
Abstract
Background:
The choice between primary arthrodesis (PA) and open reduction and internal fixation (ORIF) for acute Lisfranc injuries remains contentious. Apart from primary treatment, arthrodesis is often used for treating chronic Lisfranc injuries, including patients in whom initial ORIF or nonoperative treatment failed. The aim of this study was to compare PA and secondary arthrodesis (SA) in terms of complications and functional outcome.
Methods:
A retrospective cohort study was conducted on trauma patients with Lisfranc injuries treated at a level 1 trauma center between July 1, 2010, and July 1, 2020. Selected patients were evaluated at the outpatient clinic and received a survey. Demographics, injury characteristics, management, complications, and patient-reported outcomes (American Orthopaedic Foot & Ankle Society midfoot score, Foot Function Index) were analyzed.
Results:
Twenty-nine of 37 potential patients (78.4%; PA n = 11, SA n = 18) completed the survey with a median follow-up of 7.1 (PA) to 9.3 (SA) years (P = .01). The majority were female (n = 18, 62.1%); the mean age of PA patients was 57.1 years (SD 14.2) compared with 43.5 years (SD 17.1) in SA patients (P = .04). In the PA group, there was no infection, 100% union, and implants were removed in 5 of 11 patients. In the SA group, 11.1% (n = 2) developed infection, malunion rate was 11.1%, implants were removed in 33.3% (n = 6), and 22.2% required revision surgery. AOFAS was “good” in PA (77.7, SD 17.3) compared with rated “fair” in SA (67.1, SD 21.3, P = .19). FFI was better in PA (26.0, SD 26.2) than SA (37.6, SD 30.8, P = .32), which exceeded the minimally important clinical difference.
Conclusion:
Although this study was limited by sample size, the overall results suggest equivalent functional outcome, pain and treatment satisfaction in primary arthrodesis compared with secondary arthrodesis patients for treatment of Lisfranc injury.
Introduction
The entire spectrum of tarsometatarsal joint fracture-dislocation injuries is referred to as Lisfranc injury, named after the French surgeon and gynecologist Jacques Lisfranc de St Martin (1790-1847). The tarsometatarsal joint complex is composed of the tarsometatarsal joint, cuneonavicular joint, and intercuneiform articulations. 21 The severity of this type of midfoot injury varies from simple to complex, depending on the extent of damage to the joints and bones affected. Representing only 0.2% of all fractures, Lisfranc injuries are rare. 1 Unfortunately, 20% to 40% are overlooked or misdiagnosed, leading to delayed or inadequate management and subsequent poor functional outcome.12,29,30 Because of the effect on both the longitudinal and transverse arches of the foot, Lisfranc injuries can dramatically alter foot biomechanics and affect the patient’s daily activities, including work and sports.6,8
With respect to treatment, primary arthrodesis (PA) vs open reduction and internal fixation (ORIF) has now become one of the main topics of study and debate in retrospective cohorts, RCTs, and meta-analyses.14,18,31 It has become evident that patients may develop painful osteoarthritis after ORIF, with rates reported as high as 94% and a consequent risk of secondary arthrodesis (SA).6,20,21 Some studies indicate that PA may be the superior option because of less secondary surgery, less implant removal, less chronic pain, and higher functional outcome.9,11,14,18 It is advocated especially for pure ligamentous or dislocated Lisfranc injuries. 15 However, contradicting conclusions have been reported and clarity remains yet to be established. 17 Apart from primary treatment, arthrodesis is often used for treating chronic Lisfranc injuries, including patients in whom initial ORIF or nonoperative treatment failed, resulting in posttraumatic osteoarthritis.16,25 Moving to the clinical setting and (shared) decision making in acute Lisfranc injuries, it is essential for patient and surgeon to ascertain what level of functional outcome may be expected in case of SA after failed primary treatment.
Currently, there is a paucity of research on patient-reported functional outcome and complications of patients with acute Lisfranc injuries treated with PA vs SA. The aim of this study was therefore to compare demographics, complication rate, and long-term patient-reported functional outcome, quality of health, and treatment satisfaction.
Materials and Methods
Design and Patients
A retrospective cohort of all trauma patients with Lisfranc injuries who were treated at our level 1 trauma center between July 1, 2010, and July 1, 2020, was analyzed. Institutional review board approval and written informed consent were obtained. Because the Lisfranc joint was defined as the articulation between the tarsus and the metatarsal bases, Lisfranc injury was defined as a very unstable injury that was ligamentous, osseous, or a combination around the Lisfranc joint. Patients were presented to our department with acute injuries or with painful residual deformity following previous Lisfranc injury.
Treatment Rationale
For each case, treatment strategy was decided by 3 foot and ankle surgeons. Nonoperative management was initiated in case of presumed nondisplaced, stable Lisfranc injuries (that were not stable in retrospect). In case of missed diagnosis, no specific treatment had been initiated and consequent conservative measures such as change of footwear, physical therapy, and pain medication had failed to relieve symptoms prior to SA. In general, surgical treatment for Lisfranc injuries in our institution is predominantly aimed at open reduction and joint sparing with bridge plating, although some surgeons prefer transarticular fixation. PA candidates were patients with purely ligamentous injuries with gross dislocation, and those with more than 50% involvement of the TMT joints. Age played a role here as well, where elderly patients (mostly older than 60) were more often treated with primary arthrodesis.
Patient Selection
All patients treated with arthrodesis were selected. Patients who were successfully treated with nonoperative or ORIF treatment were not retrieved from the hospital database. Patients younger than 18 years at the day of injury, patients with compartment syndrome and open fractures were excluded. All patients had at least 3 years of follow-up. Patient-related, clinical, and radiographic data were extracted from the electronic hospital database. Included patients were followed by clinical evaluation at the outpatient clinic and received a questionnaire between 2021 and 2023, at least 3 years after surgery. Loss of follow-up was recorded. This study was conducted in adherence to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Variables
Variables included among others were age at injury, gender, body mass index, tobacco use, mechanism of trauma, injury pattern, number of injured rays, Myerson and Column Involvement Severity System (CISS) classification, and concomitant ipsi- or contralateral lower extremity injuries. 7 Data was collected on the type of treatment, follow-up, complications, functional outcome, and quality of life. Complications were defined as fracture-related infections and delayed union, malunion, or nonunion. Functional outcome was quantified using the Foot Function Index (FFI, best score 0 points), and the American Orthopaedic Foot & Ankle Society midfoot score (AOFAS, best score 100 points). The AOFAS score was divided into groups according to the literature: a score of 90 to 100 was graded as an excellent result, 75 to 89 as good, 50 to 74 as fair, and <50 points was graded as a failure or poor outcome. Assessment of perceived general health was done using a visual analog scale (VAS) of 0 to 10, in which 10 represented excellent general health. Treatment satisfaction was also measured using the VAS of 0 to 10, in which 10 represents the best possible satisfaction.
Statistical Analysis
The statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS), version 29 (IBM Corp, Armonk, NY). Numeric data are expressed with means with standard deviation (SD) or median with range. Categorical data are shown as numbers with percentages. Independent sample 2-tailed t test with a significance level of .05 were used to compare means. A multivariate linear regression was performed to identify independent predictors of complications and functional outcome. Parameters included were age, tobacco use, columns fused, Injury Severity Score (ISS), and early or late diagnosis. A post hoc power analysis was performed.
Results
Demographics
Out of all trauma patients with closed Lisfranc injuries who were treated at our level 1 trauma center between July 1, 2010, and July 1, 2020, 37 patients who were treated with arthrodesis (PA or SA) and met the inclusion criteria were selected. Questionnaires were sent to all patients, of whom 29 responded (n = 11 PA, n = 18 SA), yielding a follow-up rate of 78.4% (Figure 1). The majority were female (n = 18, 62.1%) with an overall median age at the day of trauma of 48.5 (range, 20-80) years. Mean age of patients in the PA group was 57.1 years (SD 14.2) compared with 43.5 years (SD 17.1) in patients with SA (P = .04). Total mean body mass index was 26.8, and 24.1% of patients reported tobacco use (n = 7; no significant difference between groups, P = .33). The majority of SA patients (n = 10, 55.6%) were referred to our tertiary center late (more than 6 weeks) after injury. The median time from injury to referral was 11.7 (range, 3-30) months. Of these late referrals, 5 injuries were initially missed, 3 were treated nonoperatively, 1 was treated with Kirschner wire fixation, and 1 had ORIF.
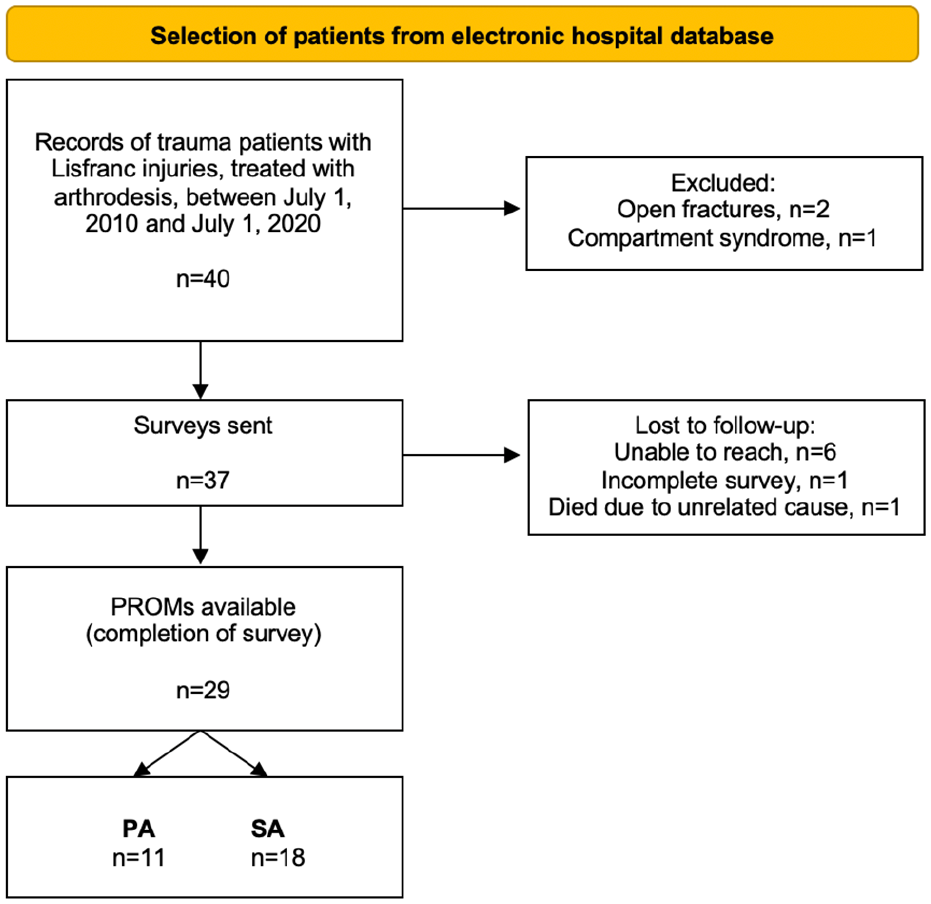
Flowchart of patient selection.
Injury Pattern
The mechanisms of trauma, in descending order of frequency, were fall or inversion during daily activities (n = 13), motor vehicle accident (n = 6), crush (n = 3), sport injuries (n = 3), fall from height (n = 1), and unknown (n = 3). The median Injury Severity Score was 4 for both PA (range 4-12) and SA (range 4-9) patients without a significant difference (P = .57). Ten patients (34.5%) had a Lisfranc fracture-dislocation, ranging from 1 to 5 dislocated tarsometatarsal joints. Five patients had a pure ligamentous Lisfranc injury (all treated with SA), of which 4 were referred 9 months after overlooked diagnosis. The total fracture distribution (including simple, comminuted, and avulsions) is illustrated in Figure 2. Three patients (10.3%) also had an injury to the midtarsal (Chopart) joint (n = 2 PA, n = 1 SA). None of the included patients sustained fractures to the contralateral foot or ankle.
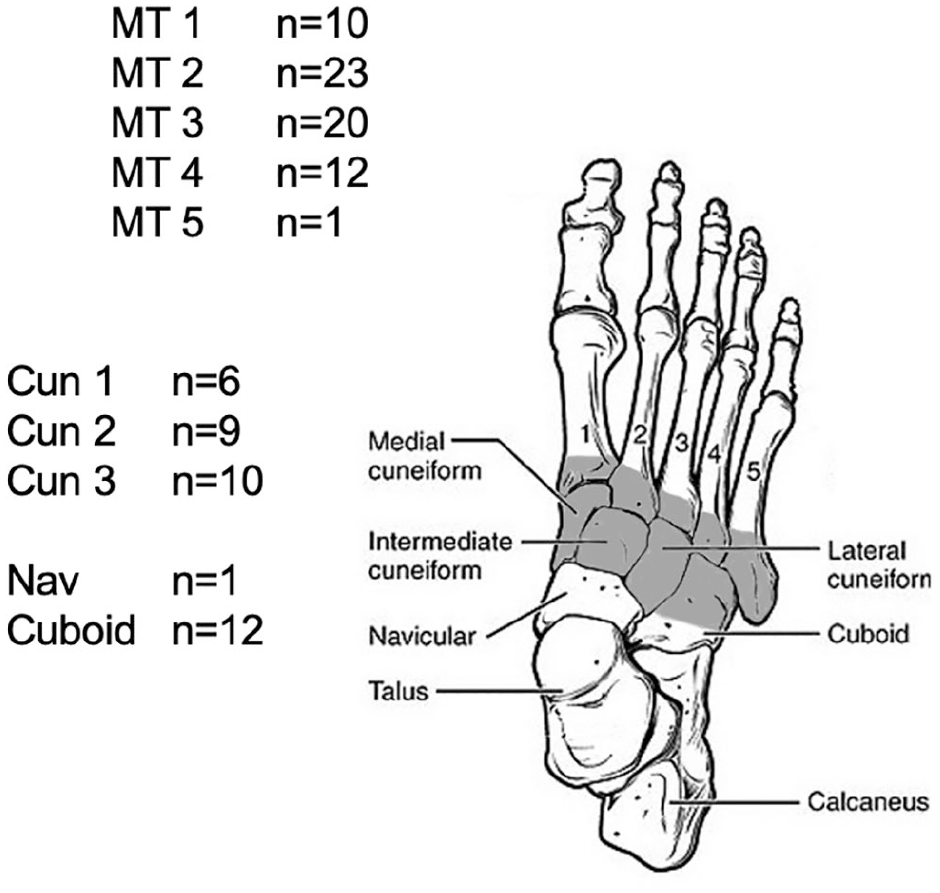
Incidence of injuries in study population, image by OpenStax College (distributed under a Creative Commons Attribution 4.0 license).
Classification
All patients were diagnosed using both conventional radiography and CT imaging. The complete range of Lisfranc injury types was included. Patients were classified according to the Myerson and CISS classification, as illustrated in Tables 1 and 2. Most patients (69% of total) sustained type B2 injury, meaning partial incongruity with lateral displacement of the lesser metatarsals. There were no significant differences in distribution of type A (P = .57), B (P = .56), and C (P = .87) injuries between the PA and SA groups. In terms of CISS, all 3 columns were involved in 48.3% patients (n = 14), and 41.4% of patients had both medial and central involvement (n = 12). The majority of PA patients sustained injuries in 2 columns, whereas the majority of SA patients had injuries in all columns. There was no statistical difference in CISS distribution.
Distribution of Injuries Based on Myerson Classification. a
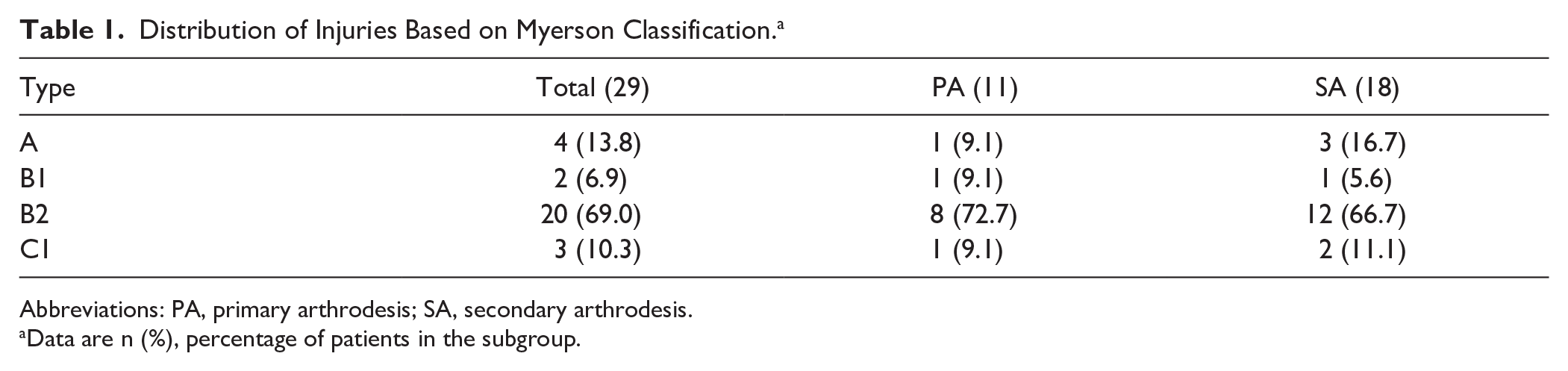
Abbreviations: PA, primary arthrodesis; SA, secondary arthrodesis.
Data are n (%), percentage of patients in the subgroup.
Column Involvement (Based on CISS). a
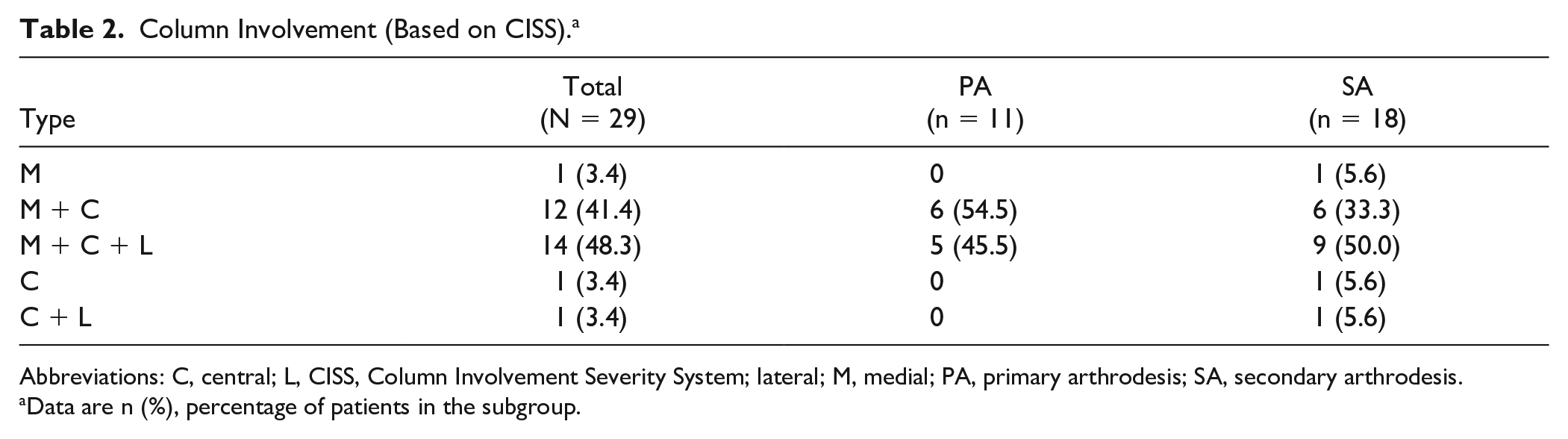
Abbreviations: C, central; L, CISS, Column Involvement Severity System; lateral; M, medial; PA, primary arthrodesis; SA, secondary arthrodesis.
Data are n (%), percentage of patients in the subgroup.
Management
In total, 11 patients (37.9%) were treated with PA and 18 patients (62.1%) with SA after failed primary treatment. Comparison of the surgical characteristics are shown in Table 3. Prior to PA, one patient was temporarily treated with percutaneous Kirschner wire fixation. Most patients had arthrodesis of the medial and central column (TMT 1-3, n = 8), and joints were fused using multiple plates and screws (n = 11). Primary treatment in patients with SA was ORIF (n = 6; bridge plating and/or transarticular screws [5], transarticular screws only [1]), nonoperative treatment (n = 5), or no treatment due to overlooked diagnosis (n = 7). During the study period, 8 (n = 6 included, n = 2 excluded from this study) of a total of 118 patients with Lisfranc injuries treated with ORIF eventually underwent SA (6.8% SA after ORIF). These numbers were not available for nonoperatively treated patients. The median time between primary treatment and SA was 13 (range, 2-34) months. In the SA group, most patients had arthrodesis of the medial and central column (n = 17), mostly using 1 plate and screws (n = 7), screws only (n = 8), or multiple plates and screws (n = 2). The time to fusion was significantly shorter in the screws-only subgroup (P = .04).
Comparison of Arthrodesis. a
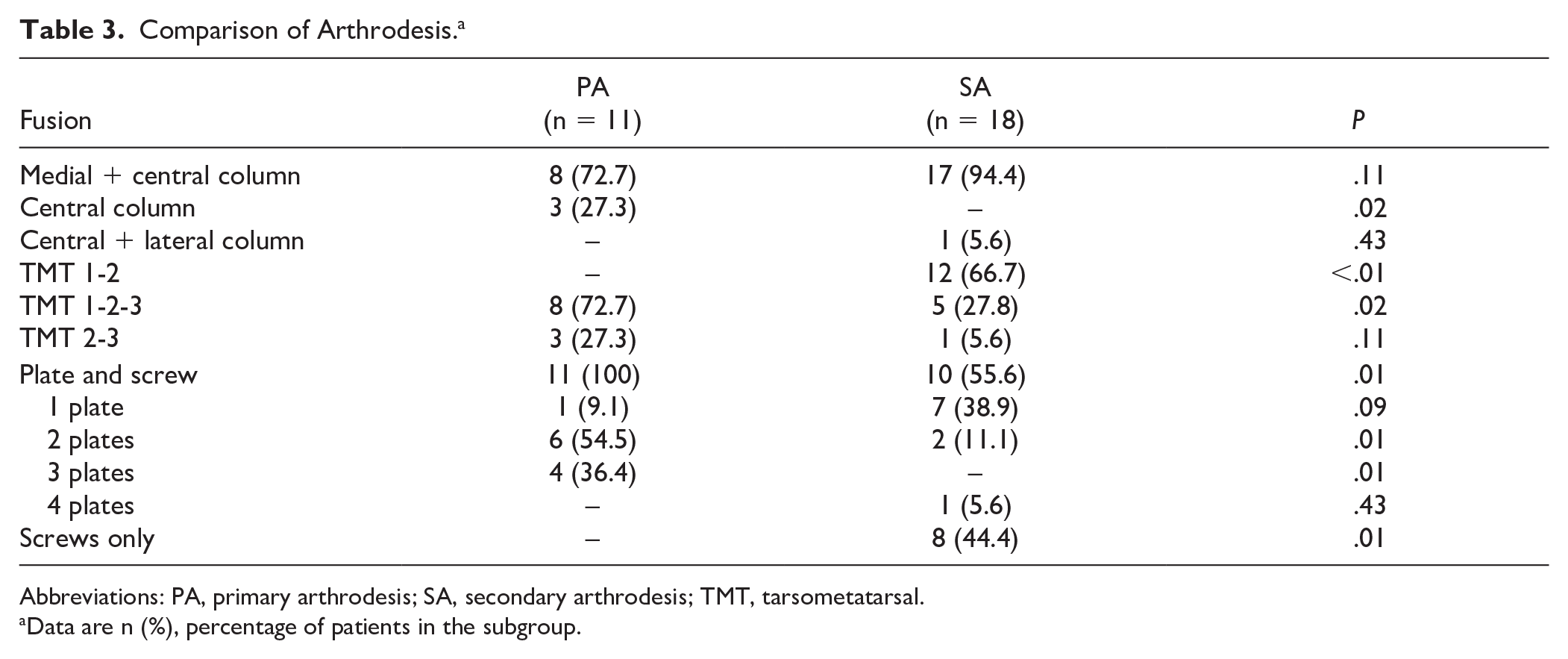
Abbreviations: PA, primary arthrodesis; SA, secondary arthrodesis; TMT, tarsometatarsal.
Data are n (%), percentage of patients in the subgroup.
Complications
Complication rates are shown in Table 4. Union rate was 100% in the PA group and 88.9% in the SA group (P = .26). In the SA group, 1 patient had infection after primary treatment (ORIF with bridge plating) and 1 patient had superficial fracture-related infection after SA. Both were successfully treated with oral antibiotics. After SA, 4 patients (22.2%) had revision surgery because of nonunion of TMT 3 after TMT 1-3 fusion (n = 1), painful osteoarthritis in TMT 1 that was not fused (n = 2, tertiary arthrodesis), or painful osteoarthritis in the calcaneocuboid joint and TMT 4-5 (n = 1, resection). In total, 45.5% of PA patients needed surgical intervention (removal of hardware) and 55.6% of SA patients (P = .6).
Complications. a
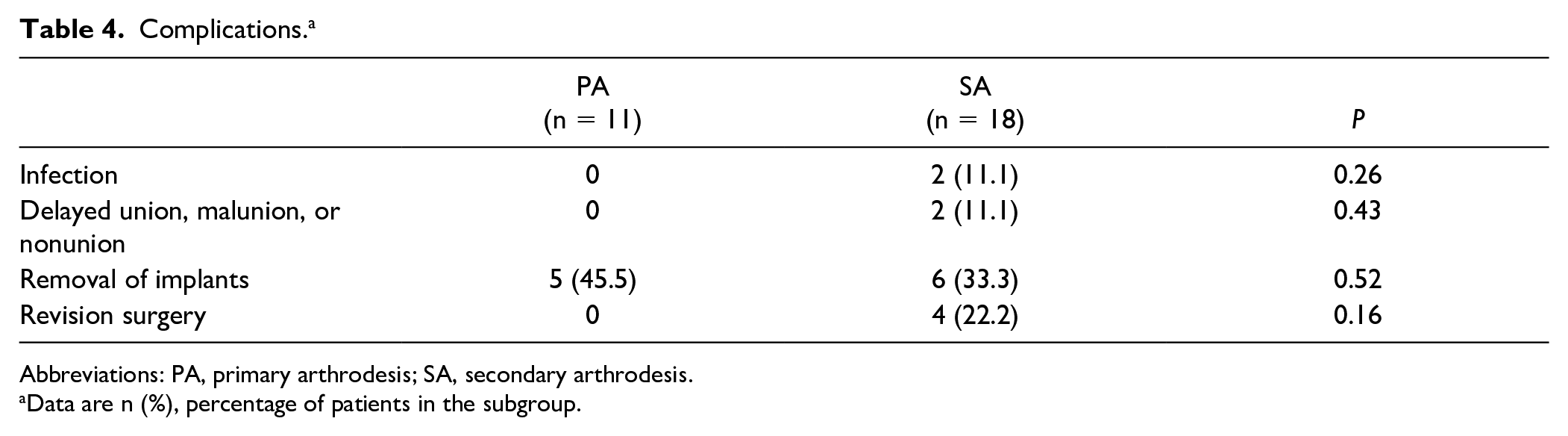
Abbreviations: PA, primary arthrodesis; SA, secondary arthrodesis.
Data are n (%), percentage of patients in the subgroup.
Functional Outcome and Other Patient-Reported Outcomes
Median follow-up time from the day of trauma was 8.5 (range, 3.5-12.3) years. Functional outcome and patient-reported outcome measures per group are demonstrated in Tables 5 and 6. Overall AOFAS was good in PA compared to fair in SA. The post hoc calculation indicated 31% power to detect outcome differences. Patients with pure ligamentous injuries had a mean AOFAS score of 70.2 (fair, SD 19.8), FFI 32.7 (SD 28.3), perceived health 7.2 (SD 1.5), and treatment satisfaction 7.2 (SD 1.8). Table 6 shows AOFAS scores per SA subgroup. With the numbers available, no significant differences were detected in functional outcome, treatment satisfaction, and perceived health between PA and SA or between SA subgroups. Multivariate linear regression indicated that none of the confounding factors (age, tobacco use, ISS, column involvement, early or late diagnosis) had a significant impact on AOFAS or FFI (R2 0.286).
Functional Outcome and Patient-Reported Outcome Measures. a
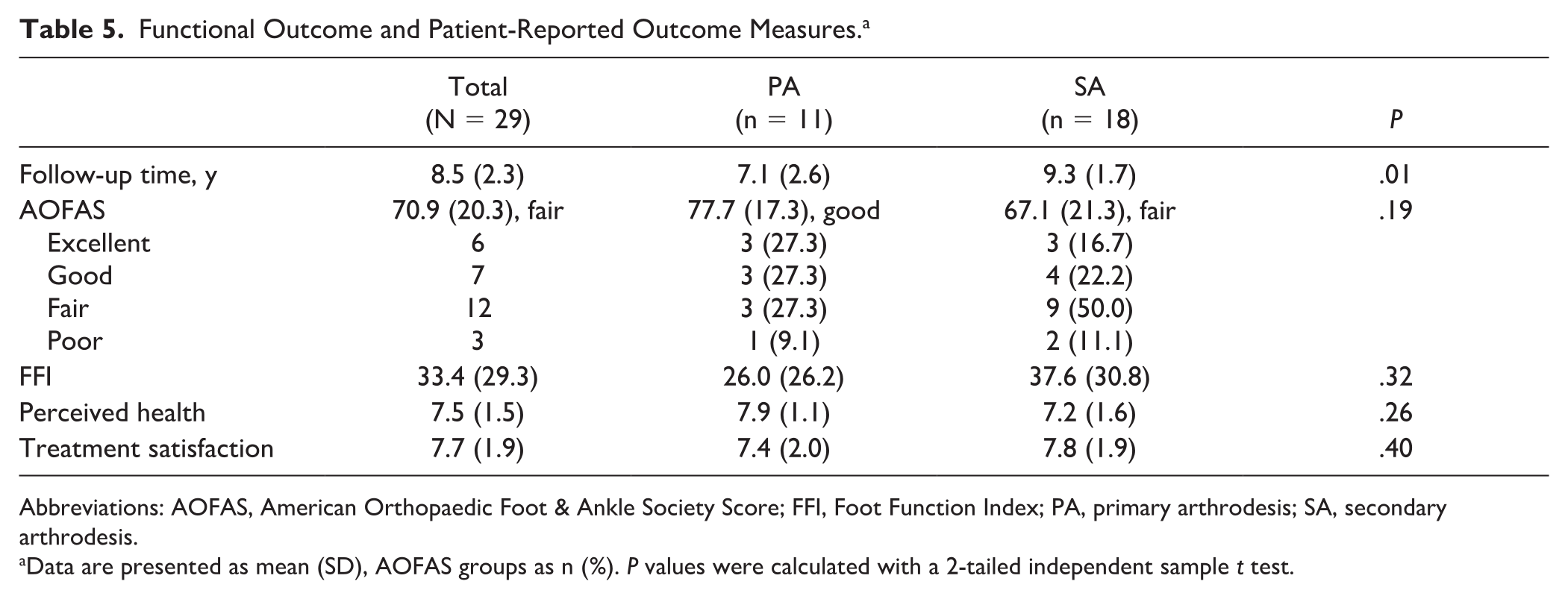
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society Score; FFI, Foot Function Index; PA, primary arthrodesis; SA, secondary arthrodesis.
Data are presented as mean (SD), AOFAS groups as n (%). P values were calculated with a 2-tailed independent sample t test.
Functional Outcome and Other Patient-Reported Outcomes per SA Subgroup. a
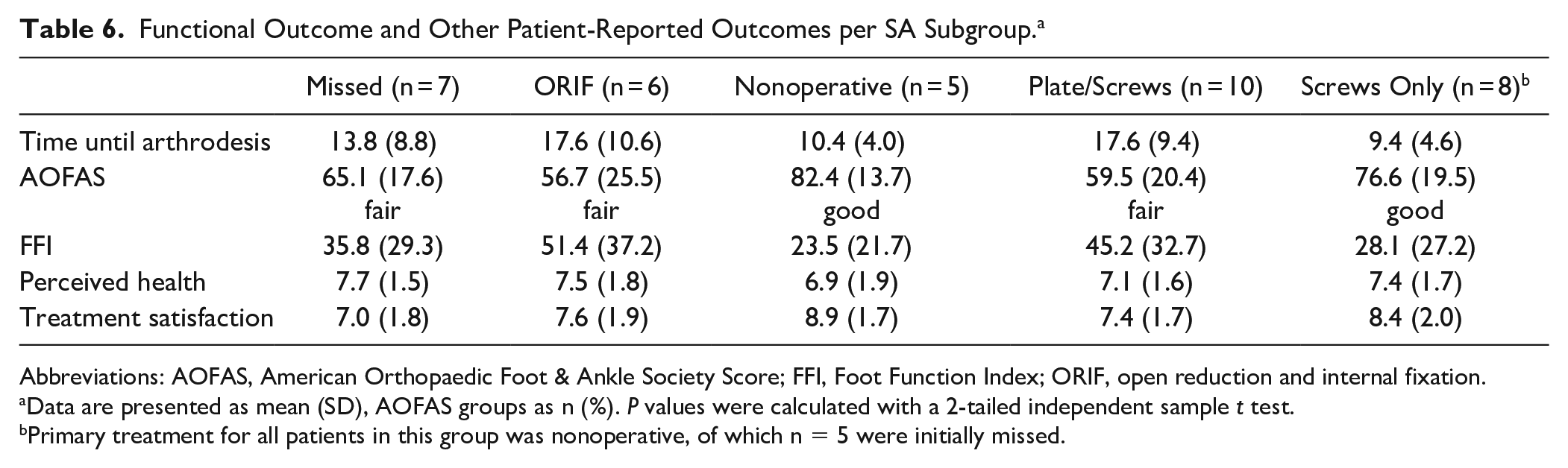
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society Score; FFI, Foot Function Index; ORIF, open reduction and internal fixation.
Data are presented as mean (SD), AOFAS groups as n (%). P values were calculated with a 2-tailed independent sample t test.
Primary treatment for all patients in this group was nonoperative, of which n = 5 were initially missed.
Overall, 87.0% returned to work (n = 20 of 23 patients who worked prior to trauma). In comparison, 83.3% of PA patients returned to work (n = 5 of 6, of whom 1 changed job) vs 88.2% of SA patients (n = 15 of 17, of whom 3 changed jobs, P = .7). In total, 58.3% were able to return to sports (n = 14 of 24 who performed sports prior to trauma). More PA (71.4%, n = 5 of 7) than SA (52.9%, n = 9 of 17) patients performed sports after their Lisfranc injury (P = .33).
Discussion
Although sample size was small and results were not statistically significant, there was an important clinical difference in AOFAS interpretation (PA good vs SA fair) and FFI. Based on the minimal important difference for total FFI of 7, a mean difference of 11.6 reflects a clinically significant difference. 13
Injury Pattern
Mechanisms of injury and injury patterns were found to correspond to those reported in the literature.12,26 The rate of concomitant midtarsal injuries was similar to that in previous outcome studies.22,25 Medial and central column involvement was evenly spread between the PA and SA groups. Because of missed diagnosis, all patients (n = 5) with pure ligamentous injuries in this cohort were treated with SA. It was reported that 20% of subtle ligamentous injuries were inappropriately managed, either because they were missed or because severity was underestimated.27,30 As found in a systematic review and meta-analysis by van den Boom et al and in this cohort, outcome of patients with pure ligamentous injuries was similar to those of patients with bone involvement. 31 After SA, there was no difference in functional outcome between early and missed diagnosis. Nevertheless, caution is warranted even for subtle nondisplaced injuries as potentially problematic Lisfranc injuries.
Management and Outcome
The rate of tarsometatarsal joint (TMTJ) fusion (96.6%) was higher than most previous studies (81.4%-97.8%).14,25 PA was done using multiple plates, based on the fractures to the metatarsal bases and cuneiform bones. Because such fractures had mostly healed already in the SA group, a substantial part of joint fusion was done by using screws only. Based on patients’ requests and/or complaints, implants were removed in 45.5% of PA and 33.3% of SA patients. No studies directly comparing routine implant removal vs retention after Lisfranc fracture fixation were found in literature. In a recent systematic review, Rhodes et al 23 reported that implants were removed in 198 of 317 patients in the retention group, yielding a 62.5% unplanned removal rate. They found a minor difference in AOFAS score of 3.38 (P = .02) between removal and retention groups in favor of removal. 23 As also argued by Ponkilainen et al, 18 the rate of secondary operations (other than implant removal) was higher in the SA group (22.2%) compared to PA (0). With respect to iatrogenic nerve injury, future evaluation of sensory loss, especially after secondary surgery (removal of hardware or SA), may provide further arguments for PA; however, currently insufficient evidence is available.
Only few studies reporting functional outcome after PA or SA, using validated outcome instruments, were found in literature. Campbell et al. conducted a study similar to ours, using Patient-Reported Outcomes Measurement Information System (PROMIS), and reported a similar non-significant trend towards better function and less pain in patients with index PA vs primary ORIF followed by SA. 3 Moreover, their post hoc power analysis indicated the same power as our study (32%). 3 In studies comparing ORIF vs PA, Ly and Coetzee 15 reported a mean AOFAS of 86.9 after PA (good, SD 9.25), Dubois-Ferrière et al 6 reported a mean AOFAS of 77.8 after PA (good, SD 7.5), Wang et al 32 reported a mean AOFAS of 85.1 after PA (good, SD 8.15), Fan et al 8 reported a mean AOFAS of 82.8 (good, SD 7.5) and Stodle et al 28 reported a mean AOFAS at 2 years after PA of 89 (good, SD 9). These scores are all interpreted as good, similar to our PA group (77.7, SD 17.3). With regard to SA, various small and old prospective studies demonstrated that corrective arthrodesis of the TMTJ results in improvement of foot function and reduction of pain after overlooked or inadequately treated Lisfranc injuries.12,23,24 Rammelt et al 22 reported a significant difference (P = .03) in functional outcome in favor of PA patients (n = 20, median AOFAS 81.4, good) compared with SA patients (n=20, who presented with painful malunion at a mean of 22 months after injury, median AOFAS 71.8, fair). Our findings in PA and SA patients are consistent with these results.
The development of chronic pain and midfoot arthritis in (failed) ORIF patients is based on the concept that although osseous reduction is possible, ligamentous injury to the TMTJ may never fully recover.9,22 This allows continuous motion at the TMTJ leading to joint degeneration and development of chronic posttraumatic arthritis and pain, even after corrective SA. In the comparison of SA subgroups, it was also observed that patients who were treated with ORIF prior to SA had worse functional outcome than patients after nonoperative or no primary treatment (Table 6). This could imply that patients in the ORIF group sustained worse injuries than (missed) nonoperative patients. While these findings must be interpreted with caution due to the small sample size, the mean difference in FFI of 27.9 was far above the minimal important difference. PA may offer a more functional recovery with less pain, without going through a phase of failed ORIF with painful secondary osteoarthritis.4,17,20 In the context of daily activities, this study showed that patients who were treated with PA or SA could typically return to work and (in a lower degree) to sports. There were no significant differences between PA and SA; however, these results should be considered in the context of a relatively low number of patients in the PA group who worked or performed sports prior to injury. In a cohort of 171 low-energy TMT fracture-dislocations in an active-duty military population, Hawkins et al 10 demonstrated that patients who underwent salvage arthrodesis (interpreted as SA) had a significantly lower return to duty rate (29%) than PA (80%) and ORIF (65%) patients.
Given the subtle yet not statistically significant trend toward better outcome in PA compared to SA, and other recent studies indicating superior outcome for PA over ORIF, this study may add evidence to the discussion on whether primary fusion should be considered for all Lisfranc injuries.3,9,10,12,14,18,25,26,31 In literature, the rate of SA after ORIF varied from 4.2% to 12% and was reported as high as 54% in nonoperatively treated patients.5,11,16,18,19 The next step is to find a way to predict who might be at risk to require SA, so to consider for PA as their index surgery. Ideally, this process would eventually lead to a single-surgery approach for all Lisfranc patients.
Limitations
Because of the very low incidence of this injury, sample size was small. Patients in the PA group were significantly older (mean difference 11.7 years), which may reflect selection bias. Results may have been skewed by a selection bias of patients with the worst injuries in the PA group, which may affect functional outcome and perceived health. However, patients with open fractures and severe soft tissue damage due to compartment syndrome were excluded. Interestingly, overall functional outcome in the PA group was good. Less severe injuries were probably treated successfully by ORIF with bridge plating and thus not included in this study. Overlooked injuries tend to have poorer outcome, and those were mainly found in the SA group. 2
Conclusion
Although sample size was small and results were not statistically significant, there was an important clinical difference in AOFAS interpretation (PA good vs SA fair) and FFI in favor of PA. Because of the low incidence, high complexity, and potentially poor outcome, early referral of patients with unstable Lisfranc injuries to dedicated foot surgeons and centralization of complex foot surgery is recommended. The question of how to predict which patients are at risk for failed primary treatment and consequent SA remains. The choice and accuracy of the initial surgery may be pivotal for a successful outcome.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007241288853 – Supplemental material for Functional Outcome and Patient Satisfaction After Primary vs Secondary Arthrodesis for Lisfranc Injuries: Toward a Single-Surgery Approach
Supplemental material, sj-pdf-1-fai-10.1177_10711007241288853 for Functional Outcome and Patient Satisfaction After Primary vs Secondary Arthrodesis for Lisfranc Injuries: Toward a Single-Surgery Approach by Esmee Wilhelmina Maria Engelmann, Jens Anthony Halm and Tim Schepers in Foot & Ankle International
Footnotes
Ethical Approval
This study was submitted to the institutional review board. Ethical approval for this study was waived by METC Amsterdam UMC (W19_247) because this is an anonymized retrospective study in which patients gave consent by completing the questionnaire and were provided with the opportunity to reject participation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.