). Other studies have shown similar trends (see e.g., Crum & Langer, 2007; Langer et al., 2010; Pagnini & Philips, 2015). This empirically supported bidirectional mind-body link is central to the theory of embodiment. For example, one’s body actions or body anatomy (e.g., posture) plays an important causal role in cognition and emotion. In fact, results from an RCT suggest significant effects of sitting body postures (i.e., slumped vs. upright) on memory bias (i.e., recalling positive vs. negative words) among patients diagnosed with Major Depressive Disorder (Michalak et al., 2014). Similarly, studies on gait patterns of depressed and formerly depressed individuals show that emotional processes and the motor system are closely interconnected (Michalak et al., 2009, 2010; Wendorff et al., 2002). Therefore, the mind-body connection includes the links between (a) cognitions and the body, (b) emotions (as identified mentally) and the body, and (c) cognitions and emotions. In addition, the mind-body bidirectional connection requires someone having developed a sufficient level of Connection with the Body (i.e., the previous skill) to extend that connection to the mind, and its bidirectional link with the body, therefore, may build on and develop sequentially to the previous skill rather than independently. The Awareness of the bidirectional Mind-Body (cognitions/emotions-sensations) Connection is also essential to the notion of “embodied mindfulness.”
Acceptance (i.e., Nonavoidance) of Feelings and Bodily Sensations
Acceptance is often defined as the opposite of experiential avoidance, which is the unwillingness to experience negatively evaluated emotions, physical sensations, and thoughts (Hayes & Strosahl, 2004). Bishop et al. (2004) included acceptance as part of their definition of mindfulness, and acceptance was suggested to be an active mechanism in MBPs, a predictor of their outcomes, and an element that distinguishes them from other therapeutic interventions (Lindsay & Creswell, 2017). Cardaciotto et al. (2008) developed a bidimensional measure of mindfulness with two key components: present-moment awareness and acceptance (called the Philadelphia Mindfulness Scale—PHLMS). The awareness and acceptance subscales were not correlated, suggesting that these two constructs can be examined independently. This finding further supports the independent role of acceptance in the conceptualization, operationalization, and measurement of mindfulness.
In two RCTs of stressed community adults, mindfulness skills were dismantled into two structurally equivalent interventions: (a) training in both monitoring and acceptance (Monitor + Accept) and (b) training in monitoring only (Monitor Only) without acceptance (Lindsay et al., 2018). Results showed that Monitor + Accept training increased positive affect compared with both the Monitor Only and control groups (Lindsay et al., 2018). These studies provide the first experimental evidence that developing an acceptance-orientation toward present-moment experiences is a central mechanism through which mindfulness interventions boost positive emotions in daily life. In another RCT, acceptance training was shown to be a critical driver of mindfulness training-based reductions in mind-wandering (Rahl et al., 2017).
In a meta-analysis of the effects of MBPs for psychosis, the combination of mindfulness and acceptance moderated the clinical effectiveness with a large effect size, whereas mindfulness alone moderated the clinical effectiveness with a medium effect size, showing that adding acceptance boosted the effects of MBPs for psychosis (Khoury et al., 2013). Taken together, these arguments suggest the importance of including acceptance versus avoidance when measuring mindfulness. This suggestion is particularly important in the context of accepting (i.e., not avoiding, distracting, or escaping from) bodily sensations, central to the notion of “embodied mindfulness.” According to our conceptualization, acceptance is a complete and non-defensive embrace and integration of all internal states whether pleasant or unpleasant. Therefore, developing acceptance as we conceptualized it may require the skills to (a) detach from the mind, (b) become aware of the body, (c) sustain connection with the body (while experiencing the feelings and sensations to process and accept), and (d) become aware how these sensations and feelings impact other aspects of the experience (e.g., the mind). Therefore, acceptance might be the most complex and difficult skill to cultivate, as it may require the cultivation of many if not all the previous skills; hence, we decided to list it as the last skill in fully embodying mindfulness.
Previous Mindfulness Scales and the Body
Although mindfulness practices are often anchored in the body (e.g., body scan, mindful breathing, stretching yoga in MBSR, MBCT, and MBRP), many mindfulness scales do not refer to the body when measuring mindfulness (e.g., Mindfulness Attention Awareness Scale or MAAS, Brown & Ryan, 2003; Southampton mindfulness questionnaire or SMQ, Chadwick et al., 2008; Cognitive and Affective Mindfulness Scale-Revised or CAMS-R, Feldman et al., 2007). Other mindfulness questionnaires include only a few items related to body awareness. For example, in the Kentucky Inventory of Mindfulness Skills (KIMS; Baer et al., 2004), six items referred to noticing sensations in the body among a total of 39, for example, “When I’m walking, I deliberately notice the sensations of my body moving”; the Five Facet Mindfulness Questionnaire (FFMQ; Baer et al., 2008) included four items related to body awareness among a total of 39, for example, “When I take a shower or bath, I stay alert to the sensations of water on my body”; the Philadelphia Mindfulness Scale (PHMS; Cardaciotto et al., 2008) included three items related to the body awareness among a total of 20, for example, “I notice changes inside my body, like my heart beating faster or my muscles getting tense”; and finally, the Freiburg Mindfulness Inventory (FMI; Walach et al., 2006) included only one item focusing on sensing the body among a total of 14 (“I sense my body, whether eating, cooking, cleaning or talking”). Furthermore, although the Toronto Mindfulness Scale (TAU; Lau et al., 2006) is used to measure state mindfulness, only one of its 13 items mentions body sensations (“I was curious about what I might learn about myself by taking notice of how I react to certain thoughts, feelings, or sensations”).
In comparison with previously established mindfulness scales, new scales tend to give more importance to the body, specifically regarding bodily awareness. For example, the State Mindfulness Scale (SMS; Tanay & Bernstein, 2013) included a body factor targeting mindfulness of bodily sensations with six items and a mind factor targeting mindfulness of mental events with 15 items (e.g., “I noticed some pleasant and unpleasant physical sensations”). A more recently developed Body Mindfulness Questionnaire (BMQ; Burg et al., 2017) focused exclusively on body awareness and is comprised of two factors: “experiencing body awareness” and “appreciating body awareness.” The first factor captures the extent to which the respondent mindfully stays in contact with their body in everyday life. For example, items include, “I’m so absorbed in my thoughts that I do not pay attention any more to my body,” and “I forget my body in everyday stress.” The second factor portrays one’s appreciation (valuing) of body awareness, for example, “I value sensing my body consciously” and “I value experiencing a strong connectedness with my body.” Finally, the multidimensionality of body awareness was captured by the Multidimensional Assessment of Interoceptive Awareness (MAIA; Mehling et al., 2012) that measures eight independent dimensions of body awareness; however, the MAIA does not assess mindfulness nor embodiment.
Although recent mindfulness scales (e.g., SMS and BMQ) integrate aspects of the body when measuring mindfulness, they still focus solely on body awareness. Therefore, they do not include all aspects of mindfulness and the body. Specifically, they do not integrate embodiment into mindfulness. The role of the body and specifically embodiment as a potential mechanism of action of mindfulness-based programs and its influence on clinical disorders such as depression was repeatedly emphasized by authors in the field (see, for example, Cook-Cottone & Guyker, 2018; Michalak et al., 2012).
Proposed New Embodied Mindfulness Questionnaire
The proposed questionnaire (Embodied Mindfulness Questionnaire—EMQ) aims to operationalize the proposed notion of “embodied mindfulness” as a set of skills or abilities that can be cultivated incrementally through practice. The EMQ is intended to be used with individuals with different degrees of mindfulness/meditation experience (i.e., with naïve and with moderately and highly experienced meditators) as it might be able to capture a different level of meditative expertise according to its conceptualization as a sequence of incremental skills building on each other. While most previous mindfulness disposition measures were developed for naïve meditators (e.g., FFMQ, KIMS, MAAS, and SMQ), the FMI was developed for expert meditators. The EMQ is intended to be used for both groups of meditators and among non-meditators and is also intended to be used following embodied mindfulness programs among both clinical and non-clinical populations. Note that mindfulness programs might differ in their intensity and level of training and practice. This, therefore, may influence differently the skills proposed in the EMQ. In the following, we present the method used to design and develop the items of the EMQ according to the five dimensions described above as well as three studies aiming at validating the EMQ. Study 1 aims to develop and test an initial version of the EMQ for structure evaluation and internal consistency. Study 2 tests an enhanced version of the EMQ for reliability and construct, evaluating convergent and discriminant evidence. Study 3 tests the final version of the EMQ for changes following a mindfulness-based intervention.
Study 1: Development, Factor Structure, and Internal Consistency of the EMQ
Method
EMQ Design and Development
The content validation of the items and dimensions of the EMQ was conducted in four sequential steps. As a first step, based on the notion of “embodied mindfulness” and existing literature on both mindfulness and embodiment, an item pool was initially created by the first author, who is an expert in mindfulness and a daily meditator for more than 15 years. Items reflected the five dimensions detailed in the introduction. The first skill (Detachment from Automatic Thinking), which can be considered the basis for developing the other skills, was defined as the ability to detach from automatic (unintentional) thinking or its opposite (i.e., being attached to, caught up, absorbed by, or believing thoughts). The second dimension (Attention and Awareness of Feelings and Bodily Sensations) includes the skill of directing attention to, attending, noticing, and being aware of feelings and physical sensations and changes in the sensations throughout the body. The third dimension (Connection with the Body) builds on the previous one and includes the ability to sustain attention and awareness of the body throughout time and, therefore, the impression of either being connected or disconnected (i.e., detached, removed, distanced, and separated) from the body. As mentioned above the duration of maintaining attention during mindfulness training varies across different practices. It is noteworthy that the feelings of disconnection from the body are not to be equated or even linked to dissociative experiences, which include a set of sensory (e.g., out of body), perceptual (altered sense of time and self), and cognitive (e.g., memory fogs) symptoms, among others (see, for example, Bernstein & Putnam, 1986). The fourth dimension (Awareness of the Mind-Body connection) builds as well on the previous one and comprises noticing the bidirectional associations between elements of the mind (e.g., thoughts such as negative judgments, emotional labels such as sadness, anger, and anxiety) and elements of the body (e.g., physical sensations such as heaviness, tension, discomfort, and tiredness). The fifth and last dimension (Acceptance of Feelings and Bodily Sensations), which may require cultivating all the previous skills as prerequisites (at least to a certain level), portrays the ability to not avoid or distract from emotions (even when perceived as negative or difficult) and physical sensations (even when unpleasant or painful). Both positive and negative items were generated.
In the second phase, the generated pool of items was vetted by eight English-fluent graduate students (7 females, 1 male, Master’s and PhD, members of the first author’s lab at McGill University) for language clarity and precision. All students had prior experience/practice in mindfulness/meditation and were masters or doctoral trainees in the counseling psychology program at McGill University. The procedure comprised displaying each item on a board and a panel discussion about (a) whether the item should be included or not, and (b) the best ways to convey the essence of the item while using simple English syntax. This procedure took around 2 to 3 hours and led to the removal of some items due to their poor quality and rewording for most of the remaining items.
In the third phase, the list of remaining items was sent by email to 11 experts in the field who were identified through their leading publications or were contacted at an international conference on mindfulness and accepted to review and provide feedback on the questionnaire. The reviewers included four editors of a leading journal in the field among them the chief editor of a journal, three authors of established psychological scales among them the authors of three known and highly used scales of mindfulness disposition (one of them was the author of two of these measures), a director of a mindfulness and contemplative center, a Buddhist monk, four leading clinical psychologists in mindfulness-based treatments, and one with both meditative and Langer’s mindfulness backgrounds. All the reviewers have shared having personal meditation practice or experience, more than half of them have published books on mindfulness, some of these discussed the role of the body in mindfulness, most of the reviewers provided lectures on mindfulness on the international level, and all of them had one or more leading academic or clinical training position at a highly recognized institution. The reviewers were asked to comment on both the five dimensions and the items within each dimension without a predefined structure; therefore, they were free to use the style they preferred. Ten of the 11 reviewers sent back written comments about the questionnaire’s dimensions and items. The comments and suggestions the reviewers provided were carefully analyzed by the first author and used to modify existing items or add new ones to enhance the precision to the five dimensions.
The fourth and last phase involved editing the added and modified items for language simplicity and clarity by the same team of graduate students using the same procedure described above but without removing any item at that stage. This phase led to the inclusion of 48 items in the initial version of EMQ. Both students and experts were not monetarily compensated for their participation. Due to the nature of the items, the name of the third subscale was changed (reversed) from “Connection with the Body” to “Disconnection from the Body.” We will use this terminology throughout the remaining of the article.
The instructions for participants on the top of the questionnaire and Likert-type scale used to rate each item of the questionnaire (from 1 = almost never to 5 = almost always) has gone as well through the vetting process by the graduate students and the experts in the field. In the final version, the instructions were tailored to capture the everyday experiences of participants without a specific timestamp. In addition, following the feedback from experts, the instructions included asking participants to carefully read each statement (i.e., each item) and to answer according to what accurately reflects their experience rather than what they think their experience should be. The Likert-type scale remained unchanged. Following the development of the EMQ’s items, we tested this initial version of the questionnaire to evaluate its structure and internal consistency.
Participants
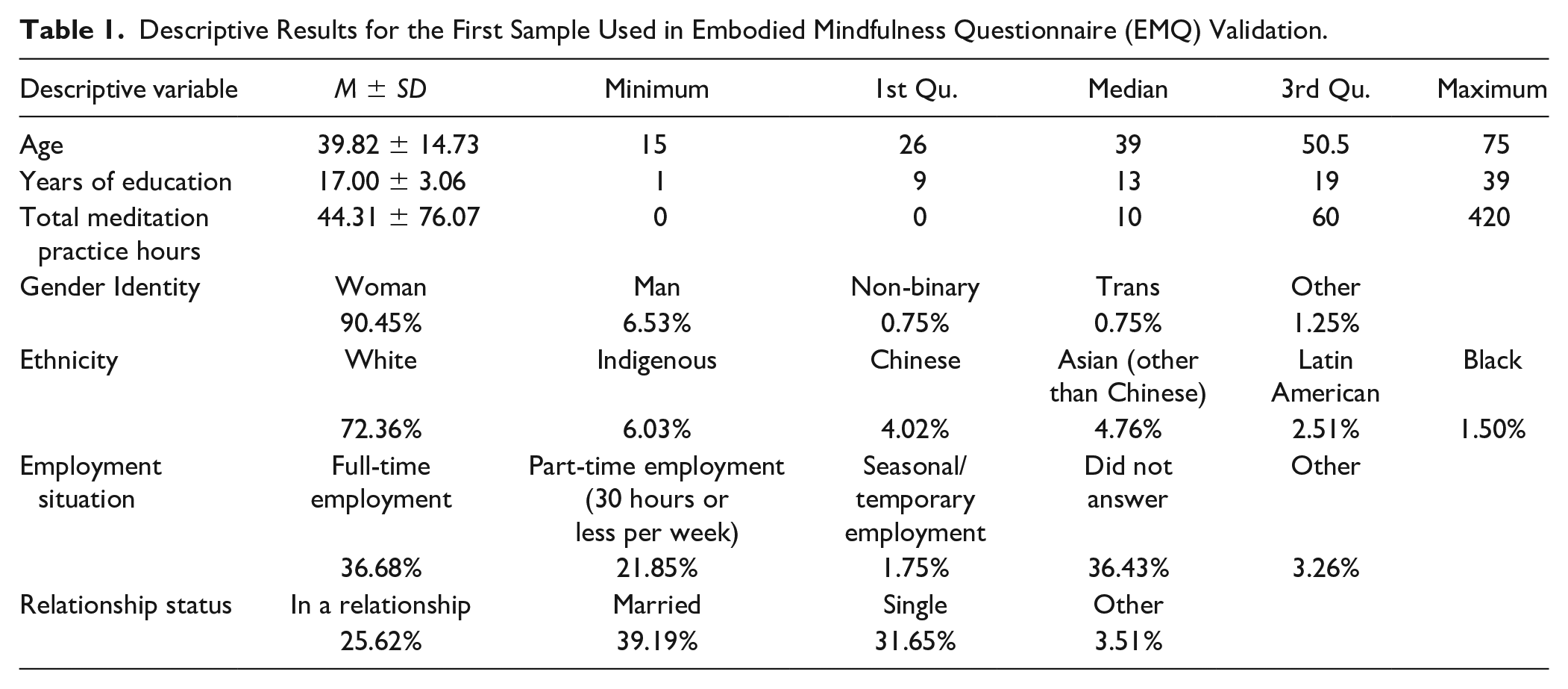
A sample of adults were recruited via paid advertising on social media (e.g., Facebook, LinkedIn, and Instagram). Participants were offered US$50 gift certificates based on a draw with a rate of winning of 1/20. We aimed to obtain a sample of over 300 participants suggested as sufficient, being above the 5:1 item:participants ratio (MacCallum et al., 1999; Reio & Shuck, 2015). The sample was composed of 407 participants, 90.1% female, 6.8% male, and 3.1% reported another gender or preferred not to answer. The mean age was 39.97 ± 14.76 years. Detailed descriptions of this sample are available in Table 1.
Descriptive Results for the First Sample Used in Embodied Mindfulness Questionnaire (EMQ) Validation.
Procedure
Study 1 was approved by the Research Ethics Board Office at McGill University. Participants gave informed consent prior to completing the study. The study was conducted entirely online using LimeSurvey and included sociodemographic data with detailed information regarding meditation practice or mindfulness training/experience along with the new measure under validation (i.e., EMQ).
Data Analysis
Given that we expected the EMQ to be used with individuals with different levels of meditation experience (i.e., not only with expert meditators) and to ensure the absence of outliers, we removed all participants with more than 600 hours of meditation experience. This reduced the sample size from 407 to 398.
EMQ structure was evaluated using a mixed Exploratory Factor Analysis (EFA) and Confirmatory Factor Analysis (CFA) approach. The rationale was to evaluate the theoretically proposed structure using CFA, but also checking whether the same structure would emerge from EFA, allowing us therefore to test the stability of the EMQ structure (Bandalos & Finney, 2010; Gerbing & Hamilton, 1996; Orcan, 2018; Schmitt, 2011). For EFA, given the multidimensional nature of the EMQ, we initially performed Parallel Analysis and Optimal Coordinates methods to determine the number of factors to extract (Hayton et al., 2004; Raîche et al., 2013). Once this number was determined, we evaluated multivariate normality using the Henze–Zirklers’s test. In the case where multivariate normality was not met, we proceeded using Principal Axis Factorization Extraction instead of Maximum Likelihood (Costello & Osborne, 2005; de Winter & Dodou, 2012). Finally, given the exploratory nature of this analysis and expecting at least some of the subscales will be correlated, we used an oblimin rotation. EFA was performed using 1,000 bootstrap iterations, reporting the mean of the loadings and 95% confidence intervals. This procedure was iteratively implemented removing crossloaders (loading in more than one factor) and subloaders (presenting all loadings in the range of −0.3, +0.3). In parallel, CFA structure was evaluated to check the weakest items by assessing residuals and local fits (R2). This iterative process was also evaluated jointly taking into consideration theoretical concerns, confidence intervals of the loadings, and crossloading characteristics, exploring solutions without total removal of crossloaders or subloaders and removing some items from the analysis.
Once the EMQ structure and retained items were defined, we proceeded to evaluate internal consistency using Cronbach’s α (Cronbach, 1951). We also included total Omega following the criticism of many authors about only using Cronbach’s alpha (Dunn et al., 2014; Huysamen, 2006; Peters, 2014; Sijtsma, 2009). Confidence intervals were also provided using 1,000 bootstrap iterations. During internal consistency estimations, we evaluated the effects of the removal of each item on the subscale’s internal consistency. Once the internal consistency analysis was completed, we conducted a final CFA, reporting global fits, root mean square error of approximation (RMSEA), and Tucker–Lewis Index (TLI) as diagnostics parameters. All statistical analyses and data processing were performed with R project (R Core Team, 2019).
Results
We started with 48 items, which were iteratively pruned according to the method described above. Once the initial solution was obtained, the analysis of each iteration, confidence intervals of item loadings, and consistency were evaluated. Using the results, each item was evaluated in terms of its potential interpretation bias. Based on these evaluations, we removed six items (EMQ15, EMQ10, EMQ28, EMQ44, and EMQ37) prior to another run of EFA–CFA analyses. Subsequently, the iterative process was repeated, which led to the EFA solution presented in Table 2. The results yielded the five proposed factors, with all absolute values of loadings and their lower 95% confidence interval above 0.3. All internal consistencies and their lower 95% confidence interval were above 0.7 (Table 2). The highest consistency was obtained for the scores of the Disconnection from the Body subscale, which had an internal consistency of 0.94. This EFA solution presented a Kaiser–Meyer–Olkin (KMO) of 0.87, RMSEA of 0.114, and TLI of 0.773, while CFA presented an RMSEA of 0.067 and TLI of 0.86.
Original Embodied Mindfulness Questionnaire (EMQ) Version Exploratory Factor Analysis Results Post Item Pruning.
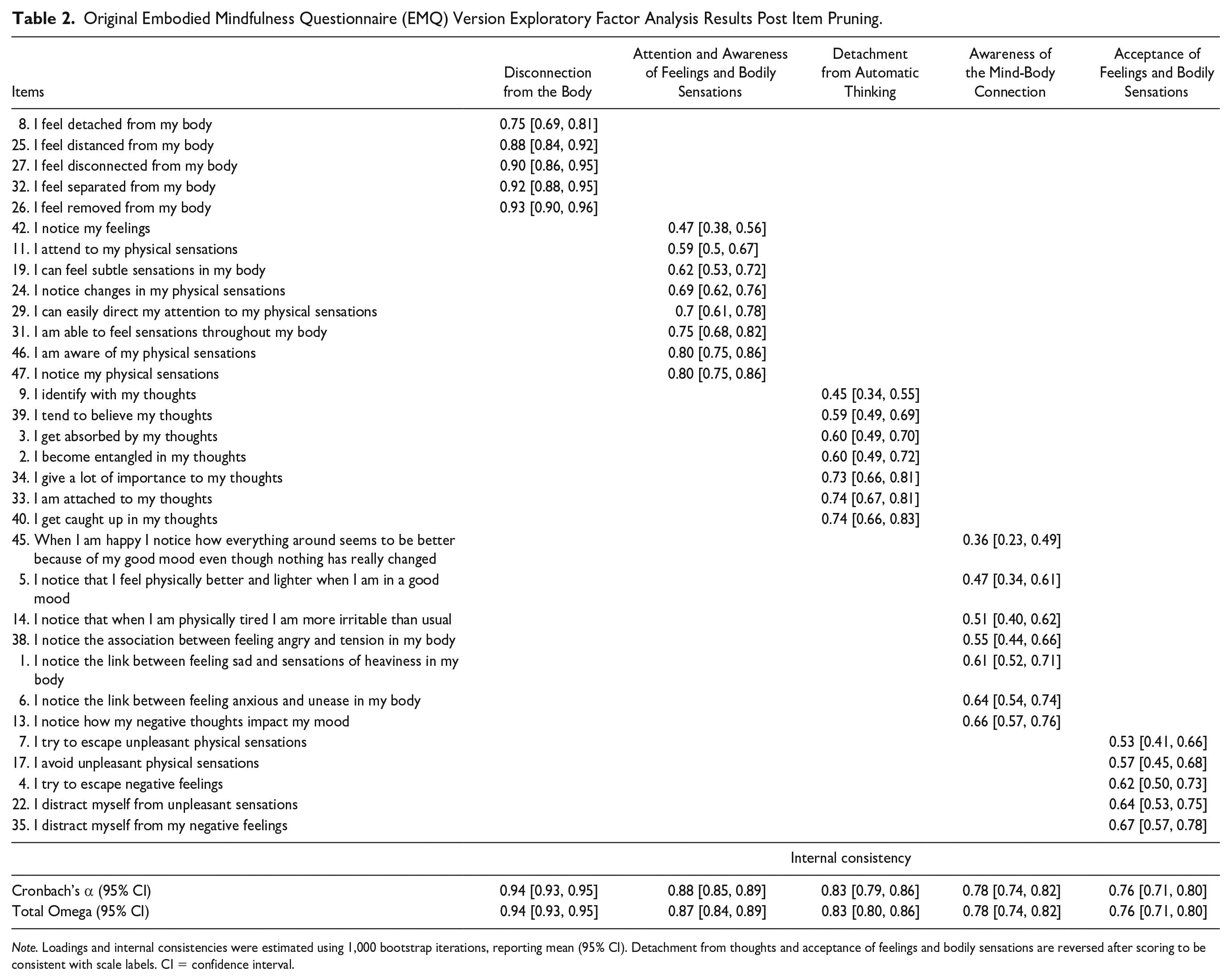
Note. Loadings and internal consistencies were estimated using 1,000 bootstrap iterations, reporting mean (95% CI). Detachment from thoughts and acceptance of feelings and bodily sensations are reversed after scoring to be consistent with scale labels. CI = confidence interval.
Discussion
The objectives of the current study were to develop and test the initial 5-dimension structure, with 48-item version of EMQ and each dimension’s internal consistency. Results from EFA and CFA confirmed the five proposed dimensions of the EMQ, with lower global fit for EFA compared with CFA. In EFA factor loading, confident intervals did not cross the 0.3 threshold, supporting it as a stable 5-dimension structure. For both EFA and CFA, RMSEA was higher than 0.05 and TLI was lower than 0.9, suggesting the need for reevaluating and improving some of the items which composed the EMQ’s five dimensions.
Based on these obtained results, we improved the instrument by balancing the number of items per subscale, as well as ameliorating the item loadings and increasing the internal consistency of the weaker subscales. To do so, we inspected items one by one, evaluating the performance of their scores on CFA, EFA, and their impact on internal consistency, as well as potential interpretation problems, such as wording ambiguity. This procedure led to the modification of some items and the inclusion of new items, yielding to the second version of the EMQ with 25 items, five items per dimension. The new version underwent the same evaluation, but we also included other instruments to present convergent and discriminant evidence (Study 2).
Study 2: EMQ’s Second Version Structure, Internal Consistency, and Convergent/Discriminant Evidence
Method
Participants
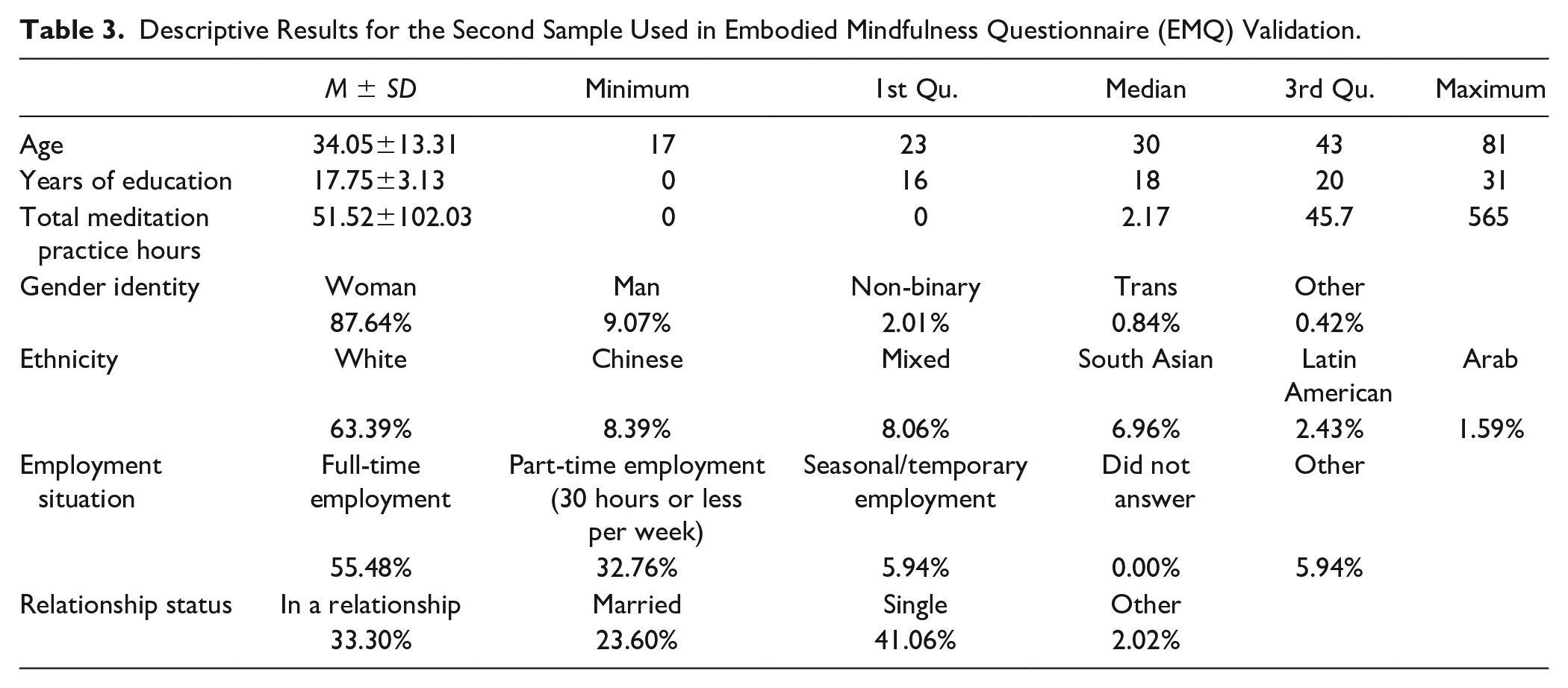
With the aim of increasing external validity for the current study, and to achieve the most conservative sample size, we aimed for a sample size of >1,000 (MacCallum et al., 1999). It is fairly accepted that there are not good recommendations for sample size for factor analysis; however, it is accepted that ranges above 500 to 1,000 using item-observation ratios above 1:5 are a conservative and safe approach (Costello & Osborne, 2005; MacCallum et al., 1999; Reio & Shuck, 2015). Using the same means as in Study 1 (i.e., paid ads on social media, for example, Facebook, LinkedIn, Instagram), 1,191 adult participants were recruited; among them, 87.6% were female, 9.0% male, and 3.4% reported another gender or preferred not to answer. The mean age was 34.04 years ± 13.31. Participants were offered US$100 gift certificates based on a draw with a rate of winning of 1/16. The monetary compensation was larger in the current study as participants had to respond to a larger number of questionnaires than in Study 1. Detailed descriptions of the sample are available in Table 3.
Descriptive Results for the Second Sample Used in Embodied Mindfulness Questionnaire (EMQ) Validation.
Procedure
Similar to the previous study, Study 2 was approved by the Research Ethics Board Office at McGill University. Participants gave informed consent prior to completing the study. The study was also conducted entirely online using LimeSurvey and included sociodemographic data with detailed information regarding meditation practice or mindfulness training/experience along with the new measure under validation (i.e., EMQ) and a list of other measures for external validation.
Additional Instruments
A total of 22 instruments were administered, while for the aims of the present report only 13 instruments were used for convergent, discriminant, and exploratory purposes. For convergent evidence, the Body Mindfulness Questionnaire (BMQ, 14 items; Burg et al., 2017), Five Facet Mindfulness Questionnaire (FFMQ, 39 items; Baer et al., 2006), Mindfulness Attention and Awareness Scale (MAAS, 15 items; Brown & Ryan, 2003), Acceptance and Action Questionnaire-II (AAQ2, 7 items; Bond et al., 2011), Multidimensional Assessment of Interoceptive Awareness (MAIA, 32 items; Mehling et al., 2012), and Cognitive Fusion Questionnaire (CFQ, 7 items; Gillanders et al., 2014) were used. In addition, we measured the amount of meditation practice. This amount was computed using four questions: (a) the average number of minutes participants practiced meditation per week (0 if they do not practice meditation), (b) the number of months since participants started practicing meditation (0 for no practice and for less than 1 month of practice; in the case of the latter, participants were also asked to enter a number between 0 and 0.99 that reflects the percentage of days they practiced during the month), (c) the number of meditation retreats participants attended (0 if they did not attend any meditation retreat), and finally, (d) the number of hours participants practiced meditation during the retreats they attended (0, if they did not attend any meditation retreat).
For discriminant evidence, the Perceived Stress Scale (PSS, 10 items; Cohen et al., 1983), Depression Anxiety Stress Scales (DASS, 42 items; Lovibond & Lovibond, 1995), Positive and Negative Affect Scale (PANAS-GEN, 20 items; Watson et al., 1988), Difficulties in Emotion Regulation Scale (DERS, 36 items; Gratz & Roemer, 2004), and Toronto Alexithymia Scale (TAS-20, 20 items; Bagby et al., 1994) were used. For exploratory purposes, the Satisfaction With Life Scale (SWLS, 5 items; Diener et al., 1985) and Oxford Happiness Questionnaire (OHQ, 29 items; Hills & Argyle, 2002) were used. Internal consistencies calculated using Cronbach’s α were computed for all scales and subscales of the instruments used for convergent, discriminant, and exploratory evidence. Overall, coefficient alphas were found to be acceptable; see Table 4 for more detailed information.
Internal Consistencies, Calculated via Cronbach’s Alpha, of Total and Subscale Scores of Instruments Used for Convergent, Discriminant, and Exploratory Evidence.
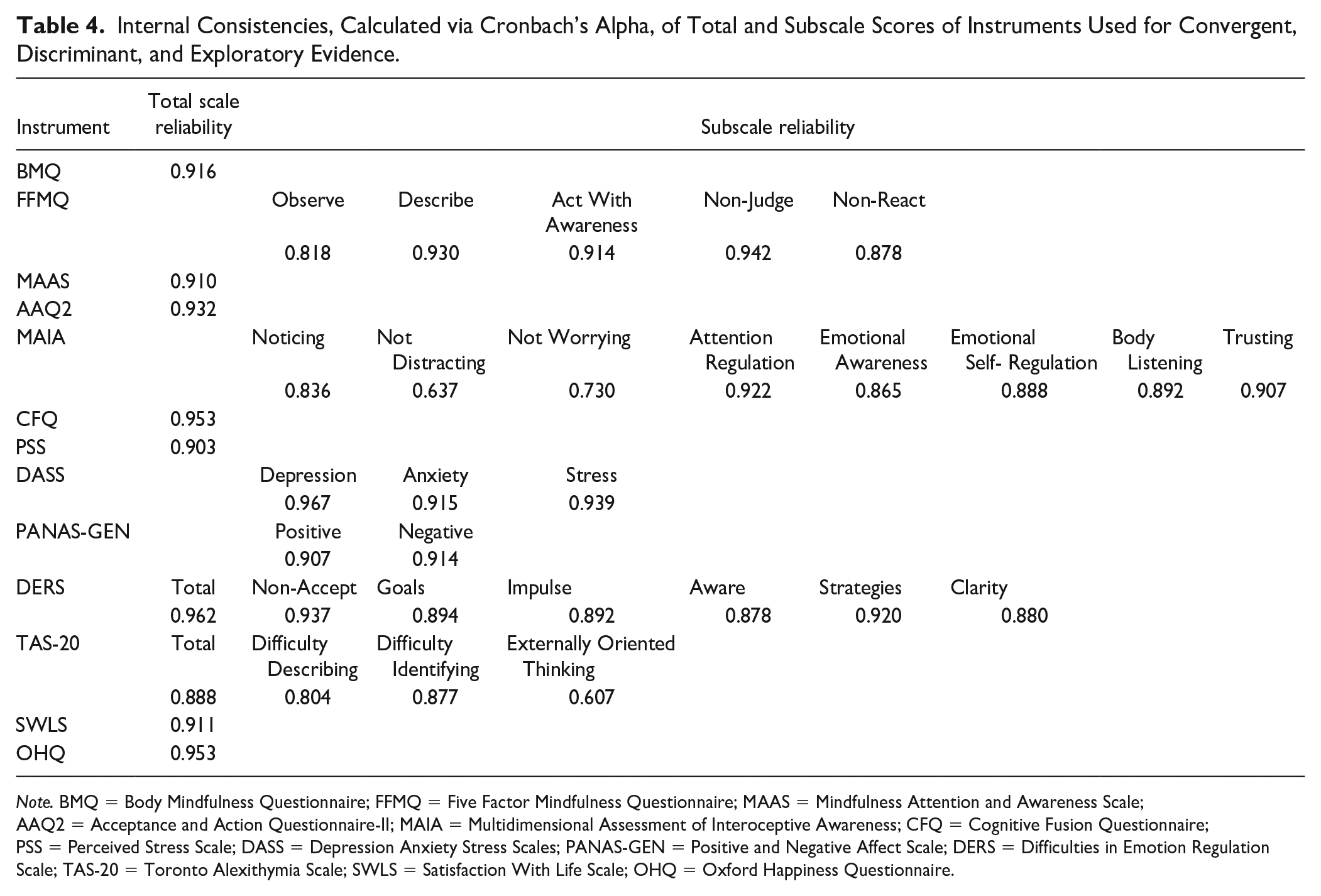
Note. BMQ = Body Mindfulness Questionnaire; FFMQ = Five Factor Mindfulness Questionnaire; MAAS = Mindfulness Attention and Awareness Scale; AAQ2 = Acceptance and Action Questionnaire-II; MAIA = Multidimensional Assessment of Interoceptive Awareness; CFQ = Cognitive Fusion Questionnaire; PSS = Perceived Stress Scale; DASS = Depression Anxiety Stress Scales; PANAS-GEN = Positive and Negative Affect Scale; DERS = Difficulties in Emotion Regulation Scale; TAS-20 = Toronto Alexithymia Scale; SWLS = Satisfaction With Life Scale; OHQ = Oxford Happiness Questionnaire.
Data Analysis
Similar to the first study and for the same reasons, we removed all participants with more than 600 hours of meditation experience. This procedure reduced the sample size from 1,191 to 1,077 participants. The obtained sample was used for all subsequent analyses including the ones related to meditation experience.
Construct evaluation started using CFA solution, followed by EFA. CFA–EFA procedure as well as internal consistency followed the same rationale used in Study 1. As with Study 1, once the internal consistency analysis was completed, we again conducted CFA. However, we also included Akaike Information Criteria (AIC) and Bayesian Information Criteria (BIC) as diagnostics parameters. The Bayesian diagnostics allowed us to contrast an oblique CFA solution against a hierarchic structure denoting the existence of one global EMQ variable. This last aspect is central to our aims, as we have proposed EMQ as a set of different skills that build over each other. Therefore, it is likely that EMQ subscales will not correlate sufficiently to produce a meaningful global score. In addition, to evaluate whether the second version of EMQ outperformed the first, we compared the CFA solutions for the first and second sample.
Following the factor analyses, we aimed to evaluate whether EMQ had convergent and discriminant evidence in favor of the theoretical proposed constructs. Convergent evidence was assessed using Pearson’s correlations of EMQ subscales with the instruments mentioned above. For discriminant evidence, we used multiple linear regression models to predict scores of different instruments measuring psychopathology or psychological symptoms. Specifically, we used EMQ subscales as independent variables and number of hours of meditative practice, DASS scores (depression, anxiety, and stress), PANAS (positive and negative affect), and PSS (perceived stress) as dependent variables. Collinearity was evaluated using variance inflation factor (VIF). In the case of VIF >2, we evaluated each variable separately keeping the model with the highest adjusted R2. Nonsignificant variables were removed using the backward method, and no interactions were evaluated. Adjusted R2 is reported for each regression model.
Finally, we explored how meditative experience may affect the discriminative evidence of the EMQ. To achieve this objective, we performed a hierarchical clustering analysis using Euclidean distance, dividing the sample according to the total number of meditation hours and the number of breaths during meditation until participants lose their focus and have to redirect attention back on the breath. Given that both variables (i.e., meditation hours and number of breaths) are expected to present highly skewed distributions, we used bestNormalize R library to explore variable normalizations (Peterson & Cavanaugh, 2020). To select the number of clusters, we used 30 different indices indicating the likely number of clusters in the sample (Charrad et al., 2014). Each method suggestion was considered as a vote. The number of clusters presenting the highest number of votes was considered as the most likely solution. Clusters were then characterized, and discriminant evidence by means of regression analyses was repeated for each obtained cluster. Similar to Study 1, all statistical analyses and data processing were performed with R project (R Core Team, 2019).
Results
Construct and Reliability Evaluation
The second version of the EMQ started with 25 items, five per subscale, with the aim to improve the EFA and internal consistency results. CFA presented five dimensions with all items being significant with a TLI of 0.90 and an RMSEA of 0.067. However, Item 5 from the subscale Awareness of the Mind-Body Connection (“I notice that when I am physically tired, I am more irritable than usual”) presented a remarkably low R2 (.06), the lowest standardized coefficients and highest residuals of EMQ. EFA also supported that Item 5 was problematic as its loading was less than 0.3. Therefore, Item 5 was removed, and solutions converged into the results reported in Table 5. In general terms, the second version maintained the good results originally obtained for the scores on the Disconnection from the Body and Attention and Awareness of Feelings and Bodily Sensations subscales and improved the results for the three remaining subscales. The lowest internal consistency was again for the scores of the Awareness of the Mind-Body Connection subscale, with a total Omega and Cronbach alpha of .79. The factor solution presented a KMO of 0.87, RMSEA of 0.07, and a TLI of 0.9. Compared with the original version, the updated EMQ presented an important improvement in general psychometrics (see Table 6).
Second Embodied Mindfulness Questionnaire (EMQ) Version Exploratory Factor Analysis Results Post Item Pruning.
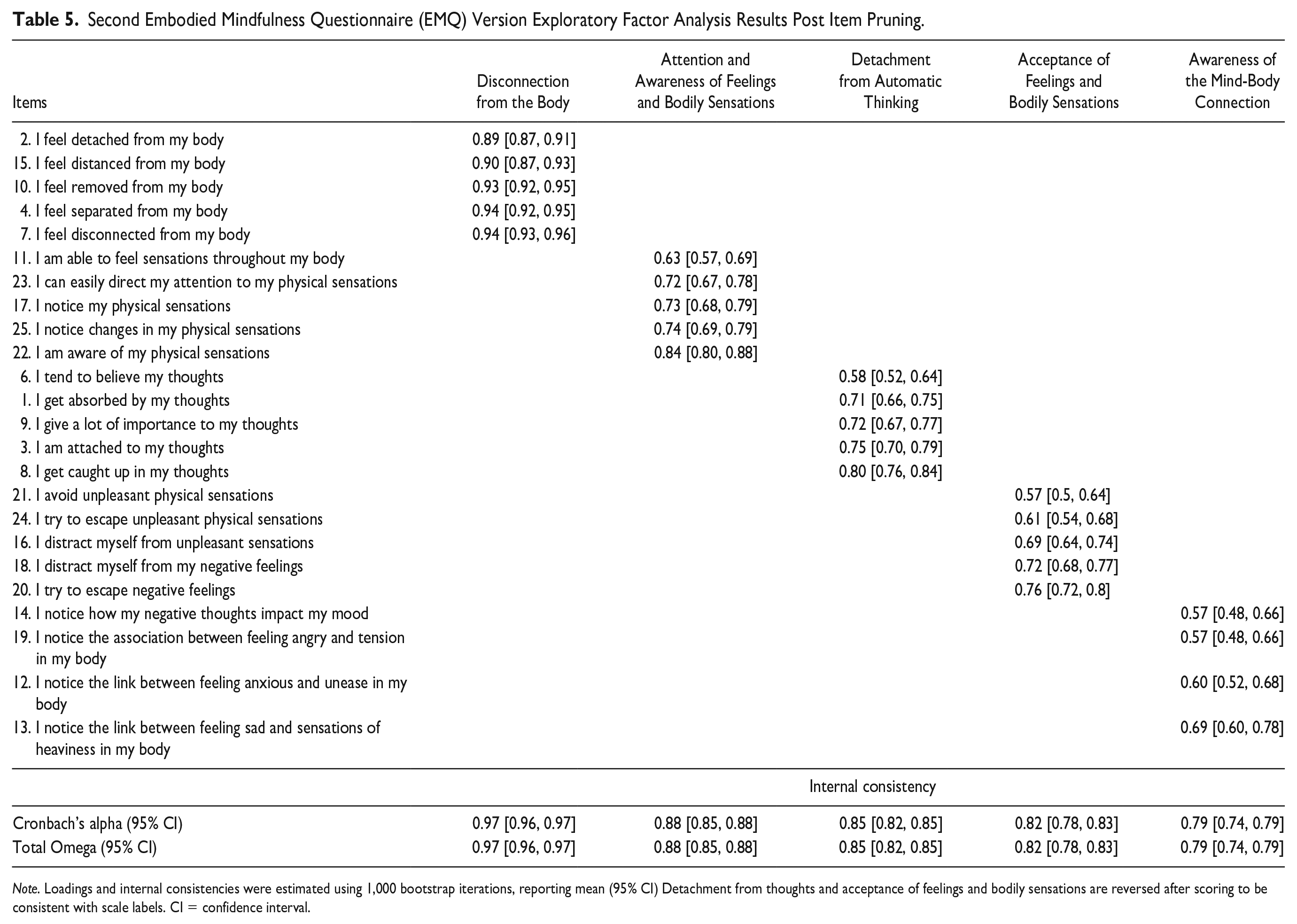
Note. Loadings and internal consistencies were estimated using 1,000 bootstrap iterations, reporting mean (95% CI) Detachment from thoughts and acceptance of feelings and bodily sensations are reversed after scoring to be consistent with scale labels. CI = confidence interval.
Exploratory Factor Analysis Diagnostics Comparison Between the Original and Second EMQ Versions.
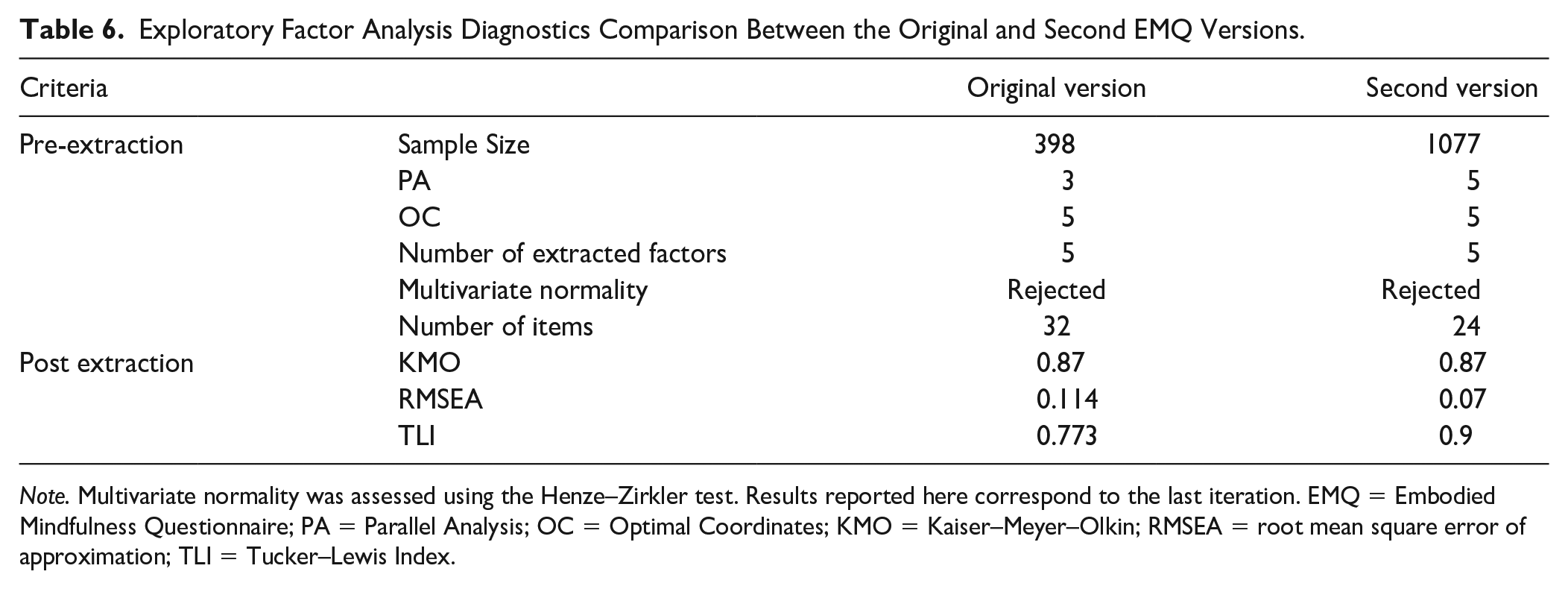
Note. Multivariate normality was assessed using the Henze–Zirkler test. Results reported here correspond to the last iteration. EMQ = Embodied Mindfulness Questionnaire; PA = Parallel Analysis; OC = Optimal Coordinates; KMO = Kaiser–Meyer–Olkin; RMSEA = root mean square error of approximation; TLI = Tucker–Lewis Index.
Since the current version was considered good enough to be final, we explored whether all the subscales’ scores combined would be able to produce the “embodied mindfulness” notion as one singular latent variable. In contrast, we also evaluated whether subscales would be considered totally or partially independent. To test these hypotheses, we evaluated two CFA models: (a) a hierarchical one, where all the EMQ subscales’ scores would load into one general “embodied mindfulness” latent variable, and (b) an oblique one, which was the alternative hypothesis where the five subscales’ scores were allowed to covariate without specifying the presence of a global unique latent variable. Illustrations of both models are presented in Figure 1. As depicted in Table 7, the hierarchical solution presented higher residuals, lower TLI, and higher Bayesian scores (AIC and BIC). We interpreted these results as less parsimonious than those of the oblique solution. As shown in Table 7, the Oblique solution was a significantly better fit than the Hierarchical solution. The main reason is the low loadings of some of the EMQ subscale scores on the EMQ latent variable. For instance, scores of “Attention and Awareness of Feelings and Bodily Sensations” subscale presented such a low loading compared with the EMQ that in Figure 1 the arrow has completely vanished. Of the remaining four subscales, only scores of Detachment from Automatic Thinking subscale presented a robust loading with the EMQ latent variable. In addition, the correlations among the five EMQ subscales’ scores were very weak (with Pearson’s r values mostly below .3; see Figure 2). The highest correlation was between the scores of Awareness of the Mind-Body Connection and Attention and Awareness of Feelings and Bodily Sensations subscales, with a Pearson’s r of .48. Therefore, the EMQ subscales’ scores are weakly associated, making it less likely for them to be produced by one single global latent variable.
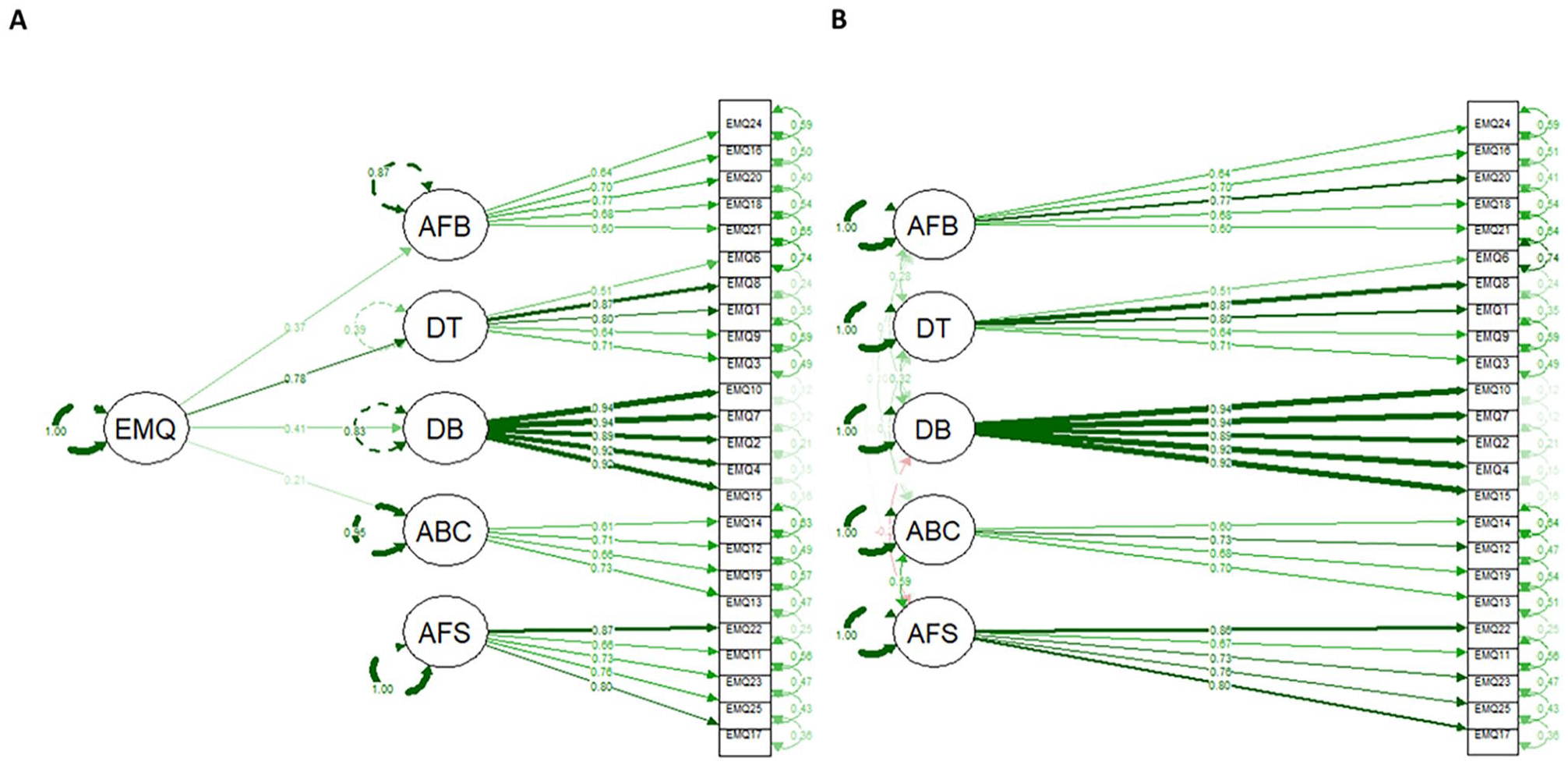
Confirmatory Factor Analysis Results for the (A) Hierarchical and (B) Oblique Scales Solutions
Confirmatory Factor Analysis Diagnostics Using Hierarchical or Oblique Embodied Mindfulness Questionnaire (EMQ) Subscales.
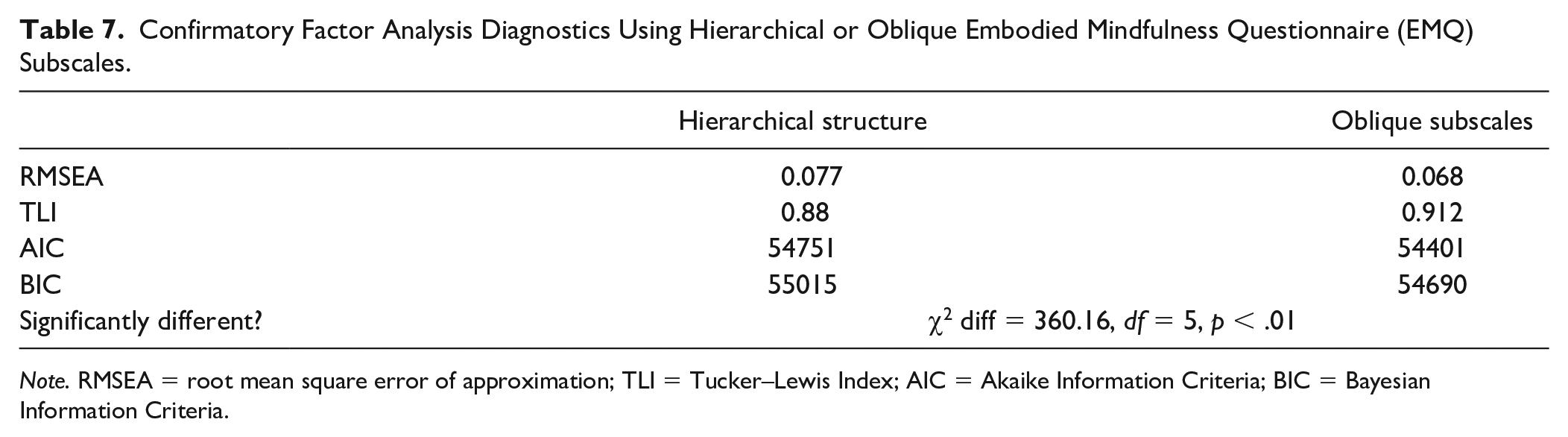
Note. RMSEA = root mean square error of approximation; TLI = Tucker–Lewis Index; AIC = Akaike Information Criteria; BIC = Bayesian Information Criteria.
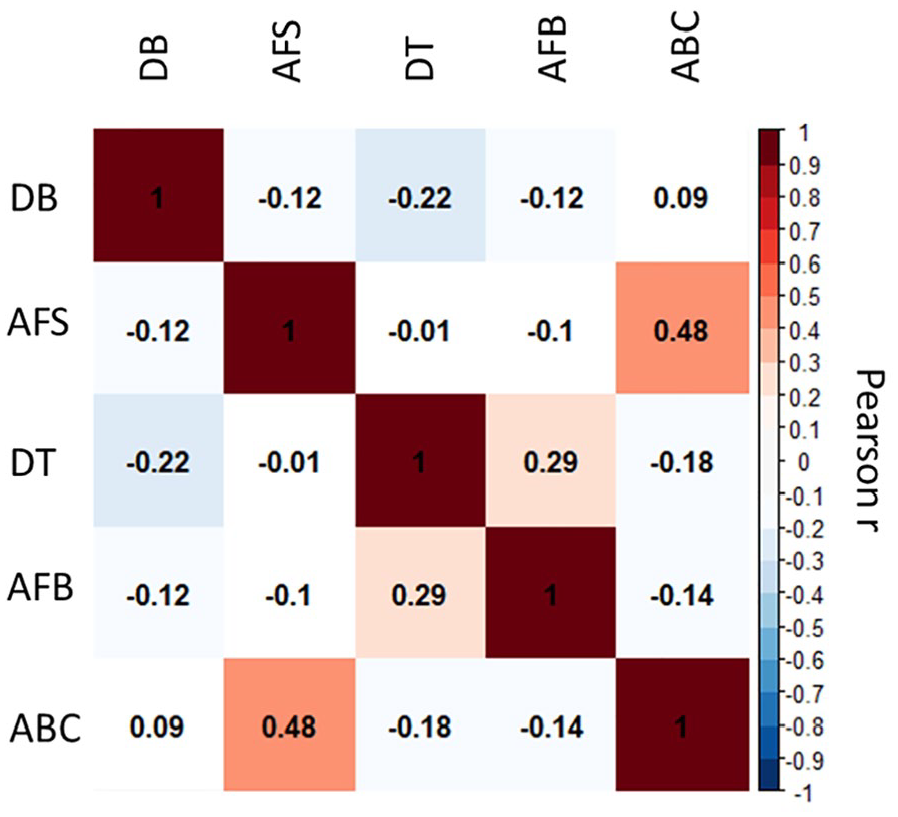
Pearson’s Correlation Matrix Between the Embodied Mindfulness Questionnaire (EMQ) Second Version Subscales
EMQ Convergent and Discriminant Evidence
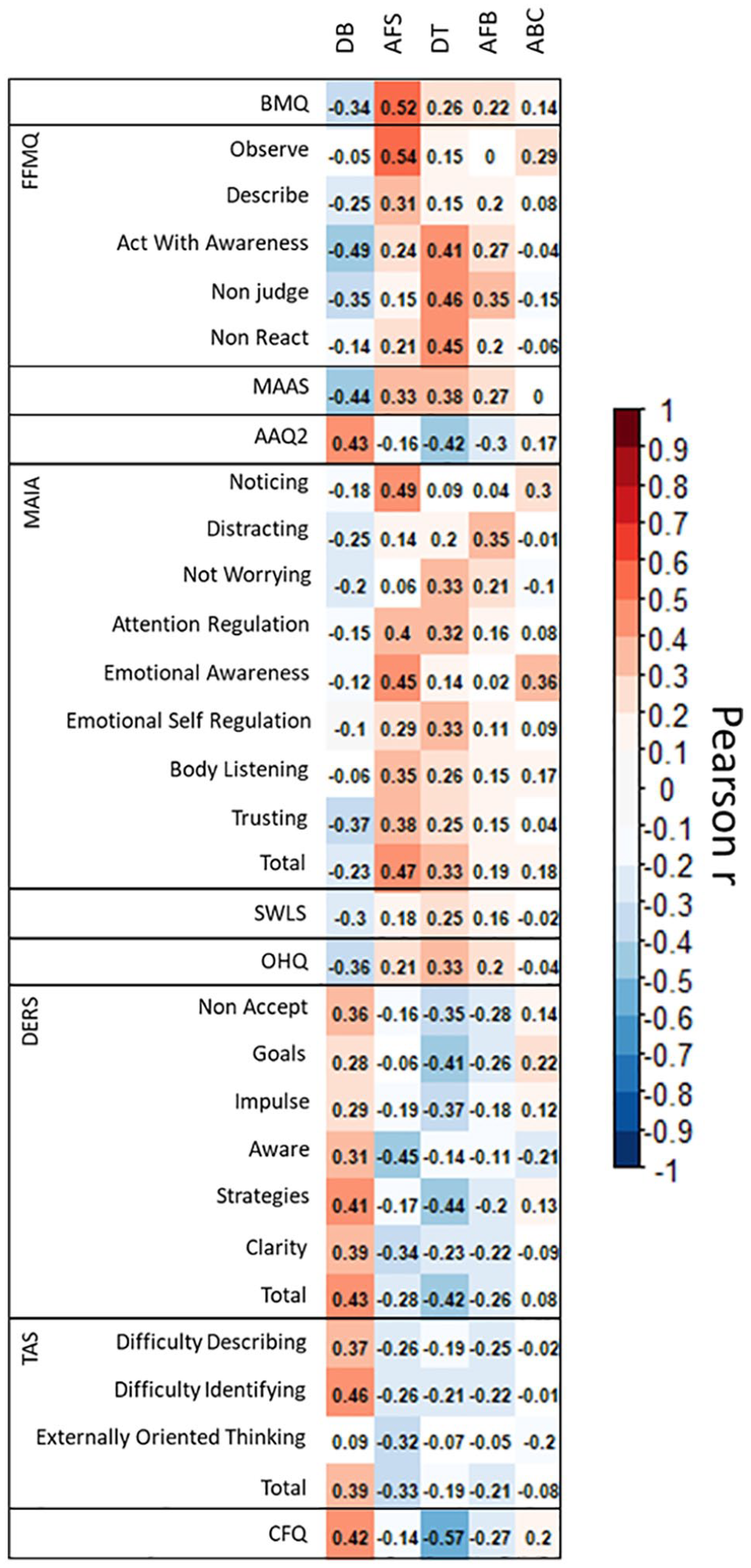
To explore convergent evidence, we first estimated EMQ subscale scores as the average of each item. For Detachment from Automatic Thinking subscale, we reversed the scoring as items were inversely phrased. Then, we performed Pearson’s correlations with mindfulness instruments, with the expectation to find significant positive associations. We expected also that scores of instruments such as the BMQ would be strongly associated with EMQ’s subscales scores, as EMQ subscales take into consideration the bodily aspects of mindfulness. As presented in Figure 3, scores of the Attention and Awareness of Feelings and Bodily Sensations subscale had a Pearson correlation r of .52. The score of this subscale was consistently associated with the scores of FFMQ Observe subscale (Pearson’s r = .54) and with many of the MAIA subscales’ scores and its total score (see Figure 3 for details). Scores of other instruments such as MAAS and AAQII and the remaining subscales of the FFMQ were mainly associated with scores of Detachment from Automatic Thinking and Disconnection from the Body subscales. Scores of Acceptance of Feelings and Bodily Sensations and Awareness of the Mind-Body Connection subscales presented the weakest correlations with scores of classic measurements of mindfulness.
Pearson Correlation Matrix for Convergent Validity
When exploring associations with scores of the SWLS and the OHQ, scores of Acceptance of Feelings and Bodily Sensations subscale, in addition to the scores of the subscales which captured the classic aspects of mindfulness (i.e., Detachment from Automatic Thinking, Attention and Awareness of Feelings and Bodily Sensations and Disconnection from the Body), showed significant correlations. Furthermore, all the EMQ subscales’ scores showed significant correlations with many of the DERS subscales’ scores. However, for the scores of TAS-20, only the scores of Awareness of the Mind-Body Connection subscale presented a significant, albeit weak, correlation. Finally, for scores of Cognitive Fusion (CF), we expected that all subscales’ scores of EMQ would be highly correlated with scores of CF. This hypothesis was supported; however, scores of the Attention and Awareness of Feelings and Bodily Sensations subscale did not correlate with scores of CF. In general, EMQ subscales presented the associations we expected when we designed the instrument’s subscales. The Detachment from Automatic Thinking, Attention and Awareness of Feelings and Bodily Sensations and Disconnection from the Body subscales capture the classic mindfulness construct as wells as domains where mindfulness is expected to be associated with other related but distinct constructs (e.g., SWLS, OHQ, DERS, TAS, and CFQ). The Awareness of the Mind-Body Connection and Acceptance of Feelings and Bodily Sensations subscales presented the lowest associations, being the most novel aspects of EMQ. The skills portrayed in these two subscales may also build on the skills depicted in the other subscales and, therefore, may require more prolonged training and intense practice. As such, we expected these subscales to be impacted by meditative experience.
For discriminant evidence, we first evaluated if the EMQ subscales’ scores could predict: (a) the total number of hours of meditative practice; scores of DASS, that is, score of (b) depression, (c) anxiety, and (d) stress; scores of PANAS, that is, scores of (e) positive affect and (f) negative affect, and scores of PSS, that is, scores of (g) perceived stress. All EMQ subscales’ scores were significant predictors of two or more of these seven dependent variables (Table 8). Scores of the Disconnection from the Body, Attention and Awareness of Feelings and Bodily Sensations, and Detachment from Automatic Thinking subscales were consistently significant predictors for the scores of all seven of the dependent variables. Scores of Awareness of the Mind-Body Connection subscale were only a significant predictor of DASS Anxiety, DASS Stress, PANAS Negative, and PSS scores. Scores of the Acceptance of Feelings and Bodily Sensations subscale presented the weakest results, predicting only PANAS negative and PSS scores and showed the lowest standardized coefficients. Most models presented R2 explaining between 20% and 30% of the total variance. Meditation experience, measured through the total of reported meditation hours, had the lowest R2, explaining only 5% of the total variance. As such, we may conclude that EMQ subscales can predict psychopathological symptoms, as expected, based on previous mindfulness instruments.
Discriminant Validity Results.
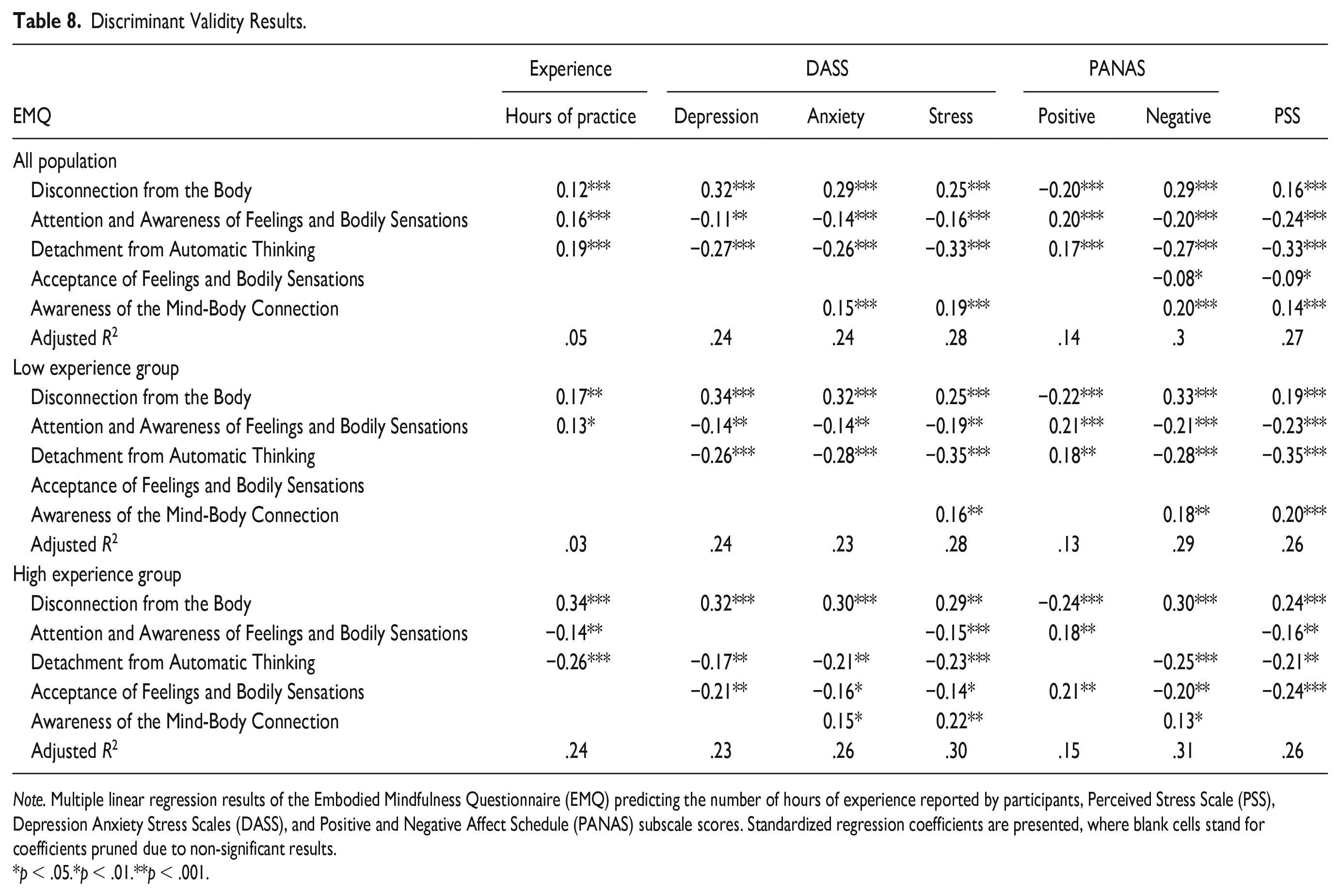
Note. Multiple linear regression results of the Embodied Mindfulness Questionnaire (EMQ) predicting the number of hours of experience reported by participants, Perceived Stress Scale (PSS), Depression Anxiety Stress Scales (DASS), and Positive and Negative Affect Schedule (PANAS) subscale scores. Standardized regression coefficients are presented, where blank cells stand for coefficients pruned due to non-significant results.
p < .05.*p < .01.**p < .001.
Meditation experience was also expected to be relevant, particularly regarding the Awareness of the Mind-Body Connection and Acceptance of Feelings and Bodily Sensations subscales as suggested above. To evaluate how meditation experience may affect discriminant analyses, we used clustering to split the participants’ samples into groups with different levels of meditative experience. Results of the analysis suggested splitting the sample into two groups (a high and a low meditation experience group). Meditation experience and the EMQ subscales’ scores characteristics of these groups are presented in Figure 4A to 4C. The high meditative experience group consistently showed lower psychopathology scores and higher PANAS positive scores. These two groups differed only on the EMQ Detachment from Automatic Thinking and Attention and Awareness of Feelings and Bodily Sensations subscale scores (see Table 8 for details). However, when repeating the linear model analyses, we found significant differences in the relative contribution of EMQ subscale scores for each predicted variable. The most important finding is that the Acceptance of Feelings and Bodily Sensations subscale score was not found to be a significant predictor for any of the seven variables in the low meditative experience group. Conversely, the Acceptance of Feelings and Bodily Sensations subscale score was a significant predictor for scores of all measures except meditative experience in the high meditative experience group (see Table 8). In addition, the EMQ subscales’ scores explained 24% of the meditation experience variance for the high meditative experience group compared with 3% of the variance explained for the low meditative experience group, using the same regression model. Attention and Awareness of Feelings and Bodily Sensations subscale score lost predictive relevance in the high meditative experience group and presented a lower level of significant results and even lower standardized coefficients. These results are in line with the hypothesis we proposed regarding EMQ’s sequential skills development. Specifically, the results suggest that as Acceptance of Feelings and Bodily Sensations skill gains relevance with the more experienced meditators, the more basic skills such as Attention and Awareness of Feelings and Bodily Sensations lose relevance. In addition, it is important to notice that both Awareness of the Mind-Body Connection and Acceptance of Feelings and Bodily Sensations subscales were sensitive to meditative experience, as we previously hypothesized.
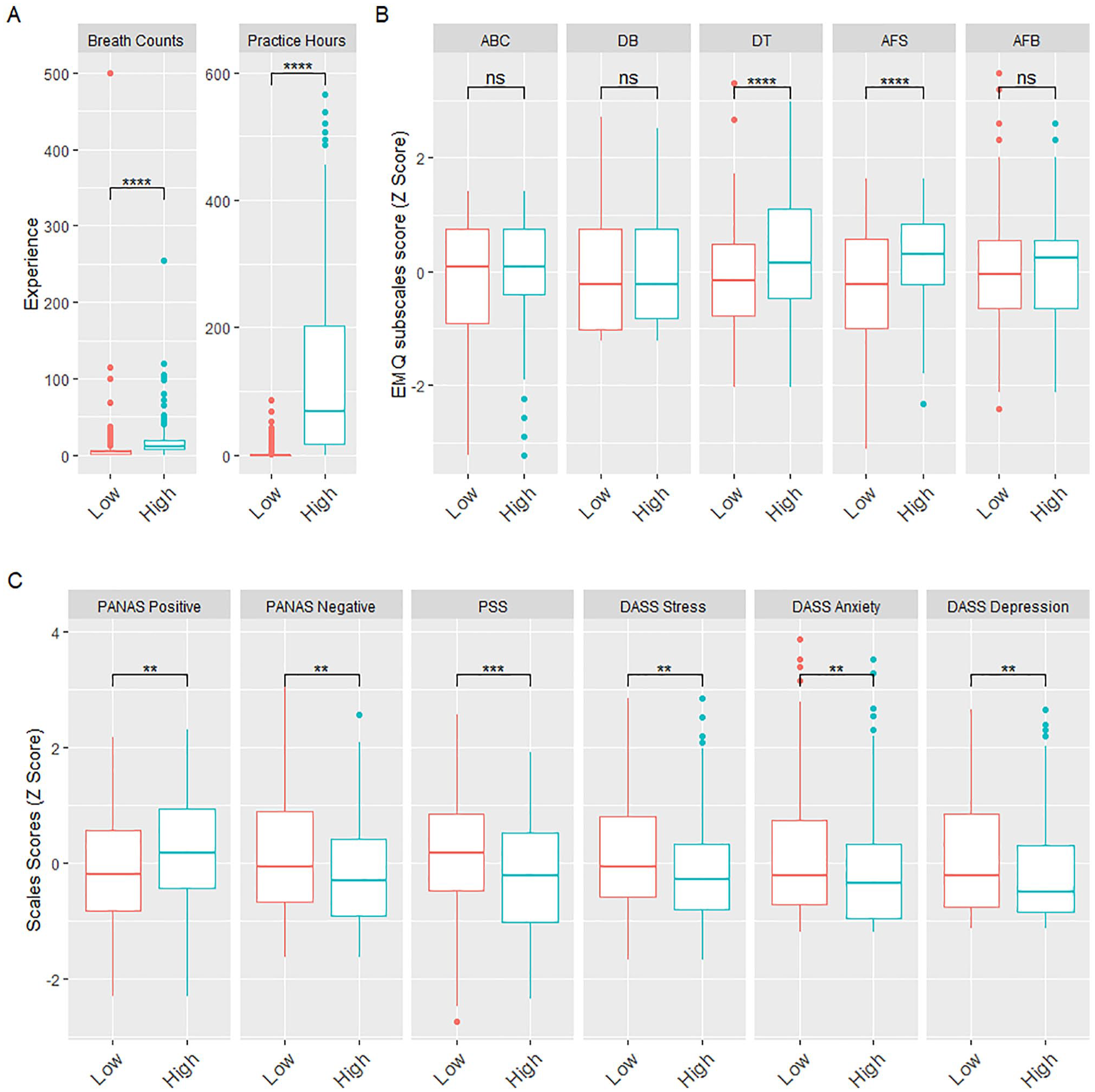
Characterization of High and Low Meditation Experience Groups.
Discussion
The aims of the current study were to evaluate the structure and the reliability of the new 25-item version of the EMQ while also evaluating convergent and discriminant evidence. EFA–CFA results support a robust structure and good internal consistencies within the five subscales’ scores. Analyses support the absence of a single latent variable of the EMQ (i.e., a global score should not be computed for the EMQ). This is aligned with the theoretical conception of EMQ. We expect that “embodied mindfulness” is trained through these five skills. Nonetheless, the five subscales’ scores of the EMQ are weakly associated and, therefore, can be considered independent. These results support that the five factors represent abilities that can be trained either independent of each other or, more likely, in a sequential way (i.e., building on each other). Therefore, a certain level of some of these abilities may be required to train others but that having one does not per se produce the other. In accordance with what was initially proposed, “embodied mindfulness” does not appear to be a personality attribute or trait but rather a set of abilities that can be cultivated through behavioral practices. Therefore, in contrast with other mindfulness scales that conceptualize mindfulness as a set of factors underlying a single latent trait/disposition (e.g., FFMQ and MAAS) or state (e.g., TMS or SMS), the EMQ conceptualizes mindfulness as a multidimensional construct with a set of independent or sequentially trained skills.
Detachment from Automatic Thinking scores were expected to be negatively related to scores of emotional disorders (see e.g., Mathews & MacLeod, 2005) and positively related to scores of mindfulness measurements which could reflect decentering (Feldman et al., 2010). This subscale’s scores were significantly correlated with all of the subscales’ scores of the DERS, with a particularly strong correlation with cognitive fusion scores. In discriminant analysis, scores of the Detachment from Automatic Thinking subscale were found to be significant predictors of all DASS subscales’ scores (i.e., stress, anxiety, and depression). These scores were also a significant predictor of meditation experience scores but only for participants with high meditation experience. In addition, scores of the Detachment from Automatic Thinking subscale predicted other mental health variables such as scores of the positive and negative subscales of the PANAS and the PSS. These results strongly support Detachment from Automatic Thinking subscale being related to automatic thinking and, therefore, to psychological symptoms and affect as well.
Attention and Awareness of Bodily Sensations intends to capture the ability to direct attention toward bodily sensations which is a central part of mindfulness practice (MBSR; Kabat-Zinn, 1982, 1990; MB-EAT, Kristeller et al., 2014; Kristeller & Hallett, 1999; MBCT, Segal et al., 2013). Thus, we expected to find significant associations with the FFMQ Observe scores and the MAIA subscale scores. In fact, the strongest correlation of Attention and Awareness of Bodily Sensations subscale’s scores was with the FFMQ Observe scores. However, they did not correlate with scores of the MAIA Not Worrying and MAIA Distracting, suggesting that this subscale measures a non-judgmental attention to bodily sensations. In discriminant validation, scores of Attention and Awareness of Bodily Sensations subscale negatively predicted scores of psychopathology-related variables. These results support that Attention and Awareness of Bodily Sensations is measuring the ability to direct non-judgmental attention to bodily sensations, regardless of the nature of the sensations (i.e., both pleasant and unpleasant sensations), which in turn positively impacts psychological symptoms.
Disconnection from the Body refers to the difficulty of sustaining attention and awareness of the body throughout time and, therefore, feeling disconnected from the body. As mentioned above, connection to the body is also reflected in the higher level of activation in the insular and somatosensorial cortex among meditators during functional magnetic resonance imaging (fMRI) studies (Chiesa et al., 2013; Hölzel et al., 2011; Lutz et al., 2008). Increasing connection to the body has been reported to reduce depression severity (de Jong et al., 2016) and improve negative affect (Füstös et al., 2012) and empathic responses (Singer et al., 2004). Discriminant evidence showed this subscale’s scores to be significant predictors of the scores of the DASS and the PANAS, decreasing PANAS positive affect’s score. Surprisingly, there were no significant differences between high and low meditative experience groups, suggesting that the effects of being disconnected from the body are independent of meditation experience. The independent effect of meditation experience and being disconnected from the body may be explained by the limited meditation experience of the participants, which was perhaps insufficient to show a clear difference between meditators with more experience from those with less experience. In addition, the negative wording of the items that were included in the final version (positive items were eliminated through analyses) did not cover the positive dimension of connection to the body, which likely undercut the potential association with meditation experience. However, evidence from convergent results analyses supports that the Disconnection with the Body subscale scores are negatively related to FFMQ Act with Awareness’ scores; therefore, this subscale can predict avoidance and impulsivity.
Awareness of the Mind-Body Connection reflects the more complex phenomena of cultivating awareness of how the mind impacts the body and vice versa. As such, it aims to measure the bidirectional mind-body connection. Previous research has found a low mind-body connection to be associated with depression (Michalak et al., 2009, 2010; Wendorff et al., 2002). However, to our surprise, scores of Awareness of the Mind-Body Connection were able to predict scores of DASS Anxiety and Stress but not Depression. In addition, its predictive power was higher for experienced meditators in comparison with the low experience group. The highest correlations of scores of Awareness of the Mind-Body Connection were with scores of MAIA emotional awareness and MAIA Noticing. No other relevant correlations were found. Altogether these results suggest that this subscale is measuring emotional awareness and its impact on the mind and body, specifically on stress and anxiety. The inability of Awareness of the Mind-Body Connection to predict depression might be related to the central role of cognitive mechanisms (such as rumination) in depression (McLaughlin & Nolen-Hoeksema, 2011; Olatunji et al., 2013), in comparison with other processes such as mind-body connection (Lo et al., 2013). Furthermore, it might require more sustained practice to cultivate this skill for individuals with low to moderate meditation experience.
Acceptance of Feelings and Bodily Sensations is probably the most difficult skill to develop (we purposefully listed it last among the five skills related to “embodied mindfulness”), as it involves exposure to unpleasant sensations and feelings (Hayes & Strosahl, 2004). Acceptance is expected to produce psychological improvements (Khoury et al., 2013; Lindsay et al., 2018; Rahl et al., 2017), most likely through emotional regulation (Blackledge & Hayes, 2001; Lindsay & Creswell, 2019). The scores of this subscale were significantly associated with scores of many of the DERS subscales and with scores of the TAS20; however, all these associations were weak. Discriminant results suggested that scores of the Acceptance of Feelings and Bodily Sensations subscale did not predict scores of DASS, PANAS, or PSS among participants with a low meditative experience. In contrast, scores of the Acceptance of Feelings and Bodily Sensations subscale significantly predicted all but scores of DASS Depression among participants with a high meditative experience. It is likely that participants without meditative experience may use other strategies than acceptance to cope with their symptoms or unpleasant feelings. Therefore, Acceptance of Feelings and Bodily Sensations is properly measured by the EMQ and is sensitive to meditative experience.
In general terms, convergent results showed that three EMQ subscales (Attention and Awareness of Feelings and Bodily Sensations, Detachment from Automatic Thinking, and Disconnection from the Body) capture the key elements usually measured when assessing mindfulness (i.e., using other scales such as FFMQ and MAAS). In addition, the EMQ subscales incorporate two more dimensions (Acceptance of Feelings and Bodily Sensations and Awareness of the Mind-Body Connection), which are aspects often ignored in measuring mindfulness. Therefore, these aspects can extend the conceptualization of mindfulness to integrate the notion of embodiment. The subscale whose scores presented the lowest association with scores of the classic measures of mindfulness was Awareness of the Mind-Body Connection, which presented a high association with the MAIA Emotional awareness subscale. Despite its low associations, scores of this subscale presented convergent evidence that it is measuring the ability to notice bodily sensations and to relate them to emotional events.
Discriminant results showed that the EMQ subscales can predict scores of measures of psychological symptoms (e.g., scores of depression, anxiety, and stress), scores of positive and negative emotions, and total number of hours of meditative practice, explaining between 20% and 30% of the total variance of the scores on these measures. When participants were divided into two groups according to their meditation experience, the group with more meditation experience showed lower psychological symptoms and higher positive emotions. In addition, in the group with high meditation experience, the EMQ subscales’ scores explained 24% of the variance for meditation experience, compared with only 3% of the variance for the low meditation experience group. Moreover, two of the EMQ subscales’ scores (Detachment from Automatic Thinking and Attention and Awareness of Feelings and Bodily Sensations) showed sensitivity to meditative experience, suggesting, therefore, an important change in its prediction pattern according to the level of the meditative experience of participants.
Given that we expected that the EMQ subscales would be helpful in assessing interventions and patient follow-up, we conducted a brief 6-week mindfulness-based intervention (Study 3) to evaluate how EMQ subscales change following the intervention in comparison with other mindfulness measures.
Study 3: Following an Online Mindfulness and Compassion Training Program
Method
Participants
Twenty-seven counselors-in-training (i.e., graduate students in counseling programs) were recruited from Canadian universities across Canada using social media advertisements (e.g., Facebook and Lab website), emails sent via university resources (e.g., program Listservs), and brief presentations. Four participants withdrew before the end of the study, leaving 23 participants (Female = 22, Mage = 29.04, SDage = 6.46). Most participants identified as White (n = 13) and spoke English as their mother tongue (n = 18). While they had prior experience practicing mindfulness (n = 19) and had some formal mindfulness training (n = 14), they described mindfulness to have little to no role or importance in their daily life at baseline (n = 12). All participants were offered pro-rated monetary compensation to a maximum of US$100 each.
Mindfulness and Compassion Training Program
The program aimed to provide support and increase the tolerance to ambiguity among novice in-training counselors through mindfulness and compassion. The program included six weekly 90-minute online sessions (via Zoom) due to the COVID pandemic. The program included components related to tolerating ambiguity in life and clinical work, emotions and their regulation, mindfulness in intrapersonal and interpersonal contexts, compassion toward oneself and others, self-transcendence through the connection with the external environment (including nature and animals), and gratitude in times of transition and change. The program was partially based on the embodied and embedded mindfulness and compassion framework (EEMCF; Khoury, 2018, 2019; Khoury & Dionne, 2020; Khoury et al., 2017, 2019, 2020). Each session comprised of didactic, discursive, and practical components that were designed specifically for novice therapists. Each session included at least two different meditation practices such that participants meditated between 15 and 25 minutes per session. Between sessions, participants were encouraged but not required to engage in daily at-home mindfulness exercises (e.g., guided meditations or meditative walks). A total of three groups were held with two groups in the fall of 2020 (n = 6 and n = 8) and one in the winter of 2021 (n = 9). All the groups were facilitated by the fourth author, who has 4 years of training in clinical work and group facilitation as well as 4 years of training in mindfulness research and practice. A complete description of the program is available in Spinelli et al. (2021).
Procedure
The study was approved by the Research Ethics Board Office at McGill University. All data were collected online using LimeSurvey. Participants gave informed consent prior to starting the study and completed several measures including a sociodemographic questionnaire, the measure under validation (i.e., EMQ), the FFMQ, and the DASS-21. The latter two measures are included to provide a comparison with the EMQ and to show the impact of the intervention on participants’ mental health, respectively.
Data Analysis
Subscale and total scores were calculated such that only participants who completed all items within each variable were included. Missing data were omitted using listwise deletion, and there were no univariate outliers (±3.5 SD). Normality was tested using the Shapiro–Wilks’s test, and outcomes were inconsistent in conforming to the normality assumption. This finding is unsurprising as the outcomes being measured are trainable skills or distress measures that can produce skewed distributions. Thus, we elected to use a non-parametric approach and compared post-training to baseline using Wilcoxon signed-rank tests. Nonparametric effect sizes were calculated using rank-biserial correlation (r). A small effect size is 0.1, medium is 0.3, and a large is 0.5. All analyses were conducted using IBM SPSS (version 27).
Results
Prior to participating in the training program, most participants reported practicing mindfulness less than once per week (n = 12). During the program, participants were asked to report their daily mindfulness practice. On average, participants practiced 9.85 minutes/day (SD = 10.93, range = 2.22 to 48.89). Participants reported engaging in various mindfulness meditations (e.g., breathing, body scan, and gratitude), self-compassion-based practices (e.g., loving-kindness and soothing touch), movement-based meditations (e.g., walking mediation and yoga), and informal practices (e.g., while driving or brushing their teeth).
Scores on all three instruments (i.e., DASS-21, FFMQ, and EMQ) presented significant results in at least one of their subscale scores (Table 9). In the case of the DASS-21, only stress scores were significant. The change in stress may be attributed to changes in mindfulness skills. FFMQ subscale scores presented significant results for most of its subscale scores except for the Describe facet. The highest effect size was for Observe scores (r = .42), while the remaining scores were close to .3. Regarding the EMQ subscale scores, the Detachment from Automatic Thinking subscale showed the largest effect size (r = .46), followed by scores of Attention and Awareness of Feelings and Bodily Sensations subscales (r = .29). The changes in the scores of the remaining subscales were not significant.
Results of Pilot Study Evaluating the Change in Embodied Mindfulness Questionnaire (EMQ) After a Mindfulness Intervention.
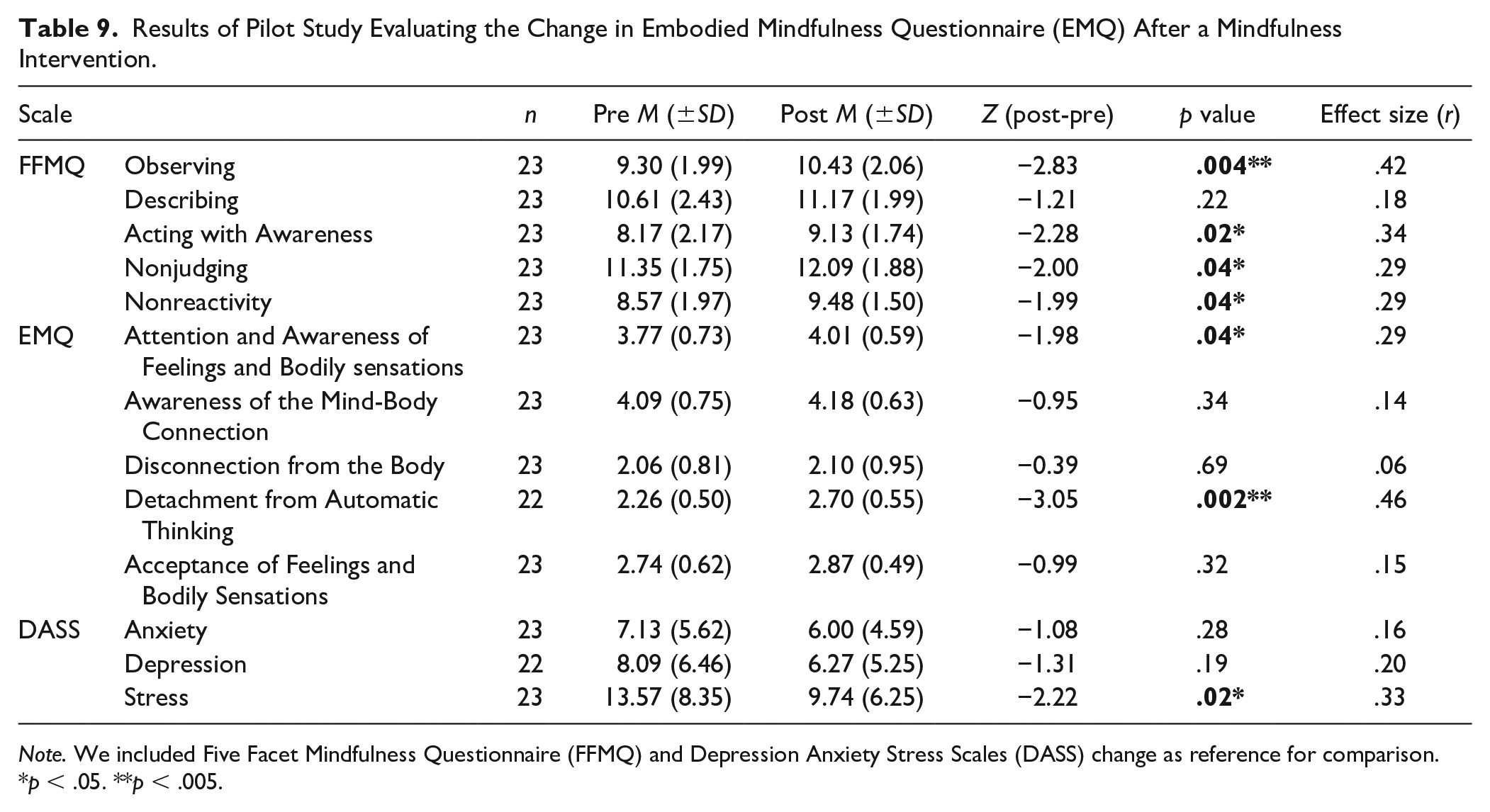
Note. We included Five Facet Mindfulness Questionnaire (FFMQ) and Depression Anxiety Stress Scales (DASS) change as reference for comparison.
p < .05. **p < .005.
Discussion
The aim of the current study was to assess the EMQ subscales’ scores changes following a 6-week mindfulness-based intervention. Overall, results suggest that two of the EMQ subscales’ scores (i.e., Detachment from Automatic Thinking and Attention and Awareness of Feelings and Bodily Sensations) were sensitive to a 6-week online mindfulness intervention (i.e., increased significantly following the intervention), while the other three subscales’ scores (i.e., connection with the body, awareness of the mind-body connection, and acceptance of feelings and bodily sensations) did not change significantly following the intervention. Scores of Detachment from Automatic Thinking subscale showed a large effect size and scores of Attention and Awareness of Feelings and Bodily Sensations subscales had a moderate effect size, suggesting that both skills may lead to improvement in mental health.
The obtained results were not surprising because (a) the two subscales’ scores that were sensitive to change following the intervention summarize some of the core and basic mindfulness aspects measured through other mindfulness scales (e.g., FFMQ) and (b) EMQ subscales were designed as a set of skills that build on each other, rather than a personality disposition or trait. The dimensions are not necessarily equally cultivated at a time point such that a participant can score high on the first two subscales while scoring low on the remaining three subscales, depending upon their level of mindfulness training. As previously noted, the order of the subscales in the EMQ was intended to reflect the proposed level of difficulty in cultivating the different skills. Results from the current study were aligned with our hypothesis about the order of cultivating the skills portrayed in the five subscales. The first EMQ subscale (Detachment from Automatic Thinking) was also the scale with the highest effect size for the pilot intervention, presumably because it was the easiest skill to cultivate. Following it was the second subscale (Attention and Awareness of Feelings and Bodily Sensations) which had more moderate effect sizes. In the same line, results from Study 2 suggest that scores of these two subscales were also the most sensitive to meditation even for participants with limited meditation experience.
Therefore, our interpretation of the results from the pilot study is that the three subscales, which are relevant to the embodiment and acceptance facets of the EMQ, might require additional training and practice to become significant and therefore influence other outcomes. This pilot study actually only included a total of 9 hours during the six online sessions, with an average of 20 minutes of meditation per session and 10 minutes of daily home practice (which totally cumulates to around 8 hours of meditation during the 6 weeks including the meditation practices in-session). This amount of training/practice constitutes a very lose dose of mindfulness training, if compared with other standard mindfulness-based programs, such as MBSR (Kabat-Zinn, 1982, 1990) or MBCT (Segal et al., 2013) which include more than an hour of meditation training per session (for 8 weekly 2.5-hour sessions) and recommend 30 to 45 minutes of daily meditation practice at home during the 8 weeks program in addition to a half-day meditation retreat (i.e., average total meditation training/practice of 36–48 hours). In addition, the program was offered online (due to the COVID-19 pandemic), which might have limited the training of the embodied components due to physical distance and absence of direct contact with other participants and with the facilitator. Moreover, the training program included other objectives besides mindfulness training, for example, cultivating compassion, and tolerance toward ambiguity in the trainees’ clinical work. As such, we conclude that the most basic EMQ skills were sensitive to a brief online intervention and that these results were expected, given the theoretical foundations of EMQ.
General Discussion
The purpose of the current article is to present the development and validation of a new questionnaire (EMQ) that operationalizes the notion of “embodied mindfulness” by grounding it into five different factors (or dimensions): (a) Detachment from Automatic Thinking, (b) Attention and Awareness of Feelings and Bodily Sensations, (c) Connection with the Body, (d) Awareness of the Mind-Body Connection, and (e) Acceptance (i.e., non-avoidance) of Feelings and Bodily Sensations.
The development and validation of the EMQ included four main phases: (a) generating a pool of items that are aligned with each of the five theoretically proposed dimensions and vetting them by (1) a panel of eight graduate students and (2) a group of 11 experts in the field, yielding an initial version of 48 items (Design and Development of EMQ); (b) evaluating EMQ structure and internal consistency using the sample of 407 participants which led to a new version of the questionnaire with 25 items (5 items per dimension; Study 1); (c) evaluating EMQ structure, internal consistency, and convergent and discriminant evidence using the second sample of 1,191 participants, which led to the final version of the questionnaire with 24 items (Study 2); and (d) evaluating the use of EMQ in measuring changes following a mindfulness-based intervention (Study 3).
Results from the three studies support the five dimensions of the EMQ while suggesting the absence of a single latent variable that represents the concept of “embodied mindfulness.” This finding is not surprising as the EMQ subscales were developed as a set of skills/abilities that can be cultivated sequentially (based on each other) through mindfulness/meditation training and practice. In line with that, results suggested differences among the subscales of the EMQ in terms of necessary training to show significant differences and degree of sensitivity to meditation practice. According to outcomes from Studies 2 and 3, the two first subscales’ scores of EMQ (i.e., Detachment from Automatic Thinking and Attention and Awareness of Feelings and Bodily Sensations) were the most sensitive to mindfulness training and meditation practice among novice and non—expert meditators. The scores of the third subscale (i.e., Disconnection from the Body) did not show significant change following the mindfulness and compassion program but were sensitive to the meditation experience. The scores of the last two subscales (i.e., Awareness of the Mind-Body Connection and Acceptance of Feelings and Bodily Sensations) showed lower sensitivity to mindfulness training and meditation experience among non-expert meditators and, therefore, might require longer and more sustaining training and practice to present significant changes.
In addition, previous mindfulness measures that included awareness and acceptance did not find strong correlations between these two factors among naïve meditators and therefore did not yield to a singular global latent variable (e.g., Philadelphia Mindfulness Scale; Cardaciotto et al., 2008). Moreover, other scales that measured interoceptive body awareness did not yield to a single latent variable when tested with naïve community samples (e.g., Body Mindfulness Questionnaire, Burg et al., 2017; Multidimensional Assessment of Interoceptive Awareness, Mehling et al., 2012). Potential explanations of such phenomenon can be the lack of body-based training among naïve participants, or also cultural factors as awareness of the body has been consistently minimized and disregarded in the West, while adopting a cartesian dualistic philosophy and a certain disembodied style of life (Lakoff & Johnson, 1999; Leder, 1990; Mehling et al., 2009). This is also true in the context of scientific research including in measuring mindfulness (see, for example, Khoury et al., 2017, 2019). It is not surprising, therefore, that concepts/practices such as body connection and mind-body connection can be challenging and difficult to cultivate in a naïve Western population.
Overall, results suggest that the three first subscales of EMQ (Attention and Awareness of Feelings and Bodily Sensations, Detachment from Automatic Thinking, and Disconnection from the Body) may summarize traditional mindfulness aspects measured through other standard mindfulness instruments (e.g., FFMQ and MAAS among others), with the first two subscales being the easier to cultivate. The last two subscales (Awareness of the Mind-Body Connection and Acceptance of Feelings and Bodily Sensations) extend the conceptualization of mindfulness to integrate the notion and practices related to embodiment and, as result, may require a higher level of training to be cultivated and can be useful among expert meditators.
Limitations
The presented studies have many limitations. First, participants in the three study samples were overwhelmingly female. This bias is common in mindfulness research, especially when recruitment takes place mainly using social media (such as Facebook). The lack of male participants might limit the use of the EMQ subscales for males, despite the absence of any observed differences between males and females in all the samples. In addition, the majority of participants were English-speaking Canadians (as the study was conducted in Canada), which might not fully generalize the EMQ to a non-Canadian sample. Moreover, most participants had limited meditation experience, which might have limited our results as the EMQ subscales were developed to capture different levels of mindfulness training and experience. Therefore, participants with higher meditation experience might score high on all the subscales, which may have substantially increased the correlations among the five subscales. As result, there may be convergence of the subscales into a single global latent variable among highly experienced meditators. In other words, “Embodied mindfulness” may emerge as a singular concept once skills are trained enough to establish such a trait. It is strongly warranted to test this hypothesis in future studies. Second, Study 2 only used two standard measures of mindfulness (FFMQ and MAAS) in establishing the convergent evidence of EMQ, and other relevant measures (e.g., KIMS, PHMS, and FMI) were not included. Including these measures might provide more precise data regarding the convergent aspects of the EMQ and is recommended in future studies. Third, items that were part of the final version were worded in a similar direction (i.e., either positive or negative) for each subscale, which might have limited the full potential of the subscales. Fourth, rest–retest reliability across time was not evaluated in the current studies. Finally, Study 3 was a pilot intervention with limited duration with a low dose of mindfulness training and practice, had a low number of participants, and targeted a specific population (counselors-in-training), which might have limited the impact of the intervention on the EMQ subscales. Robust RCTs with a longer and sustained mindfulness training and home practice (such as MBSR or MBCT) and with a larger number of community-based participants will be highly warranted to establish the use and limitations of the EMQ subscales in measuring changes following a mindfulness-based intervention.
Implications
The EMQ is the first questionnaire that operationalizes embodiment within mindfulness, with important theoretical and practical implications. On the theoretical level, it integrates the complex theory of embodiment when measuring mindfulness, making the body, and mind-body interaction, central in the definition and measurement of mindfulness. On the practical level, by measuring mindfulness as a set of skills/abilities with a different level of difficulty and requiring a different degree of training and practice, the EMQ subscales may allow enhancing mindfulness-based programs and facilitate the integration of embodiment in mindfulness training. The call to further include the body in mindfulness training and specifically include embodiment was made by researchers and clinicians in the field (see e.g., Michalak et al., 2012). In addition, the sensitivity of some of the EMQ subscales to the meditative experience of participants can be very useful in studying the influence of meditation experience on the processes involved in mindfulness and on measures of psychological symptoms, emotions, and well-being. Finally, although the current article provides an initial validation of the EMQ subscales and their potential theoretical and practical use, more research is highly warranted to further establish the validity of the EMQ subscales and their usefulness in the fields of mindfulness and embodiment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author received internal funding from McGill University.