
Abstract
Emergency responders such as firefighters, police officers, and emergency medical service (EMS) providers are exposed to significant risks of mental health issues, including depression, anxiety, post-traumatic stress disorder (PTSD), and suicidal ideation. Existing psychological interventions are focused on improving generic coping skills rather than dealing with the link between the memory of the adverse event and its reexperience. In this regard, this paper introduces a novel framework to address mental health problems among first responders by examining the impact of active virtual reality (VR) on memory and emotion following indirect exposure to an adverse event. Especially, we hypothesize that semantically irrelevant VR experience suppresses the retrieval of the memory of the adverse event and alleviate associated emotion. Our study consists of three stages: (a) watching a video of a severe car accident, (b) doing a semantically irrelevant VR activity (exploring a natural environment), and (c) taking a recall-based memory test of the car accident. To assess the changes in emotion, the Positive And Negative Affect Schedule (PANAS) survey is used before watching the car accident video, after watching the video, and after performing the VR activity. In addition, participants’ heart rate and eye tracking measures are collected to understand how physiological and eye movement changes along the phases. Expected findings will inform the design of the VR-based mental health interventions and highlight VR as an effective tool for addressing mental health challenges faced by first responders.
Introduction
Emergency responders are frontline workers who protect citizens and communities from adverse events such as emergencies, accidents, and disasters. However, the nature of their work exposes them to significant risks of mental health issues such as depression, anxiety, post-traumatic stress disorder (PTSD), and suicidal ideation. These issues are largely incurred by directly witnessing human deaths and sufferings, putting themselves into harmful and violent situations, and enduring intensive physical and cognitive workloads. According to previous studies, more than 22% of firefighters in the US were at a high risk of depression (Haddock et al., 2017). Approximately 50% of police officers involved in the September 11 World Trade Center attack suffered from severe depression and anxiety (Bowler et al., 2016). Additionally, over 50% of US firefighter deaths were related to stress and exhaustion (Dowdall-Thomae et al., 2012). In Germany, 17% of emergency physicians experienced PTSD (Pajonk et al., 2012) whereas 19% of police officers involved in Hurricane Katrina reported that they suffered from PTSD (McCanlies et al., 2014). Regarding suicidal ideation, 46.8% of US firefighters in 2015 had suicidal thoughts, plans, or attempts (Stanley et al., 2015), and 37% of fire and EMS personnel contemplated suicide, which was approximately 10 times the rate of American adults (Abbott et al., 2014).
Various psychological interventions have been developed to address the mental health problems among emergency responders. Winders et al. (2021) highlighted the effectiveness of Critical Incident Stress Debriefing (CISD), also known as psychological first aid, wherein responders share their experience, and emotion after dealing with a traumatic event and receive supports to attenuate negative feelings. Mindful meditation offers mental training to manage racing thoughts and negative emotions. Also, Cognitive Behavioral Therapy (CBT) and Exposure Therapy (ET) are often used as a psychological treatment for mental health issues among emergency responders (Winders et al., 2021). The CBT is a structured approach for teaching coping skills, while the ET aims to desensitize individuals to the sources of fear and anxiety by gradually exposing them to a weaker level of exposure. In addition, pre-traumatic vaccination (PTV), usually incorporated with the ET, offers exposure-related coping strategies to mitigate the impact of future adverse events. Despite the effects of these psychological treatments, several gaps remain. Existing interventions were focused on developing generic coping skills rather than addressing the very root causes of mental health issues, which are related to the retrieval of the memory of an adverse event and accompanied bodily reactions. For example, the CBT is aimed at changing the ways of thinking and acting in case where individuals face future situations that impose fear and anxiety. In a similar sense, the ET does not deal with the individual’s previous experience with the source of phobia, but makes the individual insensitive to the future fearful situations (e.g., walking at height). Thus, there has been little research focusing on developing interventions on the memory of the adverse event.
To bridge this knowledge gap, our study aims to use virtual reality (VR) to intervene in the memory of adverse events. Figure 1 illustrates the cognitive processing model of PTSD as the theoretical framework to understand the psychological processes involved in mental health issues among the responders (Ehlers & Clark, 2000).
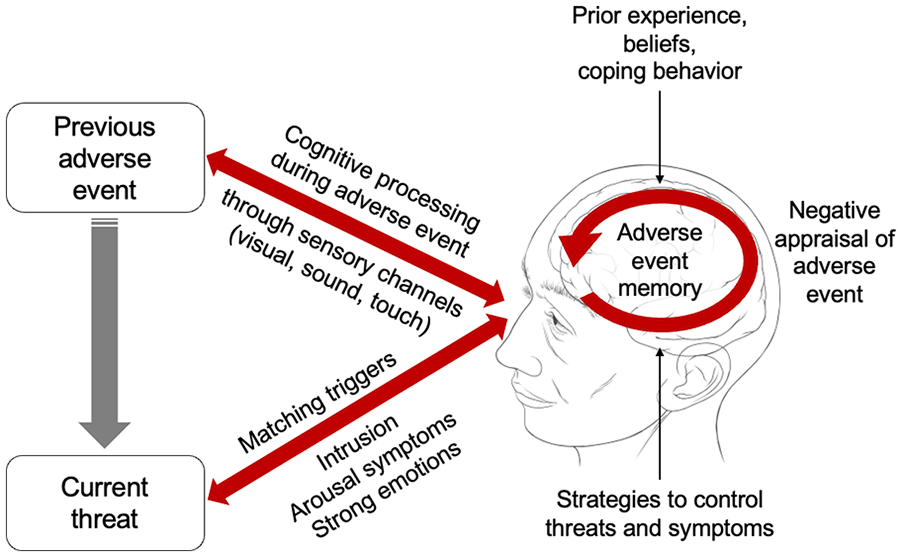
Cognitive model of memory and emotion of an adverse event.
This model posits that negative appraisal of an adverse event is reinforced as current threats trigger the reexperience of the adverse event without positive coping strategies to control the acceptance of the threats. Once an individual experiences or witnesses a severe incident (e.g., trauma) via multiple sensory channels such as visual, auditory, and tactile modalities, such an experience or witness becomes the memory of the incident. This perceptual process is influenced by one’s prior experience, belief, and coping behavior. When the individual encounters similar threats to what previously caused the fear, arousal symptoms, and strong emotions are triggered. If the individual does not have positive coping skills (e.g., cognitive reframing, meditation, deep breathing), then the previous experience and witness of the adverse event is negatively appraised, leading to fear, and anxiety.
Based on this model, it is hypothesized that if the retrieval of the memory of the adverse event is blocked or suppressed, then the negative appraisal of the adverse event will not occur. In our study, an active VR experience, in which a person performs psychomotor activities, is used as an instrument to suppress the retrieval of the adverse event memory. In particular, our study uses semantically irrelevant VR experiences to facilitate the suppression effect. In other words, exposing the individual to a situation that is distantly connected to the adverse event will make it easier to suppress the retrieval of the memory of the adverse event and reduce negative emotion caused by the adverse event.
Method
Three-stage Scheme
To investigate the impacts of a semantically irrelevant active VR experience on the memory of an adverse event and associated emotion, a three-stage experiment is used. The three-stage scheme has been widely employed to examine various cognitive phenomena such as the misinformation effect (Tousignant et al., 1986), which was to assess the accuracy of the memory of the initial information followed by the secondary, false information.
In the first stage of our study, participants are indirectly exposed to an adverse event through a short video (2–3 min) displayed on a computer screen. This video features a traumatic event such as severe fire, human injury, car accident, terrorism, or domestic violence in purpose of provoking both physiological and emotional responses as would be experienced in real-life traumatic situations. This video is intended to create the memory of a traumatic incident and render negative emotions associated with the incident.
Following the initial, indirect exposure to an adverse event, the second stage makes the participants in the intervention group experience semantically irrelevant VR activities. Semantically irrelevant activities refer to tasks that do not have meaningful associations or relationships with a previous experience. According to Storey (1993), there are various types of associations between concepts, words, or contents. Such relationships include part-whole relationship (e.g., tree–forest), case relationships (e.g., customer–shopping), antonyms (e.g., stopping–moving), and synonyms (e.g., worker–employee).
In our study, the semantically irrelevant content to the traumatic event such as fire and car accident is an activity like surfing in the sea and walking inside a think forest. These activities also require the participants to perform psychomotor actions, which involve their cognitive processes (e.g., perception, decision-making). Participants in the control group do not experience the active VR and remain seated without doing any cognitive or physical task.
In the third stage, all participants in both conditions take a recall test designated to assess their memory of the initial adverse event (e.g., fire, car accident). This recall-based test asks the participants about details in the adverse event video presented in the first stage. For example, the questions are concerned with the injury conditions of the victim in the video, the sequence of the incident, details about the response.
Experimental Design and Data Collection
A between-subject experiment is used in this study with random assignment of participants to either the control or intervention group. Figure 2 illustrates the overall process of the experiment. The first stage, where the participants watch a short video of a traumatic event, remains the same for both groups. In the second stage, the participants in the control group remain seated without any activity (i.e., do nothing) whereas the participants in the intervention group perform VR activities that are semantically irrelevant to the video they watched in the first stage.
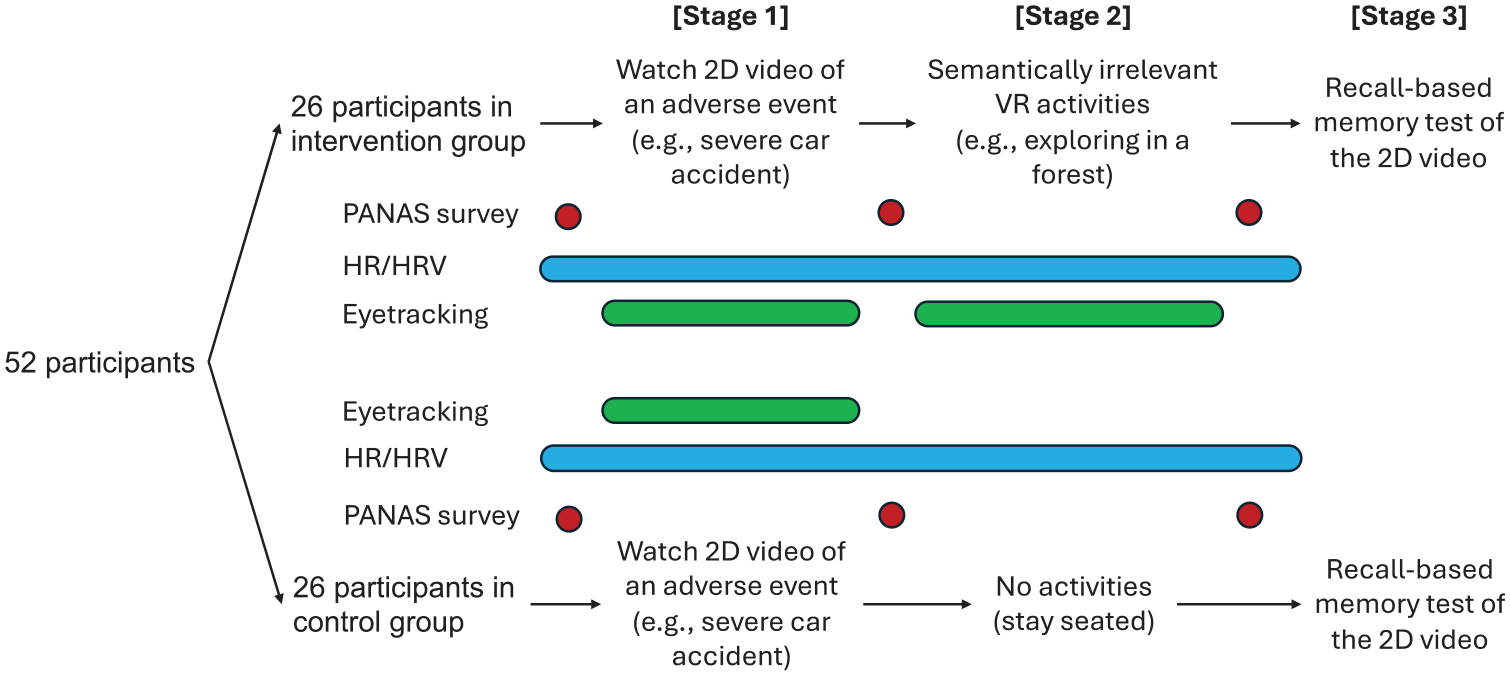
Overall process of the experiment.
Before watching the video, participants in both groups undergo pre-experiment data collection. This baseline data includes the Positive And Negative Affect Schedule (PANAS) survey (Watson et al., 1988) to obtain baseline levels of positive and negative emotions. Alongside the PANAS, the participants’ heart rate (HR) and heart rate variability (HRV) are collected using a Polar H10 device to assess physiological conditions right before the experiment begins. Following the first stage (watching the video of an adverse event), participants take the PANAS survey again to report changes in their affective states. The HR and HRV data is continuously collected throughout the stages. Especially during the video watching, eye tracking measures are obtained, including eye fixation rate and gaze entropy using a Tobii Pro Fusion Eye Tracker. The purpose of eye tracking measurement is to identify how the participants watch the video and whether the participants pay attention to the areas of interest (AOI) of the adverse event (e.g., victims, sources of danger, and surrounding environment).
In the second stage, the participants in the intervention group perform semantically irrelevant VR activities (e.g., exploring the nature) whereas the participants in the control group stay seated without any physical or cognitive task. After the VR activities, the participants fill out the PANAS survey for the third time to indicate emotional states rendered by the VR activities. While performing the VR activities, eye tracking measures are obtained to understand the visual scanning patterns of the participants in the intervention group.
In the third stage 3, a recall-based memory test is conducted for both groups to examine the participants’ memory of the adverse event presented in the first stage. Questions of the recall-based memory test ask the participants to describe sources or events of threats such as injury conditions of the victims, sequence of events that occurred during the accident, behavior of the responders, and surrounding environments.
A required sample size for this experiment was obtained using G*Power 3.1.9.7 software program. The effect size was set to be medium (=0.4) and a significance level (alpha = .05) with two conditions. A total of 52 participants is required to achieve a sufficient statistical power. One-way ANOVA will be conducted to identify effects of the VR intervention on memory accuracy, PANAS score, HR, HRV, and eye-tracking measures.
Expected Results and Implications
It is expected that the outcomes of this study offer valuable insights into developing VR-based interventions to address mental health problems among emergency responders, in line with recommendations suggested in the literature (Son, 2023). The semantically irrelevant VR activities are intended to suppress the retrieval of the memory of traumatic events and reduce associated psychological reaction. Thus, we anticipate that the VR activities make it difficult to recall what the participants have watched in the accident video. Apart from the “memory suppression effect” of the semantically irrelevant or distant follow-up VR experience, we also expect this VR experience would alleviate negative emotion rendered by watching the video of an adverse event and stimulate positive affect by putting the participants in soothing and calming virtual environment. This is analogous to “a virtual getaway” that takes a person who had experienced or witnessed a traumatic incident (e.g., emergency responders) to a very different place such that the person does not encounter similar threats or conditions that caused fear and anxiety. In addition to the memory and emotional change by the VR experience, our study will provide the benefits of using HR and HRV data to correlate physiological changes with self-reported measures like PANAS survey. Also, the eye tracking measures will unveil the visual scanning patterns of the participants when they watch the accident video and perform the VR activities.
The design of the current study is predicated upon findings and limitations of our previous study (Parker et al., 2024, in preparation), which failed to generate a significant effect on the memory of an adverse event (house fire) yet identified significantly different positive and negative emotion after having “passive (i.e., watching)” semantically irrelevant VR content. We speculate that the adverse event (house fire) did not sufficiently render disturbing reactions among the participants. Passive VR where the participants simply watched the 360° immersive VR video was considered ineffective in suppressing the memory of the fire incident.
The current study employs a recall-based memory test whilst our previous study used a recognition-based test in which visual cues (snapshot photos of the house fire video) were provided for the participants to choose between a true photo and a fake photo fabricated with image AI tool (Adobe Firefly). However, it was questionable that the false components of the photo were critical elements of the adverse event. Furthermore, the absence of pre-experimental baseline data hindered the comparison of emotional (PANAS survey) and physiological responses (HR, HRV) before and after exposure to the video of an adverse event and the semantically irrelevant VR experience.
Additionally, the current study uses a more disturbing video (e.g., severe injury from a car accident) in the first stage while ensuring the participant’s psychological safety by adhering to exposure limits.
We expect that these methodological adjustments lead to stronger evidence for the effects of a semantically irrelevant active VR intervention for the mental health issues induced by frequent exposure to traumatic incidents. Ultimately, findings from our study will the development of VR-based mental health solutions for a broader scope of emergency response personnel.
Conclusions
The current study introduces a novel VR-based intervention aimed at addressing the mental health challenges faced by emergency responders. Our intervention attempts to generate “memory suppression effect” using a semantically irrelevant VR experience after watching or witnessing a traumatic incident. Combining with other existing mental health solutions such as the CBT and medication, we believe our VR-based approach would enhance the mental health of emergency personnel.
Footnotes
Acknowledgements
The authors would like to thank first incident responders who always take risks to bring safety and well-being to the community.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partially supported by the National Academies of Sciences, Engineering, and Medicine (NASEM) Gulf Research Program (GRP) Early-Career Research Fellowship (ECRF No. SCON-10000968).