
Abstract
Background:
Hallux valgus (HV) is a common foot deformity that can cause significant discomfort. Surgical correction of hallux with minimally invasive surgery (MIS) has been gaining popularity in recent years among surgeons. The use of allograft in traditional open approaches has been proposed to improve the outcomes of foot and ankle procedures by expediting time to union. We performed a retrospective analysis of patients undergoing MIS HV correction with and without the allograft at the time of surgery. The primary aim of our study was to determine if use of allograft in HV MIS correction led to different time to union as well as rate of unions.
Methods:
A retrospective cohort study was designed to compare the radiographic outcomes of patients who underwent hallux valgus correction with or without allograft. Patients included in the analysis underwent primary HV correction using fourth-generation minimally invasive techniques and had postoperative weightbearing radiographs. Exclusion criteria included revision HV surgery, open surgery for HV correction, and patients lost to follow-up. All surgeries were performed by 3 fellowship-trained foot and ankle orthopaedic surgeons at a single center in Miami, Florida, from September 2019 to December 2022, with only 1 surgeon using allograft. All patients had similar postoperative protocols. The allograft group received 2 mL of a demineralized bone matrix (DBM) gel (Allosync; Arthrex). Radiographs were evaluated by 2 independent orthopaedic surgeons who were anonymized to the patient’s group allocation. The primary outcome of this study was time to radiographic union, defined as formation of 2 neocortices on postoperative radiographs, as well as overall rate of union. The secondary outcomes included a comparison of traditional radiographic measurements and the incidence of complications.
Results:
Sixty-eight patients (68 feet) met inclusion criteria: allograft group (n = 26) and a control group (n = 42). Demographics between both groups were similar. In our study, all 68 feet obtained complete union and no malunions or nonunions were observed in either group. The average time to complete union for the allograft group was 5.69 ± 3.16 months (95% CI 4.45-6.93) and the control group was 6.0 ± 3.95 months (95% CI 4.80-7.19); union times between groups did not reach statistical significance (P = .731). Maintenance of surgical correction was observed in all patients.
Conclusion:
In this study, the use of demineralized bone matrix allograft during MIS HV correction did not result in a statistically significant difference in time to union or overall union rates. Although the allograft group showed a slightly shorter average union time, this difference was not clinically or statistically significant. These findings suggest that the routine use of allograft in MIS HV correction may not provide a meaningful benefit.
This is a visual representation of the abstract.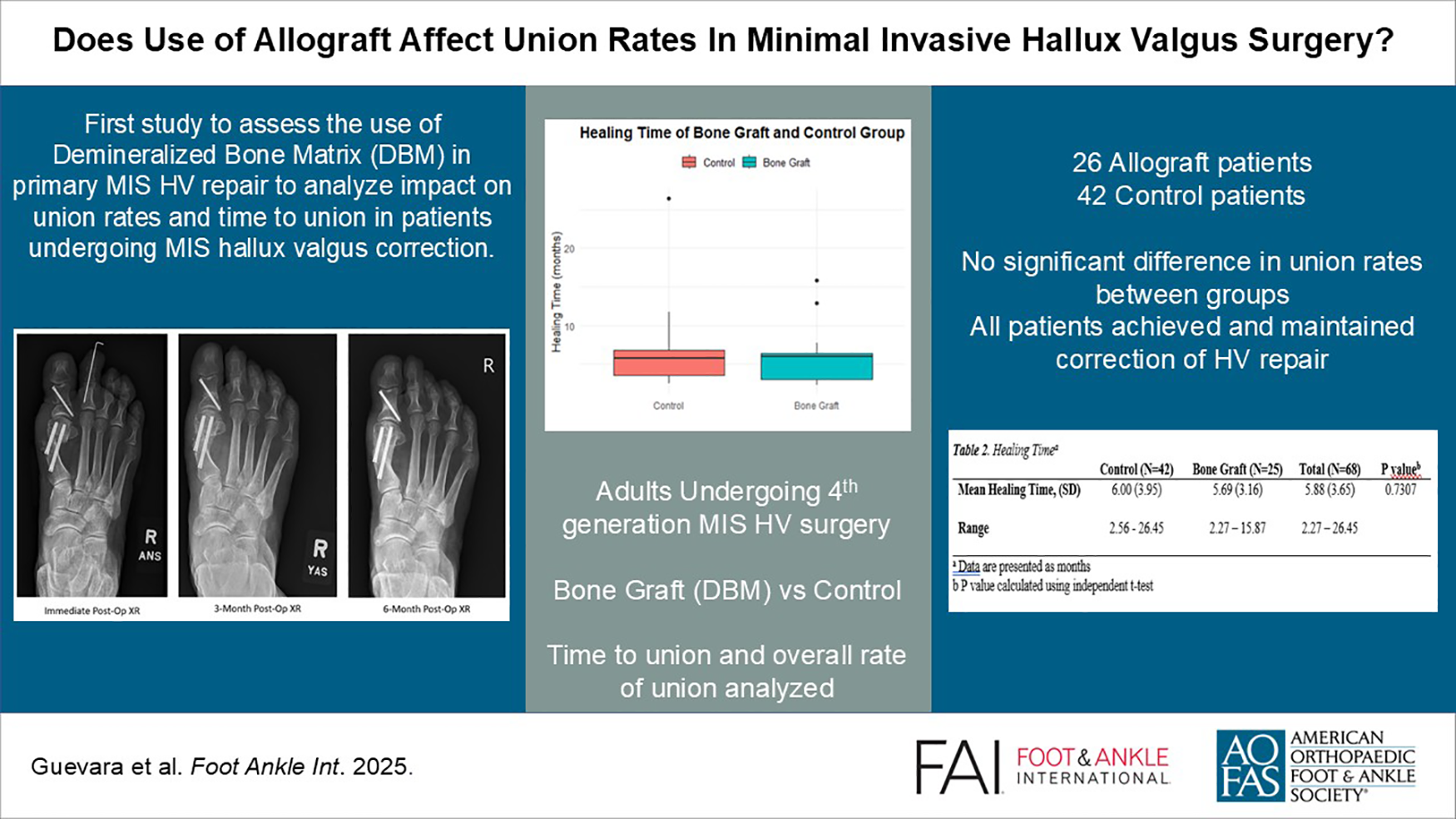
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.