
Abstract
Patient falls are common injuries in hospitals, and many occur surrounding a patient’s need to use the bathroom. In this study, we used the TripTech Method to design and evaluate early-stage design concepts for fall prevention and reduction of occupational injury associated with toileting falls. Nurse participants saw an opportunity in getting their patients to engage in their own recovery in increase the potential for cooperation, and also desired tools which could make the process physically easier for staff and patients which were also accessible when needed. Participants also discussed concerns about higher-tech tools, including affordability issues which could lead to further healthcare disparity. Overall, our research demonstrates how human-centered methods are valuable in focusing design efforts on the most pressing challenges experienced by users to avoid wasted investment in ineffective or unwanted technology.
Keywords
Introduction
Healthcare settings are highly complex systems which require a great deal of coordination in order to run safely and efficiently (Bavafa et al., 2021). One of the most common roadblocks to positive patient outcomes is when a patient falls while hospitalized (Goldsborough et al., 2019). Falls are a critical issue not only because they can lead to complications, additional injuries, and increased length of stay for patients, but are also very expensive for healthcare organizations who bear additional costs associated with falls (Florence et al., 2018). While falls occur for a variety of reasons, many patient falls are associated with a patient’s need to use the bathroom, and their tendency to attempt the process alone even when they are instructed to ask for help (Goldsborough et al., 2019).
Toileting is the process of assisting or supervising patients to use the bathroom for the purpose of ensuring safety, and is often a designated responsibility of nurses and nursing aids. This is a complex issue, and other researchers have noted that human factors methods and insights can aid in fall prevention (Hignett & Wolf, 2016). From past research (Rafferty et al., 2023), we learned that healthcare workers believe that patients are reluctant to call for help for a variety of reasons, including being embarrassed, confused, or not wanting to be a burden to staff. On the system level, nurses often suffer from excessive workloads which prevent them from responding to call bells immediately, and this delayed response can leave patients feeling like they have no choice but to attempt toileting by themselves. Toileting also poses risks of occupational injury to healthcare workers as they lift and move patients within clinical environments that are often cramped and awkward (OSHA, 2023). Current tools used by healthcare workers to aid in lifting and moving patients can cause discomfort to patients as they are transported to the bathroom, and many of these tools are deemed too expensive for wide scale implementation in hospitals, leading to disuse.
The focus of this study was to use Human-Centered Design (HCD) research and develop viable design concepts that can be effective in minimizing injury to patients and nurses while toileting. We also wanted to develop and/or identify affordable, innovative approaches to assist hospital patients and nurses which would address underlying causes and contributors to falls which current approaches do not adequately address. Our overall philosophy was that using the bathroom is a natural and necessary part of life which is most comfortably done in privacy in the bathroom, and that there are therapeutic elements of the patient-nurse touchpoint in getting a patient to and from the bathroom. We therefore used the TripTech method (Séguin et al., 2019) to develop and assess early-stage design concepts which were informed by this philosophy and prior research (Rafferty et al., 2023).
Methods
This work was carried out over the course of a year by a team of college seniors as a senior design project, and a faculty advisor in the Industrial and Systems Engineering department of SUNY Binghamton. The team’s objective was to use HCD and the TripTech method to create and evaluate early-stage design concepts that could be developed into real technologies which could reduce the risk of patient falls and healthcare worker (e.g., nurse) occupational injury. The Binghamton University Institutional Review Board oversaw this work and deemed all research activities as exempt.
Participants
In total, 40 individuals participated in this study, including 27 TripTech survey participants (n female = 25, n male = 2, n other = 0; average years in healthcare = 9.94, SD = 9.73), and 13 TripTech focus group participants across two sessions (n female = 11, n male = 2, n other = 0; average years in healthcare = 21.33, SD = 5.61). Individuals qualified for the study if they were a nurse, past or present, or nurse in training who had experience assisting patients with toileting in the clinical setting as part of their regular job. Participants were recruited through email lists distributed to nurses and nurses in training within multiple institutions across New York, through familiarity with the researchers, and snowballing. Individuals were eligible to participate in both phases if desired, and were compensated $5 for completing the survey, and $50 for participating in the focus group.
TripTech Method
The TripTech method was developed by user experience researchers and designers at Google to rapidly gather user feedback for potential designs in an early stage, prior to actually coding or building prototypes (Séguin et al., 2019). The method involves two phases, including surveys to narrow in on the most important and frequent needs felt by users, and focus groups to elicit feedback on storyboards featuring potential technologies designed to address these needs.
Surveys and Needs Statements
Guided by this method, we first drew on past research (Rafferty et al., 2023) to develop a series of “needs statements” to reflect hypothesized nurse needs in the context of toileting. We then surveyed nurses using the Qualtrics online survey platform to assess these proposed “needs” statements. Participants used a link embedded within a recruitment email to access the online survey, and first consented to participate before reading 14 individual user needs statements (see Table 1 in Supplemental Materials) presented with a simple illustration (see Figure 1 for an example). For each needs statement, participants rated how frequently they experienced each need, and how important it was to address the need using Likert. Needs statements presentation was randomized across all participants. The survey took about 15 min to complete.
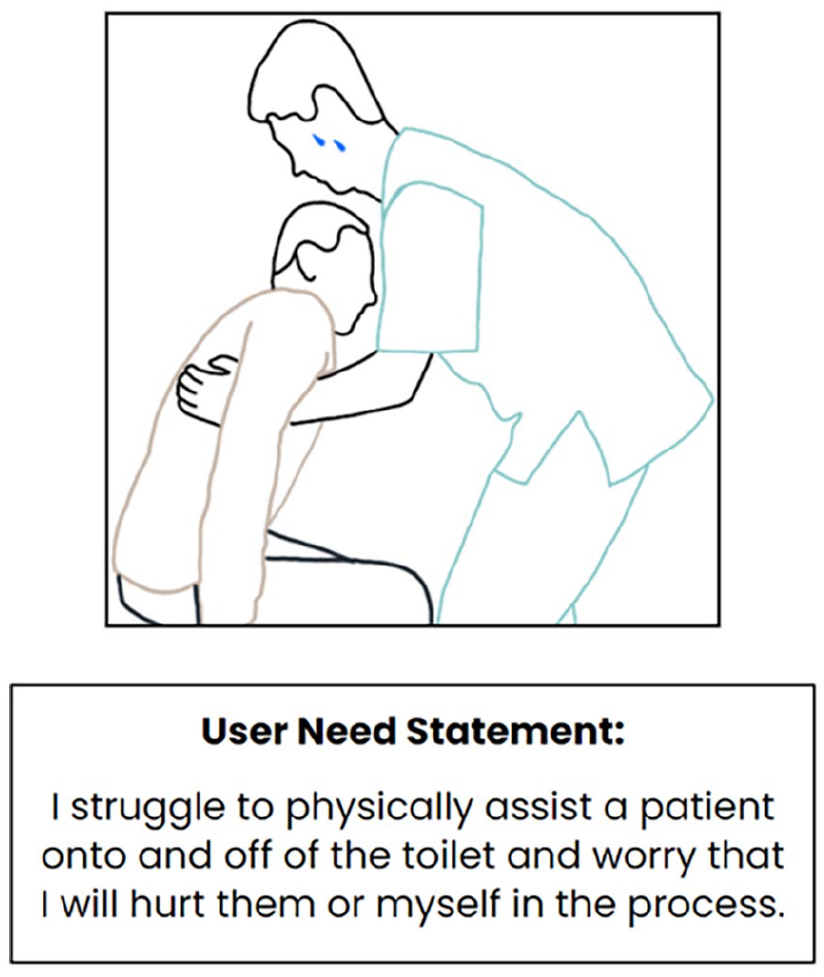
Example user need statement and illustration presented in online TripTech survey.
Focus Groups and Design Concepts
Next, we developed early-stage design concepts, consisting of three-panel storyboards in which proposed designs were depicted as addressing user needs. In addition, we included one design concept storyboard which featured an autonomous robot that took patients to the bathroom and excluded the nurse entirely, with the specific hypothesis that nurses would disfavor this technology. In developing illustrations, we found that two existing technologies were similar to the concepts we were focused on, including the Dignity lift (Handicare C-800: VIVA Mobility, 2024), and the Robear robot (Dredge, 2015), so we modeled illustrations on these products. This resulted in 6 total storyboards (see Figure 2 for an example; all storyboards can be seen in Supplemental Materials). We then conducted online focus groups over Zoom to gather feedback on the proposed designs. Participants were informed of the purpose of the session, and gave verbal consent to participate, as well as to having an automatic transcript record the conversation. After presenting each design to participants, each participant individually completed an online survey to indicate the extent to which they felt that the design was desirable and useful in the context of patient toileting using Likert scales. Afterwards, all participants engaged in an open, semi-structured discussion about their overall perceptions, concerns, desires, etc. for each proposed design. Each session took 1 hr to complete.
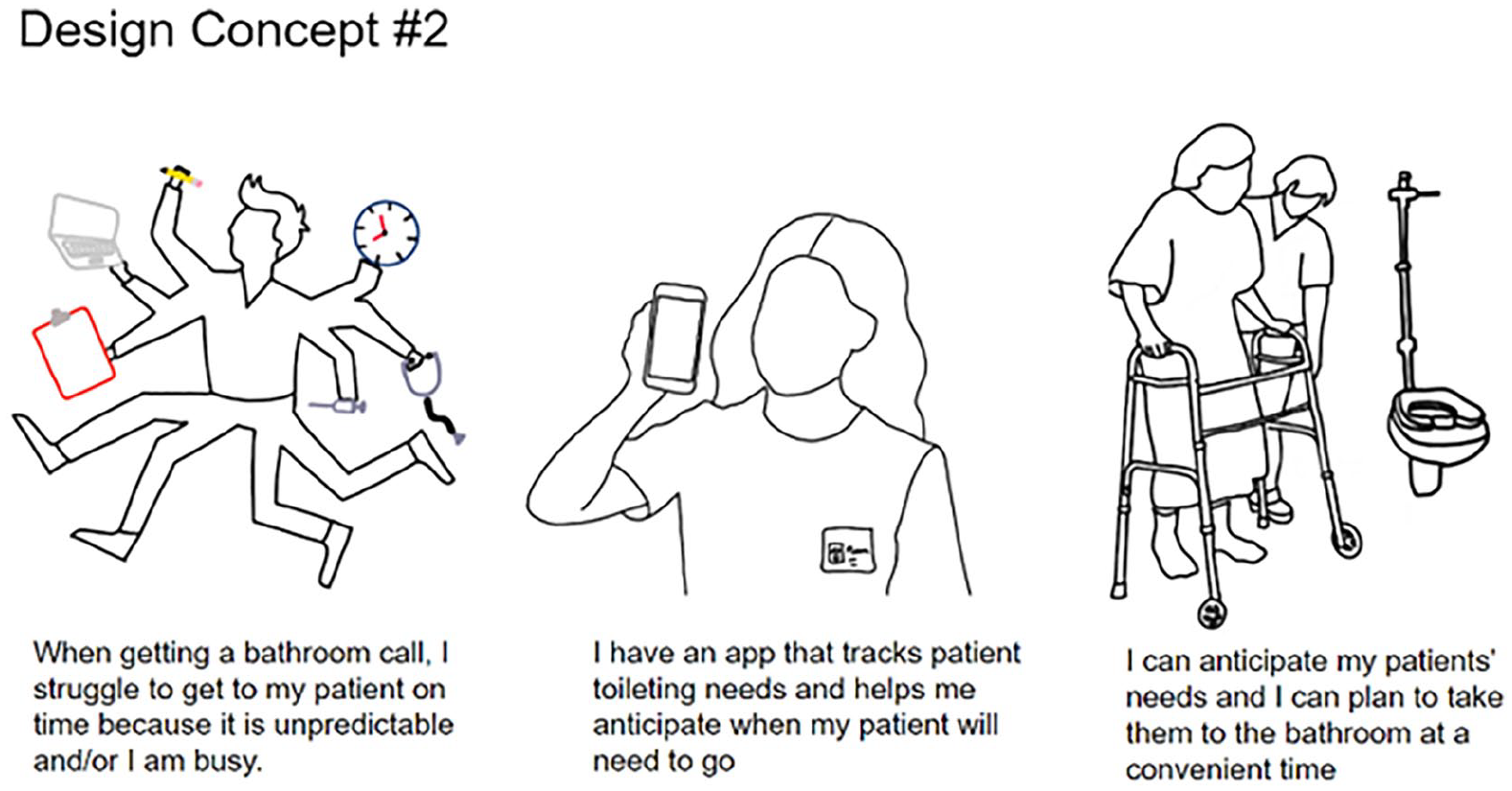
Example design concept storyboard presented in online TripTech focus groups.
Analysis
Quantitative data from surveys and focus groups was cleaned, analyzed, and visualized using R Studio. Likert data was graphed to visualize which “needs statements” had the highest average Importance and Frequency scores, and which designs had the highest average Perceived Usefulness and Desirability (see below). Qualitative data from the focus group was reviewed and a thematic analysis was performed using a normal word processor and color coded highlights.
Results
Surveys
For each of the 14 user needs statements, average ratings of the frequency at which the need is experienced (Average Frequency) and the average ratings of how important it is to solve the need (Average Importance) is presented in Figure 3. Vertical and horizontal lines have been added at the overall average Frequency and Importance ratings for all design, respectively, in order to visualize which statements have the highest ratings for each measure. The user needs statements with the highest ratings included the following:
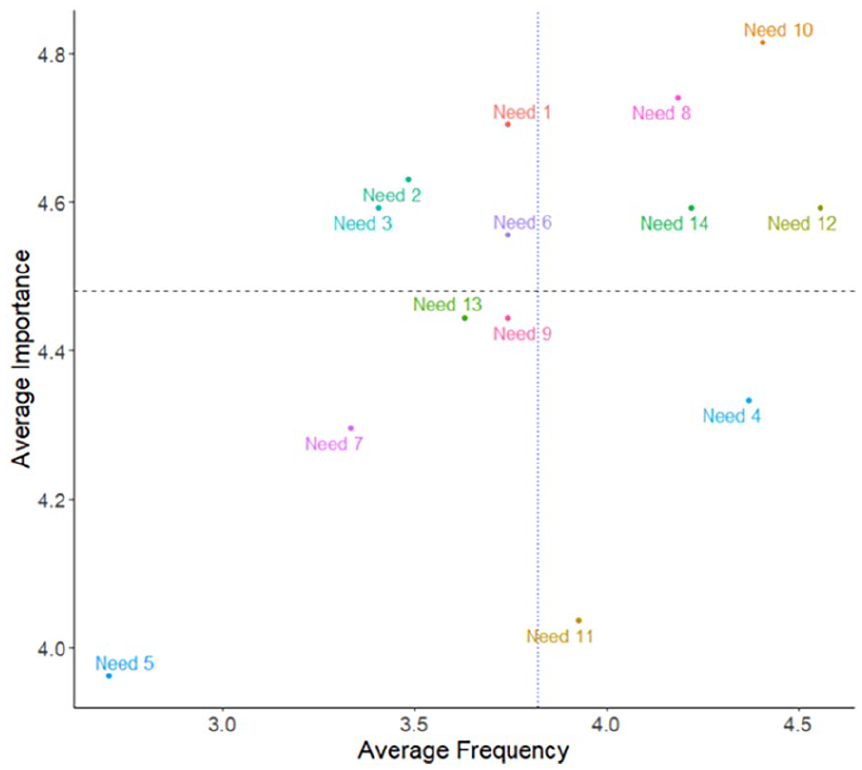
TripTech survey results for each of the 14 needs statements.
Need 8: “I worry that my patients will risk falling to/in the bathroom because they do not want assistance.”
Need 10: “I worry that my patients will risk falling to/in the bathroom because they will not wait for me.”
Need 12: “I worry that my patients delay their recovery by spending too much time in bed.”
Need 14: “I worry that my patients struggle to understand their own limitations and path to recovery.”
Focus Groups
For each of the six design concepts, average ratings of desirability for each design (Average Desirability) and perceived usefulness of design concepts (Average Perceived Usefulness) in the context of toileting is presented in Figure 4. Vertical and horizontal lines have been added at the overall average Desirability and Usefulness ratings for all design, respectively, in order to visualize which designs were most favorable. The designs with the highest ratings included the following:
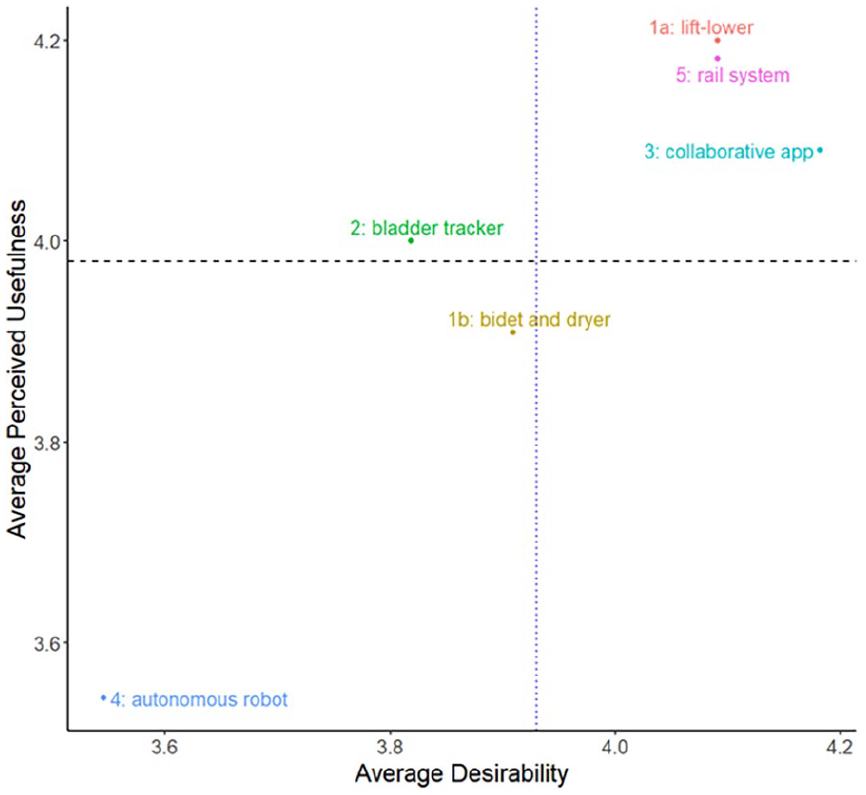
TripTech focus group results for each of the six design concepts.
Design Concept 1a: A lifting and lowering toilet seat to reduce occupational injury.
Design Concept 3: A collaborative app that helps patients engage in their own recovery and understand their own limitations.
Design Concept 5: A ceiling-mounted lift and mobility device which made toileting more convenient through increased accessibility.
A thematic analysis was also conducted on the focus group transcripts. Themes were developed iteratively over multiple team meetings and deep conversations. The final set included six themes related to Patients, the Work Environment, Technology Commentary, Compliance/Policy, Nurse Behaviors/Outcomes, and Broader Implications. These themes aided in identifying participant insights which can inform the next phases of design. These themes, including a description and representative example quote can be seen in Table 2 in the Supplemental Material.
Participant Perceptions of Design Concepts
The lifting and lowering toilet seat (Design Concept 1a) was created to address several user needs, largely having to do with the physical strain put on nurses and other staff in order to lift and lower a patient on and off either the toilet or the bed. Participants liked the idea of a device that would alleviate their physical strain and “help with back pain,” however many immediately thought about various patient characteristics which would lead to unintended consequences and must be considered in the design, including weight restrictions, seat width/depth, and if especially weakened patients could potentially fall forward when the device is in the highest position. Participants also commented on the dependability of the technology within the hospital context: “How often would it break? What if it broke on the highest level, the toilet would not be operational.” When considering adding a bidet and drying feature to the toilet seat (Design Concept 1b, see Supplemental Material), one participant thought “it would be very helpful, especially to give patients privacy,” as nurses would no longer have to clean the patient in the bathroom. Others expressed concerns, including that it was, “hard to imagine that it would get [patients] fully cleaned, and even after they [were] cleaned, they would try to get up.” Our intention with this design concept was to increase patient compliance in asking for assistance off of the toilet and back to bed, however this highlights how the design may have the opposite effect. Additionally, participants worried about “skin integrity issues” which could be exacerbated by the bidet or if a drying feature was inadequate. Another participant noted that the bidet could be better for certain types of patients such as postpartum patients who may have perineal stitches after giving birth. One additional idea from participants was to have an alarm system tied into the functionality of the bidet or lift toilet, such that nurses could tell when patients were finishing up and about to get up and leave the bathroom.
The proposed collaborative app (Design Concept 3) was designed to addresses nurse fears that patients are not actively participating in their recovery, leading to too much sedentary time as well as a lack of understanding of their own limitations while in the hospital. Participants thought the app was “symbiotic,” offering “patient benefits and nurses benefits.” Having a way to keep patients engaged would encourage them to track their progress and be informed of their condition. Nurses thought that the device was simple and would be easy to operate.
The rail system (Design Concept 5) was proposed to address user needs related to space restrictions within hospital rooms and bathrooms, inaccessibility/scarcity of existing lift equipment which leads to disuse, as well as physical strain associated with lifting and maneuvering patients. The rail system would allow the user to maneuver in tight spaces and would also be built into each room to prevent misplacement. Participants appreciated that they wouldn’t “have to go grab equipment, which is often the case,” confirming that this is a pervasive challenge within their work environment. Another participant also remarked that this inaccessibility means that current lift devices are, “really [only] used for patients who are completely immobile,” and expressed interest in this design because it would mean that they were able to use this assistive equipment for more patients.
Our two most “high-tech” design concepts included an AI-enabled bladder sensor which could predict when patients would need to use the bathroom (Design Concept 2), and an autonomous robot assistant (Design Concept 4). These designs had the lowest desirability ratings for all concepts, with the autonomous robot having the lowest average ratings for both desirability and perceived usefulness. Concerns for the bladder sensor included reservations about the ability of technology to accurately predict when a patient needs to go to the bathroom and the potential for alarm fatigue if the tool resulted in excessive alerts for nurses. The autonomous robot concept was especially contentious. Some participants scored it very high in the surveys, referencing its ability to relieve the physical strain and time, however others argued that a robot did not have a place in a hospital. Within an open response portion of the individual surveys, one participant simply wrote “No.” Participants who were more strongly opposed stated that they believed that their patients would not adapt well to the device as they “fight tech now,” and that “when you’re healing, you need that emotional connection.” Some nurses also had difficulty recognizing what patients this would work for as it seemed to require a good deal of mobility and strength for the patient to keep themselves upright: “Would the patient slide out of the robots hold? Does the patient need to have a certain amount of control to get into the robots arms?” One important “broader implication” of all proposed designs was the potential to contribute to healthcare disparities if designers exclusively focused on creating high-tech tools which were very expensive. This was brought up at multiple points during the first Focus Group, including in the discussion of Design Concept 1b: “Here at [our hospital], they would never ever see a technology like this. It would be too expensive and it would cause more inequity. Medicare and Medicaid and [the hospital], they’re not paying for that.” At a later point, in reflecting on the autonomous robot (Design Concept 4), another participant added in reference to this earlier comment: “if toilets were too expensive, what would the cost of something like this be?” This is further justification that designers should engage with individuals who are users or stakeholders in designs, prior to engaging in design
Discussion
In this study, we used the TripTech Method to design and evaluate novel technologies which could be used to prevent falls and reduce occupational injury associated with toileting patients. Overall, we found that the most pressing needs expressed by our participants were related to patients not wanting to comply and/or not being aware of their own limitations and delaying their recovery through spending too much time in bed. Of our 6 design concepts we created to address these pressing needs, nurse participants saw the greatest opportunity with devices which could improve patient and nursing experience with the process of toileting. This included lifting and mobility assistive equipment which could be embedded within existing hospital environments to increase device accessibility when needed and reduce physical strain, and a collaborative app that could encourage patients to engage in their own recovery, and understand their own limitations to increase compliance with policy. Participants also discussed concerns about higher-tech tools, including their feasibility and potential to reduce emotional connection if they eliminate a nurse-patient touchpoint. Additionally, the pointed out that affordability issues could lead to further healthcare disparity. Designers and human factors professionals can apply these insights to improve the toileting process for patients and healthcare workers alike.
Limitations
This study is limited in a variety of ways. The greatest limitation is the relatively small sample size. While the data samples were relatively small, the data collected was in depth and the sample size is consistent with other HCD research. Despite these limitations, this study is still beneficial as the rich insights gained from these first-hand accounts will guide the direction of further research.
Future Work
Future work will focus on further designing and/or refining the early-stage design concepts which were rated most favorably by participants, especially the collaborative app and the mobility assistive devices.
Supplemental Material
sj-pdf-1-pro-10.1177_10711813241276473 – Supplemental material for Using Human-Centered Design to Decrease the Risk of Toileting in Hospitals for Patients and Clinicians
Supplemental material, sj-pdf-1-pro-10.1177_10711813241276473 for Using Human-Centered Design to Decrease the Risk of Toileting in Hospitals for Patients and Clinicians by Kate O’Neill, Molly Doran, Keelin Davie, Anthony Andreano and Stephanie Tulk Jesso in Proceedings of the Human Factors and Ergonomics Society Annual Meeting
Footnotes
Acknowledgements
We would like to thank our participants again for sharing their valuable insights with us.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Additionally, we would like to thank the SUNY Binghamton’s Instructional Lab and Software Committee (ILASC) for their funding which was used to pay participants for their time and effort.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.