
Abstract
We describe a new program element in our Veterans Health Administration (VHA) healthcare system. The purpose is to pursue opportunities for efforts to complement existing VHA safety work with an emphasis on understanding how things go right and supporting activities or structures that contribute to system success. The program takes a holistic systems approach to safety by promoting system lifecycle activities that explore context of use and Work-As-Done, recognizing that the way work is performed reflects realities of the work environment, demands, resources, and organizational value system. It seeks to increase human factors capabilities with a goal of empowering design teams to understand and document current state prior to proposing changes and to explore opportunities and conduct risk assessments for current state, proposed redesigned state, and post-implementation state. An outcome should be enhanced staff ability to understand and adapt to changing demands and conditions that affect how they deliver care.
Patient Safety in the VHA
In recent decades, the field of healthcare has received increased attention in areas of safety and quality (e.g., Kohn et al., 1999; Stoelting, 2000). The Veterans Health Administration (VHA) in the Department of Veterans Affairs (VA) has a multi-pronged approach to addressing patient safety.
A key component to the VHA approach to safety was the establishment of the National Center for Patient Safety (NCPS) in 2000 (Bagian et al., 2001). NCPS supports a network of patient safety professionals—distributed at the facility and regional levels—and administers education and learning efforts (e.g., Paull & Williams, 2013; Watts et al., 2018;), tools (e.g., DeRosier et al., 2002; H. J. Fuller et al., 2017), and requirements for quality and quantity of safety efforts. The programming includes a reporting system and surrounding infrastructure as well as communication channels to national program offices and the field.
More recently, Informatics Patient Safety (IPS) was formed within the VHA to focus on patient safety concerns involving informatics systems, including electronic health records (EHRs). Similar to NCPS, IPS has both proactive and retrospective approaches to addressing safety concerns (Taylor et al., 2012; Wood et al., 2014). The program offices collaborate regularly with each other and with other groups within VHA.
There are many different models and philosophies of safety (see Arnold & Fuller, 2020), with various benefits and risks when applied in different settings. The existing VHA safety programs have been very successful in many ways. These programs have tended to align with a barrier model of safety that focuses on the prevention of things from going wrong, sometimes termed Safety-I or Protective Safety (Hollnagel, 2018). There are opportunities for complementary safety efforts aligned with Safety-II or Productive Safety, which emphasizes understanding how things go right and supporting activities or structures that contribute to system success (Hollnagel, 2018). The VHA Human Systems Integration (HSI) program office is developing a new program element to pursue these opportunities.
A Systems Safety Program
The VHA HSI systems safety program is based around the idea that systems are inherently limited. People in a system bridge the gaps between what the system can do and what it needs to do in any given instance, and in doing so they use adaptivity and resilience to create safety.
VHA HSI wishes to support viewing systems holistically with the goal of understanding influences that shape activities and motivations. Program activities will promote sociotechnical systems design to support people in adaptively managing complex and dynamic conditions and mitigating associated emergent risks.
The systems safety program will complement the existing safety infrastructure in VHA while helping to align HSI work with patient safety goals. The addition of this program within the VHA HSI division will allow us to more explicitly consider patient safety during work efforts and promote the inclusion of human factors work as a means to address patient safety concerns.
Safety and Resilience
The systems safety program has the goal of improving safety, and particularly patient safety, in the organization such that: (a) as few things as possible go wrong, (b) as many things as possible go right, and (c) we realize the greatest possible reduction in risk while considering tradeoffs, both with other system goals and with risk in other areas.
A key focus of the program is on supporting resilience. Resilience describes the ability of a system to succeed under varying conditions, including across diverse patient needs and situations, workload demands, and resource constraints (Woods, 2015). Resilience is often thought of as important to safety when viewing a system through a Safety-II lens. More traditional safety work often seeks to identify and capture risks and track adherence to safe practices. In contrast, in a system that values resilience, the role of safety professionals is to build knowledge regarding changing risks to facilitate action before harm occurs. Such work helps to create guided adaptability by developing capacity for anticipation, readiness to respond, synchronization, and proactive learning (Provan et al., 2020). These aims align well with human factors methods, including tasks analysis, contextual inquiry, and usability evaluation, which seek to understand user characteristics and system constraints during the design process (H. Fuller et al., 2023).
HSI Systems Safety Program Elements
Specific program focus areas are: (a) supporting human-centered design, (b) encouraging considerations of resilience when evaluating and designing systems, and (c) promoting the thoughtful encoding of standards as guidance, not context-insensitive enforcement, into healthcare systems. The program takes a holistic systems approach to safety by promoting system lifecycle activities that explore context of use and are supportive of Work-As-Done, recognizing that the way work is performed reflects realities of the work environment, demands, resources, and organizational value system. It seeks to increase human factors capabilities close to where work is done with a goal of empowering design teams to routinely understand and document current state prior to proposing changes and to advocate for risk assessments for current state, proposed redesigned state, and post-implementation state.
During program development, a concept map was created to identify important elements relevant to systems safety and some key relationships among them (Figure 1). Though these concepts and relationships are not comprehensive, they have been useful in thinking about the important components of a systems safety program. The visualization has also been helpful in describing important program elements to stakeholders and collaborators.
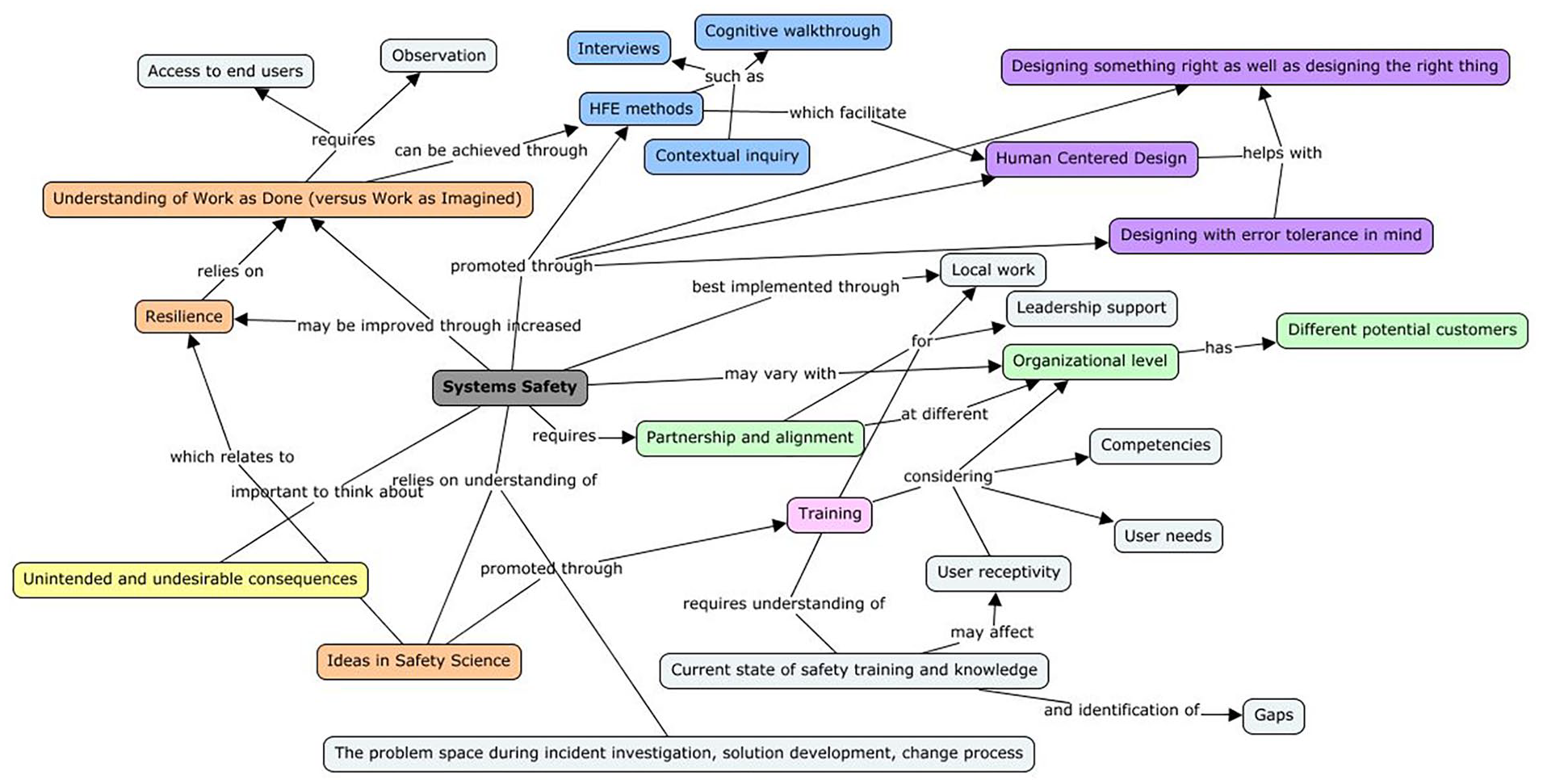
A concept map shows relationships between various ideas important to the systems safety program.
The systems safety program described here seeks to achieve and maintain acceptable levels of risk and support system resilience while treating a system holistically, accounting for interactions among its parts. The program will support human factors training at different organizational levels to promote usability and human centered design (HCD), which will work to build safety in systems. It will provide education and guidance for the HSI office and national health informatics groups on safety science, including methods and the potential for unintended consequences.
The program helps to build human factors capabilities through the dissemination of training and tools that will enable facility-level staff to incorporate human factors and HCD principles into their work. This includes systems safety education for local informaticists as well as a potential new group of field usability specialists, who will be stationed at local hospitals.
Nationally, the systems safety program is collaborating with existing safety programs to incorporate human factors work where useful and to promote inclusion of usability efforts. Training and tools support explicit considerations of patient safety in national human factors and usability work. The program is also working to identify practices that promote systems success and conditions that allow these practices to develop, complemented by exploration of whether and how to encourage the spread of these practices.
We are working to establish means to monitor accomplishments relative to these goals, course correct, and adapt to changes in the safety needs of the healthcare organization. These include specification of milestones and measures related to processes and outcomes.
Initial Reception
Initial key program activities are so far well received. Trainings on systems safety concepts and safety science, including Safety-II and resilience engineering, have been provided to national-level HSI practitioners and informaticists in the healthcare system. Following systems safety briefings to program office leadership, we have noticed a shift in language to include resilience concepts. We are holding stakeholder conversations with colleagues in leadership positions across the larger organization. These have served to educate leaders and advocates about our systems safety program and philosophy while revealing new opportunities for our team.
At the facility level, training efforts on context of use and human factors methods such as heuristic evaluation intended to support staff in designing systems that work well for their users have generated positive feedback. They reported success in using the tools designed to guide them through the application of human factors methods.
At the national level, we have added explicit consideration of safety to HSI work. This includes an addition of the category “patient safety considerations” to a heuristic evaluation template, development of a method for systematically evaluating safety implications of medication warnings, and addition of risks to task analysis work (H. J. Fuller et al., in press). We have also piloted collaboration with safety program offices and use of human factors methods to explore design decisions in safety-critical projects such as redesign of language and interfaces related to removing penicillin allergies.
Conclusions
The VHA HSI systems safety program seeks to deploy a solid portfolio of trainings and human factors methods supporting analysis, design, development, test, and evaluation to increase resilient performance of the healthcare system. The resilience-influenced philosophy of the program is that safety will emerge from thoughtful, human-centered design of informatics systems. The program will support development of ways to grow and share cross-facility safety wisdom, incorporating human factors principles.
We are addressing the challenges of building awareness of our new program, including developing education on the role of resilience principles and supporting decision making about acquisition and implementation of healthcare informatics systems. At the same time, we are working to increase the breadth of our involvement in safety initiatives and our ability to meet safety needs of enterprise facilities.
Given the present framework for safety and the mature processes in place within the organization, the systems safety program is exploring opportunities to build complementary capacity for activities that promote resilience while identifying pathways for sharing processes, products, and relevant cross-organizational wisdom. The human influence in systems is often what makes them work; the VHA HSI systems safety program will support people in creating safety within our healthcare systems.
Footnotes
Acknowledgements
I am grateful for the many thought-provoking discussions with Tim Arnold regarding systems, safety, linguistics, and engineering that have led to the refinement of the ideas underlying this program plan. I thank Kelly Neville and Michael Greenfield for our detailed conversations on systems safety and program development that have helped to shape and formalize this work.
Authors’ Note
The opinions expressed in this article are the author’s and do not necessarily represent those of the Veterans Health Administration or the United States Government.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.