
Abstract
Driving is challenging for older adults, especially those with cognitive impairments. This paper systematically reviewed 39 peer-reviewed studies to examine the impact of cognitive deficits on older adults’ driving abilities, focusing on the discussion of neuropsychological assessments including Trail Making Tests, Useful Field of View, Maze Test, and Mini-Mental Status Exam. The study proposed the concept of Road Safety Cognitive Health, which encompasses the cognitive processes crucial for safe driving, aiming to inform future driver training, licensing regulations, roadway designs, and vehicle technology innovations. Concussively, this research advances understanding of road safety challenges for cognitively impaired older adults and advocates for an integrative approach to ensure their driving safety.
Introduction
In recent years, a significant increase in motor vehicle ownership among older adults over 65 to 75 in the United States led elderly individuals to be more active on the road than ever (US Census Bureau, 2023; Zebra, 2023). Older drivers often face challenges driving in complex and unpredicted traffic situations, causing injuries or even fatalities. Age-related cognitive declines are common among older drivers aged over 65, making driving tasks challenging due to the high demands in cognitive functioning (Karthaus & Falkenstein, 2016; Older Adult Driver Safety, 2022).
Cognitive impairments (CI) are classified into three levels: mild, moderate, or severe (Cognitive Impairment | Johns Hopkins Psychiatry Guide, n.d.). Common forms of CI include mild cognitive impairment (MCI), Alzheimer’s disease, mixed dementias, and Parkinson’s disease (PD) (Alzheimer’s Association, 2018). Specifically, Alzheimer’s (AD) is the most prevalent cause of dementia (Scheltens et al., 2016), with MCI serving as an early stage between normal aging and more advanced dementia (Gauthier et al., 2006; Petersen, 2016). Declines of cognitive domains in attention, executive function, memory, language, and perceptual-motor skills potentially lead to poorer performance in complex driving tasks.
Currently, clinical diagnoses and office-setting cognitive evaluations are critical methods in diagnosing the prevalence of cognitive impairments. Biomarkers have become highly accurate tools for detecting cognitive impairments among elders, such as Cerebrospinal fluid (CSF) markers and magnetic resonance imaging (MRI) (Brys et al., 2009; De Leon et al., 2006). Cognitive batteries and screening instruments are also critical in CI diagnosis. Tools such as Mini-Mental State Exam (MMSE), Montreal Cognitive Assessment (MoCA), Mini-Cog, Global Deterioration Scale (GDS), and Clinical Dementia Rating (CDR) with different cut-off scores and rating ranges have proven effective (Holsinger et al., 2012). Driving behaviors are assessed by on-road tests, naturalistic studies, driving simulator experiments, and self-report questionnaires, combined with neuropsychological testing, to ensure a comprehensive evaluation of older adults’ capability to drive safely.
This research introduced the concept of “Road Safety Cognitive Health,” defined as the suite of cognitive processes crucial for maintaining safe driving practices and effectively managing on-road situations, to evaluate the effects of neuropsychological assessments in identifying the risk of safety. Systematic reviews and meta-analyses are conducted to examine the relationship of cognitive abilities, driving performance, and neuropsychological assessment methods in older adults with cognitive impairments. Specifically, this study aims to: (a) evaluate the effects of aging-related cognitive impairments in domains of attention and processing speed, memory, visuospatial, and executive function on driving behaviors; (b) analyze the effectiveness of neuropsychological assessments in determining older adults’ deficits in various cognitive domains; and (c) develop an integrated framework that uses cognitive test to predict driving performance, informing road safety interventions and policies.
Methods
The PRISMA Statements and Methods 2020 version (Page et al., 2021) was applied in this systematic review. Eligible studies should meet the following inclusion criteria: (a) peer-reviewed literature studies in English published between January 1st, 2010, and December 10th, 2023, (b) participants were older adults with at least one cognitive condition such as mild cognitive impairment (MCI), Alzheimer’s disease (AD), or any forms of mild or moderate dementia, (c) include one form of driving assessment, such as naturalistic driving studies, on-road driving tests, driving simulators, or driving-related questionnaires, (d) include at least one cognitive or neurological battery test to assess participants’ cognitive abilities. PubMed and Google Scholar were the main resources to conduct a comprehensive literature search. Additionally, A combination of keywords and MeSH terms are created to include as many published works and literature as possible and minimize potential bias in the study selections. Search terms include “older adults,” “driving,” “mild cognitive impairments,” “Alzheimer’s,” “dementia,” “driving assessment,” and “cognitive assessment.” Boolean operators (AND, OR) were employed to expand or narrow the search.
The study selection process commenced on January 5th, 2024, and concluded on February 2nd, 2024. Two independent reviewers participated in the study screening and selection process. Reviewers first screened the titles and abstracts of identified records by searching keywords in the proposed literature database. Next, records that pass the initial stage will go through a full-text screening to ensure compliance with all inclusion criteria.
A standardized data extraction form was developed to collect qualitative and quantitative studies. The Useful Field of View (divided attention test), Trail-Making Test (A/B), Maze Test, and Mini-Mental Status Exam were selected across studies for meta-analyses to test the batteries’ accuracy and effectiveness. Effect sizes were measured using the outcomes on a continuous scale, supposing that each study evaluated the effect of a cognitive measure by comparing the mean of a group of cognitively impaired (CI) individuals with the mean of a group of cognitively normal (CN) individuals (Hedges & Tipton, 2010) . Forest plots were also performed to provide an overview of effect size estimates across studies and their uncertainties.
Results
Figure 1 PRISMA Flowchart demonstrates the study selection results. A total of 784 records were identified. Upon removing 236 duplicates, 548 records underwent title screening, followed by a brief review of abstracts of 179 records, which further filtered out 438 studies due to the absence of driving assessments and/or cognitive evaluations (n = 405) and non-peer-reviewed or non-English studies (n = 33). Full-text reviews of the remaining 110 records led to the exclusion of 71 studies for reasons such as a focus on biomarkers (n = 10) and not meeting population criteria (n = 48). As a result, 39 studies were included in qualitative synthesis, with 15 selected for the meta-analyses.
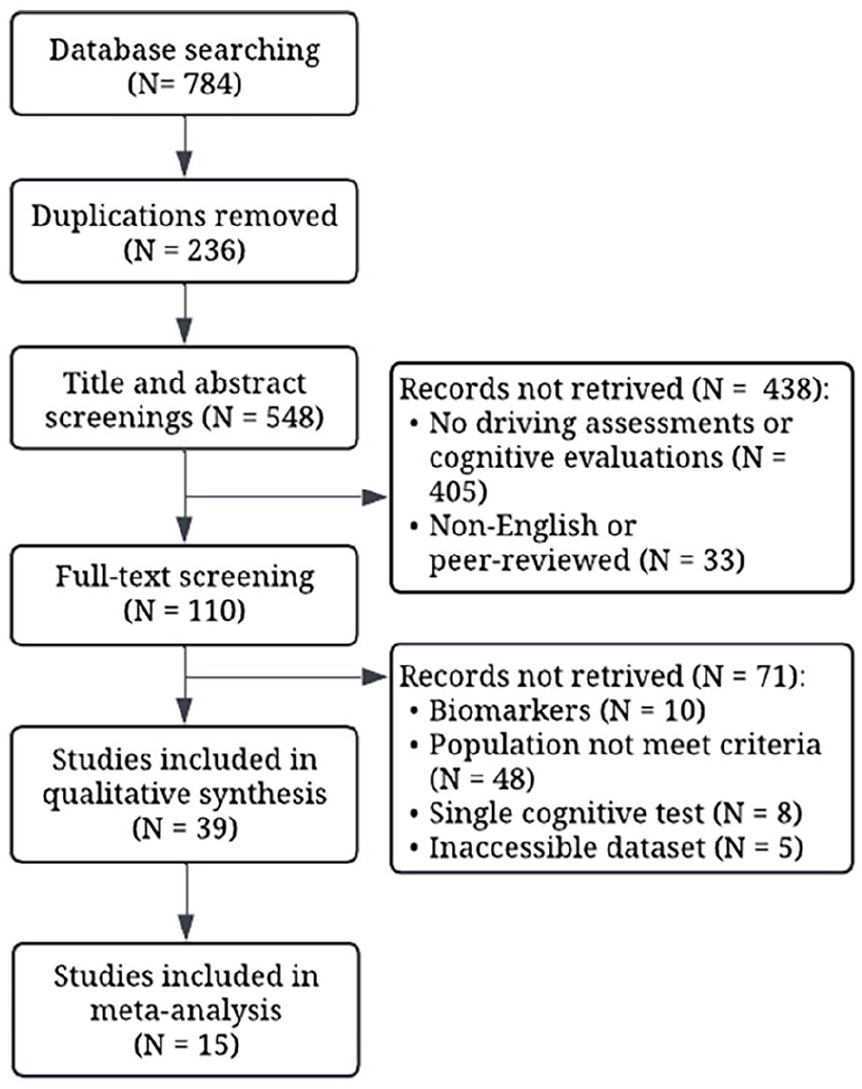
PRISMA flowchart.
Table 1 provides a partial overview of the standardized form from a selection of 11 studies. Overall, participants from 39 studies contained cognitively normal individuals and older drivers with cognitive impairments including MCI, AD, and PD. The sample sizes varied, ranging from small groups to larger cohorts. The majority of methodologies used in the studies are cross-sectional and observational (n = 32). Only a small number of studies (n = 6) adopted longitudinal designs to study driving restriction and self-regulation behaviors. Various cognitive test batteries are used. Common examinations are MMSE, Trail Making Tests (Parts A and B), and Useful Field of View (4 subs). The driving assessments involve on-road tests (ORT) with naturalistic recording, driving simulator experiments, and self-report questionnaires on driving habits. The driving outcome measures contain a broad spectrum of performance indicators, including navigation and secondary task performance, reaction times, speed variability, and safety-related errors. Additionally, numerous on-road studies have used pass/fail outcome measures with subjective rating scales, such as driving scores. Various studies also carried out analyses of maneuver behaviors related to turns and lane changes, self-regulation behaviors, daily driving patterns, and occurrences of safety-critical events.
Sample Standardized Form.
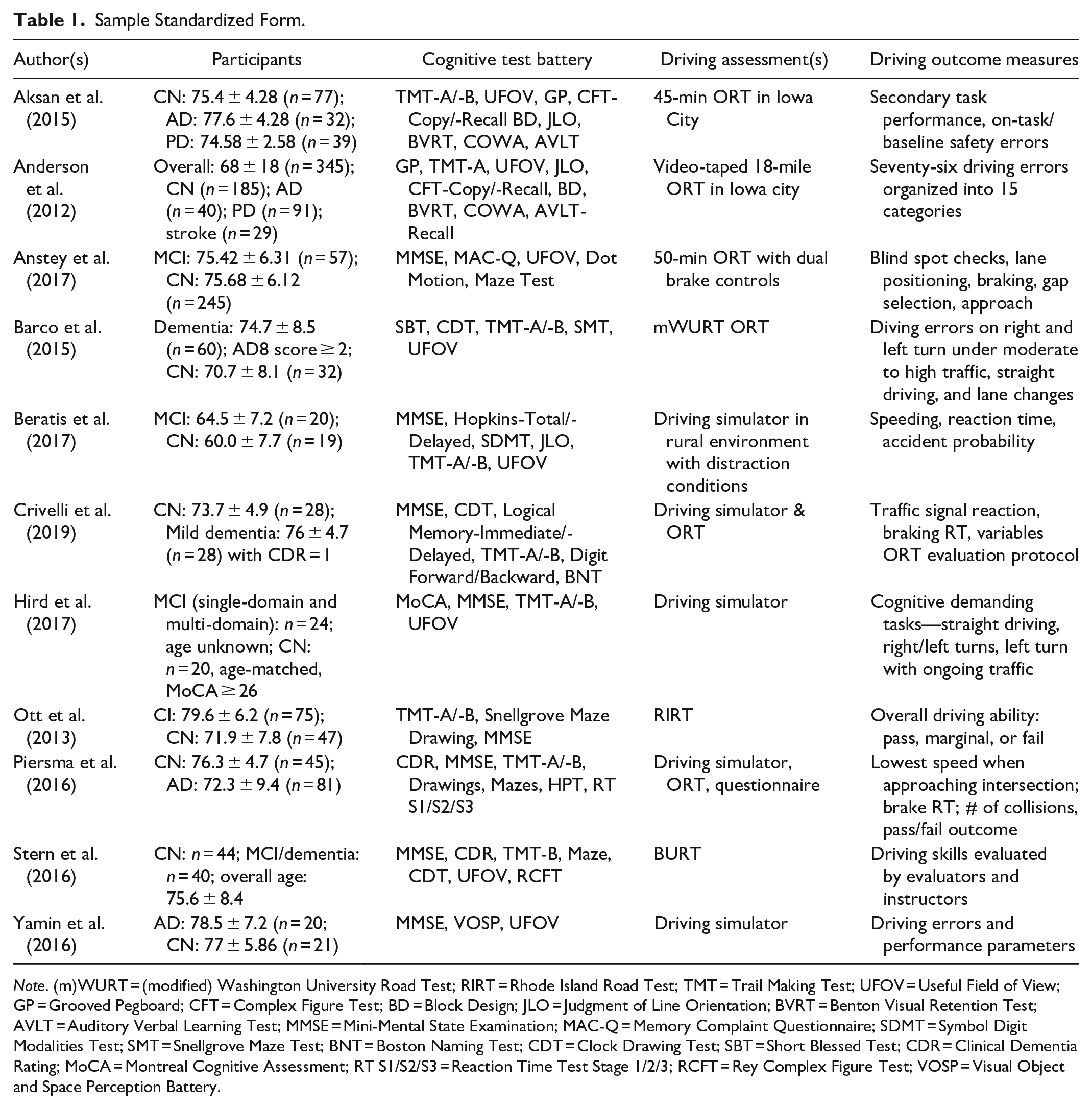
Note. (m)WURT = (modified) Washington University Road Test; RIRT = Rhode Island Road Test; TMT = Trail Making Test; UFOV = Useful Field of View; GP = Grooved Pegboard; CFT = Complex Figure Test; BD = Block Design; JLO = Judgment of Line Orientation; BVRT = Benton Visual Retention Test; AVLT = Auditory Verbal Learning Test; MMSE = Mini-Mental State Examination; MAC-Q = Memory Complaint Questionnaire; SDMT = Symbol Digit Modalities Test; SMT = Snellgrove Maze Test; BNT = Boston Naming Test; CDT = Clock Drawing Test; SBT = Short Blessed Test; CDR = Clinical Dementia Rating; MoCA = Montreal Cognitive Assessment; RT S1/S2/S3 = Reaction Time Test Stage 1/2/3; RCFT = Rey Complex Figure Test; VOSP = Visual Object and Space Perception Battery.
Cognitive Assessments
Attention and Processing Speed
The current study has found that TMT-A tests are frequently used to screen for dementia due to the high sensitivity to cognitive decline and measure visual search and psychomotor speed through completion time and error scores (Bliokas et al., 2011; Davis et al., 2018; Ott et al., 2013). TMT-A completion time is a significant predictor of driving errors, driving restrictions, road test scores, and reaction times in traffic situations such as braking reactions and reactions to traffic signals, and failure of road tests, with slower execution times indicating driving restrictions among older adults (Crivelli et al., 2019; Hird et al., 2017; Marie Dit Asse et al., 2014).
Useful Field of View (UFOV) is widely applied in driving studies to assess cognitively impaired elders’ driving fitness by examining visual processing speed, divided attention, and selective attention (Stern et al., 2016; Yamin et al., 2016). MCI and AD patients tend to score worse on the selective attention subset, particularly under demanding driving conditions with distractions (Beratis et al., 2017). Lower UFOV scores are associated with higher driving errors, increased risk of vehicle crashes, and poorer collision detection (Hird et al., 2017; Stern et al., 2016; Vaux et al., 2010).
Executive Function
Trail Making Test Part B (TMT-B) is used to assess attentional set-shifting as part of executive functioning and effectively predicts on-road driving performance (Aksan et al., 2015). Longer completion times and errors on the TMT-B are correlated with greater driving difficulties, accidental potential, and more crashes for both cognitively normal and impaired elders (Cross et al., 2017; Peng et al., 2021; Venkatesan et al., 2018). TMT-B performance is more highly correlated with actual driving behavior, such as the use of turn signals, compared to other cognitive assessments like MMSE (Ott et al., 2013; Peng et al., 2021).
The Maze Test, including the Snellgrove Maze Task (SMT) and computerized mazes, evaluates older adults’ navigational skills (Ott et al., 2013). Maze tests are notable for predicting performance errors, fitness to drive, and at-risk driving status (Davis et al., 2018; Stern et al., 2016; Toepper et al., 2021), and have been integrated with other predictors such as CDT, MMSE, TMT-A/-B, and UFOV to enhance driving competence assessments (Stern et al., 2016; Ott et al., 2013; Piersma et al., 2016).
Memory and Visuospatial Skills
The Benton Visual Retention Test (BVRT) and Complex Figure Test (CFT)-Recall assess immediate visual working memory. On-road driving studies show that visuospatial construction tests (e.g., CFT-Copy) can predict baseline safety errors, and memory is associated with navigation-related secondary task performance (e.g., lane observation and speed control; Aksan et al., 2015). Also, Anderson et al. (2012) mentioned that CFT-Recall and BVRT showed the strongest connections with on-the-road performance, which aligns with Bliokas et al. (2011)’s theory that CFT-Copy can effectively predict the pass/fail criterion as an independent factor.
Meta-Analyses and Effect Sizes
The meta-analyses show that TMT-A/B, UFOV (divided attention), Maze Test, and MMSE are valid in detecting cognitive impairments in older drivers with AD and MCI. Specifically, AD and MCI groups take longer to complete TMT-A and TMT-B tests than healthy control groups. Similarly, maze test completion times are significantly longer in the AD group compared to the control group. Also, cognitively impaired older adults have significantly lower MMSE scores, with AD having a more substantial effect (Figure 2a). However, specific limitations should be considered when operating the tests. For instance, UFOV effect size results showed a wide confidence interval and high heterogeneity, indicating a need for cautious interpretation of such test as the differences in completion times are nonsignificant between AD and MCI groups.
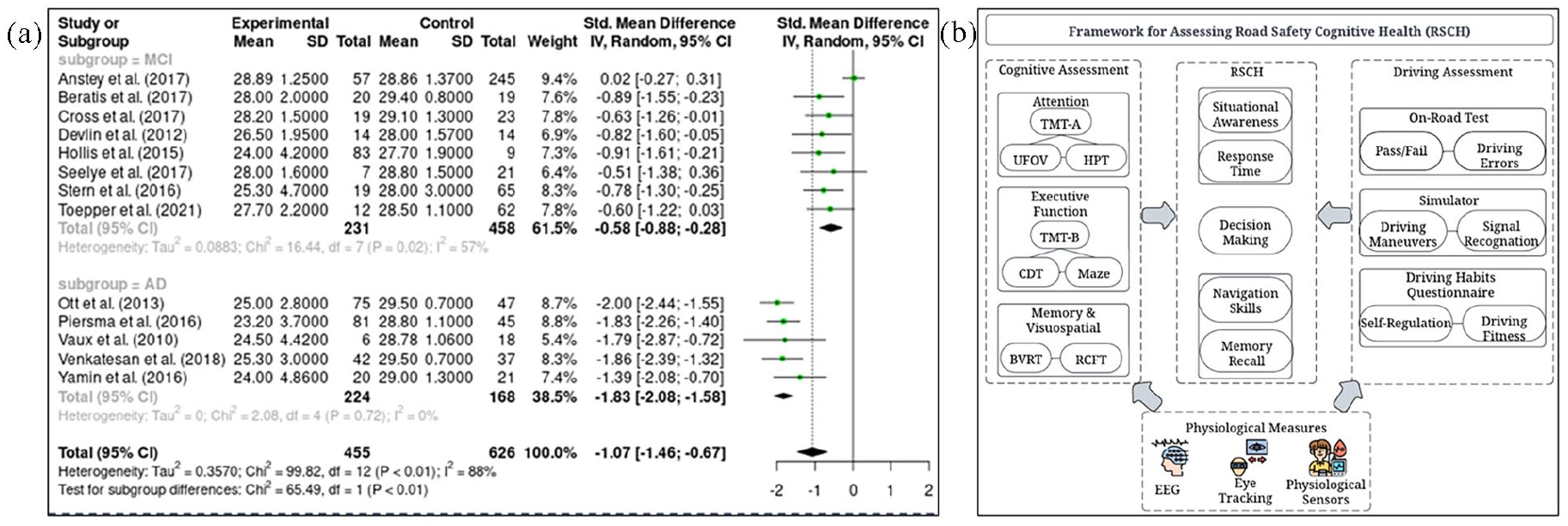
(a) Sample meta-analysis—MMSE; (b) Road safety cognitive health framework.
Driving Assessments
Driving Fitness
Aging is associated with increased safety errors and unsafe driving acts, regardless of elders’ neurological conditions (Aksan et al., 2015; Hird et al., 2017; Hotta et al., 2018). Specific maneuvers on uncontrolled intersections, two traffic light-controlled intersections, two stop signs, and roundabouts, are reported to be challenging for older drivers (Devlin et al., 2012; Eramudugolla et al., 2021). Compared to cognitively normal older individuals, patients with MCI and AD make more errors in lane maintenance and turning (Barco et al., 2015; Crivelli et al., 2019; Davis et al., 2018; Hird et al., 2017), which are likely due to impaired mental flexibility (Etienne et al., 2013). Moreover, AD drivers often exceed the posted speed limit significantly more often than the CN group but drive significantly slower when they are in a hurry (Piersma et al., 2016; Yamin et al., 2016). ORT results indicated that older adults who failed the road test have greater cognitive impairment (higher AD8 scores) than those who passed (Barco et al., 2015), which is consistent with Anstey et al. (2017) and Fuermaier et al. (2017)’s theory that MCI is a threat to safe driving and have a lower average safety rating. In addition, MCI patients show larger reaction times to unexpected driving events and respond slower in simple driving reaction tests (Beratis et al., 2017; Peng et al., 2021).
Driving Restriction and Self-Regulation
The longitudinal studies for exploring elders’ driving restrictions typically last from 6 months to a maximum of 10 years. Follow-up interviews are often compared with the baseline answers from driving questionnaires to examine the changes in driving habits or behaviors over time. Results from studies showed that MCI elders can recognize their declines in cognitive abilities and subsequently self-regulate their driving (Feng et al., 2021), while PD and AD patients tend to restrict their driving between 4- and 10-year follow-ups (Marie Dit Asse et al., 2014). Seelye et al. (2017)’ naturalistic data and self-report driving habits questionnaire results further confirm that a reducing trend of daily driving is significant among MCI patients, who showed less day-to-day fluctuations in their driving habits over 6 months.
Road Safety Cognitive Health Framework
The Road Safety Cognitive Health (RSCH) framework systematically evaluates the relationships between cognitive functions in attention, executive function, memory, and visuospatial domains with their corresponding cognitive assessments and performance in driving-related tasks with related driving outcomes (Figure 2b). This framework aims to identify potential areas of concern in older adults’ driving abilities and propose interventions that could enhance road safety from traffic safety perspectives. A critical feature of this framework is the integration of physiological measures like electroencephalography (EEG), eye tracking, and physiological sensors, providing additional layers of data to assess cognitive abilities in driving studies.
Discussion
Physiological sensors are crucial in objectively assessing pain by measuring responses such as pupillary changes, heart rate variability, and autonomic signals, combined with algorithms and neural networks, offering precise evaluations of pain levels in both clinical and experimental settings (Lin et al., 2022; Moscato et al., 2023; Wang et al., 2022; Zhu et al., 2023). Additionally, physiological features are applied in driving studies to monitor drivers’ cognitive and emotional states, including anger, distractions, and fatigue. Co-PI’s studies have proven their effectiveness in detecting changes in attention, stress, and alertness (Cai et al., 2012; Wan et al., 2019; Wang et al., 2021; Xu & Lin, 2018; Zhu et al., 2022). For example, electroencephalography (EEG) and Electrodermal activity (EDA), along with drivers’ behavioral responses from the multidimensional driving style inventory (MDSI), can be used to evaluate risky and safe behaviors in hazardous driving scenarios (Liang & Lin, 2018). Overall, numerous studies have highlighted the significant potential of using physiological sensors to explore driving behaviors, which could be further extended to older adult participants to assess driving fitness, particularly as it may be affected by their declining cognitive abilities.
The Road Safety Cognitive Health framework aligns with the capabilities of the Driver-Vehicle-Environment (DVE) simulation system, proposed by the Co-PI. Specifically, the DVE simulation system is effective in analyzing and predicting driver behaviors by taking into consideration drivers’ mental and physical actions toward the vehicle and environmental conditions (Lin et al., 1996; Lin et al., 2005), which is especially useful in assessing older drivers’ behaviors to explore their driving errors between desired and actual vehicle motions and their abilities to perceive unexpected hazardous situations.
Future implications could be developed by the RSCH framework, including (a) older driver training program: a tailored cognitive education program helps older adults better understand their cognitive status; (b) licensing regulations: licensing authorities may consider adding standardized cognitive testing to the licensing renewal process for older adults. Driving restrictions could also be issued to older drivers, which limit them to driving during the day or avoid high-speed highways; (c) roadway designs: traffic engineers could enhance roadway designs by considering cognitive constraints, improving driving safety for older adults. For example, roundabouts with multiple turns could be challenging for elders due to their impairments in spatial abilities and hazard perception. Therefore, controlled signals with lower speed limits could be considered when reconstructing roundabouts; (d) vehicle technology development: older drivers may benefit from enhanced collision avoidance systems.
Conclusion
This systematic review revealed the significant impact of cognitive declines on driving abilities and the importance of integrating cognitive assessments and driving evaluations, to understand driving fitness among older adults with cognitive impairments. The meta-analyses validate the utility of TMT-A/B, UFOV, and Maze Test in detecting cognitive decline, which correlates with increased driving errors and challenges in complex driving tasks. Furthermore, the narrative review indicates that while some older adults self-regulate their driving in response to cognitive declines, others with more severe impairments continue to face significant driving safety risks. The Road Safety Cognitive Health presents a systematic approach to evaluate the impact of cognitive health on older adults’ driving performance, guiding future directions in driving training, licensing, roadway designs, and vehicle technology development. Future works can be extended to use physiological sensors such as ECG and EEG in older adults’ driving studies.
In conclusion, this paper reviewed the disparity in driving performance between cognitively impaired and healthy older adults, which pointed out the urgency of developing a comprehensive approach to integrating cognitive health assessments into driving safety protocols to ensure that older adults can continue to navigate the roads safely and confidently.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.