
Abstract
Handoffs, that is, care transitions, convey information, responsibility, and authority between care providers. Intraoperative handoffs, which occur during surgery either due to shift changes or breaks, are high-risk, error-prone and linked with inadequate verbal communication and documentation. We explored perspectives about safety and quality of intraoperative handoffs between anesthesia providers at an academic medical center. Through an anonymous online survey, we asked participants to share their opinions on current handoff practices including teamwork, staffing and work pace, and handoffs and information exchange. The results showed positive perceptions about teamwork, while only half of the participants were positive about staffing and work pace. We also found that opinions of participants about staffing and work pace vary based on their role. Our study emphasizes the importance of considering diverse perspectives and employing a systems-based approach to address challenges and implement effective interventions for safe, high-quality handoffs in intraoperative care.
Introduction
Handoffs, also known as handovers or care transitions, involve conveying information, responsibility, and authority from one or a group of care providers to another (Abraham et al., 2014). Handoffs can be helpful in identifying errors, reassessing care decisions, and reviewing of care with the input of another perspective (Cooper et al., 1982; Perry, 2004); however, there are some risks in this process such as the loss or inaccurate transmission of information between providers, as well as ambiguity in authority and responsibility for patient care (Arora et al., 2009; Solet et al., 2005). In 2006, the Joint Commission implemented a National Patient Safety Goal in order to enhance communication during handoffs (Arora & Johnson, 2006). Much effort has subsequently been focused on designing and testing improvement interventions. Despite these efforts, there were still 7,149 reported cases of patient harm, resulting in 1,744 deaths, attributed to communication failures, between 2009 and 2013 (CRICO Strategies, 2015).
Handoffs occur frequently in the operating room, particularly between anesthesia providers such as attending anesthesiologist physicians, certified registered nurse anesthetists (CRNAs), and trainee physicians (i.e., residents or fellows; Abraham et al., 2014). Anesthesia providers play a significant role in ensuring continuity of care and hold a unique position to lead perioperative handoffs because they interact with a range of clinicians throughout the preoperative planning, intraoperative and postoperative care phases (Abraham, Meng, et al., 2021). According to Jones et al. (2018), intraoperative handoffs that occur during surgery are either due to shift changes (i.e., permanent handoffs) or breaks (i.e., temporary handoffs); Epstein et al. (2017) and Hyder et al. (2016) showed these handoffs are high-risk and error-prone, often linked with inadequate verbal communication and documentation. Based on a recent systematic review conducted by Abraham, Meng, et al. (2021), additional research considering the impact of intraoperative handoffs on outcomes and the development of tools to improve them is needed, with particular emphasis on designing and implementing standardized handoff tools integrated within Electronic Health Records (EHRs).
However, to be effective, any new or improved technology must fit with the work of clinicians. Using human factors/ergonomics-based models can help to ensure this fit. For example, the Systems Engineering Initiative for Patient Safety (SEIPS) model (Carayon et al., 2006, 2014, 2020) considers the work system elements, including people, tasks, environment, tools and technologies, and organization, and their interactions to guide improvement efforts. Subsequently, the introduction of any new technology must be accompanied by an analysis of the broader work system and process to ensure that the technology integrates with the workflow of clinicians. Often, engaging those clinicians in a participatory approach throughout intervention design and implementation is needed (Wilson et al., 2005).
Here, we aim to explore the existing intraoperative handoff process. We also seek to understand the opinions of anesthesia providers about the safety and quality of these handoffs and their ideas for improvements.
Method
This is a part of a larger study aiming to improve the safety and quality of intraoperative handoffs. It was approved by the Institutional Review Board at University of Illinois Urbana-Champaign.
Participants
We invited anesthesia providers, including anesthesia attending physicians, physicians in training (i.e., fellows and residents) and anesthetists at an academic health care center in the Eastern United States to participate. We recruited them through emails to department listservs, meetings, and flyers.
Data Collection
We collected data using an anonymous online survey administered via Qualtrics. We asked participants to describe what happens when they are relieved for a break or a shift change and to explain if anything is different when they provide relief. We administered three composite measures adapted from the Agency for Healthcare Research and Quality (AHRQ) Survey on Patient Safety (SOPS) Hospital Survey 2.0, focusing on teamwork, staffing and work pace, and handoffs and information exchange, defined as follows (Sorra et al., 2021, p. 2):
Teamwork: “Staff work together as an effective team, help each other during busy times, and are respectful.”
Staffing and work pace: “There are enough staff to handle the workload, staff work appropriate hours and do not feel rushed, and there is appropriate reliance on temporary, float, or PRN staff.”
Handoffs and information exchange: “Important patient care information is transferred across hospital units and during shift changes.”
We then asked about their opinion on what should be continued, started, and stopped to ensure safe and high-quality intraoperative anesthesia handoffs.
Data Analysis
We analyzed the descriptions of the current handoff processes using the SEIPS-based process mapping method (Wooldridge et al., 2017)
We used Excel® to compute the percentage of positive score of the three composite measures adapted from the AHRQ SOPS Survey. The survey included both positively worded items (e.g., “In this unit, we work together as an effective team”) and negatively worded items (e.g., “During shift changes, important information is often left out.”). For positively worded items, we combined percentage of respondents within the hospital who answered, “Strongly agree” or “Agree” and for negatively worded items, we combined percentage of “Strongly disagree” or “Disagree” (Sorra et al., 2021) to calculate positive evaluations. We conducted an ANOVA to determine if perception of participants about teamwork, staffing and work pace, and handoffs and information exchange vary by role.
We performed an inductive thematic analysis (Guest et al., 2012) of data from participants about what they believe should be continued, started, and discontinued to improve the safety and quality of handoffs to identify potential improvement strategies.
Results
A total of 37 participants (15 anesthesia attending physicians, 15 anesthetists, and seven residents) started the survey, with 31 completing the entire survey (three attendings and three anesthetists did not finish). Of the participants, 52% were female and 97% white.
Current Intraoperative Anesthesia Handoff Process
Before the temporary handoffs, the outgoing anesthesia provider requested a break from the in-charge anesthesiologist. During the handoff they gave a brief report (either paper based or computer based) about the patient history, current anesthesia plan, medications, IV access, etc. to the incoming clinician and answered questions of the incoming anesthesia provider. For the permanent handoffs, the incoming anesthesia provider reviewed the case in the Electronic Health Record (EHR) before handoffs. Compared to temporary handoffs, they received more detailed reports (either through phone or on the bedside) and asked more involved questions. Figure 1 shows the SEIPS-based model of temporary and permanent handoffs.
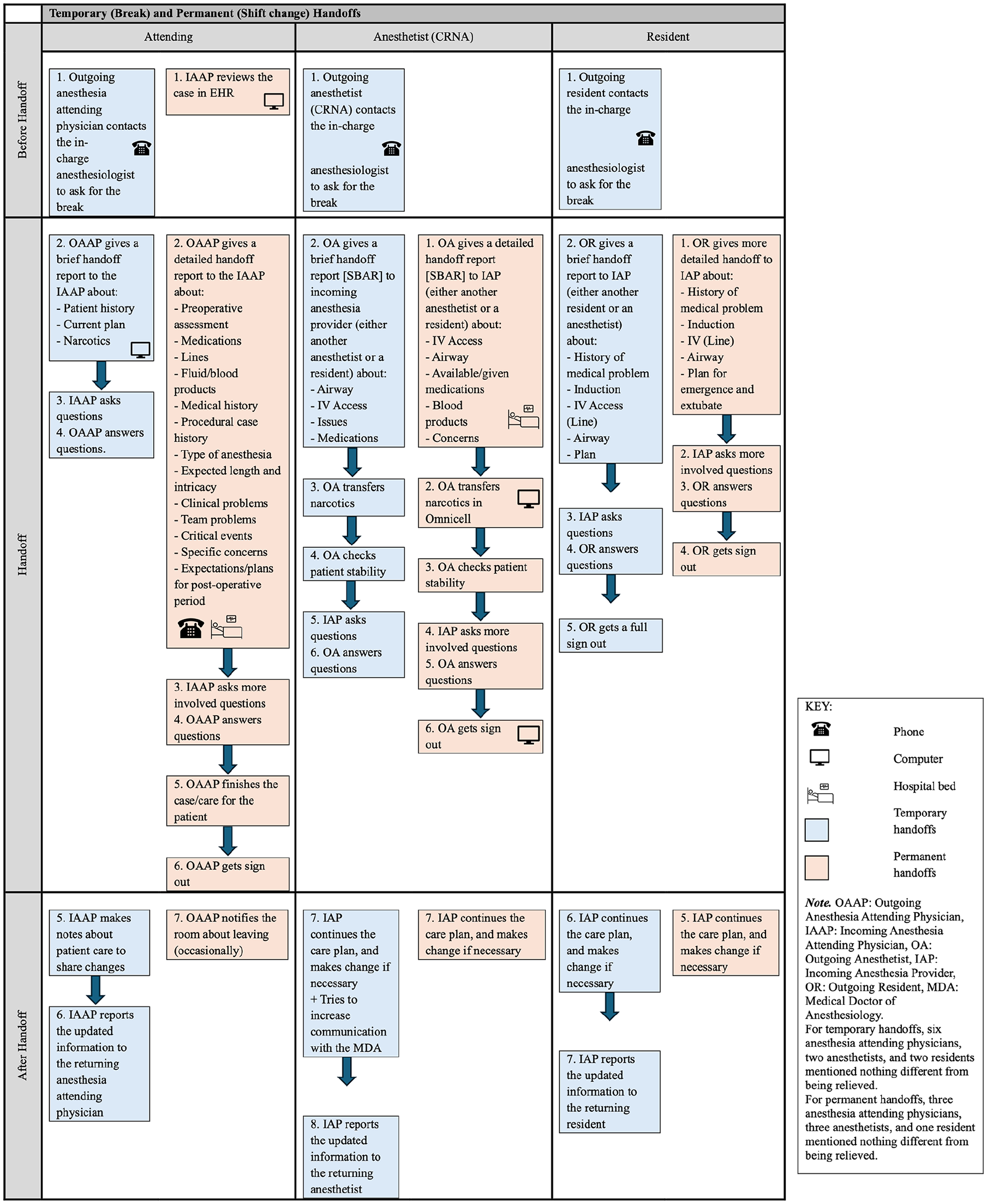
SEIPS-based process model of temporary and permanent handoffs.
Evaluation of Current Process
Almost all the participants (91%) evaluated their recent handoff experiences positively in terms of teamwork, less were positive about staffing and work pace (50%), and handoffs and information exchange (58%).
The average score for teamwork, staffing and work pace, and handoffs and information exchange are shown in Table 1. The opinions of the participants on teamwork (F (2,36) = 0.173, p = .842) and handoffs and information exchange (F (2,30) = 1.460, p = .249) did not significantly vary by role. However, opinions on staffing and work pace varied significantly based on role (F (2,36) = 28.791, p = .0001). Anesthesia attending physicians expressed a more negative opinion (M = 2.50/5) while anesthetists showed a more positive opinion (M = 4.16/5).
Descriptive Statistics of Three Composite Measures in Three Groups of Participants.
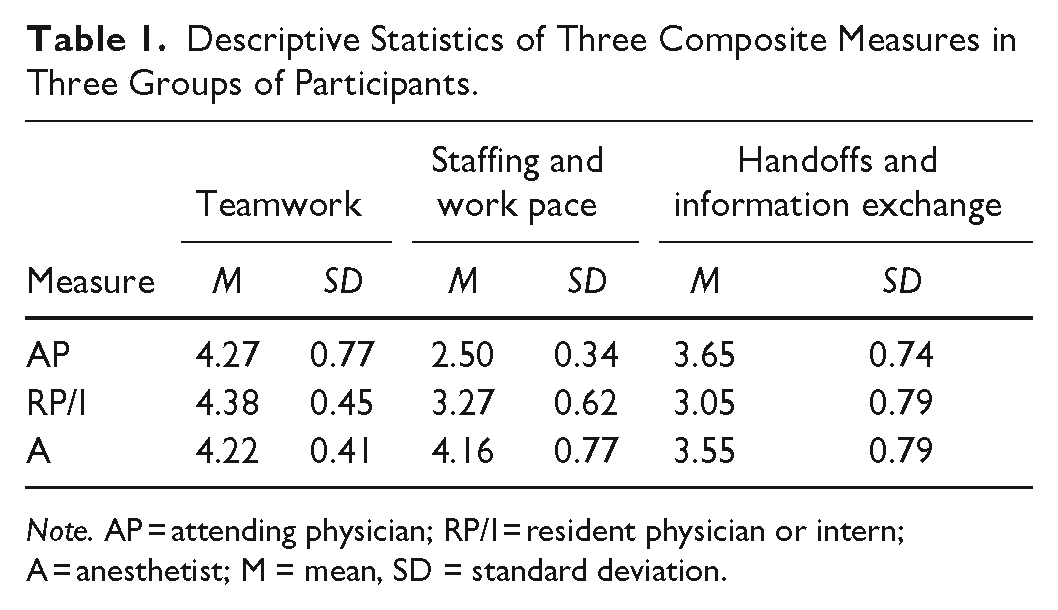
Note. AP = attending physician; RP/I = resident physician or intern; A = anesthetist; M = mean, SD = standard deviation.
Potential Handoff Improvements
To ensure safe and high-quality handoff processes, participants emphasized the importance of asking questions during handoff and face-to-face communication of all necessary information. They expressed the need to start using checklists or handoff protocols that include familiar or somewhat standardized formats of information. They also mentioned strategies that discontinued some current practices with potential for negative impact, for example, handoffs over the phone, not enough relieve staff, time constraints/rushed handoffs.
Discussion
Our process analysis showed that before temporary handoffs, the outgoing anesthesia provider requested a break, then gave a brief report to the incoming clinician and addressed any questions. After they were back from the break, they received an updated report from the care provider. For permanent handoffs, the incoming provider reviewed the case in the EHR beforehand, received a more detailed report, and asked more in-depth questions. After handoffs, they continued the care plan and made changes if necessary. Our data showed that perceptions of anesthesia providers about teamwork were mainly positive, but only half of the participants were positive about staffing and work pace, and handoffs and information exchange. We also found that opinions about staffing and work pace varied by role with more negative opinion among anesthesia attending physicians and more positive opinion among anesthetists.
Half of the participants expressed dissatisfaction with the current number of providers and the pace of the handoff process. Considering that insufficient staffing and accelerated work pace can increase the workload and stress level of existing care providers as well as the possibility of making mistakes (National Academies of Sciences, Engineering and Medicine, 2019), participants mainly suggested stopping the rush during handoffs and addressing staff shortage. Since other system factors can contribute to or mitigate the risk of burnout, implementing the SEIPS-based process analysis would provide a foundation to understand these factors.
Standardized handoff protocols and checklists were the most common suggestions from participants for improving the handoff process. Indeed, implementing similar interventions has been shown to improve quality of information transfer and clinician satisfaction with handoffs (Abraham, Pfeifer, et al., 2021). However, time restrictions can make barriers in the use of checklists especially in minor surgeries (Jullia et al., 2017). Abraham, Pfeifer, et al. (2021) suggested the implementation of standardized handoff tools integrated within EHRs as a way to address these issues. To prevent negative, unanticipated consequences of the implementation of technology-centered improvement interventions, consideration of the entire sociotechnical system is required (De Zwart, 2015; Wooldridge et al., 2024). For example, the development of an EHR-based handoff checklist may inadvertently increase the workload of anesthesia provider and/or add a distraction to patient care prior to the handoff even if it facilitates information transfer. Using a systems-based approach to design and develop interventions, technology-based and otherwise, will help to identify and address unanticipated, negative consequences in addition to ensuring positive outcomes on safety and quality of care.
Variation in the opinions of the participants about current intraoperative handoffs highlights the importance of considering multiple perspectives resulting from the diverse backgrounds of participants in addressing challenges to safe and high-quality handoffs. Recognizing and valuing the unique insights of attending physicians, residents, and anesthetists can help to inform effective interventions appropriate for team-based care.
Limitations
Our study has some limitations. First, we used a relatively small sample size which may not be representative of all anesthesia providers. Second, we relied on self-reported data and did not observe or interview the participants, which may not accurately capture handoff practices or quality. We are continuing to collect data to address the sample size issue and aim to apply a multimethod approach in future work. Lastly, our research was focused on a single academic healthcare center in the Eastern United States. This setting may have unique characteristics that do not apply to other institutions, limiting the generalizability of the findings beyond our intended case.
Conclusion
Our findings highlight the importance of considering diverse perspectives and employing a systems-based approach to address challenges and implement effective interventions for safe, high-quality handoffs in intraoperative care; Strategies suggested by the participants serves as the basis for targeted interventions and developing a culture of continuous improvement within the intraoperative handoffs at the participating health care system.
Footnotes
Acknowledgements
We would like to thank the anesthesia providers who participated in this study; our research would not be possible without them.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.