
Abstract
Interruptions that occur during high-stakes tasks in healthcare increase the likelihood of adverse events. Research on interruption management strategies has addressed the outcomes of interruptions but not what influences the decision to accept or reject them. This study examined the effects of high and low levels of three moderators on the interruption decision-making process: priority, cost of the interruption, and method of interruption. Participants entered data in a simulated patient chart while monitoring simulated patient vital signs and were interrupted four times to perform other activities. Participants could either accept or reject each interruption. The results showed that high priority, low-cost, and face-to-face interruptions were more likely to be accepted. Thus, participants considered the nature of the interrupting task when deciding to suspend work on their current task. These results suggest that a better understanding of factors that affect interruption decisions can lay a foundation to help diminish their disruptiveness.
Introduction
Interruptions are common in the workplace but when they happen during high-stakes tasks they can have serious consequences. In healthcare, it has been shown that interruptions can lead to adverse events or medication errors, the latter considered to be the third leading cause of death in the United States (Kukielka et al., 2019; Makary & Daniel, 2016).
An interruption consists of suspending progress on one task to address a second task where the intent was to complete the initial task. The interruption process begins with a signal (e.g., an alarm or co-worker initiating conversation) that must be interpreted (Latorella, 1999; Sarter, 2013; Woods, 1995). Then, a decision is made to either reject the interruption and continue working on the primary task or accept the interruption and address the requirements of the new task/activity.
Research on interruption management strategies addresses the outcomes of interruptions but often fails to account for the initial decision to accept or reject the interrupting task, and when it does, it rarely addresses moderators that influence the decision. Salvucci and Bogunovich (2010) studied one moderator, workload, and found that only 6% of participants would switch to the interrupting task when workload on the primary task was high. There has been little investigation of other moderators; however, there is some relevant research in the task-switching literature where individuals determine when to switch their effort among several tasks. Wickens et al. (2016) used the strategic task overload management (STOM) model to predict task-switching during high levels of workload and examined the effects of four task attributes: priority, interest, salience, and difficulty. The model with the best fit included a combination of interest, salience, and difficulty, but not priority.
The goal of the current study was to examine the effects of three moderators on the decision to accept or reject an interruption: priority, cost of the interruption, and the method of the interruption. Regarding priority, Barg-Walkow et al. (2021) demonstrated that the decision to switch tasks can be predicted by the priority moderator alone or through a combination of interest, salience, and difficulty in the STOM model. Which predictor is better, appears to depend on the specific task and how priority is implemented. For instance, Gilbert and Wickens (2017) found that participants spent more time on a high priority task when they set their own priority levels. Further, theories of motivation such as expectancy-valence theory suggest that individuals consider the importance of obtaining a goal and the expected outcome when managing tasks (Kernan & Lord, 1990). In other words, they will evaluate which task takes highest priority and allocate their resources to complete that goal effectively. Consequently, it was predicted that high priority interrupting tasks would be accepted more often than low priority tasks.
The cost of the interruption can be thought of as the effort needed to be expended when accepting/switching to the interrupting task. This concept has been incorporated in statistical models used to predict the disruptiveness of interrupting tasks (Freed, 1998, Horvitz et al., 2004); however, the cost construct has not been investigated within the purview of interruption research. Cost of compliance has been examined with respect to heeding safety warnings (Dingus et al., 1991; Wogalter et al., 1989). In these studies, participants were more likely to comply with safety warnings and use safety equipment when it was in close proximity than when it was located in another area far away. Thus, cost was manipulated in the current experiment by proximity. Low-cost tasks could be performed in the area where the interruption signal originated. High-cost tasks required participants to move to a different location. Accordingly, it was predicted that low-cost tasks requiring less effort would be accepted more often than high-cost tasks.
The method of the interruption is the source of the interruption signal (e.g., face-to-face interactions, phones calls, or e-mails). Nees and Fortna (2015) compared how face-to-face and virtual interruptions influenced the interruption process and found that face-to-face interruptions caused participants to change to the interrupting task faster than virtual signals. Thus, the method of interruption compared alarm signals and face-to-face interruptions. Alarms were chosen as the method of interruption due to the overwhelming number of alarms that have been documented in telemetry monitoring which can lead to alarm fatigue and desensitization (Sendelbach & Funk, 2013). Regarding face-to-face interruptions, Gupta et al. (2013) suggested that receiving interruptions from supervisors could trigger evaluative pressure. According to distraction conflict theory evaluative pressure could cause one to strain their attentional resources resulting in worse decision-making (Baron, 1986). Therefore, face-to-face interruptions were expected to be accepted more than alarm interruptions.
Method
The current study used a healthcare paradigm to examine the effects of three moderators (priority, cost of the interruption, and method of the interruption) on the interruption decision-making process. Sixty undergraduate psychology students with no formal healthcare experience participated in this IRB Exempt study.
Participants were introduced to the simulated healthcare environment and given a 20 min training session that involved instructions on how to perform the primary and interrupting tasks, and information about the consequences of not performing certain tasks. The primary task required participants to update patient charts by entering missing medication information with the use of a medication book located at their workstation. The participants were also required to monitor two EKG displays that would signal interrupting tasks via alarms. All alarm interruptions were controlled by the experimenter using The Laerdal Learning Application (LLEAP; version 8.4.0.7493; Laerdal Medical, Stavanger, Norway) to manipulate the EKG vitals or send them automated alerts over Zoom.
Participants were assigned to one of three moderator groups (priority, cost, or method). Each group experienced four interruptions over the course of 40 min. Interruptions occurred during the primary task at the same time point for every moderator condition. Participants had the freedom to accept or reject every interrupting task. The criterion for accepting an interruption was performing the interrupting task immediately and shifting focal attention away from the primary task. By contrast, if the participant returned to the primary task after acknowledging the interrupting signal, the interruption was considered as rejected. Participants still had to complete rejected interrupting tasks before the end of the experiment.
The four interruptions were split to have two high levels and two low levels (see Table 1). Each moderator condition manipulates one moderator while keeping the other two at a constant low level. The two high priority tasks involved red alarms from the EKGs that indicated the patient was experiencing a safety critical condition. To accomplish this task, participants would inform the nurse experimenter in charge of the patient to resolve the issue. The two low priority tasks required the participant to alert the nurse experimenter to turn on a blood pressure vital when it malfunctioned and to shred old patient charts. Participants were not told the priority of the interrupting tasks but were informed about the tasks and potential consequences and were left to make their own decision.
The Interrupting Tasks.
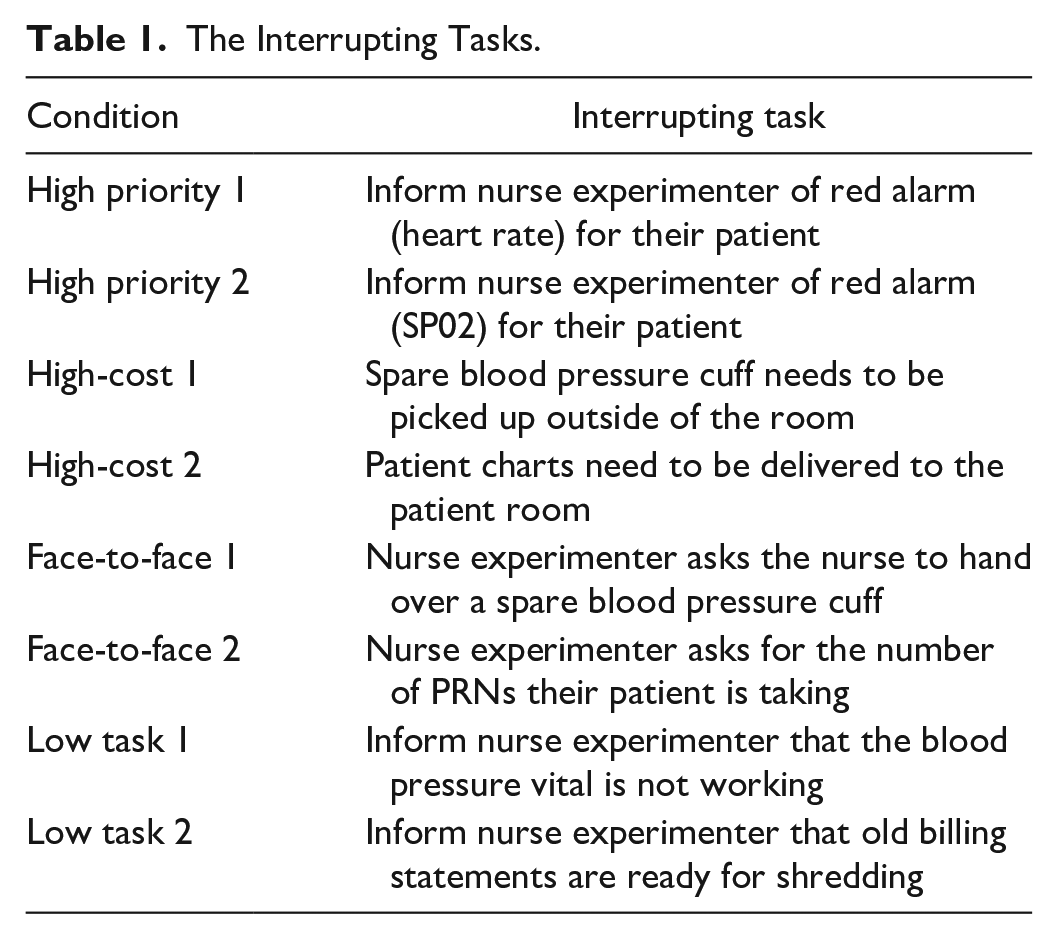
Participants in the cost condition experienced two high-cost tasks and two low-cost tasks. Cost was manipulated by the effort needed to perform a task, either at the participant’s workstation (low cost) or in another location requiring participants to leave their workstation (high cost). The high-cost tasks involved delivering patient charts to a patient room and picking up a spare blood pressure cuff for their patient. The low-cost tasks were identical to those used in the priority condition.
Participants in the method condition experienced two face-to-face and two alarm interruptions. The method of interruption was trigged either by an automated alert or having the experimenter make the request in person. The face-to-face interrupting tasks were triggered when the nurse experimenter asked the participant to count the number of medications in the patient chart and to handoff old patient charts. The alarm interrupting tasks were the same low tasks used in the priority and cost conditions.
The primary outcome was the participant’s binary decision whether to accept or reject an interruption. Errors on the charting task were recorded to determine whether differences in the interruption conditions would affect primary task performance. After the experiment, participants filled out three surveys: a priority assessment, an interruption assessment, and the NASA TLX (Hart & Staveland, 1988). The priority assessment was a manipulation check assessing the participants’ subjective priority ratings of the interrupting tasks. The interruption assessment was a subjective rating of whether the participants would accept or reject interruptions. The NASA TLX was used to gather subjective ratings of workload as to whether there were differences between moderator conditions.
Results
The experimental design was a 3 (moderator condition) × 2 (high vs. low) mixed subject design. A chi-square test was used to compare the differences among the three moderator conditions. There was a significant difference among the moderator conditions, X2 (2, 165) = 8.63, p = .13, w = .229. Those in the priority condition accepted 60 of the 80 interrupting tasks. Participants in the cost condition accepted 35 of the 80 interrupting tasks and 70 of 80 interruptions were accepted in the face-to-face conditions.
Every moderator condition included four decisions to accept or reject an interruption. Therefore, the decision-making process was investigated using the Cochran’s Q-test. There was a significant difference for decision-making in the priority condition X2 (3) = 13.39, p = .004. A McNemar pairwise comparison was run to understand the difference between the four interruptions. High priority task 1 was accepted more than low priority task 2.
There was also a significant effect for the cost of the interruption condition, X2(3) = 19.80, p < .001. A McNemar pairwise comparison demonstrated that the low-cost 1 interruption was accepted more often than the both high-cost interruptions.
The method of the interruption demonstrated a significant difference between the alarm and face-to-face conditions, X2 (3) = 18.43, p < .001. The two face-to-face interruptions were accepted more often than the alarm 2 interruption.
A mixed ANOVA was run to see if there was a difference between the moderator conditions (priority, cost, method) on the total errors made on the two patient charts. No significant differences among the moderators were found, F(2.57) = 2.493, p > .05. However, there was a significant difference in the number of errors made tied to the order of patient charts t(59) = 2.95, p = .005. More errors were made on the first patient chart (M = 3.32, SD = 2.31) than the second patient chart (M = 2.55, SD = 1.68).
Multiple one-way ANOVAs were run to investigate differences in subjective workload among the three moderator conditions. A significant difference was found on the performance; F(2.57) = 3.65, p = .03, η2 = .11; and frustration subscales; F(2.57) = 3.74, p = .03, η2 = .12). Participants in the cost condition thought they performed better those participants in the priority condition and those in the priority condition felt more frustrated than those in the cost condition. No other significant differences were found among the NASA-TLX scores.
Last, the task priority assessment demonstrated that participants indeed rated the high priority manipulations as high. The interruption assessment demonstrated that participants were more likely to accept interrupting tasks when they felt they were more important than the current task and more likely to reject when the interruption when they had to go to a location that was far away from their workstation.
Discussion
The current study investigated how three moderators influenced the decision to accept or reject an interruption. It was demonstrated that all three moderators influenced the interruption decision-making process. First, it was predicted that high priority interrupting tasks would be accepted more than low priority tasks and the results confirmed this prediction. This finding can be tied to expectancy-valance theory which highlights the importance of goals and expected outcomes when managing tasks (Kernan & Lord, 1990). Overall, participants in the priority condition managed their resources efficiently by accepting tasks they considered high priority. Although previous task switching research found mixed findings for the effects of priority (Barg-Walkow et al., 2021; Wickens, 2016; Zabala & Gutzwiller, 2021), it may be the different outcomes are tied to the method of manipulating priority. In the present study, participants determined their own priority in line with Gilbert and Wickens (2017). As a result, high priority tasks were treated as such by participants.
One unexpected finding was that the low priority task of informing the nurse experimenter that the blood pressure vital was not working on the EKG monitor was perceived as a high priority task. In fact, participants rated this task as the second highest priority. The participants were initially instructed that it was okay to leave the blood pressure unmonitored for a period of time; however, participants still treated it as a high priority to make sure the vital was fixed.
With respect to the cost moderator, low-cost interruptions were expected to be accepted more than high-cost interruptions and the results supported this prediction. Regarding the interruption cost, the high-cost interruption tasks were located inside and outside the lab and both locations seemed to represent a high cost since participants rejected these interruptions more often than the low-cost interruptions. These results are consistent with findings from the cost of adhering to safety warning research (Dingus et al., 1991; Wogalter et al., 1989). Collectively, they demonstrate that the effort needed to tend to an interruption or follow safety instructions is affected by proximity. An interrupting task was accepted more often when it was in a convenient location rather than far away.
Finally, it was predicted that face-to-face interruptions would be accepted more often than alarm interruptions. In the present study, the face-to-face interruptions did not have any consequences for delaying them; however, every instance was accepted by participants. This result is consistent with the arguments offered by Baron (1986) and Gupta et al. (2013) who suggested that the personal nature of these interruptions produces social pressure making them difficult to resist.
Turning to the primary task, interruptions had no effect on how participants handled the patient charts. The only significant difference that emerged regarding errors was between the two patient charts. Participants made more errors on the first patient chart than the second patient chart. The order of the patient charts did not vary between moderator conditions. One explanation for this finding was that participants improved their performance while working on the tasks. Alternatively, the first patient chart could have been more difficult than the second patient chart.
Likewise, there were not many differences in mental workload. The results of the NASA TLX were limited to differences between the priority and cost conditions on the performance and frustration subscales. Those in the cost condition thought they performed better than those in the priority condition. Recall that participants in the high priority condition accepted more interrupting tasks than those in the cost condition. Participants in the priority condition also felt more frustrated than those in the cost condition. One interpretation of this finding is that because participants accepted more interruptions in the high priority condition, they may have felt less able to manage their tasks (although it did not affect their accuracy). Also, the priority condition was the only condition that had red alarms. Thus, it may be that the red alarms increased feelings of urgency and anxiety over the interruptions in the cost condition.
Conclusion
Collectively, the results show that individuals make decisions to accept or reject an interrupting task and that the decision is indeed affected by different conditions/moderators. Understanding what influences the decision-making aspect of interruptions can help provide guidance for workers to better minimize their disruptiveness. Further, these results may help system designers adopt appropriate moderators for interrupting signals to better distinguish important tasks from more trivial tasks.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.