
Abstract
Background:
Sesamoid pathology can lead to significant pain and disability both with activities of daily living and high-impact athletic movements. Sesamoidectomy is a widely used procedure for patients who fail conservative treatment measures. Traditional dorsal or plantar approaches for sesamoidectomy have shown to successfully alleviate pain, but complications were reported. A proposed alternative medial approach using a burr may provide many advantages compared with traditional approaches. This study presents patient outcomes and complications for this technique.
Methods:
This was a retrospective chart review of patients undergoing sesamoidectomy (tibial, peroneal, or both) using a burr through a medial approach to the sesamoid metatarsal articulation. Data collected included patient demographics, radiographic analysis, and outcomes: Veterans Rand 12 Item Health Survey (VR-12), Foot and Ankle Ability Measure (FAAM), visual analog scale (VAS), patient satisfaction, and complications.
Results:
Twenty-seven patients (29 feet) were included. The mean age was 38.4 years followed up for a mean of 30.9 months. VR-12 physical component improved from 35.98 ± 7.86 to 51.34 ± 8.01 (P < .001), FAAM ADL and sport improved from 58.33 ± 16.61 to 83.27 ± 18.28 (P < .001) and 26.37 ± 20.31 to 63.75 ± 29.74 (P < .001), respectively. Patient satisfaction with the treatment was 80.59% ± 27.06%. The overall complication rate was 11 (37.9%) whereas the overall reoperation rate was 4 (13.7%) of 29 feet. Complications included 1 arthrofibrosis, 1 flexor hallucis longus subacute rupture, and 1 asymptomatic hallux valgus. There were no sesamoid excision revisions.
Conclusion:
Sesamoidectomy using a medial approach with a burr provided significantly improved short-term functional outcomes, 80% patient satisfaction rate, with a relatively acceptable complications rate including 20% persistent pain. The medial approach is familiar to orthopaedic foot and ankle surgeons, provides adequate exposure, and eliminates the possibility of a painful plantar scar while avoiding disruption of the plantar plate, flexor hallucis brevis tendon, and ligamentous structures attached to the sesamoids. Larger studies with long-term follow-up from other centers are needed.
This is a visual representation of the abstract.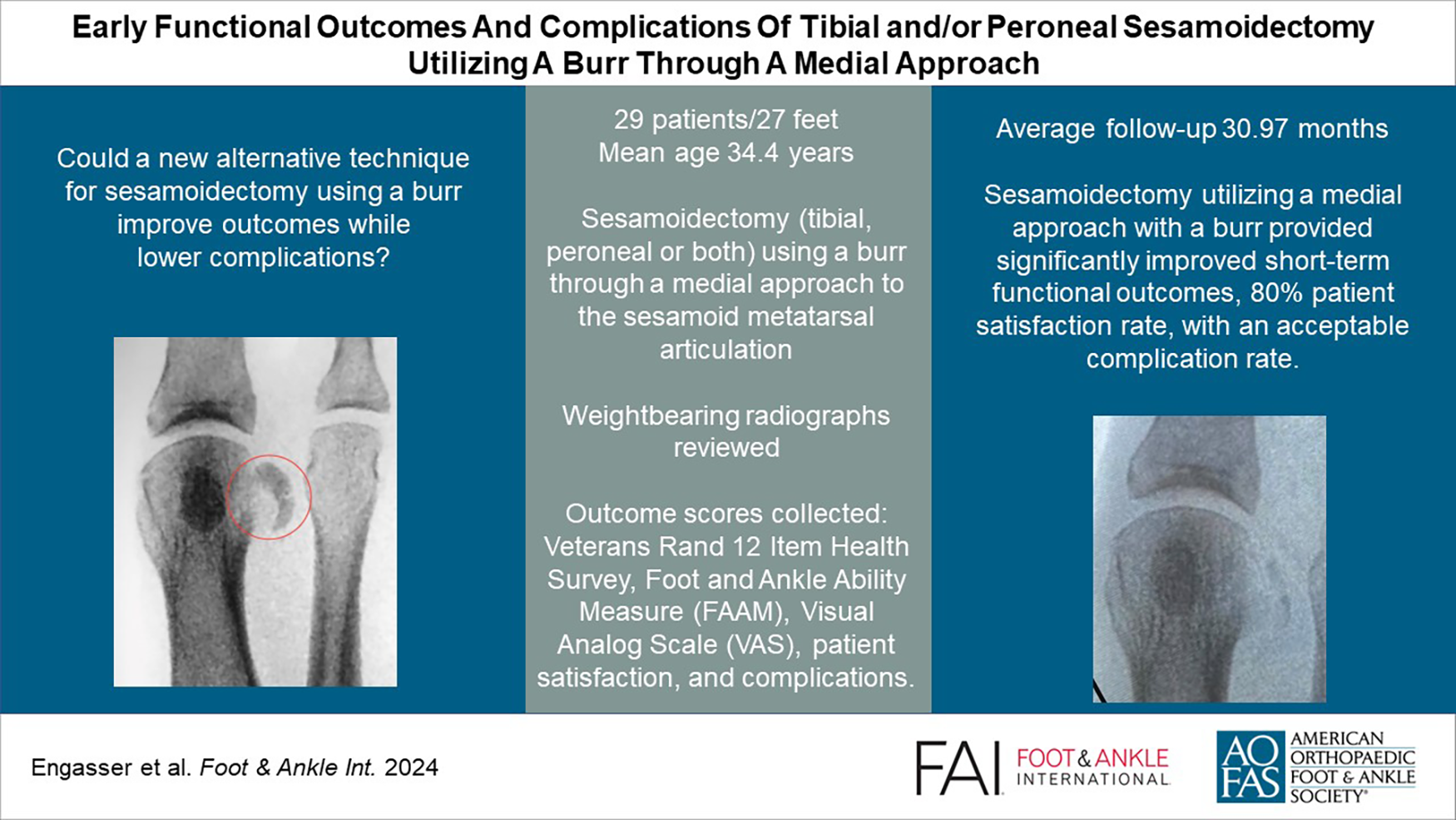
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.