
Abstract

Keywords
Introduction
Posterior ankle and hindfoot arthroscopy is becoming increasingly popular among foot and ankle surgeons as a minimally invasive technique to address posterior hindfoot pathology. The purpose of this article is to describe indications, techniques, and potential complications for addressing posterior hindfoot pathology using prone posterior ankle and hindfoot arthroscopy.
Background and Indications
Improvements in technique, arthroscopic equipment, and distraction devices have widely expanded the indications of arthroscopy around the ankle. In a 1931 cadaveric study, Burman concluded that the ankle joint was too narrow for adequate viewing and not suitable for arthroscopy. 13 After decades of progress, van Dijk published the modern-day technique for 2-portal, prone posterior ankle and hindfoot arthroscopy (Figure 1). The technique describes 2 posterior portals, placed medial and lateral to the Achilles tendon, to access the posterior tibiotalar and subtalar joints and hindfoot extraarticular space (Figure 2). 75

Posterior prone arthroscopic procedure preparation and marking in a left ankle: (A) Location of landmarks and planned portal sites are outlined using a surgical marker. Care is taken to avoid the sural nerve and posteromedial neurovascular bundle. (B) Arthroscope and shaver in use for prone posterior ankle arthroscopy.
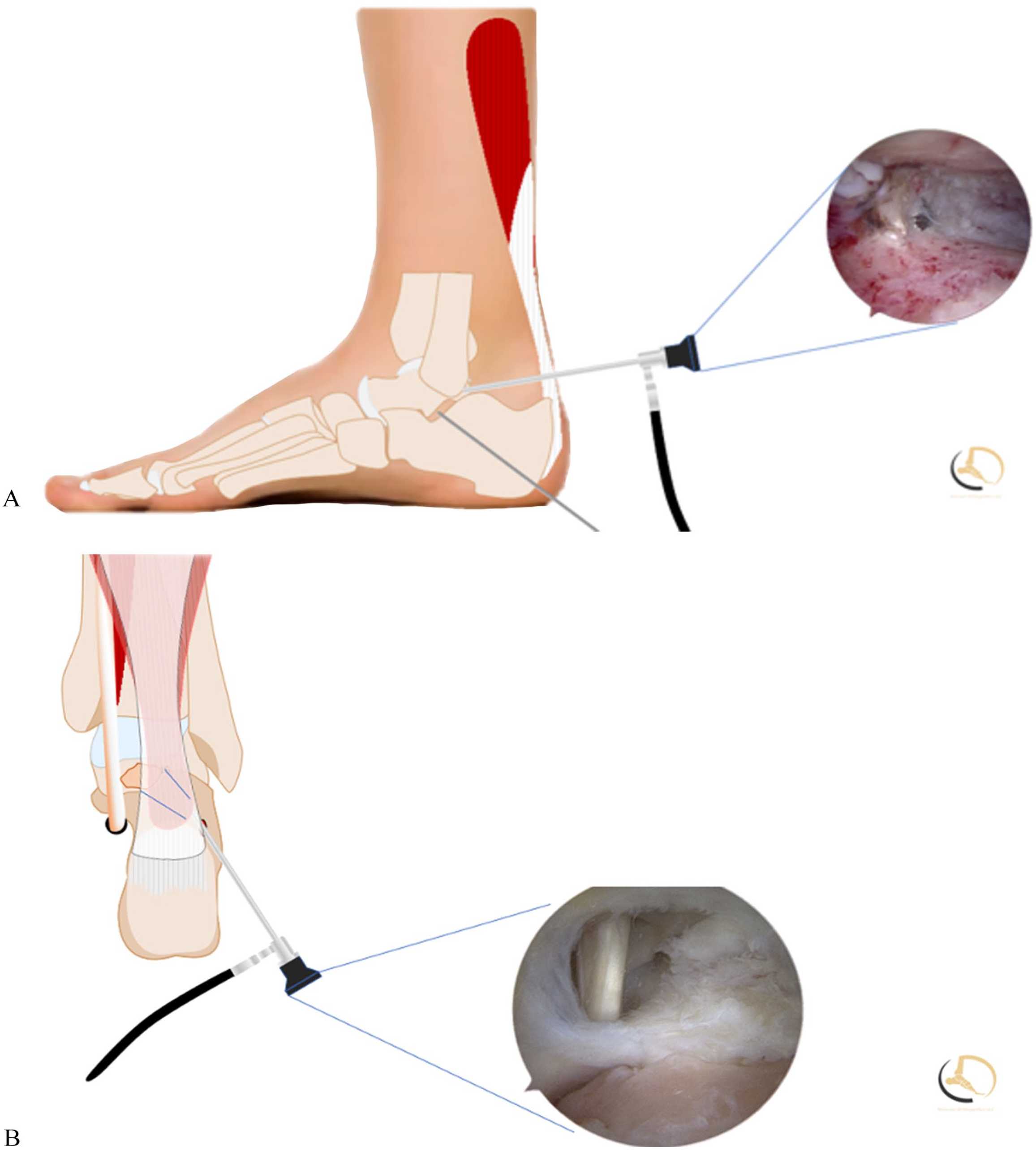
Illustration of prone posterior ankle arthroscopy in a right ankle: (A) Arthroscopic image and illustration of joint preparation during arthroscopic subtalar arthrodesis procedure. (B) Arthroscopic image and illustration of flexor hallucis longus debridement.
The safety and efficacy of this technique have been questioned, specifically regarding the risk of tibial and medial calcaneal neurovascular injury from the posteromedial portal. However, a cadaveric study published in 2002 showed that with the patient in the prone position, arthroscopic equipment could be safely introduced into the ankle without injury to the posterior neurovascular structures as long as equipment and dissection do not pass medially with respect to the FHL tendon. 63
As the body of literature concerning the safety and efficacy of prone posterior ankle and hindfoot arthroscopy has continued to grow, the indications for utilization of this technique have also expanded markedly. Grouped broadly, indications for prone posterior ankle arthroscopy can be divided into those involving bone, cartilage, or soft tissue pathologies. Commonly addressed bone pathologies include fractures of the posterior hindfoot,8,9,11 hypertrophic posterior talar process, 66 removal of loose bodies, 52 avulsion fractures, 22 posterior facet talocalcaneal coalition,7,10,51,59,69 Haglund deformity, 79 intraosseous cystic lesions, 60 and posterior impingement, which comprises os trigonum syndrome and a prominent trigonal process.57,78 Cartilage pathologies that are addressed with arthroscopy include posterior talar, tibial, or calcaneal osteochondral defects, 35 subtalar arthritis, 4 and synovial chondromatosis. 70 Extraarticular pathologies include flexor hallucis longus (FHL) tendinopathy, 41 retrocalcaneal bursitis, 79 posttraumatic synovitis, 50 pigmented villonodular synovitis (PVNS), 26 and other sources of soft tissue impingement. 66
The use of arthroscopy to treat certain ankle fractures has been proposed.8,9,11 Although arthroscopy is a valuable diagnostic and prognostic tool, definitive indications for arthroscopic reduction and internal fixation (ARIF) have yet to be established. Reported indications for ARIF include transchondral talar dome fractures, low-grade fractures of the distal tibia, syndesmotic disruptions, malleolar fractures, posterior talar body fractures, calcaneal fractures, and chronic pain following definitive management of ankle fractures.8,9,11,33,56,66,75 Additionally, there is evidence to support this approach for more simple fracture patterns without significant soft tissue damage; however, more complex fractures may be more optimally treated with open reduction and internal fixation (ORIF). 83
Posterior ankle impingement syndrome (PAIS) is a spectrum of disorders characterized by posterior ankle pain during plantarflexion or hyperflexion caused by overuse or trauma. Anatomic causes of PAIS include os trigonum displacement, hypertrophic posterior talar process, thickened posterior joint capsule, or osteophytes at the posterior distal tibia. 48 With increasing awareness of the condition and advancements in imaging, PAIS has become more commonly diagnosed in ballet dancers, soccer players, and other athletes engaging in repetitive plantarflexion.16,28,46,65,73,77 After failure of nonoperative approaches (rest, physical therapy, orthosis, analgesics, anti-inflammatory drugs, injections), surgical intervention should be considered. 66 Escalation to surgical treatment has been reported in 40% of cases. 80 Prone posterior ankle and hindfoot arthroscopy can be used to treat PAIS and remove associated pathology in cases that have failed nonoperative management.
Specific Pathology Presentation and Treatment
FHL Impingement
FHL tendinopathy or impingement is commonly associated with the onset of pain in the posterior ankle and hindfoot. Common symptoms of FHL tendinopathy include pain, swelling, stiffness, locking, or catching. Operative intervention for FHL tendinopathy in the form of tendon sheath debridement should be considered in cases that are resistant to nonoperative management. Prone posterior ankle tendoscopy for FHL tendon impingement is one of the most frequently performed procedures for PAIS. Before the modifications of Lombardi et al 40 and the hindfoot endoscopic techniques of van Dijk et al 75 , FHL release had been performed as an open procedure. Open and arthroscopic debridement have been described with positive outcomes for both techniques.27,50 A study investigating the open approach for FHL tendinitis and posterior impingement found 88% satisfaction after surgery at the expense of 15% complications. 27 However, the tendoscopic approach is less invasive and typically done with the 2-portal posterior approach through the fibrous osseous tendon tunnel at the posterior aspect of the talus.1,40,60,75
Once the working area is established for the prone posterior arthroscopic approach, the FHL is exposed on the posteromedial aspect of the hindfoot. This landmark creates a boundary to the neurovascular bundle and can help orient the surgeon to the posterior anatomy. The surgeon can then carry out debridement of restrictive soft tissue and mucoid degenerative tissues as well as address any bony pathology such as a Stieda process of the posterolateral talar tubercle or symptomatic os trigonum (Figure 3). 66 Outcomes for this procedure are favorable, with American Orthopaedic Foot & Ankle Society (AOFAS) score improvement of 48.7 preoperatively to 83.2 postoperatively when hindfoot endoscopic FHL release is performed without concomitant procedures. 50
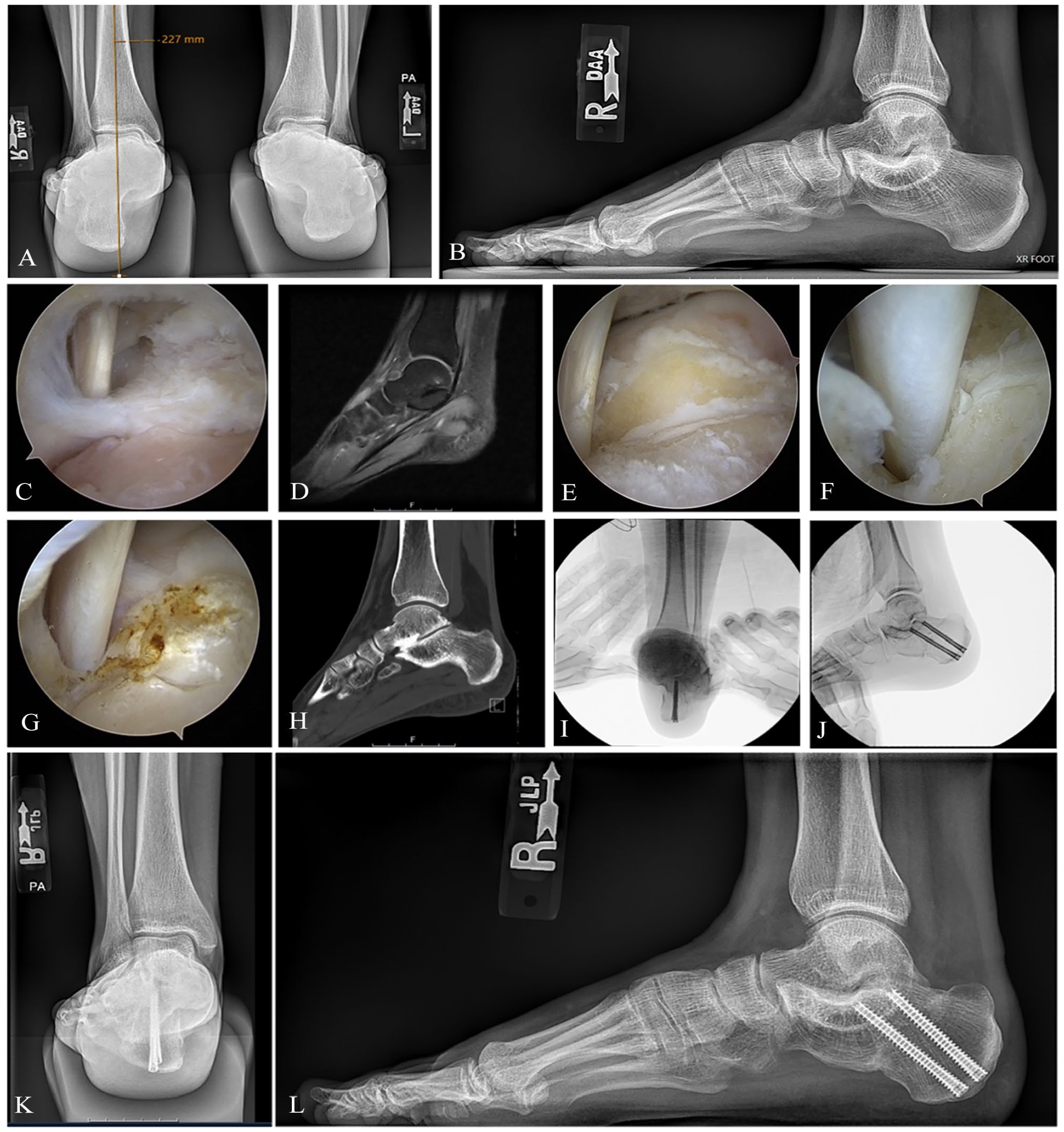
Case example of flexor hallucis longus (FHL)/posterior impingement decompression with subtalar coalition resection using prone posterior ankle arthroscopy and minimally invasive surgery (MIS) medial displacement calcaneal osteotomy (MDCO) for a right hindfoot valgus foot position. (A, B) Posteroanterior and lateral radiographic views of the foot revealing valgus position of the hindfoot. (C) Initial visualization of the FHL tendon reveals impinging scar tissue and Stieda process. (D) Exposure of the Stieda process using arthroscopic wand. (E, F) Posterior decompression with full exposure and debridement of the FHL and removal of the Stieda process. (G, H) Sagittal views of magnetic resonance imaging (MRI) of right foot revealing subtalar coalition that was resected using subtalar joint arthroscopy. (I, J) Intraoperative fluoroscopic images revealing MDCO that was completed using MIS techniques and fixated using two 5.5-mm canulated screws. (K) Posteroanterior and (L) lateral radiograph at the 3-month postoperative visit.
In a case report of an extreme massive effusion in the FHL tendon sheath with stenosing tenosynovitis and os trigonum, the patient was successfully treated by removal of the os trigonum, tenosynovectomy around the FHL, and release of the tendon via posterior ankle arthroscopy. The patient was asymptomatic and able to resume activities of daily living 1 week postoperatively. 71 Additionally, in a study evaluating the surgical technique and outcomes of all-inside arthroscopic treatment of FHL tendon impingement syndrome, Feng and colleagues 21 found meaningful advantages. These included small surgical trauma, fast functional recovery, and reliable outcomes with an average AOFAS score increase to 97 postoperatively (with all cases rated excellent or good). There were also no complications associated with the procedure.
Os Trigonum Syndrome and Painful Trigonal Process
A secondary ossification center at the posterolateral talar process mineralizes in 7% to 30% of individuals during adolescence. In most cases, the ossicle fuses with the talus within 1 year. However, if it persists, the accessory ossicle is known as the os trigonum. 44 The os trigonum may become symptomatic and cause chronic or acute pain, especially in cases with repetitive plantarflexion or concurrent FHL pathology.83,84 Clinical presentation includes tenderness and load-dependent pain between the Achilles and peroneal tendons as well as reduced plantarflexion (known as the “nutcracker phenomenon”). 44 Nonunion of a posterior talar process fracture can have a similar presentation.
The primary indication for surgical intervention for a painful os trigonum is persistent pain despite a trial of nonoperative treatment including activity modification, nonsteroidal anti-inflammatory drugs, physical therapy, immobilization, or ultrasonography-guided corticoid injections. 23 A posterolateral portal in combination with an anterolateral portal or a posteromedial portal has been used. The posterolateral portal is made just lateral to the Achilles tendon at the level or slightly above the tip of the lateral malleolus. The posteromedial portal is made just medially to the Achilles tendon in the horizontal plane at the same level as the posterolateral portal. Some authors have stated that os trigonum removal with the 2-portal approach reduces procedural difficulty and minimizes the risk of damaging posteromedial neurovascular structures.31,44,75 However, the posteromedial portal along with the posterolateral portal works effectively without any additional risk to the neurovascular bundle.47,54,63,78 The preferred technique involves partial detachment of the posterior talofibular ligament attached to the posterior talar prominence. The pathologic bony fragment can then be removed in one piece, in parts, or with a burr in the case of an intact enlarged trigonal process.
Substantial improvements in patient-reported outcomes (PROs) have been demonstrated after this procedure. 30 Across 252 os trigonum excisions from 15 studies, all demonstrated postoperative improvement in meta-analysis. 66 Compared to open procedure outcomes reporting a complication rate of 17% to 24% and an average postoperative AOFAS score of 87.6% with 5 months to recovery,1,43 the arthroscopic technique has demonstrated complication rates of 9% and an average AOFAS score of 86.4 with 3 months to recovery. 44 The primary benefit of the arthroscopic approach is the significantly shorter recovery time.
Subtalar Arthroscopy
Subtalar arthritis commonly develops after traumatic injury to the calcaneus or talus and can cause debilitating pain and deformity. Subtalar arthrodesis is a reliable procedure for pain relief and improved function in patients with isolated subtalar arthritis (Figure 4). 4 It may also be indicated for posterior tibial tendon dysfunction (now often termed chronic progressive flatfoot deformity) and congenital deformities when nonoperative treatments fail.17,19,23,24,42,61 Open procedures, although generally considered safe and effective, are associated with the risk of nerve injury and nonunion rates that range from 5% to 16%.33,34
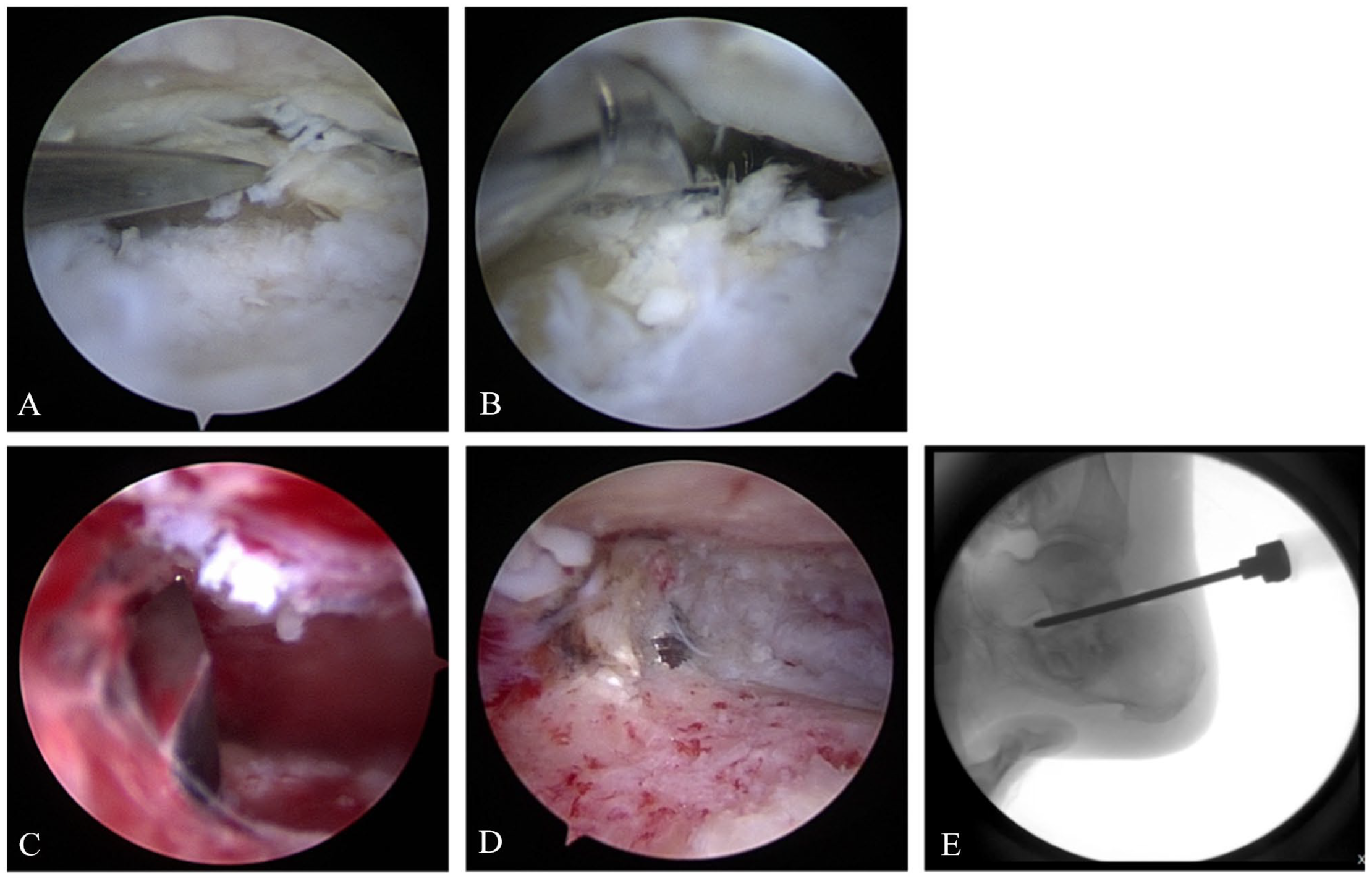
Technique for arthroscopic subtalar fusion. (A) Utilization of an osteotome for cartilage elevation and exposure of the subchondral bone. (B) An osteotome is used to complete cartilage removal. (C) Use of a drill bit for fenestration of the subchondral bone. (D) After joint preparation, a bed of bleeding, cancellous bone is achieved. (E) Fluoroscopic image demonstrating application of biologic products to enhance arthrodesis-site union.
The posterior ankle or subtalar arthroscopy (PASTA) 2-portal approach in the prone position was developed to improve outcomes after procedures addressing subtalar pathology (Figure 5). 75 PASTA provides safe, reliable, and minimally invasive access, superior visualization of the posterior talocalcaneal facet, easy screw fixation, less postoperative pain, and preservation of calcaneal/talar blood supply.38,83

Subtalar arthroscopy in a left ankle. (A, B) Anatomic landmarks are drawn. The posterior facet of the subtalar joint is marked using a dotted line. The course of the sural nerve is drawn out and care is taken to avoid this structure. (C) Accessory lateral portal is created to access the subtalar join for subtalar arthroscopy.
Fusion rates with this technique range from 91% to 100%.4,15,39,61,68,69 Moreover, PASTA obviates the need for an incision and extensive dissection to access the subtalar joint. Thus, in patients with risk factors for poor wound healing, PASTA represents an excellent option for subtalar pathology.
The portal placement for the PASTA technique is similar to the technique described above. The use of a third anterolateral or central portal has been described posterior to the sinus tarsi for introduction of a blunt trocar as a joint distractor to more adequately access and prepare the subtalar joint.2,4,7,39,52,59,61,69 In addition to the standard instrumentation described above, a burr and an arthroscopic rasp are also used to assist in joint preparation. 7 Although the posterior facet is the primary area of focus during joint preparation, access to the middle facet can also be obtained if necessary through the proper use of a blunt trocar as a joint distractor. Once the joint is prepared, guidewires can be passed across the subtalar joint to aid in the placement of the cannulated screws. In this position, it is very easy to use a minifluoroscopy unit for screw placement. The arthroscope can also be used to visualize guidewire placement across the joint to confirm ideal placement. If needed, a minimally invasive calcaneal osteotomy can also be combined with the subtalar arthroscopy.
With regard to complications encountered with the PASTA technique, in a multicenter study, subtalar arthroscopy outcomes reported an 8.5% complication rate in 189 cases. 47 The 16 complications included plantar numbness (3 of 4 resolved), sural nerve dysesthesia (2 of 3 resolved), Achilles tendon tightness (all 4 resolved), and complex regional pain syndrome and infection (both cases resolved). Overall, subtalar arthroscopy can be performed with a low incidence of major postoperative complications.
Posterior Talar Body Fractures
Fractures of the talus represent 3% to 6% of foot and ankle fractures and can be categorized into fractures of the talar neck, dome, processes, or body. These injuries typically result from falls, motor vehicle accidents, repetitive kicking in sports, or direct trauma. 11 Talar body fractures under the Sneppen classification occur in 5 categories: compression, shearing, posterior tubercle, lateral tubercle, or crush fractures.2,9,64 Although definitive indications for ARIF have not yet been determined, ARIF is thought to be optimally suited for simple fracture patterns without severe soft tissue damage and for fractures involving portions of the talus that are visible through the posterior arthroscope such as the posterior talar body and the posterior portion of the talar dome. More complex fractures and those involving the talar neck or anterior talar body may be difficult to access and reduce using fully posterior arthroscopic techniques and may be associated with a risk of compartment syndrome. These fracture patterns often require either the addition of an anterior arthroscopic approach or an open approach for adequate reduction and fixation. 11
As a further extension of this technique, prone arthroscopy may be combined with ORIF for fractures that require the removal of small fragments and can be used in conjunction with minimally invasive reduction techniques to confirm adequate reduction of the articular surface. Posterior arthroscopy is also indicated for fractures involving the posterior one-third of the talus. Moreover, arthroscopic techniques are emerging for use in management of complications of talar fracture such as infection, skin necrosis, osteonecrosis, malunion, and posttraumatic arthritis. 25
Although this procedure is in its infancy, several case series and case reports have demonstrated successful outcomes with ARIF of talar fractures through the posterior approach.33,34 Despite some promising reports on the utilization of prone posterior ankle and hindfoot arthroscopy for talar fracture, 33 ORIF remains the standard of care for surgical management, and utilization of ARIF is not an excuse for inadequate restoration of the talar morphology. Future research should aim to continue to delineate the role of ARIF in the treatment of fractures of the talus.
Posterior Osteochondral Lesions of the Talus
Posterior talar osteochondral lesions (OCLs) are defects of the posterior talar cartilage and subchondral bone typically due to a traumatic event that causes complete or partial detachment of the osteochondral fragment. Many of these lesions continue to be symptomatic after nonoperative measures have been employed. The more widespread recognition of this pathology over the last several decades has led to a growth of treatment strategies that include nonsurgical treatment (rest and immobilization), surgical excision (excision and curettage, excision with curettage and drilling/microfracture), placement of bone graft, retrograde drilling, and osteochondral transplantation.
Indications for arthroscopic treatment depend on the size and duration of the lesion, patient age and alignment, use of previous conservative treatments, and symptoms such as reduced function or range of motion, stiffness, catching, locking, and swelling. Although certain posterior OCLs may be accessible through the anterior arthroscopic approach with distraction, the authors believe posterior OCLs are best visualized with a prone posterior approach. Range of motion (ROM) of the ankle can be assessed preoperatively to evaluate whether a certain OCL may be amenable to anterior arthroscopy in a patient with adequate ROM. In certain cases, a CT scan in plantarflexion additionally helps determine which lesions are amenable to anterior arthroscopic treatment. In cases where the posterior approach is deemed more effective, posterior arthroscopy provides an excellent working area for posterior OCL, and half of the talar dome can be reached with this technique in dorsiflexion and distraction. 54 Lesions posterior to the dome are easily accessible utilizing the prone posterior arthroscopy. 35 Moreover, although a large portion of the posterior talus can be accessed by dorsiflexing the ankle, noninvasive distraction can be used as well to help facilitate access to the lesion if needed.
The outcomes of OCL treated with a prone posterior arthroscopic approach have yet to be reported in large sample sizes. In a prospective study of 36 patients who underwent posterior endoscopic OCL treatment, the average AOFAS score improved from 42.3 preoperatively to 89.3 postoperatively. The average visual analog scale (VAS) also improved from 7.75 preoperatively to 1.54 postoperatively. There were 3 minor and transitory complications, including pain on the portals, ecchymosis, and hypoesthesia of the heel. 6 Future research should aim to explore whether the enhanced visualization from the prone posterior arthroscopic approach leads to higher success rates than those reported with anterior arthroscopy. 82
Haglund Retrocalcaneal Bursitis
Haglund syndrome is a common source of posterior heel pain localized to the retrocalcaneal region. Haglund syndrome represents a triad of posterosuperior calcaneal bony enlargement (Haglund deformity), retrocalcaneal bursitis, and Achilles tendinopathy. The Haglund deformity is a bony enlargement on the posterosuperior aspect of the calcaneus. 41 Patients with a cavus foot may be at an increased risk of developing this deformity because of the vertical nature of the heel resulting in increased bone tendon contact. The presence of a Haglund deformity can lead to painful inflammation of the bursa between the ventral aspect of the Achilles tendon and the posterior border of the calcaneus or Achilles tendinosis at the site of bony impingement.18,29,37,45,58,62 Patients present with pain, swelling, and stiffness at the posterior heel. Surgical treatment is recommended in patients with persistent symptoms after a prolonged course of conservative treatment. The goal of surgical treatment is to increase the retrocalcaneal space by resecting the retrocalcaneal bursa and removing the posterosuperior calcaneal prominence.5,32,53 Open techniques use a midline incision and have been associated with a prolonged recovery and postoperative complications including stiffness, scarring, Achilles tendon avulsion, and skin breakdown.5,32,53
Endoscopic treatment of Haglund syndrome is a minimally invasive technique that has been shown to be safe and efficacious. This endoscopic Achilles tendoscopy and endoscopic calcaneoplasty allows for improved visualization and reduces the risk of wound dehiscence, painful scars, and subsequent nerve entrapment. 74 Additionally, it has been shown to decrease bony resection, therefore decreasing the risk to the Achilles tendon insertion and iatrogenic calcaneus fracture. Several studies show lower morbidity with less pain and earlier return to function compared to open techniques. 79 The primary indications for an endoscopic approach are insertional Achilles tendinopathy or Haglund syndrome. Intratendinous calcifications are a relative contraindication for an endoscopic approach and are treated best with an open technique.
Several approaches to endoscopic calcaneoplasty have been proposed, both prone and supine. The 2-portal technique utilizes a medial and lateral posterior portal. A lateral portal is made first just above the superior portion of the calcaneus, between the calcaneal branch posteriorly and the sural nerve anteriorly. A trocar is passed from the lateral portal to the medial side and the medial portal is made under direct visualization. The retrocalcaneal bursa is resected using a 4-mm shaver from the superior aspect of the calcaneus and borders of bony resection are defined. A burr is then used to resect the Haglund deformity from proximal to distal, down to the Achilles tendon insertion (Figure 6). A 3-portal technique was described by Wu et al 79 where a proximal posterolateral portal is established 5 cm proximal to the Achilles tendon insertion. The proximal portal allows for full visualization of the posterosuperior calcaneal prominence and instrumentation is used interchangeably in the distal portals. Fluoroscopy may be used to confirm the adequacy of resection. The case series published by these authors showed improvement in AOFAS scores at 3-year follow-up.
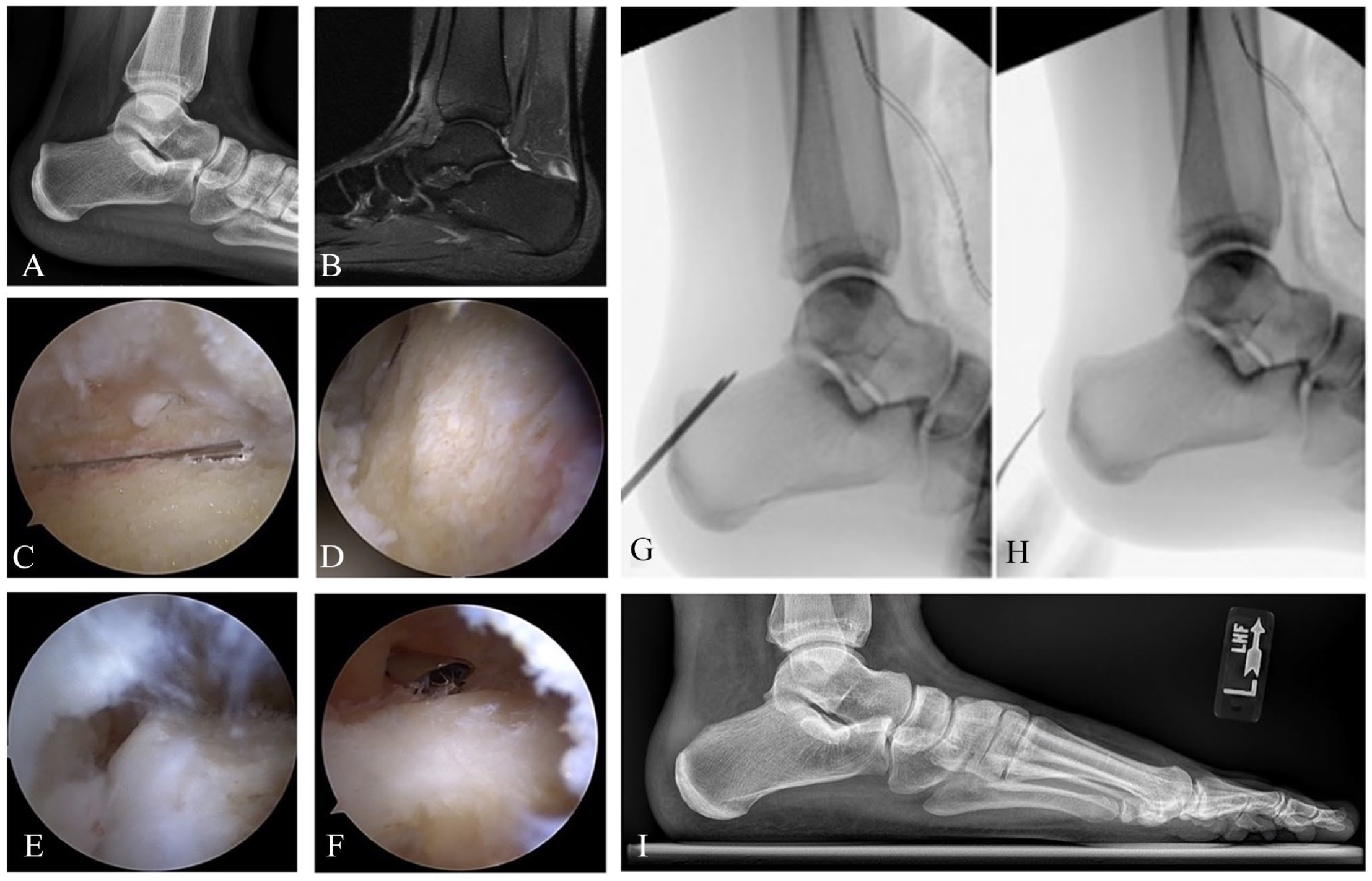
(A, B) Lateral radiograph and sagittal magnetic resonance imaging reveal prominent Haglund deformity and insertional Achilles tendinopathy in a left ankle. (C) Initial arthroscopic view of the prominent calcaneal exostosis. (D) An arthroscopic shaver is used to expose subchondral bone prior to introduction of the arthroscopic burr. (E, F) The arthroscopic burr is used to remove the Haglund deformity. (G, H) Intraoperative fluoroscopy confirms complete removal of the Haglund prominence. (I) Postoperative lateral radiograph.
Endoscopic and minimally invasive surgical treatment for Haglund deformity, retrocalcaneal bursitis, and Achilles tendonitis is an area of active research. High satisfaction rates (92%) and relatively low complication rates (8%, including 1 nonunion and 1 case of symptomatic hardware in a series of 26 patients) have been reported using this technique. 49 Future research should aim to expand the indications for endoscopic management of Haglund deformity, and further delineate which patients are better served through either open or endoscopic techniques.
Complications
Although generally considered a safe, minimally invasive technique, a variety of complications have been reported after prone posterior ankle arthroscopy. Damage to the surrounding neurologic structures is considered the most common serious complication following prone arthroscopy. In a sample of 189 posterior and hindfoot arthroscopic procedures, Nickisch et al 47 report a rate of injury to the tibial medial calcaneal branch or the sural nerve of 3.7% (7 cases in total, 4 to the tibial nerve, and 3 to the sural nerve). Of those 7 injuries, 2 failed to resolve. Other authors have reported similar nerve injury rates of 4.2%. 51 Although these numbers are not insignificant, other authors have reported higher rates of sural nerve injury with open subtalar arthrodesis when compared to arthroscopic. 59
Although many authors have raised concerns regarding the proximity of the posteromedial portal to the vascular structures in cadaveric studies,20,76 the large number of reports demonstrating safety with regard to injury to the tibial neurovascular bundle have questioned this line of thinking.3,12,25,36,47,70,78 As the number of cases performed without injury to the vascular structures of the hindfoot grows, we can be reasonably reassured that the neurovascular bundle is at very low risk during posterior ankle arthroscopy and endoscopy, assuming adherence to standard safety measures including appropriate portal placement, accurate identification of anatomic landmarks and direct visualization during cutting, burring, or resection portions of the procedure.
Other complications that have been reported in the literature after hindfoot arthroscopy include superficial and deep infection, tendinous and ligamentous injury, tourniquet-related pain, hardware-related complications, and deep venous thrombosis. With regard to infection, in a large series of 311 posterior ankle arthroscopies, a superficial infection rate of only 0.3% was reported. 81 Other authors have reported slightly higher rates of infection: 1.05% (2 of 189 posterior ankle arthroscopies). 47 Given the relative rarity of this complication, however, specific definitions of what constitutes an infection and differing patient comorbidity burden may greatly impact the incidence reported across studies. In brief, posterior ankle and hindfoot arthroscopy is associated with lower complication rates and faster recovery than similar open procedures.1,43,44 Tendinous and ligamentous injury can also occur after posterior ankle arthroscopy, with very low reported rates. In a review of 499 posterior ankle and hindfoot arthroscopies by Ribbans et al, 57 iatrogenic injury to the FHL was recorded as 0.2%. Achilles tendon contracture can be observed as well, with rates at high as 4.1%. 78 As a historical complication, Achilles tendon rupture has been observed with the use of a trans-Achilles portal for posterior arthroscopy (no longer used today). 14
Authors’ Preferred Treatment and Technique
The authors’ preferred technique for prone posterior ankle and hindfoot arthroscopy is presented here and can be slightly modified based on the specific procedure in question. The procedure and order of portal placement have been extensively described by van Dijk48,72,73,75 in which the posterolateral portal is established first. The authors’ preferred technique differs from this traditional approach in 2 ways; first, the posteromedial portal is established followed by the posterolateral portal under direct vision, and the subtalar joint space is entered primarily without extraarticular debridement.
To begin the procedure, the patient is positioned prone at the edge of the operating room table. A sterile bump is placed under the ankle joint. Although noninvasive traction can be used, most posterior ankle and hindfoot arthroscopy cases can be performed without the use of traction. The posteromedial portal is established first, at or just proximal to the level of the tip of the medial malleolus and slightly medial to the Achilles tendon. A 20-gauge needle at the site of the future posteromedial portal is used to inject 5-10 mL of saline into the posterior recess. Once a small vertical stab incision is made, a hemostat is introduced into the wound, staying central in the hindfoot, and is directed laterally and anteriorly away from the neurovascular bundle, pointing in the direction of the interdigital web space between the second and third toe. Establishing the portal from the medial to lateral aspect of the ankle reduces the potential risk of blunt injury to the neurovascular bundle. Once the posterior compartment and subtalar joint are visualized and the posterolateral portal is established under direct vision from the posteromedial portal, the scope can then be placed in the established posterolateral portal with less risk. The camera is inserted into the subtalar joint or space posterior to the talus or subtalar joint through the posteromedial portal. With intraarticular pathology, a smaller-caliber arthroscope is preferred (such as 2.4 or 2.7). There are also commercially available “nanoscope” technologies (Arthrex, Naples, FL) that can facilitate access to areas that have limited exposure. The nanoscope is a relatively new and evolving approach and is particularly useful for diagnostic indications or less extensive surgeries with narrow spaces, such as osteochondral lesions of the subtalar joint. 55 Fluid distension is required, however, for extensive arthroscopic surgeries, such as os trigonum removal, arthrodesis, osteochondral debridement and curettage, and retrocalcaneal debridement excision. For these cases, the authors recommend using a larger scope to improve fluid flow and visualization. In cases that do not require substantial intraarticular exposure (ie, os trigonum excision or subtalar arthrodesis), a 4.5-mm arthroscope can also be used.
The posterolateral portal is established next and is placed slightly lateral to the Achilles tendon at the level of or just above the tip of the lateral malleolus, at the same horizontal level as the posteromedial portal. Care should be taken to remain medial to the sural nerve in order to avoid iatrogenic nerve injury. A 20-gauge needle is introduced at the site of the proposed posterolateral portal. The needle is used to triangulate with the camera prior to making this portal. A vertical incision is then created, and a hemostat is again introduced into the wound, toward the arthroscope currently in place through the posteromedial portal. The arthroscope is then used as a guide to travel anteriorly in the direction of the ankle or subtalar joint, facilitating triangulation. 75 When establishing the posterolateral portal, the second metatarsal can be used as a visual guide for the direction of the hemostat to avoid iatrogenic injury to the neurovascular bundle. 67 Once the tip of the hemostat has been visualized, the hemostat is spread slightly, establishing a working track for the introduction of instrumentation. An arthroscopic shaver is then introduced to clear the posterior periarticular space and establish a working area immediately posterior to the talus. When clearing the tissue, care is taken to point the open face of the shaver in a lateral direction, to avoid inadvertent injury to the medial structures. Synovial debridement is carried out until the subtalar joint can be visualized. Debridement is continued medially along the subtalar joint until the FHL tendon is visualized medially within the arthroscopic field. The medial neurovascular bundle is located anterior and medial to this structure and is therefore safe if the portal remains lateral to the FHL tendon during surgery. The tibiotalar joints can also be visualized, occasionally requiring resection of posterior capsular structures above the posterior process of the talus. Care should be taken to avoid injury to the ligamentous structures of the tibia and talus, such as the posterior inferior tibiofibular ligament.
Conclusion
Prone posterior ankle and hindfoot arthroscopy continues to grow in popularity and has demonstrated favorable outcomes in comparison with open approaches, especially regarding minimizing complications. As techniques are continually refined and perfected, prone posterior ankle arthroscopy will become a requisite skill for the orthopaedic foot and ankle or sports surgeon. Further research should continue to expand on the indications and outcomes of procedures performed using prone posterior ankle and hindfoot arthroscopy.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007231204882 – Supplemental material for Posterior Ankle and Hindfoot Arthroscopy: A Contemporary Review
Supplemental material, sj-pdf-1-fai-10.1177_10711007231204882 for Posterior Ankle and Hindfoot Arthroscopy: A Contemporary Review by Albert Thomas Anastasio, Katherine Kutzer, Lacey Giambelluca, Nicholas Lee Strasser and Annunziato Amendola in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.