
Abstract
Background:
Posttraumatic osteonecrosis (ON) of the lateral distal tibia is a rare but severe complication of malleolar fractures. Treatment options include ankle fusion, arthroplasty, osteotomy, and drilling but clinical data on outcomes are limited to single case reports. The aim of this study was to prospectively evaluate the outcome following joint-preserving reconstruction.
Methods:
Over a 10-year period, 10 patients (8 females and 2 males, average age 36 years; range, 27-68 years) with posttraumatic ON were treated with intra-articular osteotomy of the distal tibia and bone grafting. All patients initially sustained a closed pronation injury, 7 with initial tibiotalar subluxation. Chronic syndesmotic instability following initial treatment was present in 4 patients and 5 were smokers. All patients were followed for a median of 68 (range, 12-103) months, 7 returned in person for clinical and radiographic follow-up.
Results:
No immediate postoperative complications were seen. Secondary ankle fusion was necessary in 1 case (10%) because of progressive osteoarthritis. At the time of follow-up, anterior ankle arthritis leading to impingement and requiring cheilectomy was noted in 4 cases, partial graft necrosis, and secondary syndesmotic instability requiring revision surgery was seen in 1 case each. Compared with the preoperative values, significant improvement in the Olerud-Molander Ankle Score (P = .012), EuroQuol-5 Score (P = .008), and Foot Function Index (FFI-D pain, P = .028; FFI-D restriction, P = .038) was seen. Average range of motion at the ankle was 45 degrees.
Conclusion:
In our limited series of patients with posttraumatic ON of the lateral distal tibia, we found that joint-preserving reconstruction using an intra-articular distal tibial osteotomy with autologous bone grafting usually provided significant functional improvement and pain relief. In our cohort secondary fusions by a median 5.5-year follow-up were rare, but secondary, joint-sparing surgeries were common.
Level of Evidence:
Level III, prospective study.
Keywords
Introduction
Ankle fractures are one of the most common injuries with a rate of 4.22/10 000 in the United States. 43 A rare but serious complication is osteonecrosis (ON) of the lateral tibial plafond. The incidence is roughly estimated at approximately 1000 cases per year in the United States. 31
Several potential mechanisms for the development of posttraumatic ON or avascular necrosis (AVN) at the lateral distal tibia following malleolar fractures have been proposed. These include poor vascular supply to the anterolateral distal tibia, 30 iatrogenic injury to the perforating branch of the peroneal artery, 36 excessive periosteal stripping, 2 impaction of the lateral tibial plafond, 41 and reduced perfusion of the soft tissues and skin from open injuries and fracture-dislocations.5,31 Drug-induced or idiopathic AVN as well as AVN of the lateral tibial plafond following pilon fractures are beyond the scope of this study.
Posttraumatic AVN of the distal tibia was probably first reported by Siffert and Arkin in 1950 following nonoperative treatment of a closed bimalleolar Salter-Harris type II fracture in a skeletally immature patient. 44 The first case report of an adult with AVN of the lateral distal tibia following open reduction and internal fixation (ORIF) of a Maisonneuve injury was provided by Lagier 26 and a first retrospective series of 9 adult patients by Assal et al. 1 Since then, only 1 retrospective case series 7 and 2 case reports have been published.21,39 With the exception of 2 single cases followed for 9-12 months,21,39 no treatment results for distal tibial ON/AVN have been provided.
Despite the low overall number of reported cases with this specific entity, a multitude of techniques has been proposed including bone grafting followed by arthrodesis or arthroplasty, 1 reconstruction with unipolar autograft, 21 percutaneous drilling, 39 and nonoperative treatment using prolonged offloading. 7 All studies concluded that further investigations are necessary to determine an optimal treatment strategy.
The aim of the present prospective study was to determine the medium-term clinical and radiographic outcomes of joint-preserving reconstruction of the lateral tibial plafond for posttraumatic ON following malleolar fractures and to analyze potential risk factors for its occurrence.
Materials and Methods
Study Design
Over a study period of 10 years, 15 patients with posttraumatic osteonecrosis (ON) of the lateral tibial plafond following malleolar fractures were treated at our institution with preservation of the ankle joint. One patient opted for nonoperative treatment and 3 patients declined to be involved in a prospective clinical study for personal reasons. One patient was treated with percutaneous drilling of the lateral distal tibia. Patients who sustained a lateral tibial ON due to a pilon fracture, infection, or diabetic neuropathy and patients who underwent ankle fusion as a salvage procedure for Kellgren and Lawrence third to fourth degree ankle arthritis 23 were not included in this study. Other exclusion criteria were patient age <18 years, rheumatoid arthritis, manifest osteoporosis, gout, and AVN beyond the lateral tibial plafond, limiting the study population to 10 patients (Table 1).
Patient Characteristics.
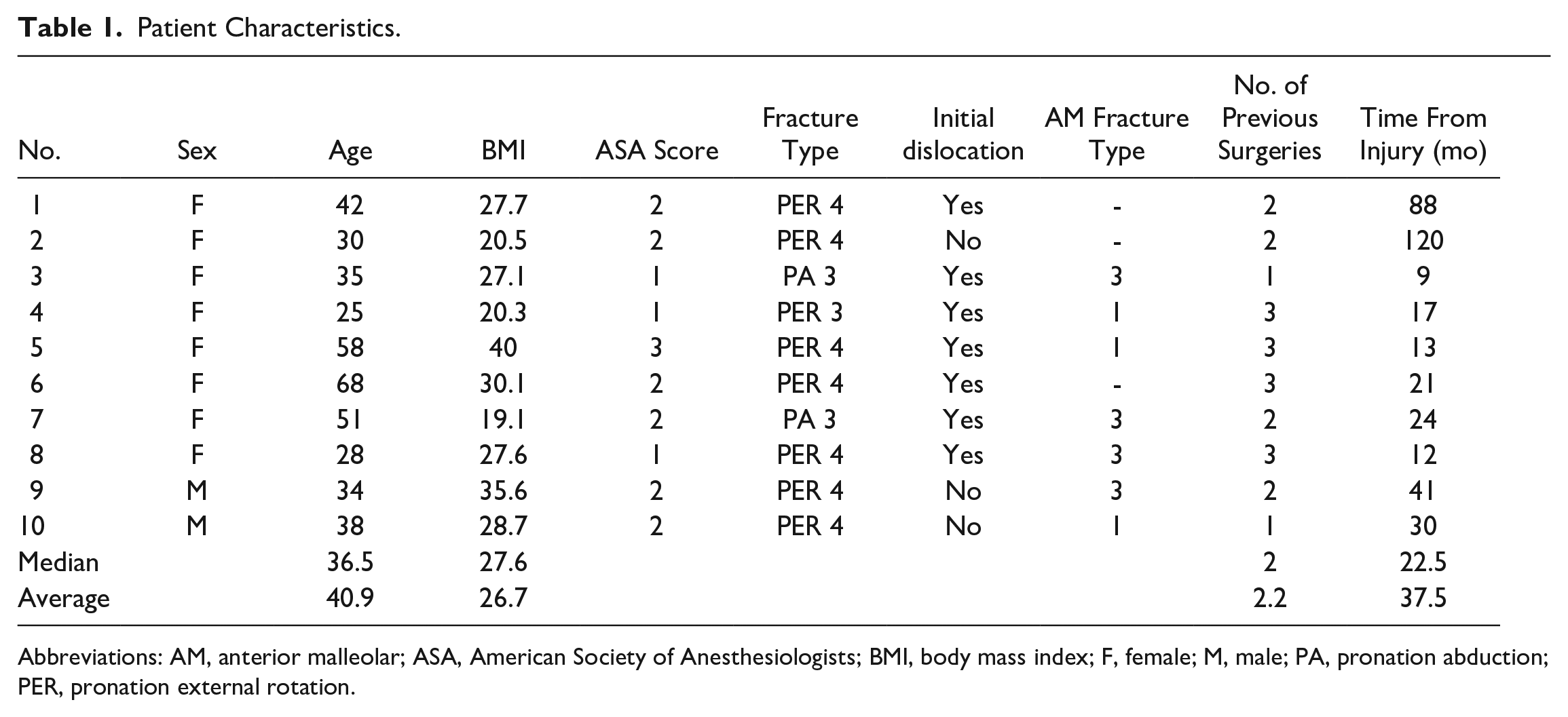
Abbreviations: AM, anterior malleolar; ASA, American Society of Anesthesiologists; BMI, body mass index; F, female; M, male; PA, pronation abduction; PER, pronation external rotation.
Of these 10 patients, 2 were initially treated with an ankle fracture at our center. During the same period, 1900 ankle fractures were treated at the same institution. The remaining 8 patients were referrals. The median interval between the initial trauma and diagnosis of ON was 22 months (range, 9-120 months).
All patients were assessed prospectively with physical examination and imaging. The latter included bilateral standing lateral and anterior-posterior (AP) radiographs of the ankles (Figure 1), computed tomography (CT) scanning (Figure 2), and magnetic resonance imaging (MRI). Preoperative status and functional outcomes at follow-up were assessed using the Olerud-Molander Ankle Score (OMAS), 35 EuroQuol-5 score (EQ-5D), 38 Foot Function Index (FFI-D), 6 and the American Orthopaedic Foot & Ankle Society (AOFAS) ankle/hindfoot score. 24 The degree of arthrosis was graded according to Kellgren and Lawrence. 23 Ankle and hindfoot alignment was determined by anterior-posterior standing radiographs. Comorbidities are listed in Table 2.
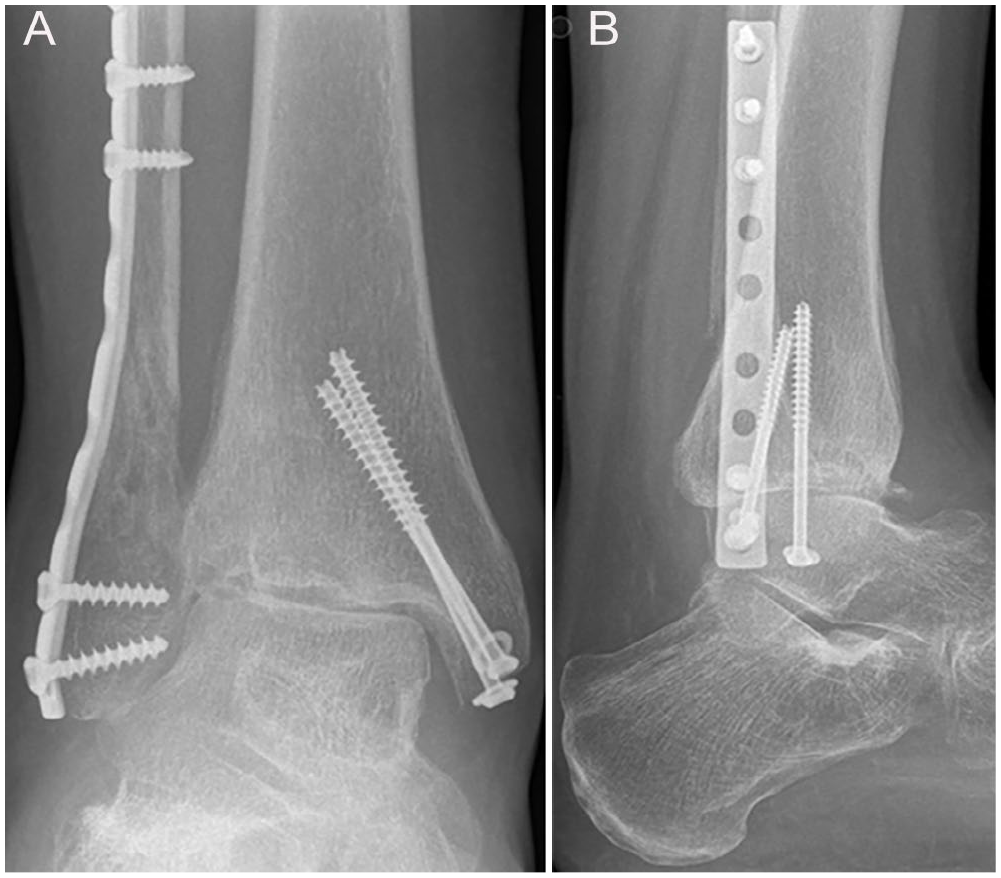
(A) Anteroposterior and (B) lateral radiographs of a 35-year-old female patient presenting 9 months after a pronation-abduction stage 3 ankle fracture-dislocation with increasing pain and limited ankle motion. The anteroposterior view shows valgus malalignment possibly following impaction at the lateral distal tibia (type 3 anterior malleolar fracture 41 ) with osteonecrosis of the lateral tibial plafond and subsidence of the talus.
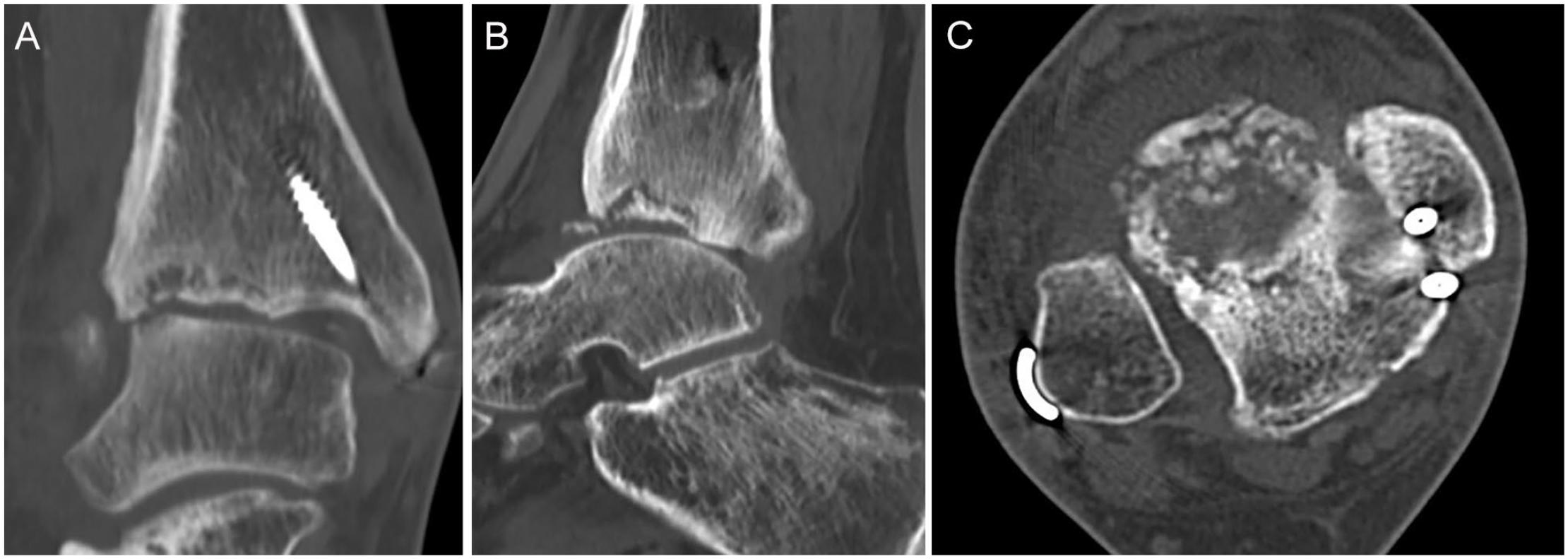
(A-C) Computed tomographic scans showing the extent of anterolateral distal tibial avascular necrosis of about one-third of the tibial plafond (same patient as in Figure 1).
Comorbidities.
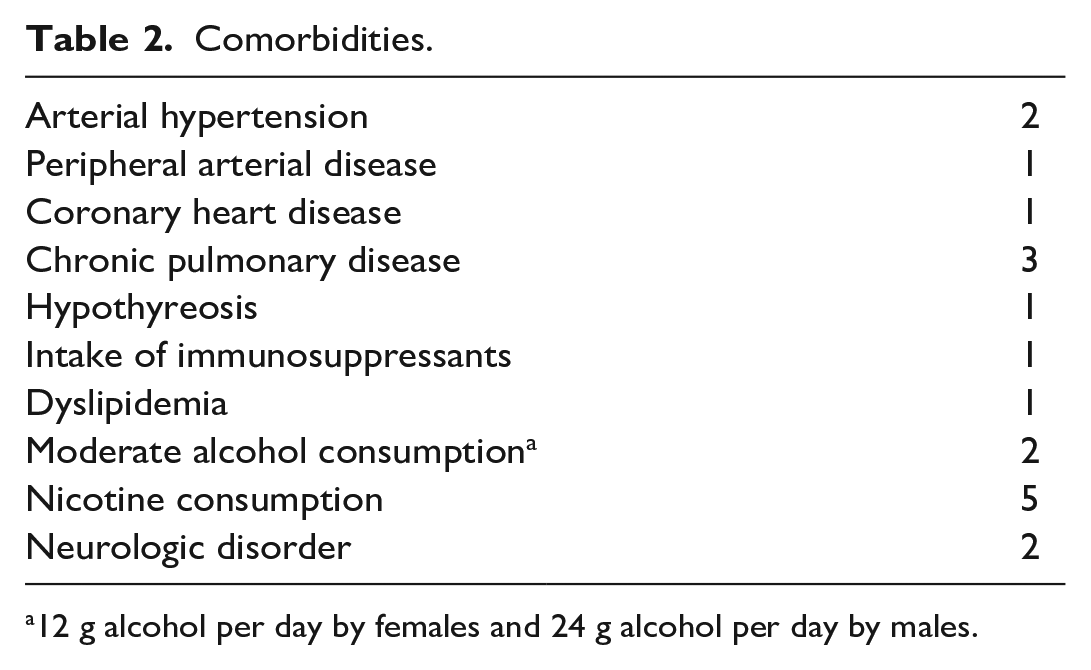
12 g alcohol per day by females and 24 g alcohol per day by males.
The same parameters were obtained at follow-up. Patients were asked to rate their satisfaction using a school grade system (1 being very satisfied, 5 equaling completely unsatisfied).
The study protocol was approved by the local institutional review board.
Surgical Technique
Patients were placed in the supine position with a tourniquet applied to the thigh and a support wedge under the ipsilateral hip to bring the foot into a neutral position. All procedures were performed by 3 senior surgeons.
The surgical approach was chosen depending on the individual pathology, preexisting scars, and implants. A preexisting anterolateral approach was extended distally in 5 cases. The superficial peroneal nerve was protected and gently displaced anteriorly within the subcutaneous tissue. In 4 cases, a preexisting lateral approach was extended anteriorly. In 2 cases of fibular shortening, a fibular lengthening osteotomy to correct the valgus deformity was performed. An anterior approach was used in 1 case.
The extensor retinaculum was dissected in a Z-shape. The cartilage at the tibia and talus was examined for viability and stability. If deemed intact, the osteotomy of the lateral tibial plafond was performed at a minimum of 1 cm above and parallel to the articular surface at the full extent of the articular impaction. The bone block was lowered carefully with a chisel. All necrotic bone was resected. Unstable chondral and osteochondal fragments with intact cartilage were fixed to the bone with resorbable pins and fibrin glue. In addition, the tibial metaphysis was drilled to stimulate the bone marrow. The metaphyseal defect at the osteotomy site was filled with a corticocancellous autograft from the iliac crest (n = 6), or fibula (n = 2). Local osteophytes from the talus or tibia were used in 1 case each. The correct joint alignment was confirmed with intraoperative fluoroscopy. The osteotomy was fixed with a locking plate in 6 cases and screws in 4 cases. In 1 case, a combination of both was used. In 1 case, a fibular osteotomy was added because of an additional fibular malunion (shortening). In 2 cases, a fibular osteotomy was added to shift the load medially in the ankle joint. The fibula was fixed with a locking plate (Figure 3). The anterior syndesmosis was readapted. Following osseous correction and fixation, syndesmotic stability was reassessed clinically and with external rotation under fluoroscopy. In 5 cases, residual instability was treated with open fibular reduction and insertion of a syndesmotic screw.
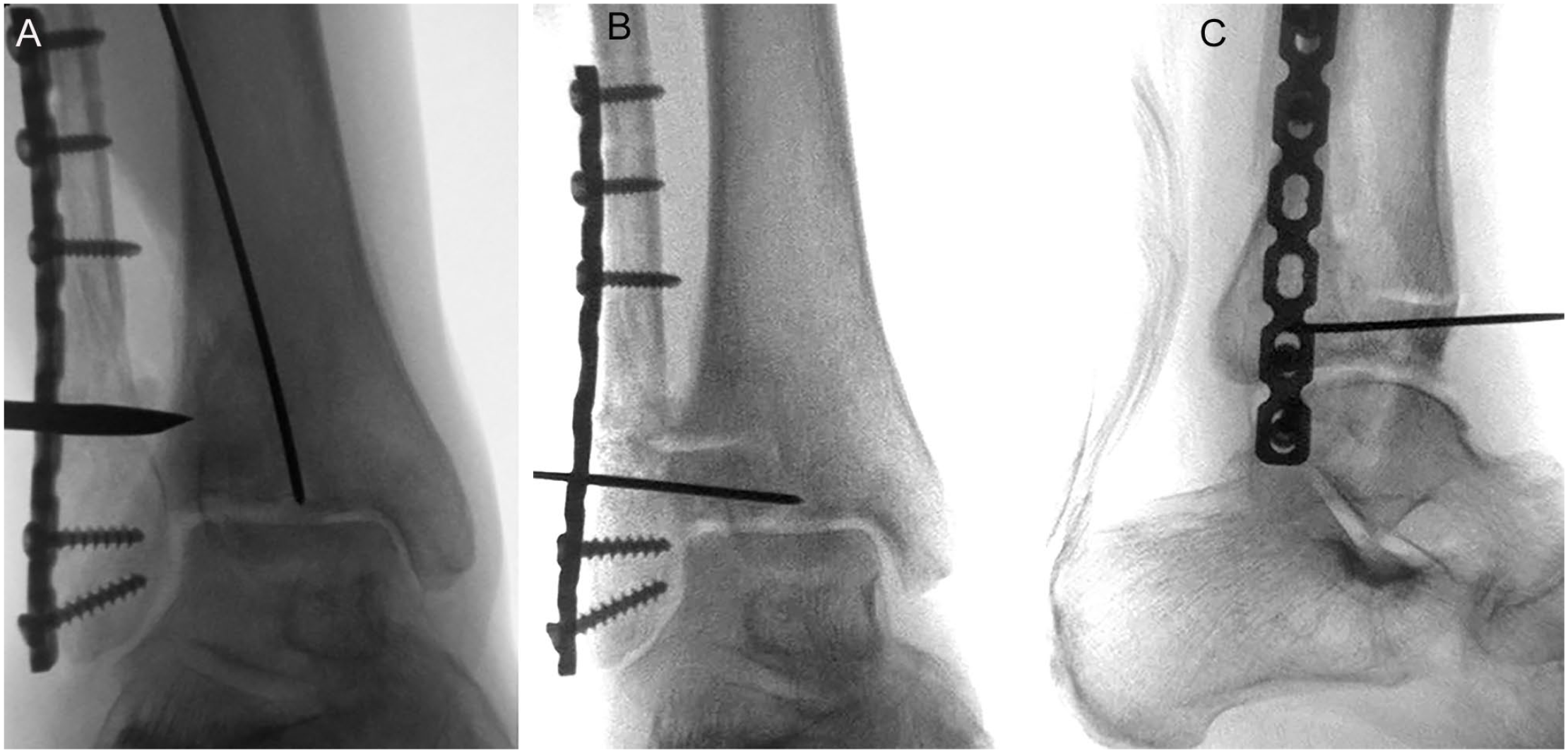
(A-C) Technique of intraarticular corrective osteotomy of the anterolateral distal tibia and lengthening fibular osteotomy for offloading of the lateral ankle joint with implantation of corticocancellous grafts from the iliac crest placed into the distal tibia and fibula followed by plate fixation of the distal fibula and tibia and drilling of the lateral talar dome and tibial plafond (same patient as in Figures 1 and 2).
Postoperative Management
The leg was immobilized in a splint that was removed temporarily for ankle range-of-motion exercises beginning at the second postoperative day. Patients were instructed to put their leg to the ground with its own weight, which translates to partial weightbearing of about 20 kg for 10-12 weeks postoperatively in a special boot on 2 crutches. If a syndesmotic screw had been used, it was removed in the operating room under local anesthesia prior to full weightbearing. After bony union was confirmed with radiographs, a gradual increase in weightbearing over 2 weeks was allowed.
Statistical Analysis
Statistical analysis was performed using SPSS (version 27; IBM, Armonk, NY). The Shapiro-Wilk test was used to check for normal distribution. For non-normally distributed data, results were presented as median with interquartile range (±IQR). Comparison between pre- and postoperative parameters was performed with the Wilcoxon test. Differences were considered statistically significant at P <.05.
Results
Complications
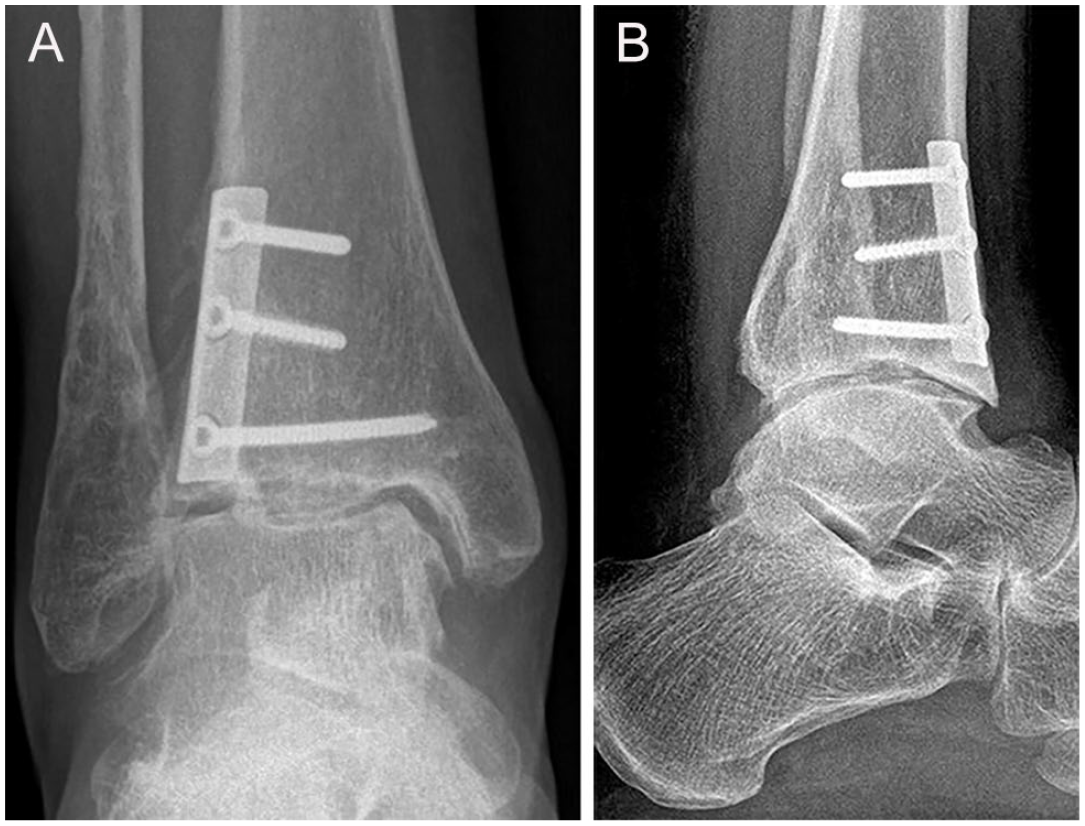
No early complications like hematoma, wound necrosis, or infection were seen. A late complication requiring surgical revision between 14 and 27 months postoperatively was noted in 6 patients (60% of cases). Four patients underwent complete implant removal, arthrolysis, and osteophyte resection for impingement resulting from anterior ankle arthritis (Figure 4). In a fifth case, a symptomatic fibular plate was removed.
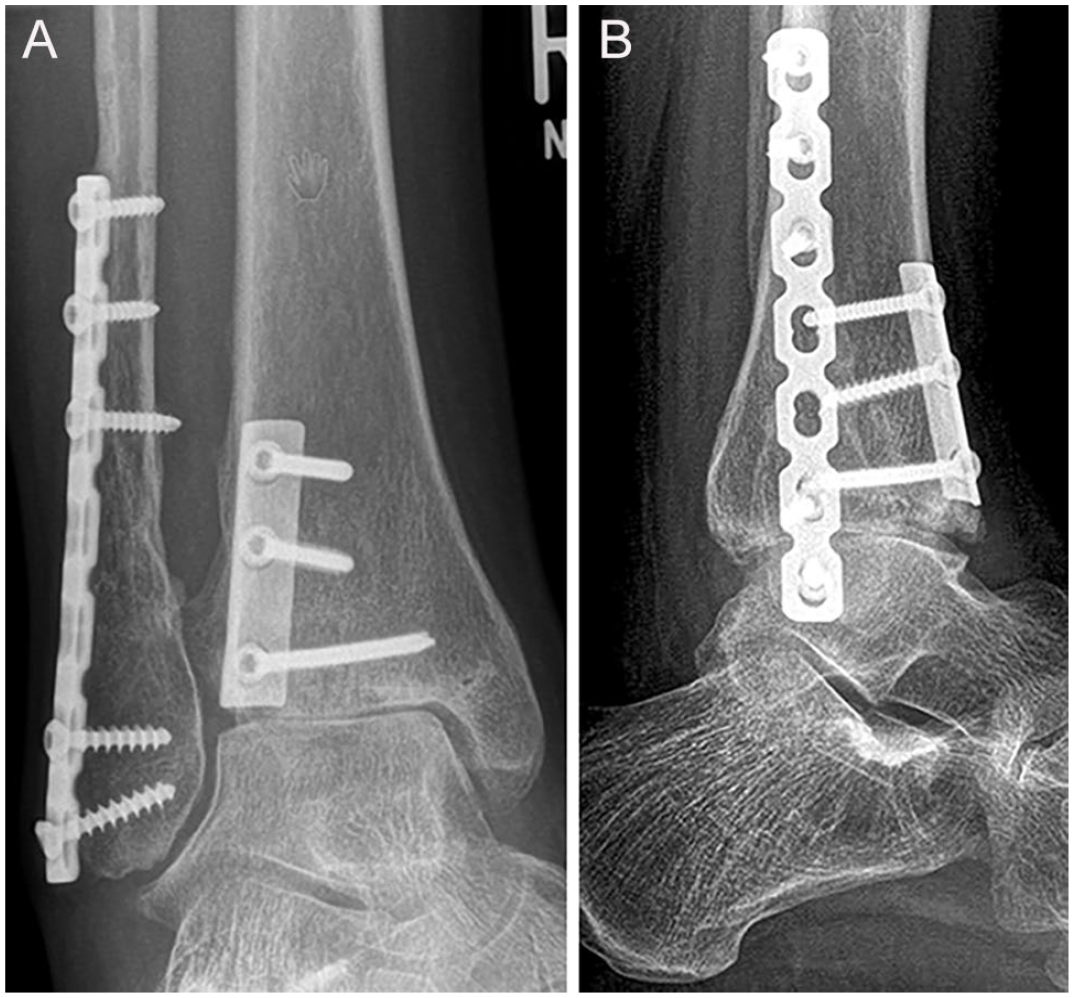
(A) Anteroposterior and (B) lateral weightbearing radiographs at 2-year follow-up showing physiological alignment of the ankle and full integration of the bone grafts. The patient was much improved but had symptoms of anterior ankle impingement. Therefore, removal of the fibular plate, anterior osteophyte resection (cheilectomy), and arthrolysis of the ankle joint was performed (same patient as in Figures 1–3).
Superficial peroneal nerve irritation and partial necrosis of the inserted bone graft were observed in 1 patient. Implant removal, arthrolysis, and osteophyte resection was accompanied by debridement, drilling, and neurolysis. At the time of follow-up, the patient still complained about persistent neuropathic pain at the dorsum of the foot whereas the discomfort in the ankle joint was relieved. A follow-up CT scan at 53 months showed no progression of necrosis.
Syndesmotic instability was observed on weightbearing radiographs in 1 patient, in addition to anterior ankle impingement. Following debridement at the syndesmosis and fibular reduction into the incisura, a flexible repair system (TightRope; Arthrex, Munich, Germany) was used for permanent syndesmosis stabilization. During the further course, the ankle mortise remained stable.
Rapid progression of osteoarthritis in the tibiotalar joint associated with pain was observed in 1 patient (10%). Ankle arthrodesis was performed 12 months after reconstruction.
Clinical and Radiographic Evaluation
Seven of 10 patients returned for a complete clinical and radiographic follow-up at a median of 68 months (range, 12-102 months) following reconstructive surgery (Figure 5). The remaining 3 patients were contacted by telephone and returned the questionnaires by mail.
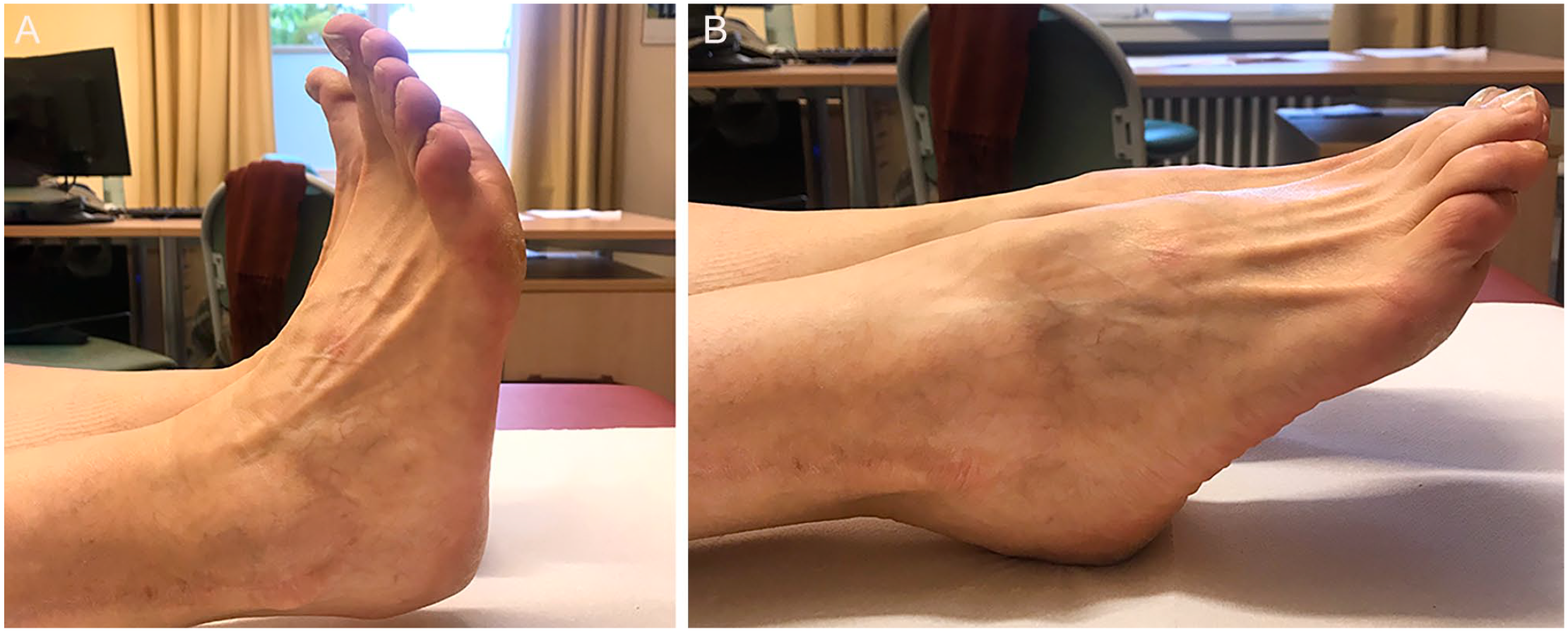
Subjectively, 4 patients were highly satisfied with the postoperative result, 4 were satisfied, and 2 were only partially satisfied. Of the latter, 1 patient had an additional longitudinal rupture of the of the peroneus brevis tendon with functional instability. The other patient reported dysesthesia below the scar. The pre- and postoperative functional scores are summarized in Table 3. All patient-reported outcome scores improved significantly when compared to the preoperative values. Ankle range of motion as measured by goniometer averaged 10.6 degrees of dorsiflexion and 31.3 degrees of plantarflexion (Figure 6). The overall three-dimensional eversion and inversion of the foot averaged 12.9 and 27.2 degrees, respectively.
Pre- and Postoperative Functional Outcome Scores. a
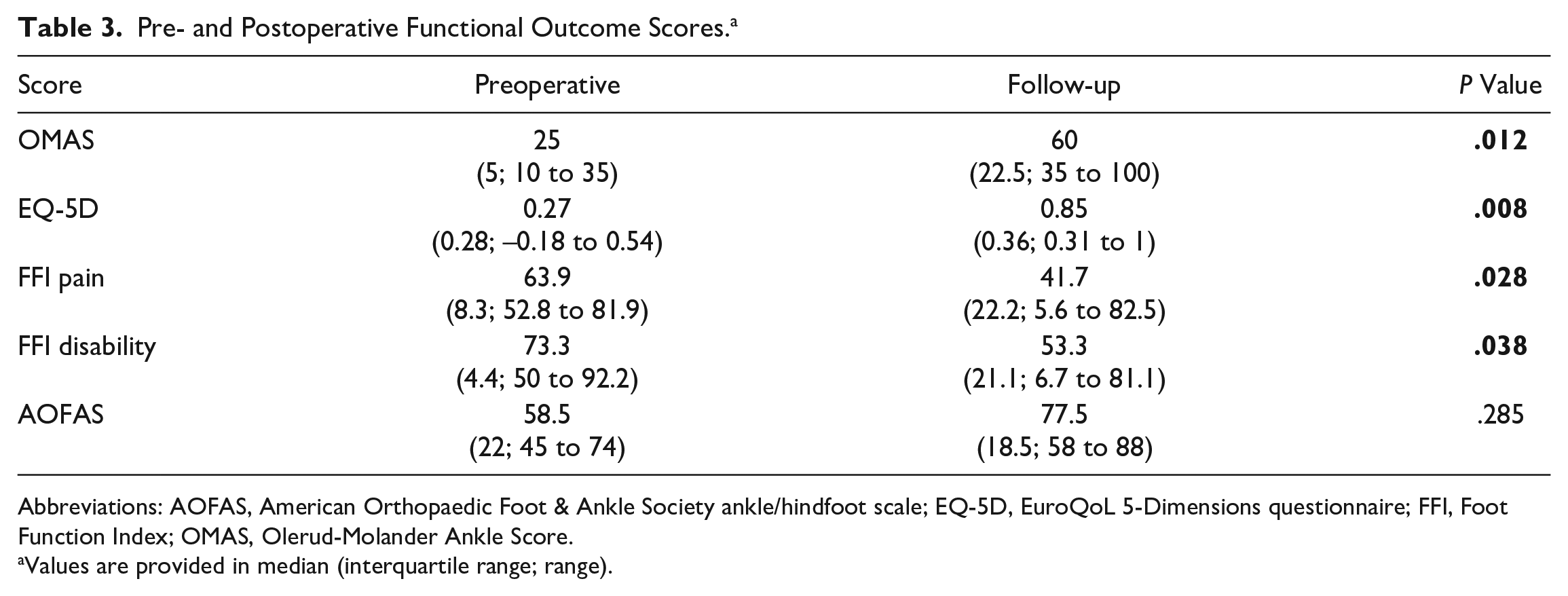
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society ankle/hindfoot scale; EQ-5D, EuroQoL 5-Dimensions questionnaire; FFI, Foot Function Index; OMAS, Olerud-Molander Ankle Score.
Values are provided in median (interquartile range; range).
(A) Anteroposterior and (B) lateral weightbearing radiographs at final follow-up, 7.5 years after correction, with some recurrent anterior osteophyte formation but without signs of progression of osteoarthritis compared with the initial standing radiographs (see Figure 1A and B). (Same patient as in Figures 1–5).
Preoperatively, radiographic evidence of ankle arthritis was present in 50%, and adjacent joint arthritis in at least 1 joint was detected in 100% of cases. At follow-up, a progression of the degenerative changes at the ankle joint by was detected in 2 of 7 cases (28.6%) with a complete set of radiographs. Progression of arthrosis of at least 1 adjacent joint was seen in 4 of 7 cases (57.1%), all by 1 degree (Table 4).
Radiographic Parameters Compared to Preoperative Values. a
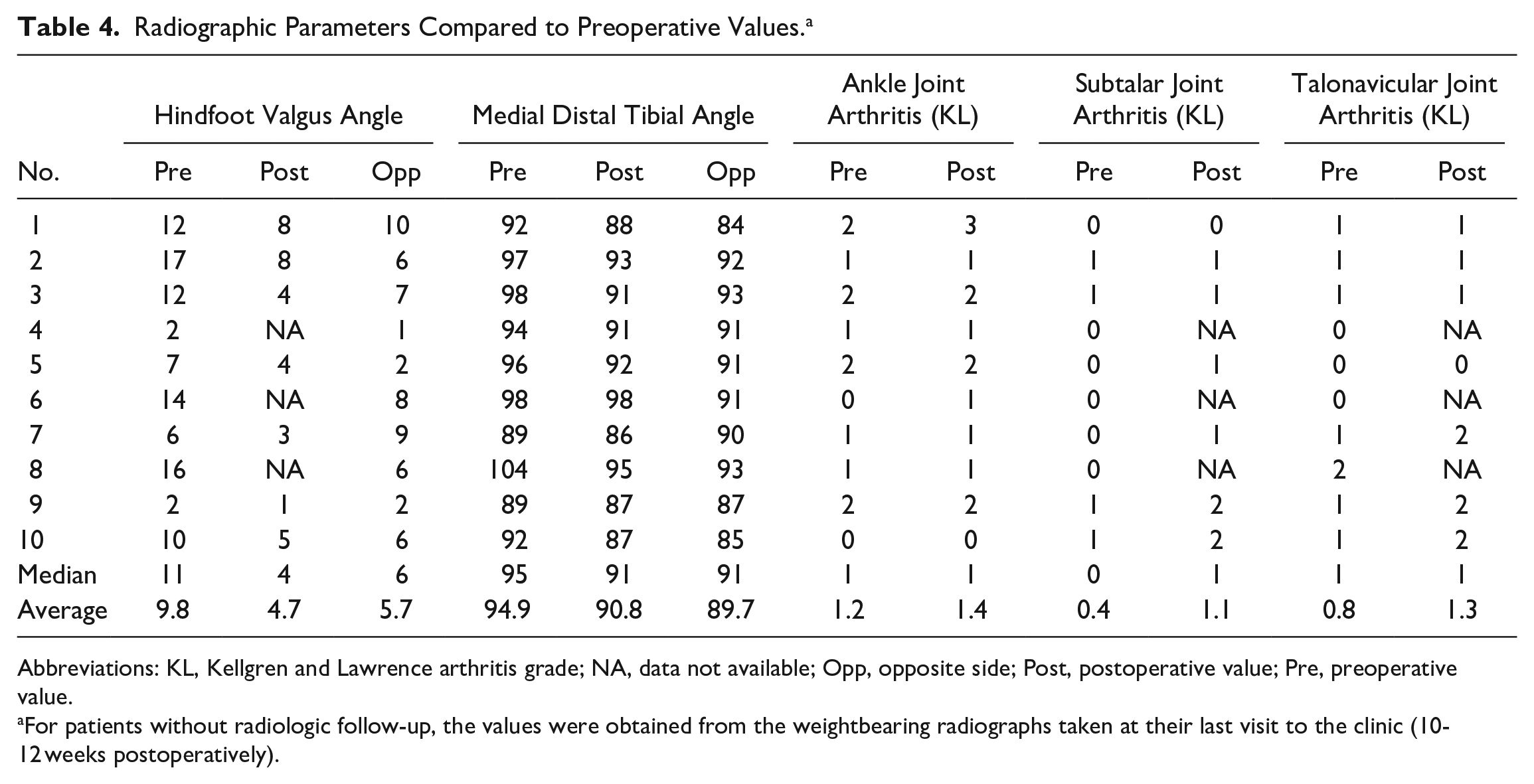
Abbreviations: KL, Kellgren and Lawrence arthritis grade; NA, data not available; Opp, opposite side; Post, postoperative value; Pre, preoperative value.
For patients without radiologic follow-up, the values were obtained from the weightbearing radiographs taken at their last visit to the clinic (10-12 weeks postoperatively).
No nonunion or malunion of the tibial plafond was seen. The median hindfoot valgus and medial distal tibial angles were reduced close to the values of the opposite side (Table 4).
Discussion
Post-traumatic ON of the lateral distal tibia is a rare but serious complication of ankle fracture-dislocation that is probably underreported in the literature. To our knowledge, short-term results of treatment have been published in 2 cases only. Rajagopalan et al 39 reported successful percutaneous drilling of the posterior distal tibia at 4.5 months following percutaneous screw fixation of a Maisonneuve injury and subsequent ORIF with flexible implants for initial malreduction. At 9 months after percutaneous drilling, the patient was reported to have resumed all regular activities without further detail. Jaffe et al 21 performed unipolar allograft reconstruction of the lateral tibial plafond and syndesmotic fusion in a 41-year-old male patient 1 year following ORIF of a Maisonneuve injury. One year after reconstruction, the patient complained about diffuse pain and stiffness at the ankle. On radiographic examination, there was progressive subsidence of the graft with valgus deformity.
Here, we report on the first prospective series investigating the results of joint-preserving reconstruction for posttraumatic ON at the lateral distal tibia. Important arguments in favor of reconstructive procedures are the preservation of near physiological ankle function, thus protecting the adjacent joints and defer problems associated with alternative, joint-sacrificing procedures. Prerequisites for successful joint preservation are good cartilage quality over a minimum of two-thirds of the articular surface, reasonable bone stock, the absence of infection, and good patient compliance. 40 In analogy to the recommendations for supramalleolar osteotomies of the distal tibia, patients with Kellgren and Lawrence third to fourth degree of ankle arthritis 23 were not considered for a joint-preserving procedure.25,45,48
Ankle arthroplasty is an alternative for advanced arthritis of the ankle joint. 20 However, in the presence of distal tibial necrosis, the indication should be made with caution given the limited fit of the tibial component. Ankle arthrodesis is another established treatment method for advanced ankle arthritis with a high fusion rate, substantial pain reduction, and good residual functional capacity of the foot.17,20 Concerns include nonunion, malalignment, and adjacent joint arthrosis in the long term.11,17,19,46,49 Arthrodesis or arthroplasty may be considered valid salvage procedure in case of ongoing pain or progression of arthritis following joint-preserving correction that may be carried out with good bone stock at a well-aligned ankle. In the present series, 1 patient (10%) underwent ankle fusion 1 year after corrective osteotomy for progressive arthritis. The patient was still satisfied with the final result at 7-year follow-up with solid union. Adjacent joint arthritis progressed in 4 cases in our series. None of these became symptomatic to require fusion but patients have to be counseled about that risk.
Necrosis of grafted bone at the ankle has been reported with a range from 0% to 56%.8,14,18,21,22,33,34 Reported risk factors are an excessively thin bone graft with a poor fit, high body mass index and patient age, and preexisting varus or valgus deformity.22,29 In 1 case of the present series, debridement and microfracturing were successfully performed for symptomatic partial graft necrosis. At 53-month follow-up, the patient was asymptomatic without evidence of graft failure on CT scanning.
Anterior ankle arthritis with impingement was the most common complication with recurrent limitation of motion. Implant removal, arthrolysis, and osteophyte resection were performed in 4 of 5 cases with good final outcome (Figure 6). These procedures have also been used successfully in similar cases. 21
Subjectively, 8 of 10 patients were satisfied or very satisfied with the outcome. In analogy, validated outcome measurements tailored to foot and ankle function6,15,35,38,47 showed a significant improvement compared with the preoperative values. However, pain scores at follow-up were still substantially higher than in the general population. The high satisfaction rate despite only moderate pain reduction might be explained by an improved ankle function after being offered a fusion, arthroplasty, or nonoperative treatment elsewhere.
The risk of atraumatic AVN of the distal tibia is reported at approximately 2% in the literature.12,13 Data for posttraumatic AVN/ON of the distal tibia after malleolar fractures are not available. 21 At our level 1 trauma center, the rate of ON of the lateral tibial plafond after ankle fractures was estimated with 0.11% over a 10-year period. However, this may be an underestimate because patients were not followed systematically. Overall, it appears that posttraumatic ON of the lateral distal tibia may be underreported.
The genesis of posttraumatic ON at the lateral tibial plafond is not completely clear. Blanke et al, 5 in their analysis of 28 cases, summarized 3 risk factors for posttraumatic AVN under the term “necrotic triad.” These include a high fibular fracture (Weber type C), a Gustilo-Anderson grade 3 open fracture, and complete dislocation of the talus from the ankle mortise. With all 3 present, AVN of the lateral tibial plafond occurred in 100% (6 patients). 5 Similarly, Assal et al 1 found open fractures in 7 of 9 patients and Weber type C fracture-dislocations in all patients with AVN of the lateral distal tibia. It may be speculated that impaction of the lateral distal tibia in pronation fractures (type 3 anterior malleolar fractures) also has the potential to induce ON 41 as reflected by the relatively high incidence in pilon fractures. 10 Thus, CT scanning should be used generously in the presence of an anterolateral distal tibial fragment in malleolar fractures to rule out plafond impaction and allow primary ORIF if present. 41 In the present study, correction of anterior tibial malunion restored ankle alignment (Table 4), syndesmotic congruity, and stability.
Initially, a high fibular fracture (Weber C) was present in 8 of 10 patients in our cohort and 7 had an ankle subluxation. No patient initially had an open fracture. In addition, high-energy trauma and a slightly higher proportion of women were observed in the literature and in the study group.1,5,7,21,26-28,39 Yet, the age of the patients does not seem to have any influence as AVN in the distal tibia was also detected in the MRI of 3 children with premature posttraumatic growth arrest 16 and in 2 cases each after Salter-Harris type I 37 and type II fractures.4,42
Finally, posttraumatic AVN may result from inadequate perfusion and venous outflow. 9 An anatomic study revealed a poor vascular supply to the lateral tibial plafond that may further be compromised by trauma and surgical dissection. 30 In addition, there is a risk of injury to the peroneal artery that passes through the interosseous membrane approximately 3 to 5 cm above the tibial plafond, when drilling or implanting a syndesmotic screw. 36 In fact, 4 of 10 patients in the present study had syndesmotic instability following the initial treatment. Previous reports described identical initial complications necessitating surgical correction at the level of the tibiofibular syndesmosis.1,7,21 The comorbidities and risk factors in the present study showed an average profile compared to the normal population. However, 5 of 10 patients were smokers, suggesting a negative influence of smoking on local circulation and bone healing following ankle fractures as suggested by earlier studies.3,32
This study has the inherent limitations resulting from a small patient number because of the rarity of the condition. The patient cohort was heterogeneous, there is a risk of selection bias, and there was no control group. On the other hand, we report the first prospective case series on joint-preserving osteotomy of the anterolateral distal tibia for posttraumatic AVN with a 100% follow-up of 1-9 years.
Conclusions
Posttraumatic ON of the lateral tibial plafond is a rare but serious complication of ankle fracture-dislocations. Probable risk factors include pronation injury, open fractures, high-energy trauma with compression of the lateral plafond, violation of the perforating branch of the fibular artery, and smoking. In the absence of advanced arthritis, joint-preserving corrective osteotomy with bone grafting is a reasonable treatment option, leading to high subjective patient satisfaction with moderate to good functional outcome and mobility and correction of the valgus deformity in most patients in our limited experience. Patients should be cautioned that revision surgery may be necessary mostly for anterior ankle impingement resulting from arthritis. With careful patient selection, fusion or arthroplasty may be deferred in the medium term, which is particularly useful in younger patients.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007241227928 – Supplemental material for Joint-Preserving Osteotomy of the Lateral Tibial Plafond for Posttraumatic Osteonecrosis: A Prospective Cohort Study
Supplemental material, sj-pdf-1-fai-10.1177_10711007241227928 for Joint-Preserving Osteotomy of the Lateral Tibial Plafond for Posttraumatic Osteonecrosis: A Prospective Cohort Study by Stefan Rammelt and Eric Jörg Walther in Foot & Ankle International
Footnotes
Ethical Approval
The study protocol was approved by the local institutional review board.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.