
Abstract
Background:
A reliable landmark and precise distances from the ligament attachments are needed for lateral ankle stabilization surgery. The distal fascicle of the anterior inferior tibiofibular ligament (AITFL) has been used to locate the anterior talofibular ligament (ATFL) or calcaneofibular ligament (CFL) centers on the fibula. However, there is no anatomic study to validate the distal fascicle of the AITFL as a landmark of lateral ankle ligament stabilization, and more importantly, the exact distances from the ATFL or CFL attachments to the distal fascicle of the AITFL are unknown.
Methods:
Sixteen frozen cadaveric specimens (8 paired specimens) with no previous history of ankle injury were used in this study. Whether the distal fascicle of AITFL was present in each specimen was confirmed. Then, the distances from the most distal insertion of the AITFL’s distal fascicle to the footprint centers of the ATFL and CFL on the fibula were measured. All measurements were performed by 2 observers, and the intraobserver and interobserver reliabilities were analyzed by intraclass correlation coefficients (ICCs).
Results:
The distal fascicle of the AITFL was found in all specimens (100%). The mean distance from the most distal insertion of the AITFL’s distal fascicle to the footprint centers of the ATFL, CFL, and the intersection center of the 2 ligaments on the fibula was 6.0 to 7.1 mm, 11.5 to 13.2 mm, and 9.0 to 10.0 mm, respectively. Excellent interobserver and intraobserver agreement (all ICCs > 0.9, P < .01) was shown in the anatomic measurements of these distances.
Conclusion:
In this cadaveric study, we found that the distal fascicle was a constant structure of the AITFL in the lateral ankle. The distances from the most distal insertion of the AITFL’s distal fascicle to the ligamentous footprint centers were reliable and may be used to identify the origins of the ATFL and CFL for lateral ankle ligament reconstruction.
Clinical Relevance:
This anatomic study validates the AITFL’s distal fascicle as a potential landmark and, more importantly, determines the range of distances from AITFL’s distal fascicle to the attachment centers of lateral ankle ligaments by anatomic measurements. The data may be used to identify the ATFL and CFL for lateral ankle stabilization surgery and become particularly valuable for endoscopic or arthroscopic techniques.
Introduction
The anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL) are 2 main structures that stabilize the lateral ankle.11,15 Patients with ATFL and CFL injuries who fail conservative treatment are likely to develop chronic lateral ankle instability (CLAI), and surgical management may be required after failed nonoperative treatment. 7 Anatomic repair or reconstruction with open or arthroscopic procedures with favorable outcomes relies on accurate locations of suture anchors or osseous tunnels.3,20 Ligament injuries are likely to occur at the fibular side. 18 Therefore, reliable landmarks and their precise distances from the ATFL and CFL centers on the fibula are needed.
The obscure tubercle of the fibula is reported to be found in all specimens in a cadaveric anatomic study and is a reliable bony landmark for percutaneous minimally invasive surgery. 23 Nevertheless, when osteophytes and scar tissue hide this bony landmark or when avulsion fracture of the obscure tubercle occurs 32 (Figure 1), accurately locating the insertion centers of ligaments becomes challenging. In such cases, an alternative landmark is essential. The distal fascicle of the anterior inferior tibiofibular ligament (AITFL) is easily found under ankle arthroscopy and open vision,6,16 with an incidence of 21% to 92%. 29 Previously, Vega et al 30 located the anchor on the fibular attachment of the AITFL to reproduce the native insertion of the ATFL. Lan et al 19 also used the distal fascicle of the AITFL to locate the fibular tunnel when the remnant tissue of the ATFL could not be found. Indeed, the distal fascicle has good potential to be an anatomic landmark to identify ligamentous attachments during surgery, particularly during arthroscopic procedures. 23 However, there is no anatomic study to validate the distal fascicle of the AITFL as a landmark of lateral ankle ligament stabilization, and more importantly, the exact distances from the ATFL or CFL attachments to the distal fascicle of the AITFL are unknown.
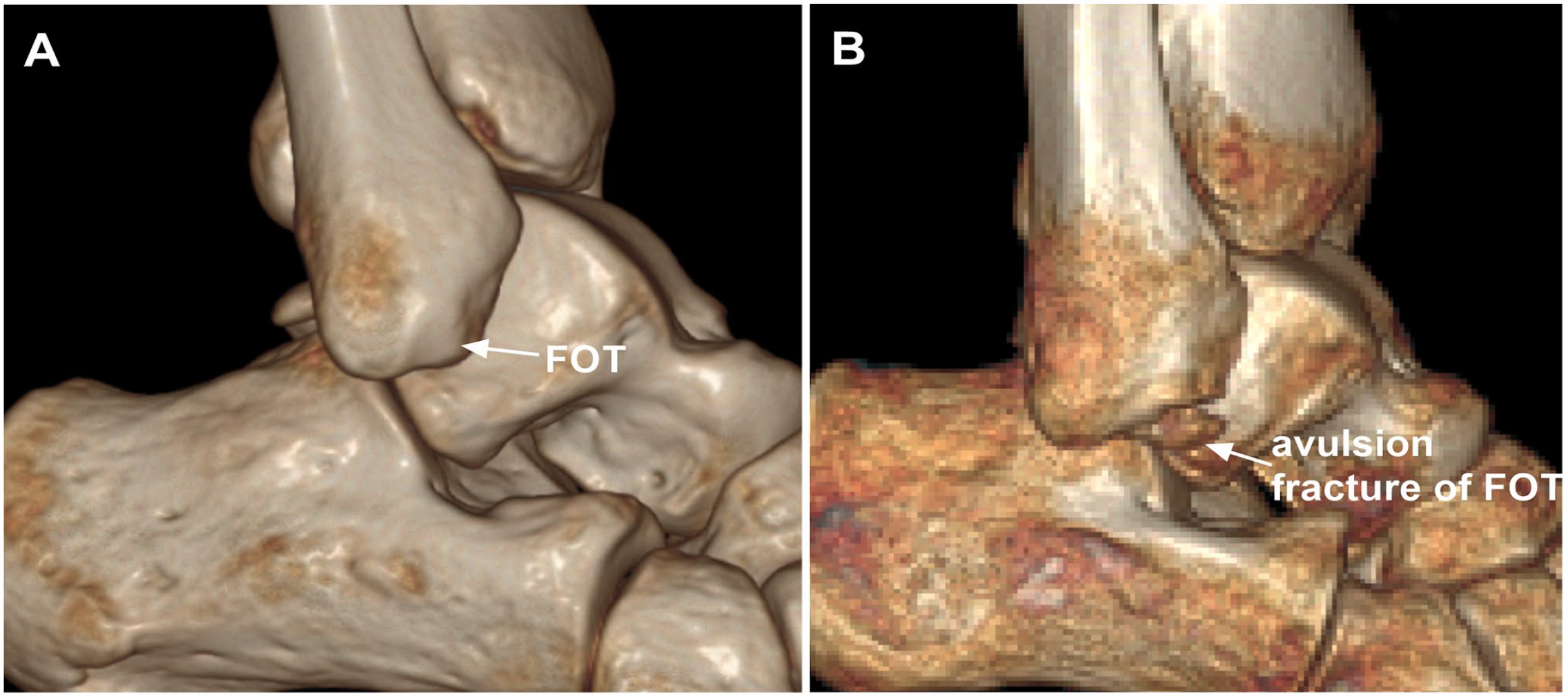
(A) The location of fibular obscure tubercle. (B) The avulsion of FOT. FOT, fibular obscure tubercle.
The purpose of this study was to determine the detectability of the distal fascicle of the AITFL and to measure the distances from the most distal insertion of the AITFL’s distal fascicle to the attachment centers of the ATFL or CFL on the fibula. This study hypothesizes that the distal fascicle of the AITFL could be used as a landmark for lateral ankle stabilization. The results of this study can provide quantitative data for identifying ligamentous centers when anatomic repair or reconstruction is performed using the landmark of the distal fascicle of the AITFL.
Materials and Methods
Cadavers
This study was approved by the Institutional Ethics Committee (M2021566). Sixteen frozen cadaveric specimens (8 paired specimens) with no previous history of ankle injury were used in this study. Three of the specimens were male, and 5 were female. The mean age was 65 ± 8.3 years. Magnetic resonance imaging (MRI) was performed in all specimens to exclude lateral ankle ligament injury. After carefully dissecting all overlying soft tissues, the distal fascicle of the AITFL and the footprint centers of the ATFL and CFL were identified. In addition, the intersection point of the ATFL and CFL (intATFL-CFL) in the fibula was identified by minimal dissection of the most inferior and posterior fibers of the ATFL and the most anterior fiber of the CFL (Figure 2). 24 Two observers performed all measurements to calculate the intraclass correlation coefficients (ICCs). Each observer measured the distances using a caliper 3 times to calculate the mean values.
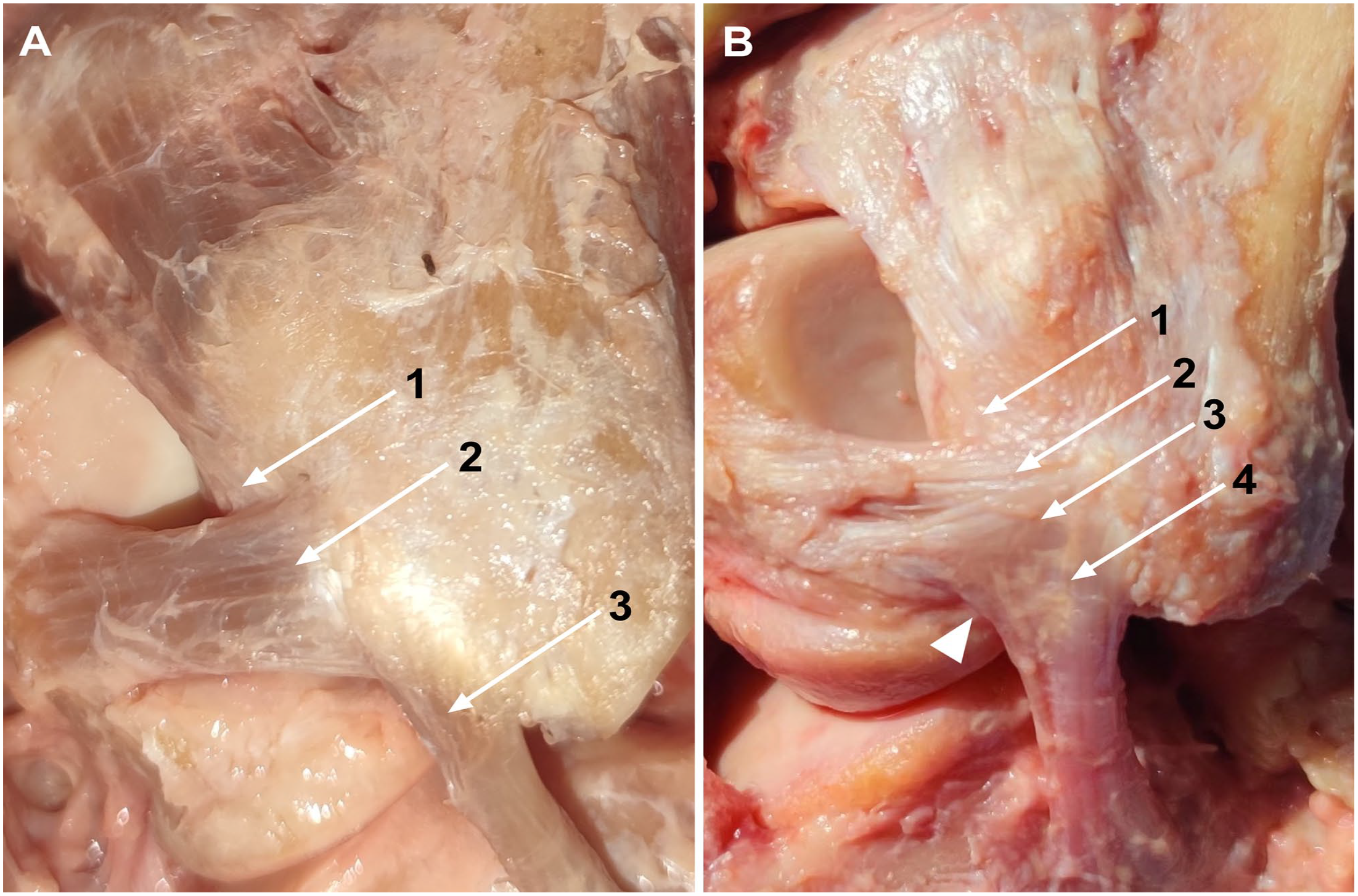
Lateral view of AITFL, ATFL, and CFL in a left ankle. (A) 1, The insertion of the distal fascicle of AITFL on the fibula; 2, ATFL, 3, CFL. (B) 1, The most insertion of the distal fascicle of the AITFL on the fibula; 2, superior fascicle of the ATFL; 3, inferior fascicle of the ATFL; 4, CFL; arrowhead, arciform fibers connecting the inferior fascicle of the ATFL and CFL. AITFL, anterior inferior tibiofibular ligament; ATFL, anterior talofibular ligament; CFL, calcaneofibular ligament.
Measurements
The distance from the most distal insertion of the AITFL’s distal fascicle to the footprint center of the ATFL on the fibula.
The distance from the most distal insertion of the AITFL’s distal fascicle to the footprint center of the CFL on the fibula.
The distance from the most distal insertion of the AITFL’s distal fascicle to the intersection point of the ATFL and CFL on the fibula is shown in Figure 3.
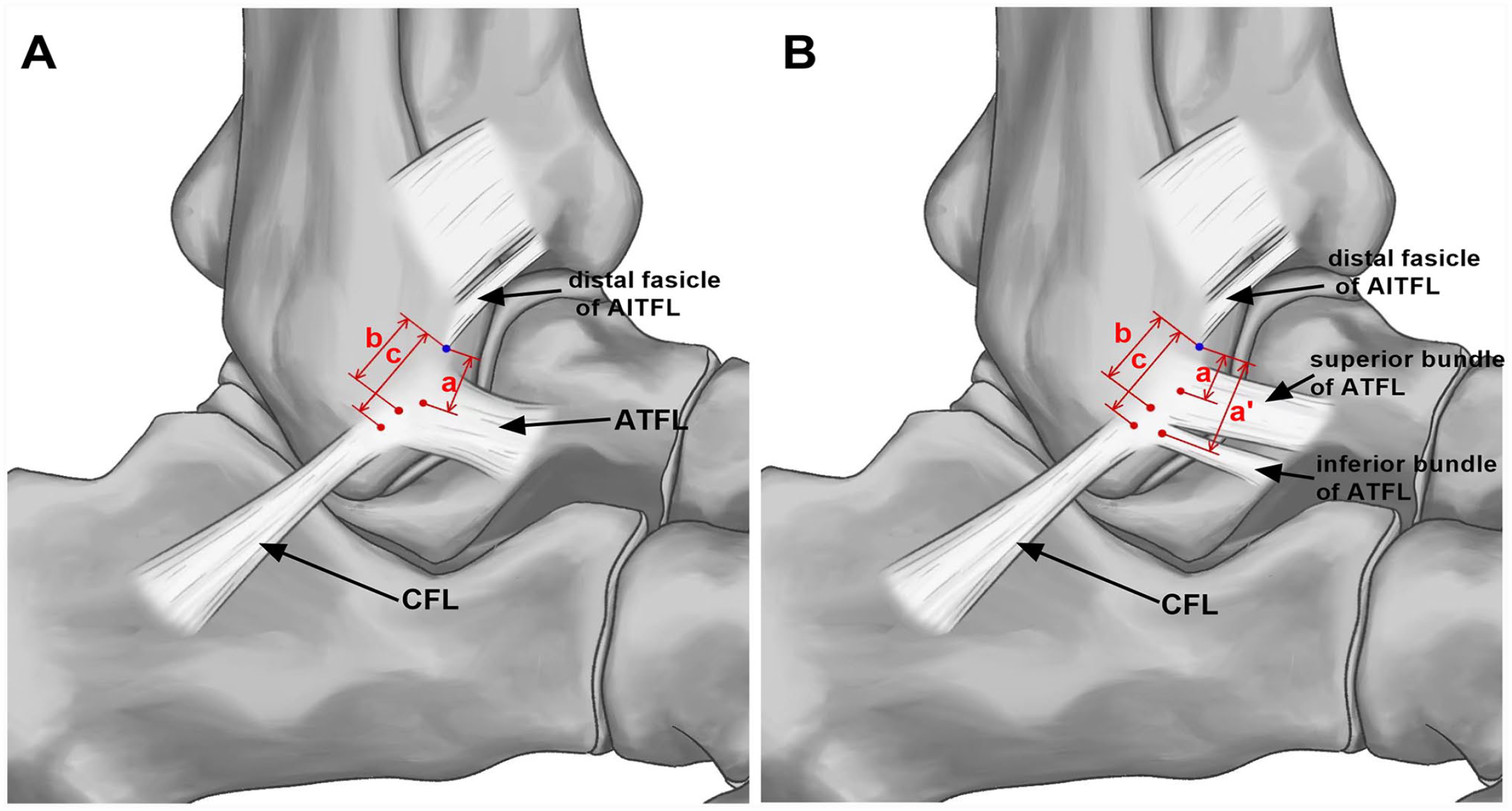
Illustration of anatomic measurements. (A) The measurements in the ATFL with a single bundle: a, b, and c represent the distance from the most distal insertion of the AITFL’s distal fascicle (blue point) to the footprint center of the ATFL (7.1 mm), the intersection point of the ATFL and CFL (10.0 mm), and the footprint center of the CFL (11.5 mm). (B) The measurements in the ATFL with 2 bundles: a, a', b, and c represent the distance from the most distal insertion of the AITFL’s distal fascicle (blue point) to the footprint center of the superior bundle of the ATFL (6.0 mm), the footprint center of the inferior bundle of the ATFL (12.8 mm), the intersection point of the ATFL and CFL (9.0 mm), and the footprint center of the CFL (13.2 mm). AITFL, anterior inferior tibiofibular ligament; ATFL, anterior talofibular ligament; CFL, calcaneofibular ligament. [See online article for color figure.]
Statistical Analysis
Distances between ligamentous attachments and the most distal insertion of the AITFL’s distal fascicle on the fibula were reported as the means ± SDs. Interobserver and intraobserver reliabilities for all anatomic measurements were analyzed using the intraclass correlation coefficient (ICC) and 95% CI. All statistical analyses were performed using the Statistical Package for the Social Science (SPSS 25.0, IBM) software. Statistical significance was established at P <.05.
Results
The distal fascicle of AITFL was found in all (100%) specimens. The ATFL was observed with a single bundle structure in 8 of 16 (50%) ankle specimens and with 2 bundles in the remaining 8 of 16 (50%) ankles. The mean distance from the most distal insertion of the AITFL’s distal fascicle to the footprint center of the ATFL on the fibula was 6.0 to 7.1 mm. The mean distance from the most distal insertion of the AITFL’s distal fascicle to the footprint center of the CFL was 9.0 to 10.0 mm on the fibula, which varied with different bundles of the ATFL. The distance from the most distal insertion of the AITFL’s distal fascicle to the intersectional center of the ATFL and CFL on the fibula was 11.5 to 13.2 mm, which also varied with different bundles of the ATFL (Table 1).
Anatomic Measurements From the Insertion of the Most Distal Insertion of the AITFL's Distal Fascicle to the Ligamentous Attachments.
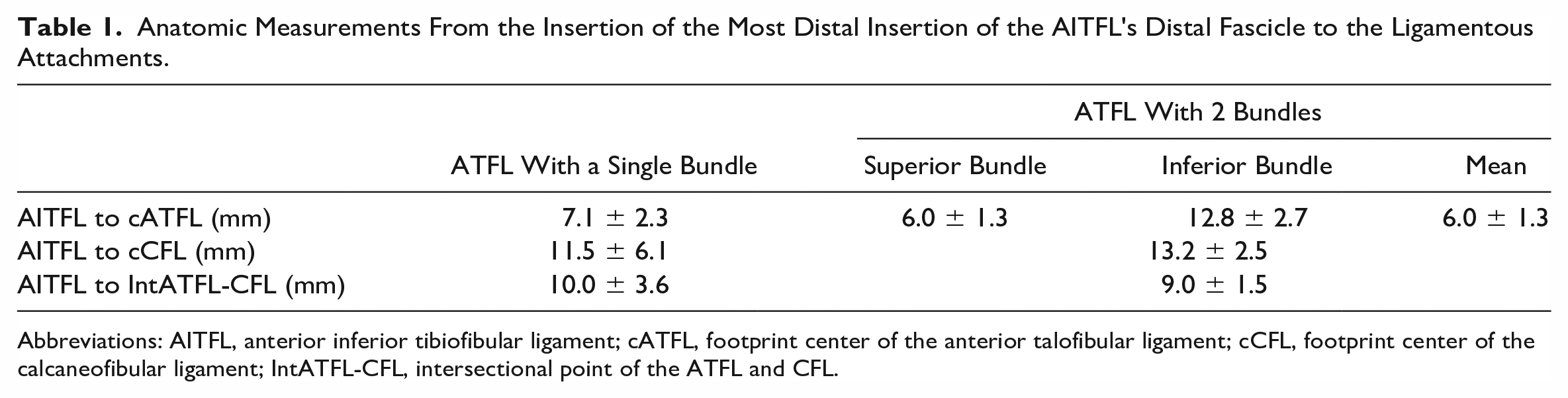
Abbreviations: AITFL, anterior inferior tibiofibular ligament; cATFL, footprint center of the anterior talofibular ligament; cCFL, footprint center of the calcaneofibular ligament; IntATFL-CFL, intersectional point of the ATFL and CFL.
Excellent interobserver and intraobserver agreement (all ICCs > 0.9, P < .01) was shown in the anatomic measurements of distance from the most distal insertion of the AITFL’s distal fascicle to the ligamentous attachment centers (Tables 2 and 3).
Interobserver Reliability of Anatomic Measurements.
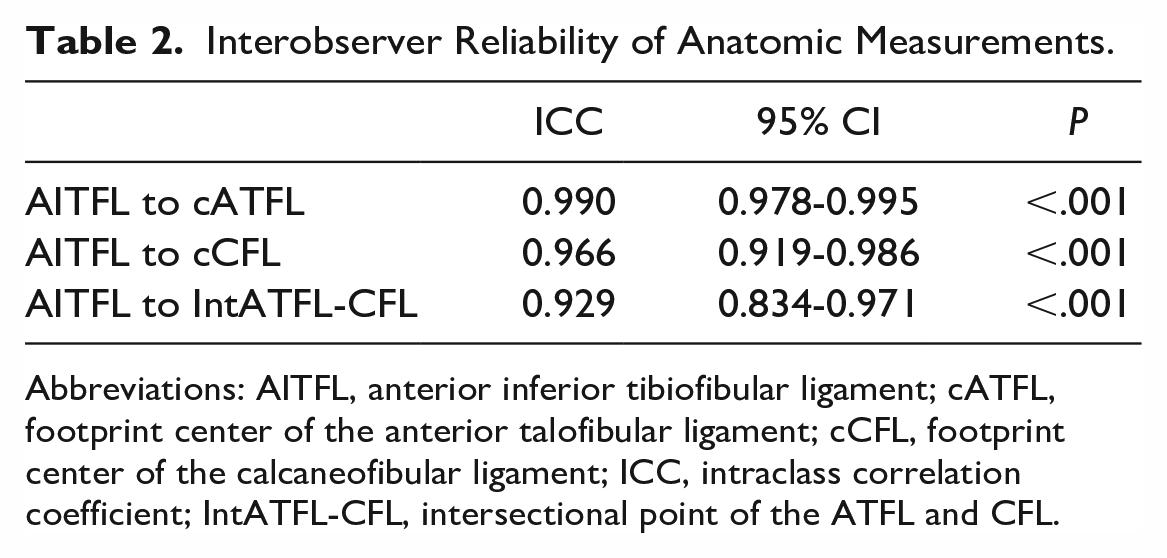
Abbreviations: AITFL, anterior inferior tibiofibular ligament; cATFL, footprint center of the anterior talofibular ligament; cCFL, footprint center of the calcaneofibular ligament; ICC, intraclass correlation coefficient; IntATFL-CFL, intersectional point of the ATFL and CFL.
Intraobserver Reliability of Anatomic Measurements.
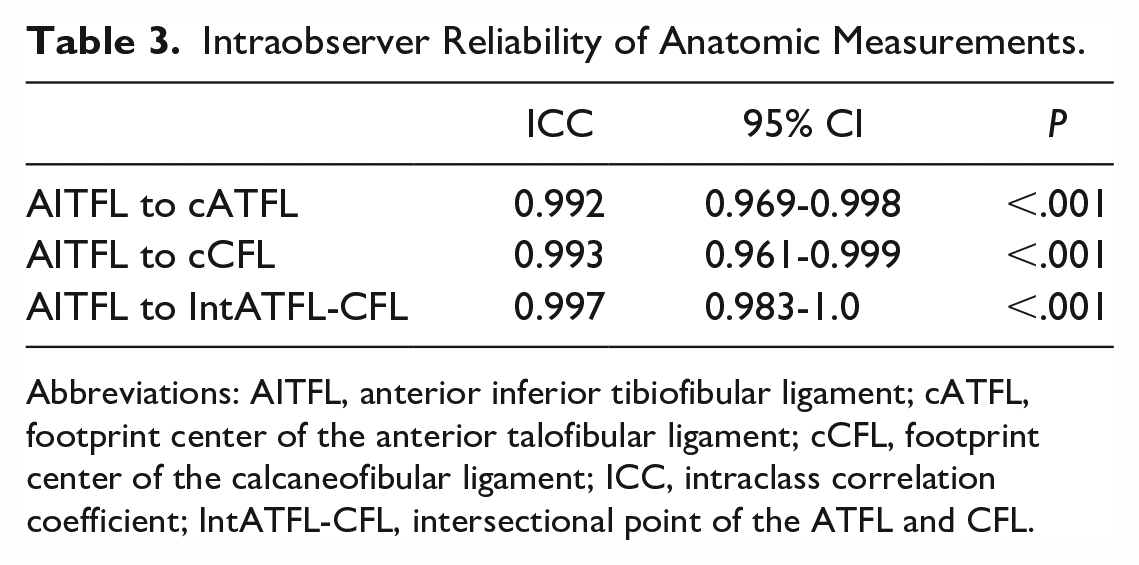
Abbreviations: AITFL, anterior inferior tibiofibular ligament; cATFL, footprint center of the anterior talofibular ligament; cCFL, footprint center of the calcaneofibular ligament; ICC, intraclass correlation coefficient; IntATFL-CFL, intersectional point of the ATFL and CFL.
Discussion
The main findings of this study were that the presence of the distal fascicle of the AITFL in all specimens, and the exact distances from the most distal insertion of the AITFL’s distal fascicle to the footprint centers of the ATFL and CFL on the fibula. The results validated that the distal fascicle of the AITFL had potential to be used as a landmark for lateral ankle ligament stabilization.
The distal fascicle of AITFL was found in all (100%) specimens. Previously, the incidence of distal fascicle of AITFL was reported to differ in different studies, which probably resulted from different definitions. 29 However, recent studies have revealed that the distal fascicle is a constant part of AITFL,5,9 which was the same as the result in our study. The AITFL originates from the tibia, runs obliquely in an inferolateral direction and attaches to the fibula,1,11 which is divided into several bundles, and the distal fascicle appears to be an independent intraarticular structure.5,9,11 The ATFL attaches just below the fibular insertion of the distal fascicle of the AITFL.8,9 Some authors have transferred AITFL’s distal fascicle to reconstruct ankle stability.16,28,31 Therefore, the distal fascicle of the AITFL and ATFL are in close proximity in open or arthroscopic views.6,16,31 The anatomic feature allows the distal fascicle of the AITFL to be used as an alternative anatomic landmark to locate the ATFL and CFL, particularly under the arthroscopic view.
The mean distance from the most distal insertion of the AITFL’s distal fascicle to the footprint center of the ATFL (6.0-7.1 mm), the CFL (11.5-13.2 mm), and the intersection of the ATFL and CFL (9.0-10.0 mm) on the fibula were measured. The modified Brostrom procedure is still the gold standard to repair injured ligaments.10,21,33,35 For poor quality or absence of residual ligament, anatomic reconstruction using a free tendon is reported by Takao et al 26 and Guillo et al,12-14 in which a common osseous tunnel in the fibula is created. Anatomic repair or reconstruction requires precise knowledge of the anatomic attachments of the ATFL and CFL on the fibula, including the intersectional attachments of the ATFL and CFL. Lan et al 19 described a distance of 5 to 7 mm from the distal fascicle of the AITFL to locate the fibular tunnel in lateral ankle ligament reconstruction. The anatomic measurements in this study indicated that the tunnel locations might be slightly lower than which described by Lan et al. Bony landmarks, such as the inferior tip of the fibula and fibular obscure tubercle, have been widely used in anatomical studies to assess the fibular insertions of the ATFL and CFL. The distance from ligamentous attachments to the inferior tip of the fibula varied in the literature,2,4,17,24,25,27,34 whereas the fibular obscure tubercle was available and reliable for identifying the attachments of the ATFL and CFL. 23 Using the distal fascicle of the AITFL, the locations of the ATFL and CFL corresponded with the fibular obscure tubercle.
Limitations
First, the sample size in this study is relatively small, and the heterogeneity of specimens may influence the results. Second, only Chinese or Asian specimens were included in this study, and the distance measurements may be different in different races. In addition, the older age of the specimens may also be a source of bias. 22 Finally, and potentially clinically relevant was that in this group of specimens we always were able to identify the distal fascicle of the AITFL as a landmark for measurement. In clinical practice, some patients may have had previous injury to the AITFL with resultant loss or scarring around this potential landmark. For that reason, this approach may have clinical limitations.
Conclusion
In our cadaver study, we found the distal fascicle to be a constant structure of the AITFL in the lateral ankle. The precise distances from the most distal insertion of the AITFL's distal fascicle to the ligamentous footprint centers are reported. We hope these values can help surgeons identify the ATFL and CFL origin locations for lateral ankle stabilization surgery, which may be especially helpful for endoscopic, arthroscopic approaches or when previous scarring, osteophytes or avulsion fractures obscure other anatomical landmarks.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007231201343 – Supplemental material for The Distal Fascicle of the Anterior Inferior Tibiofibular Ligament: A Potential Landmark for Lateral Ankle Ligament Reconstruction
Supplemental material, sj-pdf-1-fai-10.1177_10711007231201343 for The Distal Fascicle of the Anterior Inferior Tibiofibular Ligament: A Potential Landmark for Lateral Ankle Ligament Reconstruction by Anhong Wang, Feng Zhao, Weili Shi, Chenyu Lian, Xing Xie, Lizhong Jing, Ziming Liu, Keying Zhang, Dong Jiang and Qinwei Guo in Foot & Ankle International
Footnotes
Ethical Approval
This work was approved by the Institutional Review Board in Peking University Third Hospital (M2021566).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Key Clinical Project (Grant No. BYSY2018011) of Peking University Third Hospital.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.