
Abstract
Background:
With the growing popularity of total ankle arthroplasty (TAA), there is an expectation that revision surgeries will increase. However, limited data exist on revision TAA outcomes using a revision-specific implant. The INVISION Total Ankle Revision System is a modular revision implant (Wright Medical Group/Stryker). The purpose of this study was to report implant survivorship, complications, and radiographic and clinical outcomes of revision TAA using the INVISION system at a minimum 2-year follow-up.
Methods:
A retrospective review was conducted of 27 patients that underwent a revision TAA using the INVISION implant at a single institution with minimum 2-year follow-up between 2016 and 2020. Implant survivorship was the primary outcome. Demographics, complications, reoperation, and radiographic and clinical outcomes were recorded.
Results:
Implant survivorship was 81.5% (22/27) at a mean of 3.6 years following revision TAA using the INVISION implant. There was evidence of aseptic loosening in 3 patients and talar subsidence in 4 patients on final radiographs. Reoperation rate at final follow-up was 40.7%, most commonly for aseptic loosening (n = 3), septic TAA (n = 2), or gutter impingement (n = 2). The mean American Orthopaedic Foot & Ankle Society (AOFAS) total score was 54.5, Foot and Ankle Ability Measure (FAAM) activities of daily living (ADL) subscale score was 52.9, and FAAM Sports was 31.0.
Conclusion:
Revision TAA using the INVISION implant demonstrated 81.5% implant retention at a mean of 3.6 years in this complex cohort. Patient-reported outcomes were lower than those reported after primary TAA. Physicians and patients should recognize that revision TAA remains a challenging procedure with a high rate of complications and reoperations.
This is a visual representation of the abstract.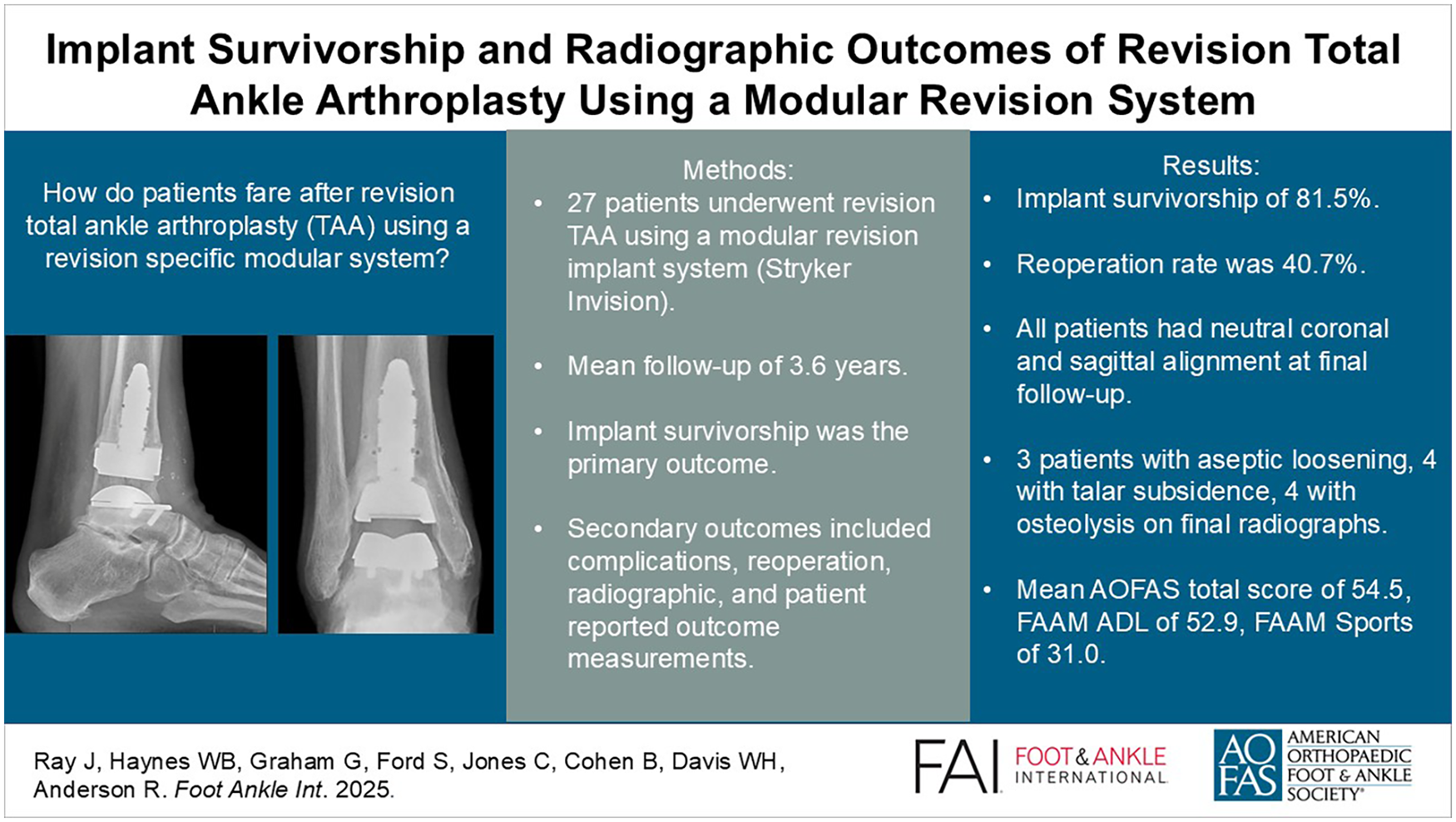
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.