
Abstract
Background:
Malunion of tibial pilon fracture, especially with a large cartilage loss of the tibial plafond, is a tough clinical conundrum. This study describes a joint-preserving technique that mainly involves corrective intraarticular osteotomy and osteoperiosteal iliac autograft transplantation for treating these generally considered unreconstructable tibial plafond.
Methods:
Sixteen patients with an average age of 33.6 years who were treated with this joint-preserving method between 2013 and 2020 were retrospectively analyzed. Ankle distraction was applied in all patients. Additional osteochondral autograft transplantation for talus was performed in 4 patients and supramalleolar osteotomy in 2 patients. The visual analog scale (VAS) score, the American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot score, the 36-Item Short Form Health Survey (SF-36) score, and the ankle range of motion (ROM) were used for outcome analysis. Radiographic assessment was conducted, and the complications were recorded.
Results:
At a mean follow-up of 41.1 months, the mean VAS, AOFAS, and SF-36 scores improved from 6.3, 47.6, and 38.0 to 1.7, 84.4, and 70.8, respectively (P < .001 for each). The ankle ROM improved from 27.5 to 32.2 degrees (P = .023). The mean area of ilium blocks was 3.5 cm2, and the mean external fixation time was 94.1 days. Radiographs showed that good osteointegration was found in all patients and no significant progression of osteoarthritis in 15 patients. The major complications included poor incision healing in 2 patients and severe ankle stiffness in 2 patients, with one of them developing considerable varus-type osteoarthritis but reporting no pain. No deep infection, nonunion, or malunion occurred, and no secondary arthrodesis was performed during the final follow-up.
Conclusion:
Osteoperiosteal iliac autograft transplantation might be an alternative surgical option for reconstructing unreconstructable malunited pilon fractures with a large cartilage loss of the tibial plafond in young patients.
Level of Evidence:
Level IV, case series.
Introduction
Pilon fractures are typically high-energy injuries that mainly affect young men of working age,26,48,50,54 and malunions of these fractures can occur because of the complicated fracture pattern and suboptimal treatment. The residual articular step-off and/or malalignment of the distal tibia,11,43,46,51 apart from the comminuted property and the initial death of articular chondrocytes,29,49 make large-area cartilage loss of the tibial plafond not rare. Often, this kind of malunited distal tibia combined with a massive osteochondral defect is considered unreconstructable, and ankle arthrodesis or replacement are considered options for further treatment. However, for young patients, the known long-term complications brought by these ankle-sacrificing procedures may continue to plague them later. Managing this kind of injury, especially in young patients, remains a challenging issue.
In this study, we report our results with a joint-preserving method mainly involving intraarticular osteotomy and osteoperiosteal iliac autograft transplantation (OPIAT) to address the malunions of pilon fractures combined with large-area cartilage loss of the tibial plafond in young patients.
Methods
This retrospective study was approved by the ethics committee of our hospital and carried out in accordance with the Declaration of Helsinki. From 2013 to 2020, a total of 16 patients were included in this retrospective study (Table 1). The inclusion criteria included skeletally mature patients who suffered malunited pilon fractures treated with corrective intraarticular osteotomies and OPIAT. The exclusion criteria were patients with concomitant injuries in the ipsilateral foot, incomplete clinical information, and less than 2 years of follow-up.
Details of the 16 Patients.
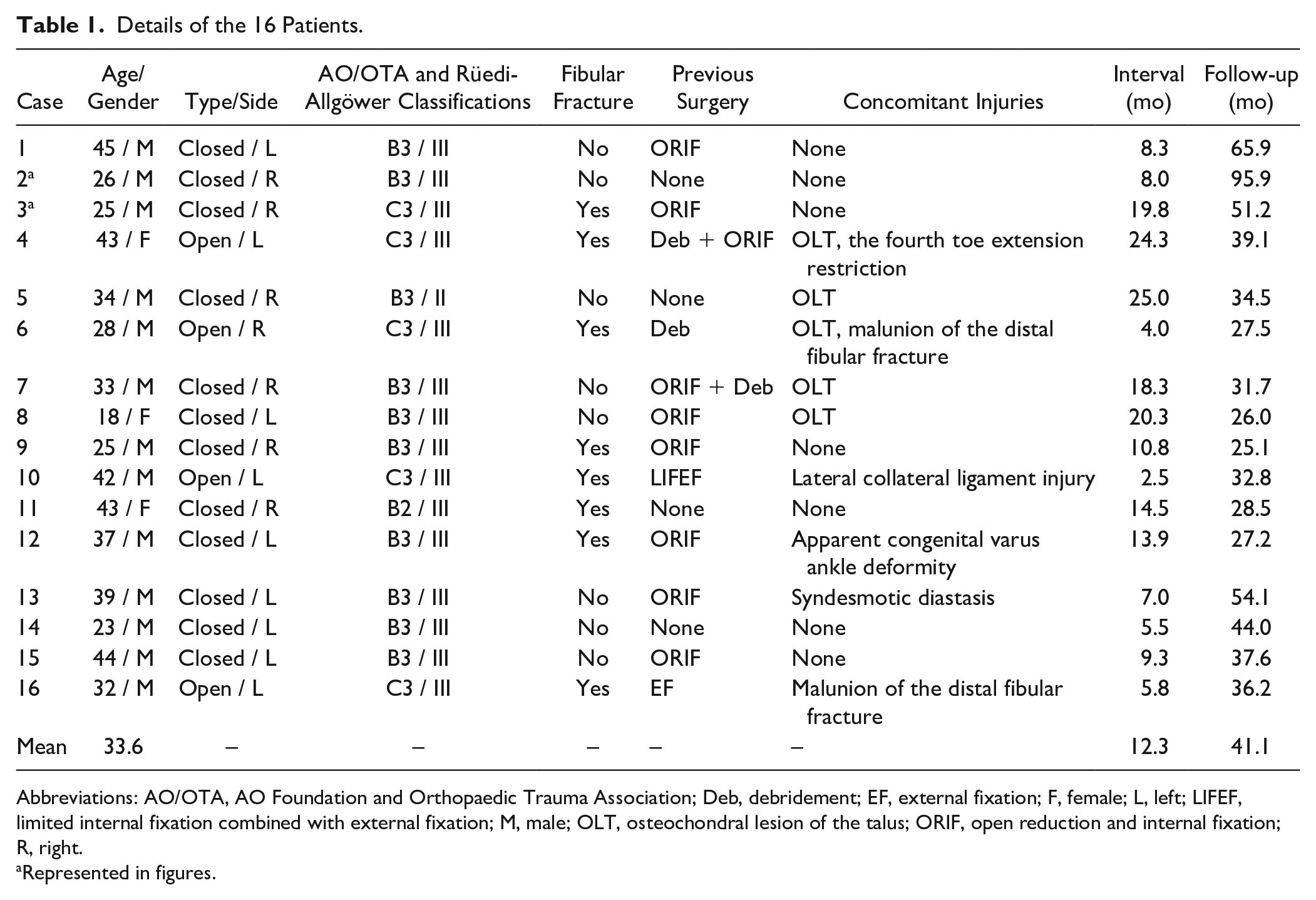
Abbreviations: AO/OTA, AO Foundation and Orthopaedic Trauma Association; Deb, debridement; EF, external fixation; F, female; L, left; LIFEF, limited internal fixation combined with external fixation; M, male; OLT, osteochondral lesion of the talus; ORIF, open reduction and internal fixation; R, right.
Represented in figures.
Preoperative Management
Plain radiographs, long-leg standing radiographs, and CT scans with 3D reconstruction were performed to assess the deformity and design the surgical plan. MRI for evaluation of cartilage damage was helpful in some cases. The initial radiologic films were normally required to analyze the injury mechanism and develop thoughtful treatment protocols. Fractures were graded by the AO Foundation and Orthopaedic Trauma Association (AO/OTA) classification 31 and the Rüedi-Allgöwer classification. 41 A modified Kellgren and Lawrence (K&L) score 42 was used to classify the grade of ankle osteoarthritis: stage Ⅰ, early sclerosis and osteophyte formation without joint space narrowing; stage Ⅱ, narrowing of the joint space; stage Ⅲ, tibiotalar subchondral bone contact; and stage Ⅳ, complete destruction of the tibiotalar joint. Each radiograph was reviewed independently by 2 senior orthopaedic surgeons, and any discrepancies were settled by discussion and consensus. The indications for the joint-preserving procedure were young active patients, adequate bone mass, relatively well-preserved talar articular surface, without signs of active infection, and good compliance with strong intentions to preserve the joint. The preoperative plain radiographs and CT images of a typical case (case 3) are shown in Figure 1.
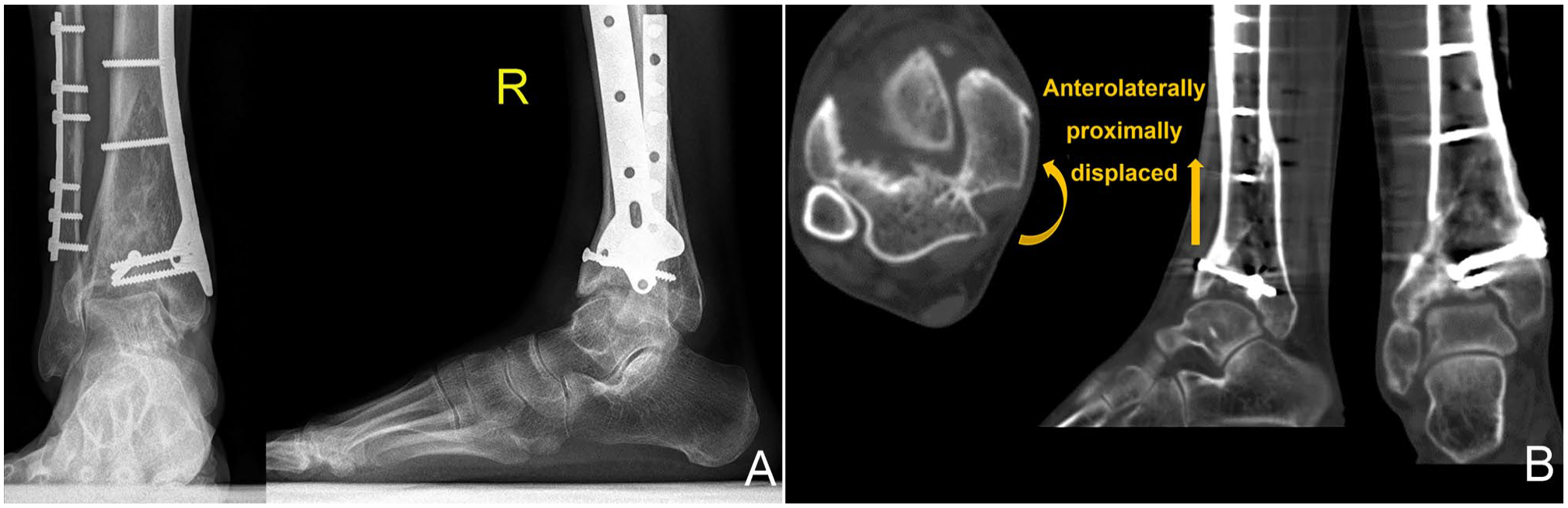
Preoperative plain radiographs and computed tomographic (CT) scans of a 25-year-old man (case 3 from the included table) with a malunited tibial plafond after a pilon fracture treated operatively elsewhere 19.8 months ago: (A) The anteroposterior and lateral view radiographs show a malunited plafond and an incongruent ankle mortise with the talus varus tilt and anterolateral displacement. (B) The axial, coronal, and sagittal views of the CT scans show an anterolaterally proximally displaced medial fracture block and a large-area osteochondral defect of the tibial plafond.
Surgical Technique
All procedures were performed under general anesthesia and thigh tourniquet control in the supine or floating position by a senior surgeon. Appropriate approaches were performed for adequate exposure and proper fixation with respect to the previous incisions and the soft tissue envelope status. After articular debridement and arthrolysis, the osteotomy was performed through the original main fracture lines. After reducing the malunited bone blocks, the unreconstructable osteochondral segments of the plafond were removed. A corresponding shape and size of full-thickness autologous ilium was harvested from the patient’s ipsilateral iliac crest, with the periosteum carefully preserved. After properly tailoring and drilling the convex side with a 2-mm pin to facilitate bone healing, the concave side of the ilium with periosteum was embedded into the cavity to articulate with the surface of the talus. The images of intraoperative implantation and fixation of the osteoperiosteal autograft of the typical case are shown in Figure 2. Cancellous bone from the iliac crest was used to fill the metaphyseal bone defect and the space between the osteoperiosteal graft and the wall of the defect cavity. Temporary fixation with K-wires was performed to confirm the articular congruity under direct visualization and intraoperative radiography. Then, rigid definitive internal fixation was achieved, and the incisions were closed without undue strain. Ankle distraction was then carried out with circular Ilizarov ankle–hinged external fixator with approximately 7 mm putative distraction across the ankle.
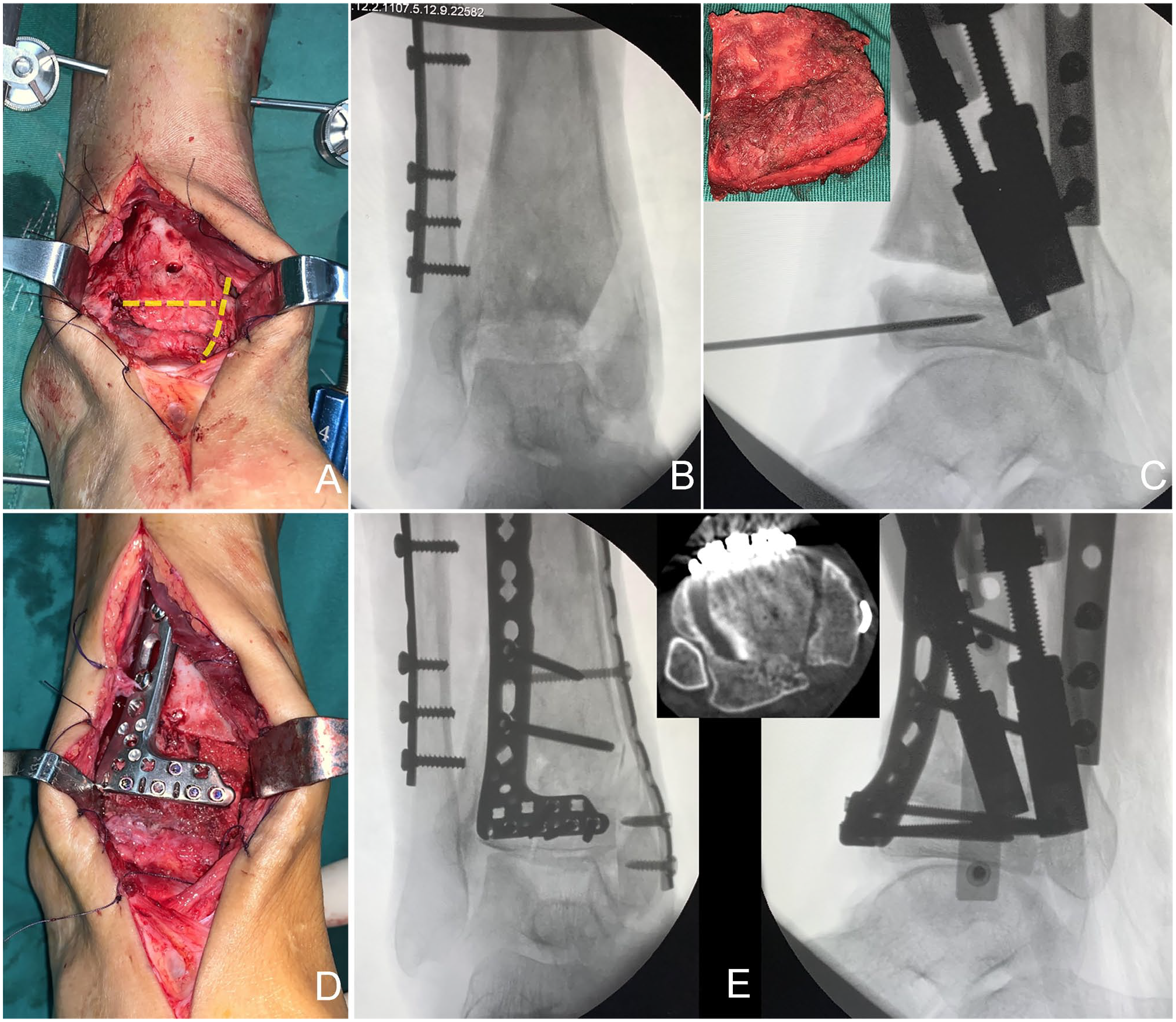
Intraoperative gross appearance and radiographs of case 3: (A) The yellow dash lines display the sites of osteotomies. (B) Anteroposterior view radiograph shows anterior and medial malleolar osteotomies have been completed. (C) Properly embed the osteoperiosteal iliac autograft into the cavity with a K-wire as a joystick. (D) Definite fixation with plates and screws. (E) Radiographs and axial view computed tomographic scan show the reconstructed tibial plafond with a large osteoperiosteal iliac autograft. [See online article for color figure.]
If residual supramalleolar deformity existed after restoring the contour of the plafond with corrective intraarticular osteotomies, supramalleolar osteotomy (SMOT) was performed to realign the lower extremity. If osteochondral lesions of talus existed, simultaneous mosaicplasty procedure was performed with osteochondral autograft grafts harvested from the ipsilateral lateral femoral condyle. Achilles tendon lengthening, ligament repair, and syndesmotic fixation were conducted if necessary.
Postoperative Management
The ankles were immobilized for 2 weeks with the ankles in a slight dorsiflexion position and elevated until the incision healed. Early active and passive joint training was then performed under the guidance of a senior physiotherapist during the day, and at night, the ankle was immobilized in a 5- to 10-degree dorsiflexion position. Patients received partial weightbearing exercises 6 weeks postoperatively assisted with crutches, and were allowed to gradually progress to full weightbearing after confirming bone union by the surgeon at approximately 12 weeks. Then the external fixators were removed, and rehabilitation exercises continued for another month.
Outcomes Assessment
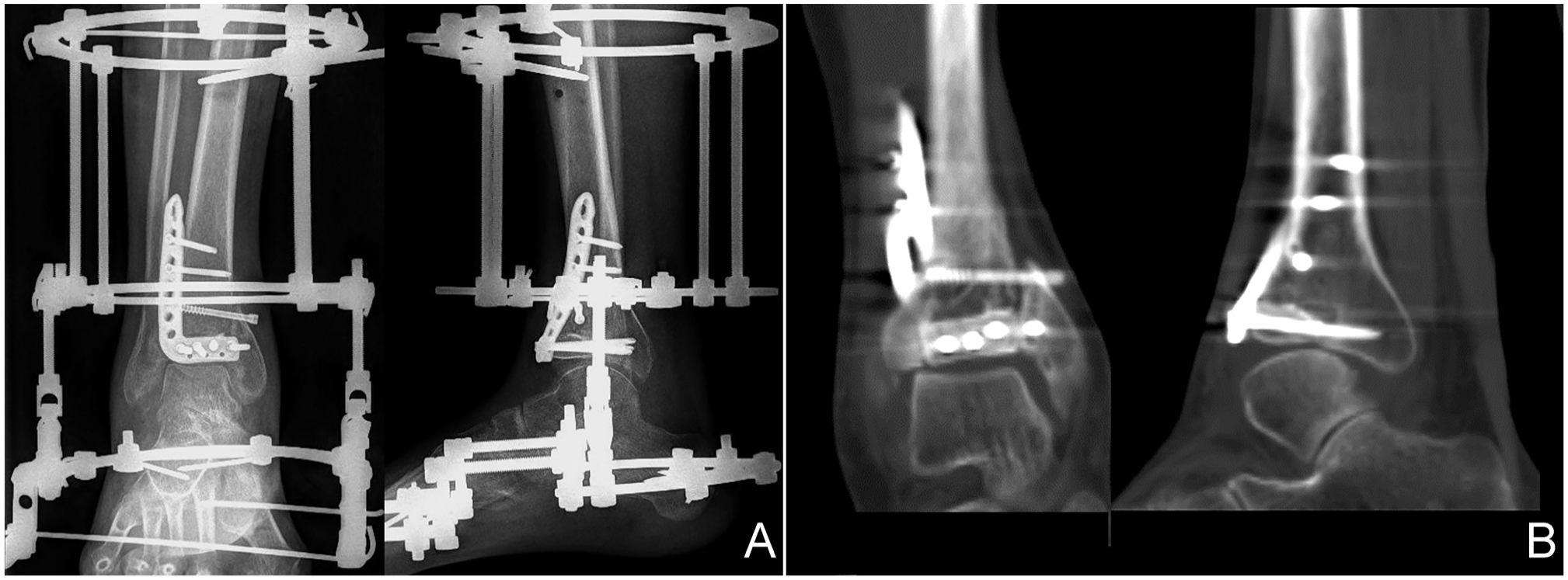
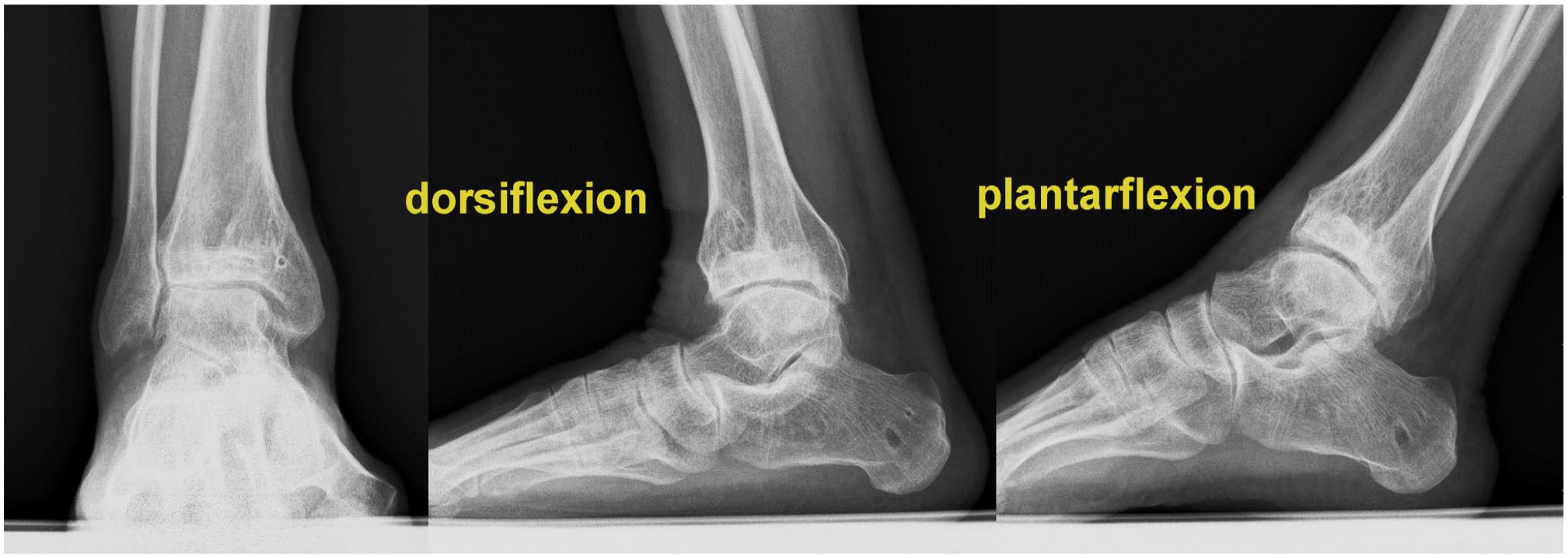
Patients were followed up for clinical and radiologic assessment at 1, 3, 6, and 12 months after the surgery and annually afterward. The American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot score, the visual analog scale (VAS), the 36-Item Short Form Health Survey (SF-36) score, and the ankle range of motion (ROM) were evaluated. Radiographic assessment was conducted, and the complications were recorded. The radiographs and CT images of the typical case at the end of follow-up are shown in Figure 3.
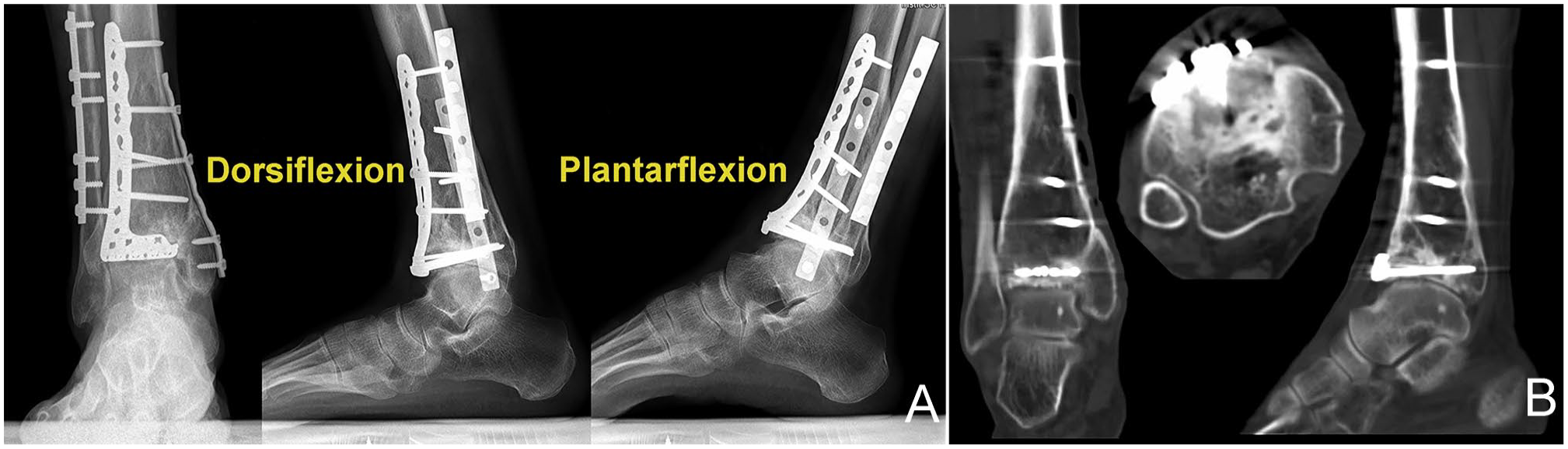
Postoperative radiologic images of case 3 at the 4.3-year final follow-up: (A) Weightbearing radiographs and (B) computed tomographic scans demonstrate a mildly painful arthritic change tibiotalar joint with reasonable range of motion and good osteointegration.
Statistical Analysis
Statistical analysis was performed using the R statistical software (version 3.5.3) with the paired 2-tailed t test in normally distributed data or the Wilcoxon t test in nonnormally distributed data to compare preoperative and postoperative parameters. Significance was assumed at P <.05.
Results
A total of 16 patients were included for analysis, including 13 men and 3 women with a mean age of 33.6 years. The type of initial fractures was classified as B2 in 1 ankle, B3 in 10, and C3 in 5 according to the AO/OTA classification, and 1 was type Ⅱ and 15 were type Ⅲ according to the Rüedi-Allgöwer classification. Five underwent nonoperative treatment, and 11 underwent suboptimal operations. The average time interval from the initial injury to the reconstructive operation was 12.3 (range, 2.5-25.0) months. The mean area of ilium blocks was 3.5 (range, 1.7-8.1) cm2. Apart from corrective intraarticular osteotomy and OPIAT, osteochondral autograft transplantation for talus was conducted in 4 patients and SMOT in 2 patients. Ankle distraction arthroplasty was performed in all patients, and the average time for external fixation was 94.1 days.
At a mean follow-up of 41.1 (range, 25.1-95.9) months, all patients achieved solid bony union and good osteointegration. The mean preoperative VAS, AOFAS, and SF-36 scores were 6.3, 47.6, and 38.0, respectively, and improved to 1.7, 84.4, and 70.8 at the final follow-up (P < .001 for each). The ankle ROM improved from 27.5 to 32.2 degrees (P = .023) (Table 2). Radiographs showed no significant progression of osteoarthritis in 15 patients according to the modified K&L score. The preoperative osteoarthritis stages were stage Ⅱ in 9 patients, stage Ⅲ in 7. Postoperatively they were stage Ⅱ in 13 patients, stage Ⅲ in 2, and stage Ⅳ in 1 patient. Two patients had pin site infections, and 2 presented with poor incisional healing, which recovered after local care, skin grafting, and dressing changes. Two patients developed severe ankle stiffness, and one of them developed considerable varus-type osteoarthritis but reported no pain. Two patients had mild persistent donor site pain. No patient presented deep surgical site infection, malunion, nonunion, or failure of internal fixation, and no secondary arthrodesis was needed during the final follow-up. Although most patients still had residual mild periodic pain after excessive use and did not acquire normal ROM, they believed that their daily activities improved compared with preoperation.
Details of the Surgeries and Outcomes.
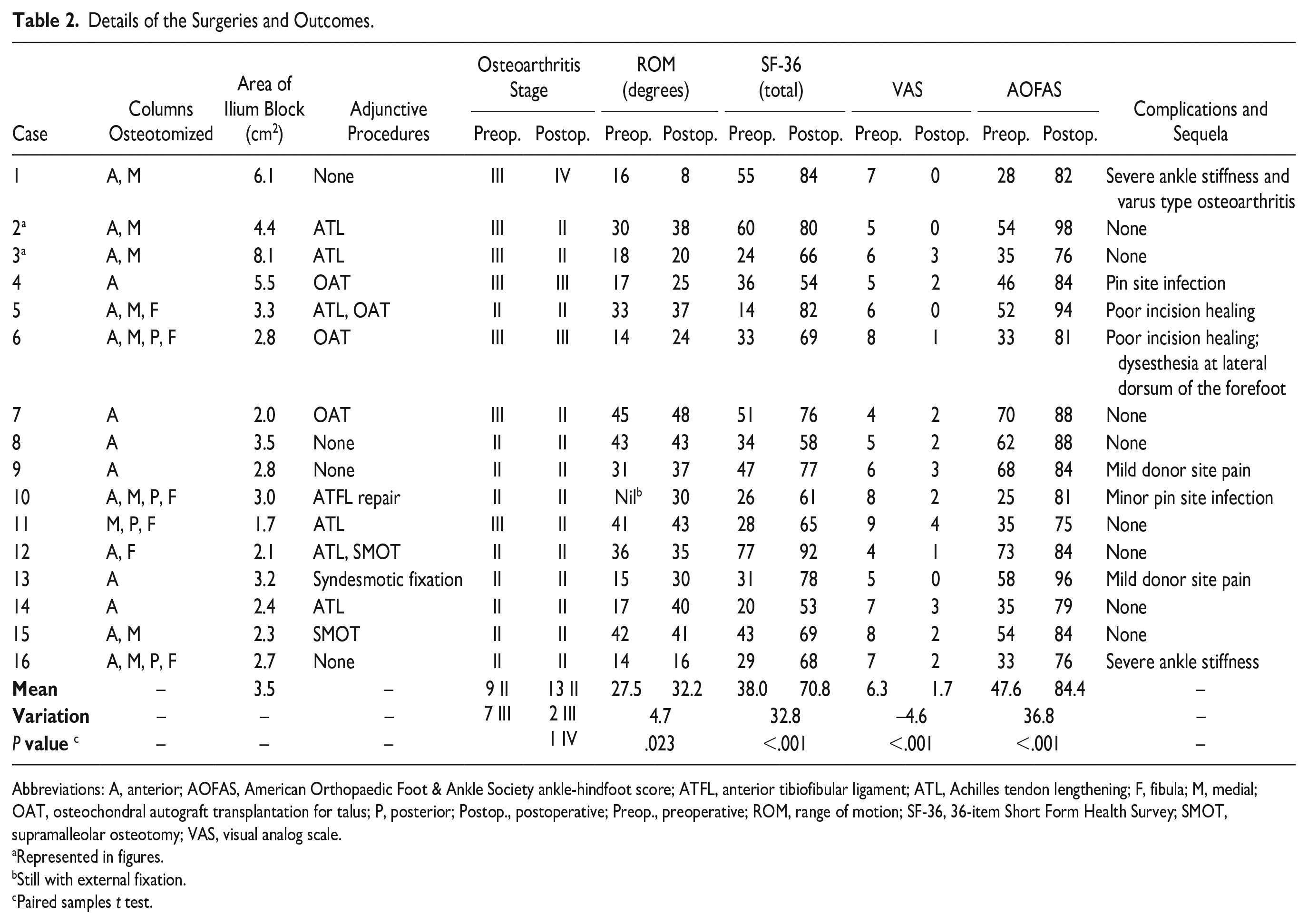
Abbreviations: A, anterior; AOFAS, American Orthopaedic Foot & Ankle Society ankle-hindfoot score; ATFL, anterior tibiofibular ligament; ATL, Achilles tendon lengthening; F, fibula; M, medial; OAT, osteochondral autograft transplantation for talus; P, posterior; Postop., postoperative; Preop., preoperative; ROM, range of motion; SF-36, 36-item Short Form Health Survey; SMOT, supramalleolar osteotomy; VAS, visual analog scale.
Represented in figures.
Still with external fixation.
Paired samples t test.
A second typical case (case 2) is as shown in Figures 4 to 7.

Preoperative plain radiographs and CT scans of a 26-year-old man (case 2 from the included table) with a malunited tibial plafond after a pilon fracture treated nonoperatively 8 months ago: (A) the anteroposterior and lateral view radiographs and (B) the coronal and sagittal view CT scans show a severe axially compressed plafond with a large-area osteochondral defect and an anterior subluxated talus. CT, computed tomography.
Postoperative plain radiographs and CT scans of case 2: (A) ankle distraction arthroplasty with circular Ilizarov external fixators; (B) the coronal and sagittal view CT scans show the resurfaced plafond and the graft in position. CT, computed tomography.

Postoperative radiologic images of case 2 at 4-year follow-up after removing the internal fixation devices: (A) weightbearing radiographs and (B) computed tomographic scans show a stage II osteoarthritic ankle according to the modified Kellgren and Lawrence score and good osteointegration.
Postoperative radiographs of case 2 at the 8-year final follow-up after the reconstructive surgery show a pain-free arthritic change tibiotalar joint with reasonable range of motion.
Discussion
We report our initial results with a method of articular reconstruction using periosteum-covered autologous ilium transplantation and intraarticular osteotomies for malunited pilon fractures with unreconstructable articular surfaces in young patients. At 3.4 years’ average follow-up, overall clinical and radiographic outcomes appeared fairly good. The ankle ROM increased on average about 20%, and the pain was reliably relieved. No secondary arthrodesis or replacement was needed during the follow-up.
We recommend ankle distraction arthroplasty as an auxiliary surgery for the following reasons: first, joint distraction theoretically improves the mechanical environment of the joint space,2,17,36 helping the survival of the grafted bone and the repair of the original cartilage; second, it helps to release the contracted soft tissue around the ankle, which is beneficial to maximize the ankle ROM; third, it allows early weightbearing and carrying out joint mobility rehabilitation training as soon as possible while avoiding the reconstructed articular collapsing again; fourth, intermittently immobilizing the ankle in a dorsiflexion position with an external fixator helps reduce equinus occurrence. 5
OPIAT can help salvage an unreconstructable articular surface with large-area cartilage loss and help prolong the survival of the tibiotalar joint. Success depends on proper patient selection, operative planning, and very likely the experience and skill of the surgeon. Patients should have realistic expectations for return to function following these procedures; the primary goal is reasonable to good pain relief and preservation or light increase in ankle ROM. Even if preservation of the ankle joint ultimately fails, reestablishing a well-aligned lower extremity with a congruent ankle joint may facilitate secondary fusion or replacement. 3
Tibial pilon fractures can be devastating injuries. Late complications, such as stiffness and posttraumatic osteoarthritis, correlate with the severity of the initial injury and the accuracy of reduction. 48 Malunions resulting from nonoperative treatment or inadequate operative reduction undoubtedly greatly increase the probability of these long-term complications. When the joint is irretrievable and the clinical symptoms are severe, arthrodesis and arthroplasty are frequently the mainstay procedures. However, tibiotalar arthrodesis is reported to be associated with ongoing gait changes, limitations on daily activities, and accelerated degeneration of the adjacent joints.10,27,35,47 And despite the promising prospects of ankle arthroplasty nowadays, the survival and complication rates still remain a concern, and it is currently not generally offered as an option to this particular patient population. 14 As for young active patients, the potential long-term complications of these ankle-sacrificing procedures are generally not well accepted by most patients. Nevertheless, young patients account for most of these types of injuries. Thus, other joint-preserving therapeutic modalities are required to resolve this dilemma.
Joint-preserving osteotomies for malunions of ankle fractures have been extensively discussed in the literature and the results were good.39,52 However, the appropriate joint-preserving strategy and patient selection for malunions of pilon fractures have rarely been reported in the literature.9,23,37,38,44 According to Rammelt et al, 38 young active patients with good bone stock, sufficient cartilage cover over the weightbearing areas (first- to second-degree chondromalacia), and good compliance with postoperative rehabilitation might be candidates for joint-preserving intraarticular osteotomies. Unfortunately, the condition of the cartilage cover over the weightbearing areas of the malunited tibial plafond is usually very poor in actual clinical settings due to prolonged periods of wear. Thus, how to properly resurface this kind of cartilage lesion is a very difficult clinical problem. We previously reported encouraging results from autologous osteochondral graft transplantation to repair the osteochondral defect in young patients with posttraumatic osteoarthritis following severe pilon fractures. 24 However, its adoption in this type of injury is restricted by concerns that the donor sites must be taken from a less weightbearing area of the knee joint and that the use of large grafts can cause substantial donor site morbidity.15,16,19,32 Alternatively there have been multiple reports about bipolar or unipolar fresh osteochondral allograft transplantation for the treatment of posttraumatic arthritis of tibiotalar joints and appears to be a viable option to arthrodesis or arthroplasty.3,12,30 However, the relatively low long-term survival rate, unsolved immunologic issues, and donor shortage must be taken into consideration. 13
The chondrogenic capacity of periosteum has been widely reported.7,8,18 In experimental animals, full-thickness cartilage defects of the patellofemoral joint have been treated with autologous periosteal grafts generating hyaline-like cartilage tissue.4,20,28,33,34,40 Clinical evidence also appears to parallel the experimental evidence.1,21,25 Remarkably, however, most of these cartilage lesions were at nonweightbearing areas and used free periosteal grafts. In recent years, there have been small reports of using osteoperiosteal autologous grafts to treat osteochondral lesions of the talus with surprisingly comparable results with osteochondral transplantation.6,45,53 In 2020, Li et al 22 reported using large autologous ilium with periosteum to manage severe acute pilon fractures with favorable short-term results. In our clinical experience, however, such large regions of unreconstructable articular surfaces are rarely seen in acute injuries, and large autologous ilium with periosteum grafts may be unnecessary in the majority of fresh pilon fractures. Conversely, this approach may be reserved for malunited pilon fractures where the articular surface is really difficult to reconstruct. Autologous ilium with periosteum transplantation, in these circumstances, may be considered for attempting to reconstruct what otherwise appears to be an unreconstructable articular surfaces. Notably, osteochondral lesions of the talus caused by protracted abnormal wear and supramalleolar deformity following unsatisfactory reduction of the metaphyseal area in malunited pilon fractures are not rare; in these cases, distal tibial realignment osteotomies and talar defect reconstruction may be beneficial.
The major weaknesses of the present study were the small sample size and the lack of a control group. Besides, macroscopic appearance through arthroscopy and histology examination of the repaired tissue were absent. In addition, the adjunctive procedures apart from OPIAT could be a cause of heterogeneity and bias. Thus, the good findings shall be interpreted cautiously, and further high-quality research is needed.
Conclusion
Osteoperiosteal iliac autograft transplantation might be an alternative surgical option for reconstructing malunited pilon fractures with large tibial plafond cartilage loss in young patients. Further studies with large samples and long-term follow-up are required to clarify this.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007231201823 – Supplemental material for Osteoperiosteal Iliac Autograft Transplantation for Unreconstructable Tibial Plafond After Malunions of Pilon Fractures in Young Patients
Supplemental material, sj-pdf-1-fai-10.1177_10711007231201823 for Osteoperiosteal Iliac Autograft Transplantation for Unreconstructable Tibial Plafond After Malunions of Pilon Fractures in Young Patients by Ting-Jiang Gan, Xi-Kun Ma, Ya-Xing Li, Yu Chen, Xi Liu, Jia Li and Hui Zhang in Foot & Ankle International
Footnotes
Ethical Approval
This study was performed in accordance with the Helsinki declaration of 1964, and it was approved by the relevant Institutional Review Board at the West China Hospital of Sichuan University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Sichuan Province of China (NO: 2022NSFSC0734).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.