
Abstract

Objective
Heavy nursing workload presents a significant challenge in the neonatal intensive care units (NICU) since it is closely associated with adverse patient safety outcomes such as missed care (Tubbs-Cooley et al., 2018), medication errors (Nawwar et al., 2015), hospital-acquired infections (Stone et al., 2008) and mortality (Callaghan et al., 2003). While multiple studies examined the challenges encountered by intensive care unit (ICU) nurses that contribute to their high workload (Gurses et al., 2009; Mohammadi et al., 2015; Rivera et al., 2021), most of these studies were done in adult ICUs, with limited investigation in the NICUs that have their own unique complexities of caring for critically ill infants. These infants, whether premature or full-term but unwell, are susceptible to even minor variations in care due to their fragility, underdeveloped organs, weight-dependent medication requirements, limited communication abilities, and susceptibility to environmental stressors (Raju et al., 2011). Although there has been research focused on the subjective measurement of perceived nursing workload in the NICU (Hoogendoorn et al., 2021; Hoonakker et al., 2011; Tubbs-Cooley et al., 2018), there is a research gap in comprehensive and contextual understanding of work system-based challenges that may lead to unanticipated increases in nursing workload in the NICU. In this study, we implemented a qualitative research approach guided by a conceptual framework of nursing workload (Carayon & Gürses, 2005) to identify these unanticipated challenges experienced by NICU nurses that may increase their workload unexpectedly. Additionally, using a Safety-II approach (Hollnagel, 2018), this study explores strategies that these frontline care professionals self-develop and employ to mitigate the effects of these challenges. Moreover, this is also the first study looking at overall “ICU nursing workload management” from a Safety-II perspective.
Approach
The study involved a 3-hour observation of 12 bedside NICU nurses at an academic hospital, followed by a 30-minute semi-structured interview. Observations were conducted across weekdays and weekends, with each session randomly distributed over the beginning, middle, and end of the participant’s selected 3-hour work shifts. The median of experience in years among nurses was 4.5, ranging from one to 25 year. The observation data was collected using an observation tool developed and pilot-tested in previous research (Gurses & Carayon, 2007) combined with handwritten descriptive notes. Semi-structured interviews were conducted with the participants within 1 to 7 days after the observation. The interview guide consisted of two major subsections: (1) questions on unanticipated changes/challenges that contributed to high workload during the particular observation session, and (2) questions on challenges that increase workload unexpectedly based on overall past work experience of the participating nurse. Additionally, participants were asked about any strategies they have either self-developed or learned from others and used to overcome these unexpected challenges and spikes in their workload. Handwritten observation notes were typed immediately after each observation session, and interviews were audio-recorded and transcribed. A blend of deductive and inductive approaches were utilized to analyze the data: A deductive approach was crucial as an established conceptual framework (Gurses & Carayon, 2007) to steer our study and an inductive approach is indispensable for capturing concepts that may not be explicitly articulated within existing framework.
Findings
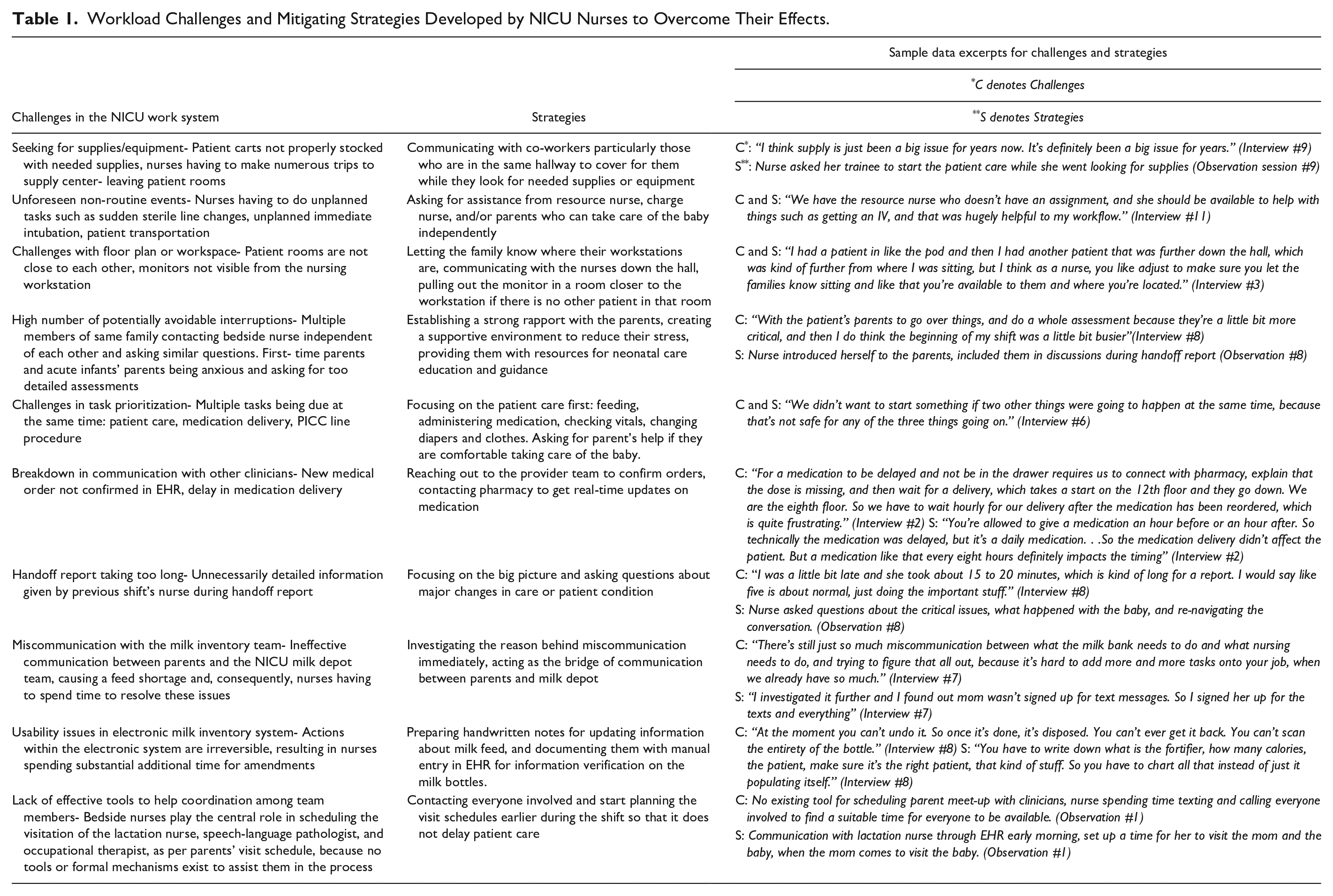
Analysis revealed 10 major categories of challenges in the NICU work system that consistently contributed to high nursing workload in the NICU: (1) Seeking for supplies/equipment, (2) Being have to attend to non-routine/unforeseen patient-care events (e.g., sudden need for sterile line change), (3) Challenges with floor plan or workspace (e.g., patient rooms not close enough), (4) High number of potentially avoidable interruptions, (5) Competing demands with no clear guidance on how to prioritize, (6) Breakdown in communication with clinicians, (7) Handoff report taking too long, (8) Ineffective communication with the milk inventory team, (9) Usability issues in electronic milk inventory system, (10) Lack of tools to help with team coordination. Our results indicate that NICU nurses strategize to mitigate the effects of these high workload challenges. Examples to major strategies include (i) asking for help from the NICU unit, specially from nurses in the same hallway or the resource nurse on the shift, (ii) establishing strong rapport with the family members early in their NICU journey, (iii) making small modifications in their workspace, (iv) planning ahead for scheduled events as early as possible to have buffer, (v) prioritizing clinical tasks over others (e.g., documenting), (vi) taking primary role in clarifying communication between parents and other healthcare professionals in the NICU (see Table 1 for details). Future steps include collecting additional data for a thorough and detailed analysis, where we will aggregate observational and interview data and develop a comprehensive coding scheme to systematically categorize challenges and strategies for overcoming them.
Workload Challenges and Mitigating Strategies Developed by NICU Nurses to Overcome Their Effects.
Takeaways
The theoretical contributions of this study lie in the exploration of the perspectives of the Safety-II framework (Provan et al., 2020) for workload management at the frontline by emphasizing the different ways of adapting to gaps, challenges, and surprises and by identifying strategies to overcome or mitigate the impact of high workload. Further, by uncovering specific unanticipated changes or spikes in workload and their implications for workload management, this study sheds light on where intervention efforts should focus to reduce nursing workload in the NICUs. Research efforts are ongoing to uncover challenges and strategies to reduce workload in the healthcare environment and our study provides further empirical evidence for this type of research. Collectively, the systematic examination of tailored workload management strategies presented in this study contributes to field discussions on healthcare system efficiency, resource allocation, interventions to optimize nurse performance, and efforts to reduce stress and improve job satisfaction.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by grant number R01HS028430 from the Agency for Healthcare Research and Quality. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality.