
Abstract
Background:
The purpose of this article was to report the feasibility and effectiveness of 3-stage Masquelet technique and 1-stage operation for different stages of foot and ankle tuberculosis (TB).
Methods:
Ten consecutive patients with foot and ankle TB were retrospectively analyzed between January 2014 and December 2018. Five patients were treated with the 3-stage Masquelet technique, including thorough debridement with vacuum sealing drainage, implantation of antibiotic cement spacer, and subsequent reconstruction. Five patients were treated with a 1-stage reconstruction. The American Orthopaedic Foot & Ankle Society (AOFAS) and visual analog scale (VAS) pain scores were recorded at the last follow-up. The follow-up was 30.3 ± 17.8 months.
Results:
No reactivation of TB was observed in any patients. For the 3-stage operation group, 1 patient developed a distal tibia fracture. The duration of anti-TB therapy was 12.0 ± 0.8 months. The AOFAS score increased from 39.5 ± 9.9 preoperatively to 75.3 ± 7.0 postoperatively (P < .05). The VAS pain score decreased from 6.3 ± 1.9 to 1.5 ± 1.3 (P < .05). For the 1-stage operation, 1 patient had wound necrosis. The duration of anti-TB therapy was 13.8 ± 1.1 months. The AOFAS score increased from 51.8 ± 15.0 to 81.8 ± 6.3 (P < .05). The VAS pain score decreased from 5.4 ± 1.1 to 1.0 ± 0.7 (P < .05).
Conclusion:
Three-stage operation was effective for foot and ankle TB with stage IV, sinus tracts or other infections, and 1-stage reconstruction was effective for early-stage TBs.
Level of Evidence:
Level IV, case series.
Introduction
Although patients infected with tuberculosis (TB) are primarily encountered in developing countries, current trends of globalization have led to TB being the deadliest infectious disease worldwide, with 1.6 million deaths yearly. 30 The TB incidence was 2.8 per 100 000 persons in 2018 in the United States, of which musculoskeletal TB consistently accounted for 2% to 3%.18,27 However, foot and ankle TB, a rare disease, accounting for 5% of musculoskeletal TB in Los Angeles County and less than 1% of musculoskeletal TB in developing countries, induces severe dysfunction and economic burden.7,8,9,18 It is important that orthopedic surgeons know how to properly address this rare but complicated and debilitating disease.
Tuberculosis in the foot and ankle is a chronic disease that is often secondary to TB elsewhere in the body, especially in the lungs, including synovial TB, bone TB, and panarthrosis. It develops gradually and is characterized by deteriorating joints, pain with mild fever, inflammation of the joint, and even cold abscesses combined with sinus tracts in late stage. Patients with foot and ankle TB usually complain of pain, swelling, and movement limitation in involved bones and joints. Sometimes sinus tracts disappear, often accompanying infection with complicating bacteria. In addition, pathologic fracture may occur. Fever, weight loss, and other local symptoms are rare.15,29 Imaging findings include osteoporosis, soft tissue swelling, joint space narrowing, and bone invasion. The diagnosis of foot and ankle TB is based on clinical examination, radiographic findings, and representative tissue obtained for histopathologic and microbiological analyses. Biopsy yields the definitive diagnosis of TB. 12 However, because of atypical symptoms and nonspecific imaging findings in bone and joint TB, the diagnosis can be difficult, and foot and ankle TB may be misdiagnosed as other infectious diseases.3,5
Long-term antituberculosis drugs are the basic treatment for tuberculosis in the foot and ankle. Single antituberculosis treatment (ATT) is effective in the early stage, as Karkhur reported. 14 Operative treatment includes biopsy and, for cases that were not diagnosed clearly, debridement and arthrodesis. If obvious destruction and pain persist around the foot and ankle joints, arthrodesis can be used to achieve a stable and painless foot. Operative treatment can shorten the anti-TB drug usage period and improve prognosis. 1 In Chen et al’s study, 3 a 1-stage operation, including debridement, biopsy, synovectomy, and arthrodesis, was performed for 29 patients based on radiologic staging in which 22 patients achieved excellent or good outcomes. However, in the presence of a combination of other infections, debridement only and arthrodesis with antituberculosis drugs works poorly for controlling mixed infections that continue to destroy the soft tissue. 6 In addition, implants in the absence of controlled infection can increase the rates of infection, inducing fixation failure. Indeed, skin flap transplantation and external fixation are reported as effective methods to address complicated mixed infections and soft tissue injury.6,28 Currently, foot and ankle TB is seldom discussed in the literature, and there are no detailed operative guidelines.
Since Masquelet presented the concept of “induced membrane” and applied the induced membrane technique (Masquelet technique), the 2-stage Masquelet technique has been used for long bone defects, even infected long bone defects and nonunion, achieving satisfactory efficacy.22,23,25,31 Zou et al 35 recently reported that in contrast to 1-stage treatment, arthrodesis with bone grafting can be performed after complete elimination of infection in the midfoot. However, their cases contained major TB infection in the midfoot. Attempting to control TB mixed with other infections more effectively, the 3-stage Masquelet technique (debridement with vacuum sealing drainage [VSD], implantation of antibiotic cement spacer, and subsequent reconstruction) was applied for TB of foot and ankle with sinus tracts. In addition, in terms of different stages of TB in the foot and ankle, 1-stage operation was also performed for relatively early stages of TB.
By retrospective case study, we collected data from 5 cases with destructive TB in the foot and ankle (4 cases with sinus tracts) treated with 3-stage operation and 5 cases with no sinus treated with 1-stage operation in our department to evaluate our experiences of the feasibility and effectiveness of the treatments.
Methods
Between January 2014 and December 2018, 10 patients who were diagnosed with foot and ankle TB were enrolled in this study. This study was conducted with approval from the Medical Ethics Committee. Tuberculosis protein chip tests were performed in 9 patients. All patients had their erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) checked preoperatively. All patients underwent a chest X-ray or computed tomography (CT) examination. Plain film, CT, and magnetic resonance imaging (MRI) of the foot and ankle were taken regularly preoperatively (Figure 1, C-E). Five patients with stage IV TB were treated by 3-stage Masquelet technique, and 1 patient with stage II, 3 patients with stage III, and 1 with stage IV were treated with 1-stage operation (the score relied on X-ray or CT images with reference to Zou et al 35 ).
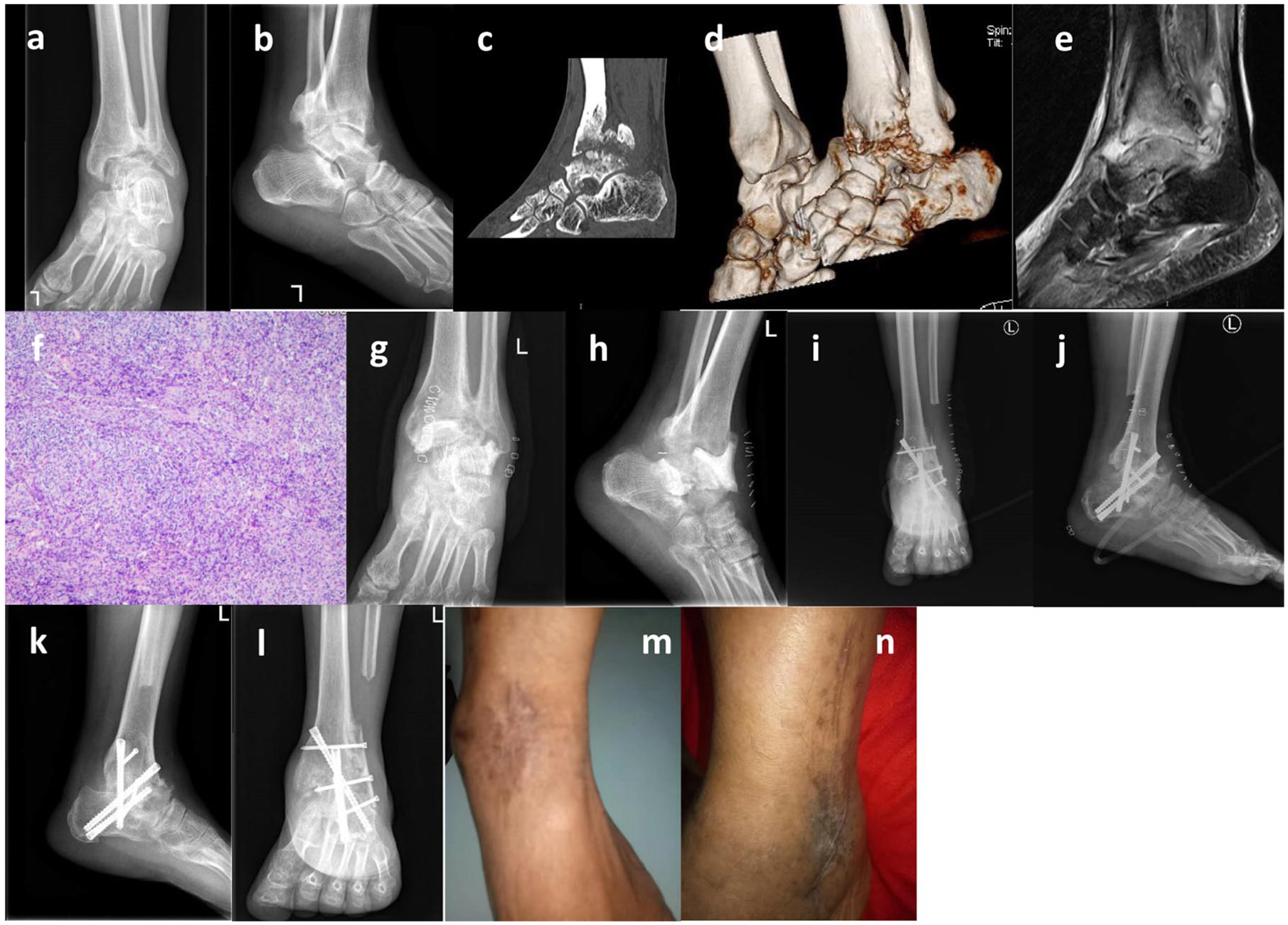
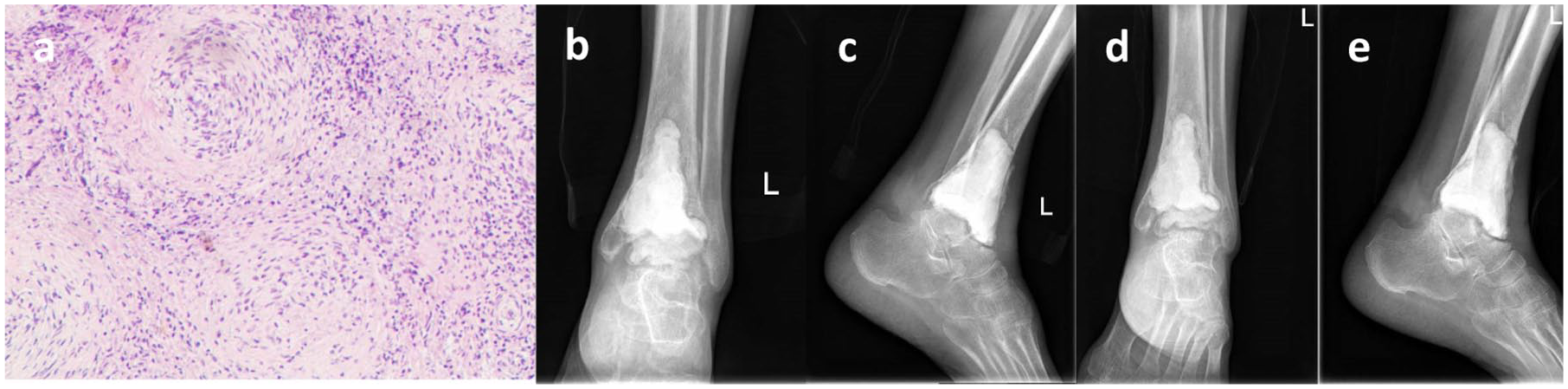
A 50-year-old man who had suffered pain and deformity of the left ankle for 4 months before treatment received 3-stage Masquelet operation. (A, B) Preoperative radiographs showing the destructive talus and distal tibia. (C, D) Preoperative computed tomographic scan and 3-dimensional reconstruction. (E) Preoperative T2 sequence of magnetic resonance imaging showing the long signal of the ankle. (F) Histopathology at the first surgery showing granulomatous inflammation and pyogenic inflammation, which demonstrated tuberculosis. (G, H) Radiographs taken after the second-stage operation receiving the implant of antibiotic bone cement. (I, J) Instant radiographs taken after the removal of bone cement and bone reconstruction. (K, L) Radiographs taken 6 months after the third-stage operation showing good bone union of fusion. (M, N) Appearance of the left ankle 1 year after the last surgery showing that the ankle is satisfactorily repaired without swelling or sinus.
Operative Methods
For the 3-stage Masquelet technique (flow diagram is shown in Figure 2), at the first stage, a medial incision, lateral incision, or combined incision was used to expose the talus and ankle joint or its surrounding joints and eliminate TB-infected tissue. Any articular surface involving TB, surrounding skin, and soft tissue of the sinus tract was removed until normal tissue was exposed. TB-infected tissue was sent for bacterial and pathologic examination. Diluted povidone-iodine solution, normal saline, hydrogen peroxide, and normal saline were used to clean the wound repeatedly. Subsequently, sparse suture and VSD were performed to irrigate and aspirate the wounds. If the ankle and nearby joints were severely destroyed, the ankle could be fixed in a neutral position by external fixation. Sometimes, the first stage could be repeated if the mixed infection was controlled poorly until there was a clean wound, negative bacterial culture, and continuous decrease or nearly normal level of inflammatory indicators such as ESR and CRP. At the second stage (Table 1), approximately 7 days after the first stage, the same debridement procedure was performed except that the final VSD was replaced by a drainage tube or continued usage of VSD according to the wound condition. In addition, before suture, the defective bone tissue was filled with antibiotic cement spacer. In total, 1.0 g vancomycin and 2.0 g streptomycin were mixed into 40 g moderate- or high-viscosity cement. Enough bone cement was used to cover the cavity but protrude slightly beyond the bone for the sake of suturing. Normal longitudinal arch height was restored and fixed by multiple K-wires in the cases with collapsed arch. External fixator ora brace was used while the ankle was placed in a neutral position postoperatively. The third-stage operation (Table 2) was performed at least 3 months after the second operation until ESR and CRP were both normal, and all the symptoms were under control. Arthrodesis of the tibiotalar joint and/or subtalar joint, even triple or quadruple arthrodesis, was used. A lateral incision on the ankle or the original incisions were selected. After the bone cement was completely removed, there was a large bone cavity left. Autologous iliac and/or homolateral fibula grafts were harvested and cut into suitable sizes to implant into the bone cavity. After the anatomy and force line of the ankle or foot were restored, K-wires were used to temporarily stabilize the bone sites. If the alignment was satisfactory according to fluoroscopic monitoring, cannulated screws and lag screws or locking plates were used for rigid fixation.
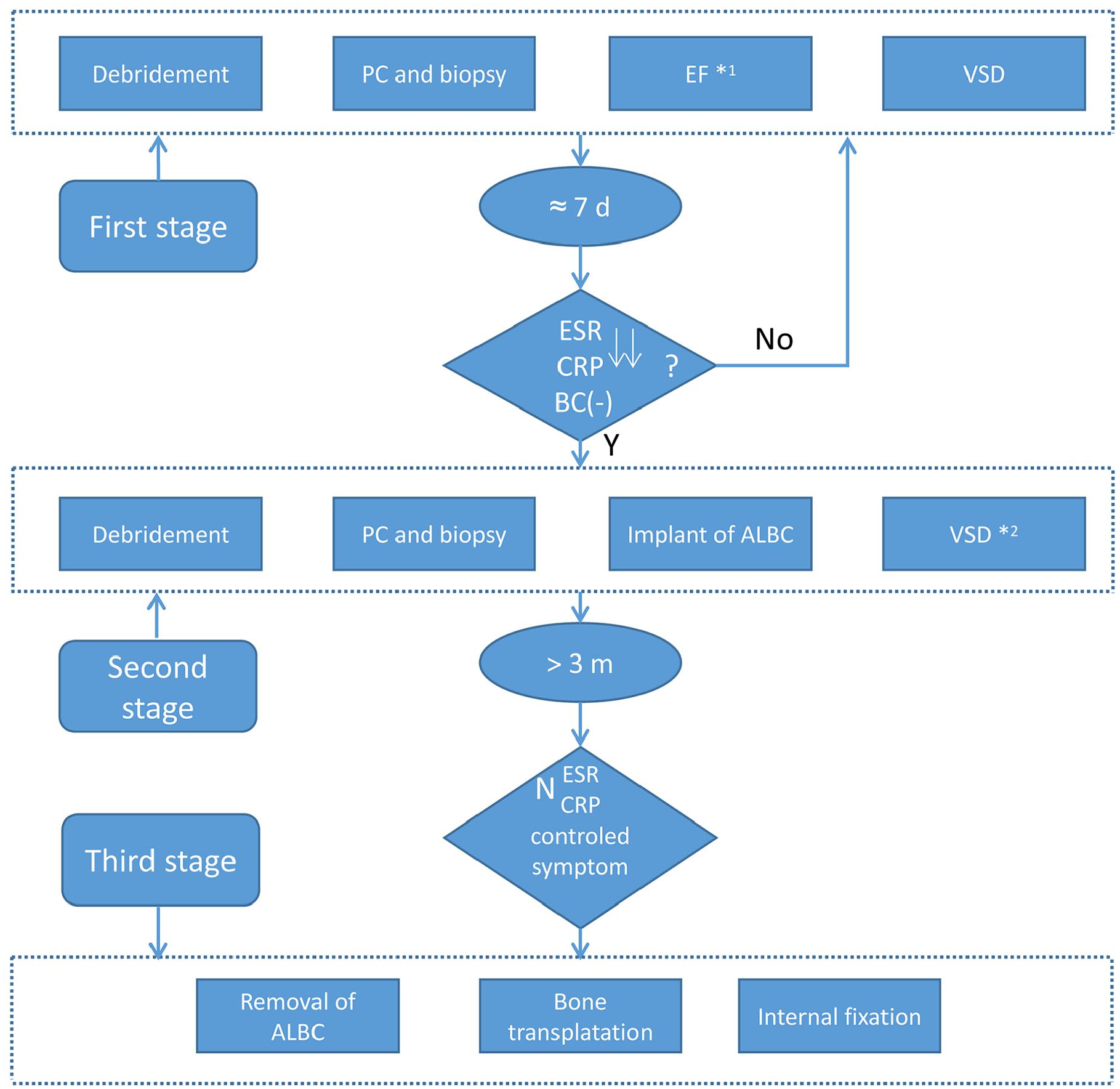
The flow diagram of the 3-stage Masquelet technique. ↓↓, continuous decrease or nearly normal level of ESR and CRP; *1, external fixation is not necessary (if the ankle and nearby joints were severely destroyed, external fixation could be used to fix the ankle in a neutral position); *2, whether the VSD is used according to the wound condition; ALBC, antibiotic-laden bone cement; BC(–), negative bacterial culture; CRP, C-reactive protein; d, days; EF, external fixation; ESR, erythrocyte sedimentation rate; m, months; N, normal level of ESR and CRP; PC, pathogen culture.
Management During Second-Stage Operation.
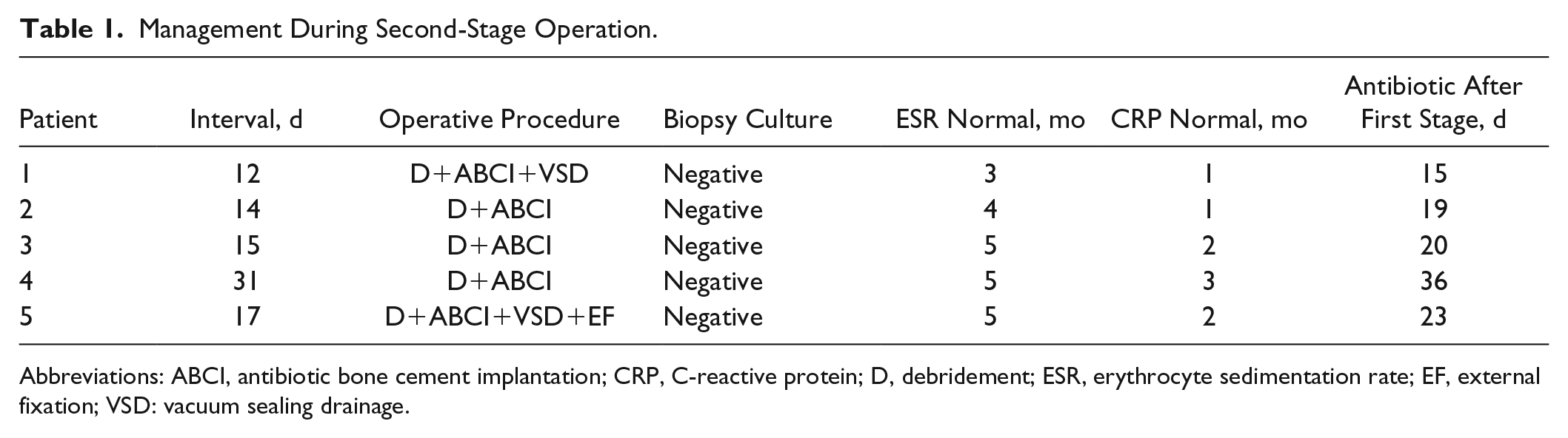
Abbreviations: ABCI, antibiotic bone cement implantation; CRP, C-reactive protein; D, debridement; ESR, erythrocyte sedimentation rate; EF, external fixation; VSD: vacuum sealing drainage.
Management During Third-Stage Operation.
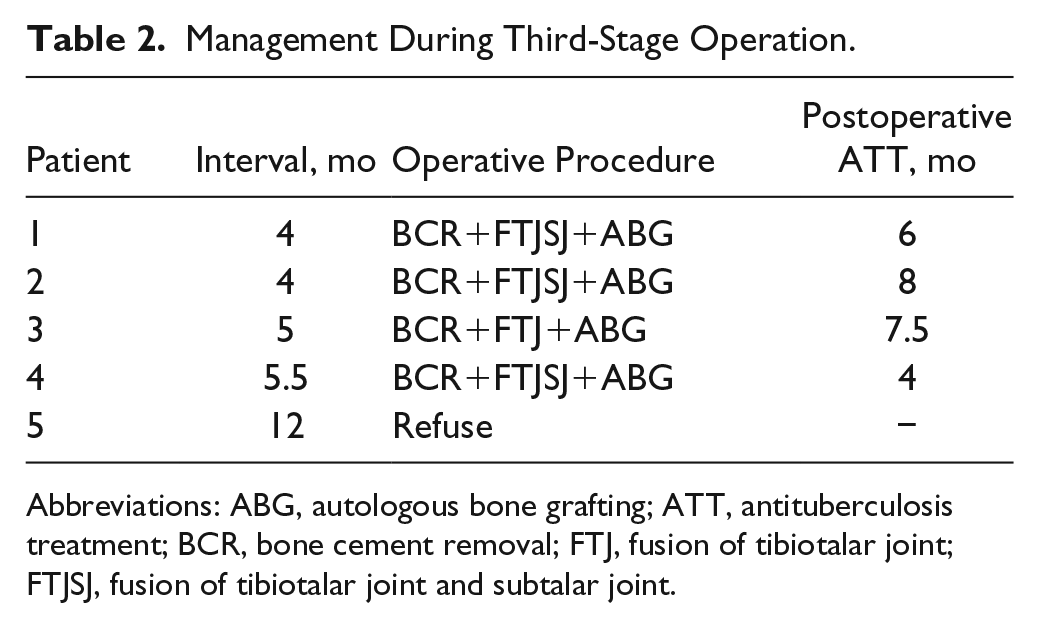
Abbreviations: ABG, autologous bone grafting; ATT, antituberculosis treatment; BCR, bone cement removal; FTJ, fusion of tibiotalar joint; FTJSJ, fusion of tibiotalar joint and subtalar joint.
For the 1-stage operation, medial, lateral, or combined incisions were used to expose the ankle joint or calcaneus and eliminate TB-infected tissue. One dorsolateral incision of the first metatarsophalangeal joint was used for the first metatarsophalangeal tuberculosis. The operation was similar to the first-stage operation described above, except that bone transplantation and arthrodesis were done at the same stage.
Postoperative Management
For the 3-stage operation, we actively observed peripheral circulation and the condition of the affected limbs as well as the irrigation and tube patency of the VSD after the first operation. In addition, appropriate antibiotics were used. An estimated 7-10 days after the second operation, patients could start partial weight-bearing with the protection of a brace or external fixation to decrease the incidence of osteoporosis from disuse. Intravenous antibiotics were also used until 2 weeks after the second-stage operation. We cautiously observed the wound. If the infection was not controlled, debridement was performed again. After the third operation or the 1-stage surgery, appropriate antibiotics were used for 3-7 days. Patients used a boot nonweightbearing until partial union of the bone and then started partial weightbearing exercise.
For both operations, continuous, reasonable, and combined ATT, such as isoniazid, rifampicin, pyrazinamide, and streptomycin, were used orally every day postoperatively for 2-3 months. Then, isoniazid, rifampicin, and streptomycin were used every day for 10-12 months. Routine blood test, ESR, CRP, and hepatorenal function were checked during treatment. A follow-up was performed each month including plain film examination and blood examination. Respective operative outcomes were assessed prior to surgery and again every 3 months postoperatively with the use of clinical, laboratory, and radiographic outcome measures. The American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot and VAS pain scores were recorded at every follow-up. Complications including recurrence, infection, implant failure, etc were also recorded.
Statistical Methods
Statistical analysis was performed using SPSS software, version 20. Continuous data were expressed as mean values ± standard deviation. Comparisons between different time points were made using paired Student t tests. A significant result was taken as P <.05.
Results
In the present cases, 6 patients were male and 4 were female. The age of the 10 patients was 56.7 ± 17.7 (range, 33-81) years. There were 6 patients with TB on the left side and 4 patients on the right side. The chronicity of infection ranged from 2 months to 4 years. Nine patients complained of pain and dysfunction in the ankle and its surroundings, and 1 in the medial forefoot. A sinus tract was present in 4 of 10 patients. All 10 patients denied any history or known diagnosis of tuberculosis at the time of evaluation. The ESR and CRP before the operation were 59.5 ± 38.6 and 42.0 ± 23.1, respectively. Lung tuberculosis was present in 5 patients. There was no patient with HIV infection. The biopsy results showed that all cases were TB. However, 5 patients had been definitively diagnosed relying on imaging examinations and laboratory tests preoperatively, and 5 other questionable patients were definitively diagnosed relying on biopsy. Details of the patients for the first-stage operation and the 1-stage surgery are shown in Table 3. Nine of 10 patients were followed up 30.3 ± 17.8 (range, 6-57) months after the third operation or single surgery (Table 4).
Details of the Patients During the First Operation or 1-Stage Operation.
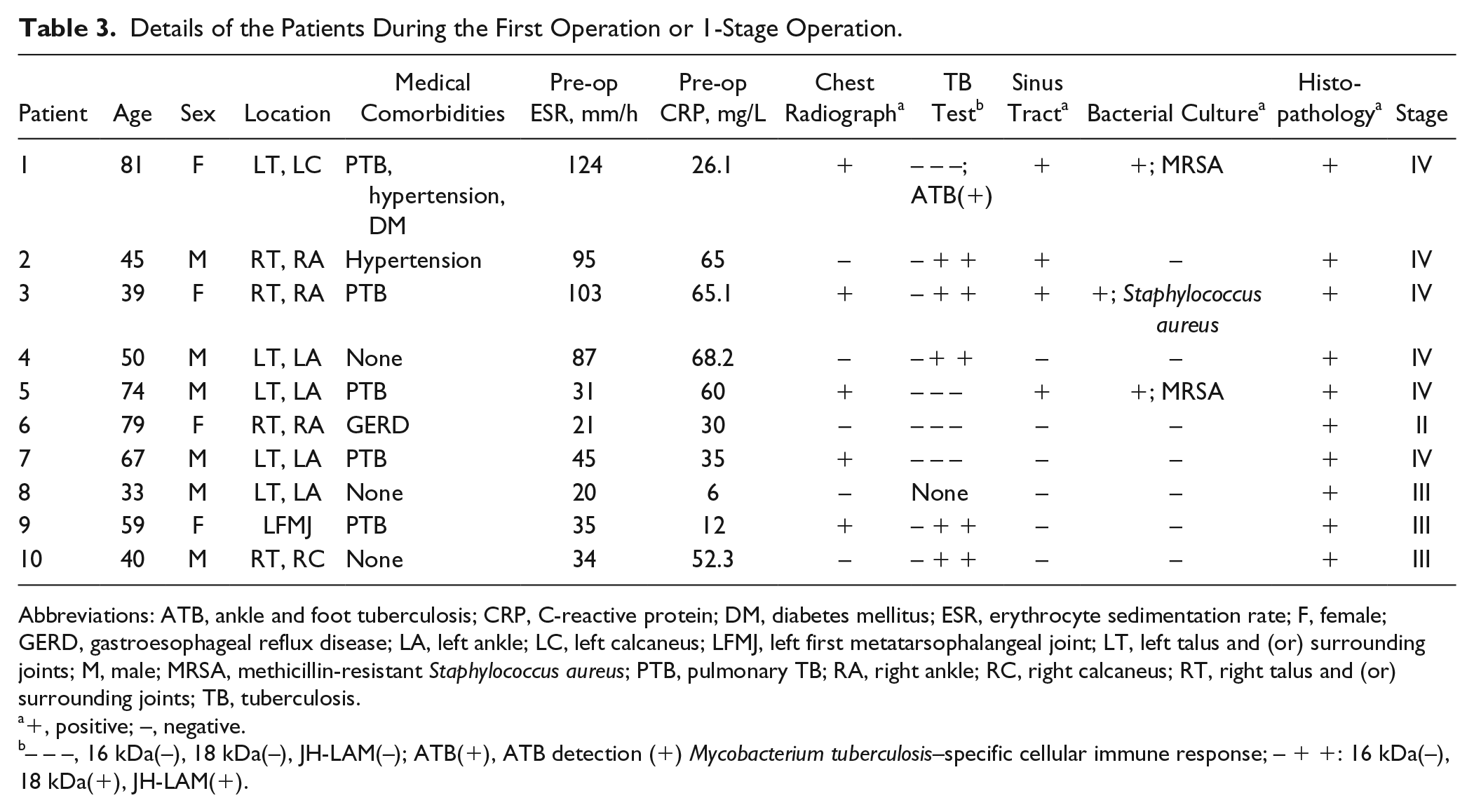
Abbreviations: ATB, ankle and foot tuberculosis; CRP, C-reactive protein; DM, diabetes mellitus; ESR, erythrocyte sedimentation rate; F, female; GERD, gastroesophageal reflux disease; LA, left ankle; LC, left calcaneus; LFMJ, left first metatarsophalangeal joint; LT, left talus and (or) surrounding joints; M, male; MRSA, methicillin-resistant Staphylococcus aureus; PTB, pulmonary TB; RA, right ankle; RC, right calcaneus; RT, right talus and (or) surrounding joints; TB, tuberculosis.
+, positive; –, negative.
– – –, 16 kDa(–), 18 kDa(–), JH-LAM(–); ATB(+), ATB detection (+) Mycobacterium tuberculosis–specific cellular immune response; – + +: 16 kDa(–), 18 kDa(+), JH-LAM(+).
Follow-up.
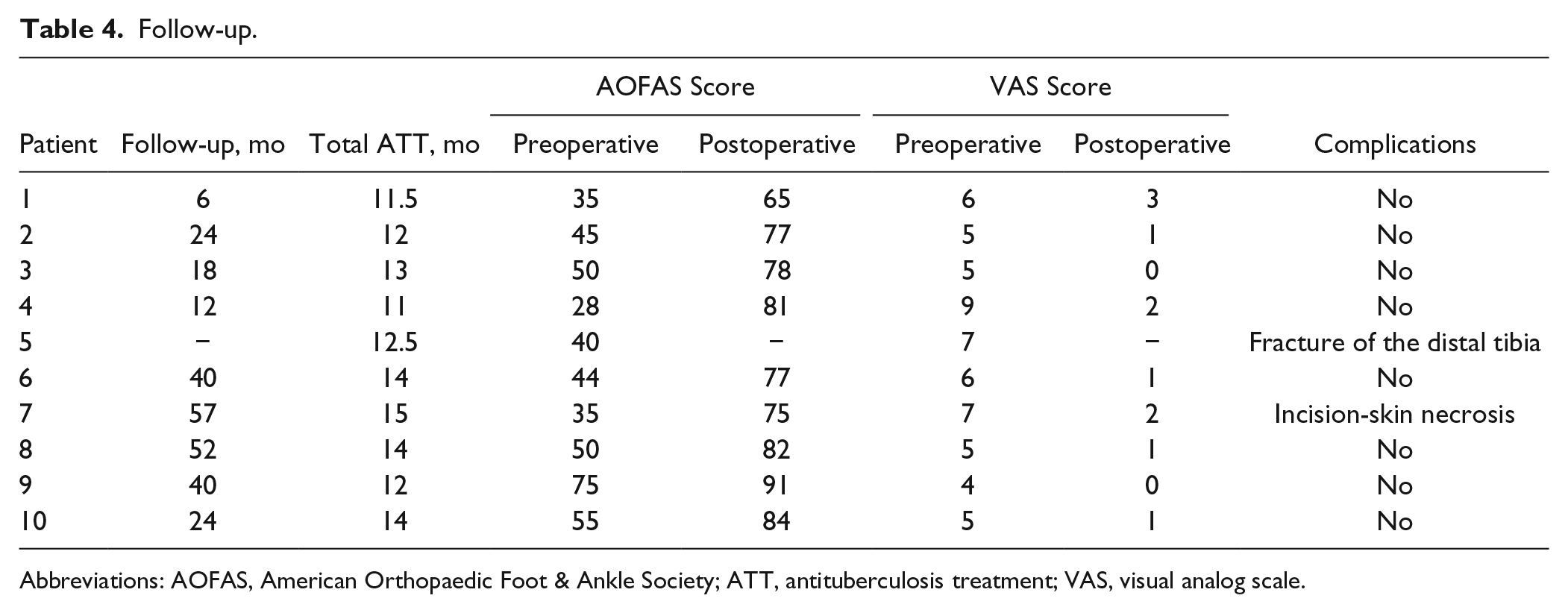
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; ATT, antituberculosis treatment; VAS, visual analog scale.
In the 3-stage operation group, there was no reinfection. Blood ESR and CRP decreased to normal levels 4.4 ± 0.9 months and 1.8 ± 0.8 months after the second operation, respectively. The duration of antibiotic use after the first-stage operation was 22.6 ± 8.0 days. The interval between the second and third operations was 6.1 ± 3.4 months. All 4 patients who received the third-stage operation achieved bone union at an average of 3.7 months. The total duration of anti-TB therapy was 12.0 ± 0.8 (range, 11-13) months. There was no case of local recurrence or skin sinus. No implants were broken or screws loosened in this group. A typical case example is shown in Figure 1. However, 1 patient only agreed to 2 surgeries but his TB infection was eliminated before he refused the surgery (Figure 3). The AOFAS score increased from 39.5 ± 9.9 (range, 28-45) preoperatively to 75.3 ± 7.0 (range, 65-81) postoperatively (P < .05). The VAS pain score decreased from 6.3 ± 1.9 (range, 6-9) preoperatively to 1.5 ± 1.3 (range, 0-3) postoperatively (P < .05).
A man with tuberculosis (TB) of ankle received the first 2 surgeries of 3-stage operation. (A) The histopathology at first surgery showing TB infection. (B, C) Radiographs taken 6 months after second operation. (D, E) The radiographs 12 months after the second surgery showing a distal tibia fracture despite eliminating TB.
In the 1-stage operation group, 1 patient experienced skin necrosis and recovered after skin flap transplantation. There was no reinfection and no broken implants or loosened screws in the group (Figure 4). The total duration of anti-TB therapy was 13.8 ± 1.1 months (range, 12-15). The AOFAS score increased from 51.8 ± 15.0 (range, 35-75) preoperatively to 81.8 ± 6.3 (range, 75-91) postoperatively (P < .05). The VAS pain score decreased from 5.4 ± 1.1 (range, 4-7) preoperatively to 1.0 ± 0.7 (range, 0-2) postoperatively (P < .05).

A 33-year-old man accepted 1-stage operation. (A, B) Anteroposterior (AP) and lateral views 40 months after the surgery and before he opted to have the internal fixation removed, showing bone union of fusion. (C, D) AP and lateral views after the removal of internal fixation.
Discussion
Generally, appropriate long-term combined antituberculosis therapy, involving multiple antituberculous medicines, such as isoniazid, streptomycin, rifampicin, and pyrazinamide, is used to manage osteoarticular TB involving the foot and ankle. A minimum of 9-12 months of multidrug antituberculosis treatment has been shown to be enough for medical treatment. 12 In Karkhur’s case, conservative treatment with ATT achieved good outcomes. 14 However, solo ATT is only advised in the early stage, as Chen et al 3 reported that 4 of 29 patients used only ATT (and 3 of those 4 patients received surgery later). Because of the atypical symptoms, laboratory results, and imaging features of osteoarticular TB, delayed diagnosis often occurs, resulting in destruction of bone and joint and even soft tissue sinus mixed with other infections. In the present cases, all 10 patients denied any history or known diagnosis of tuberculosis at the primary evaluation. The probable reasons are that the symptoms of TB are atypical and these patients were not aware of those symptoms. Contrary to them, those who recognized early symptoms may have received ATT, avoiding delayed musculoskeletal TB. In addition, 5 of the present cases were considered bacterial infections or questionable TB infections at first. Only by biopsy could the TB be definitely determined. Similarly, in Choi et al’s study, 5 only 7 of 15 patients with a final diagnosis of tuberculosis were diagnosed on the basis of clinical findings and imaging studies. Under these conditions, it is difficult to completely control TB with a single chemotherapy course of treatment. Although there are no specific guidelines with indications for surgery, with the following conditions it is appropriate to proceed with operative interventions, according to the author’s experience and the literature:3,12,35
Marked erosions above stage I on radiologic imaging.
Erosions accompanied by sinus or mixed infections.
No healing or deterioration after appropriate ATT.
Inability to get ESR/CRP to normal levels despite ATT.
Failure to identify TB or other diseases.
Traditionally, the operative treatment for advanced active TB of the foot and ankle includes debridement and arthrodesis in 1 stage, combined with a certain duration of antituberculosis therapy.3,4,12,15 As the author’s results from the 1-stage operation showed, 5 patients (1 in stage II, 3 in stage III, and 1 in stage IV) achieved good outcomes, with AOFAS score 81.8 ± 6.3 compared to 51.8 ± 15.0 before the operation (P < .05), although 1 patient had incisional necrosis. The duration of ATT was 13.8 ± 1.1 months. These findings suggest that 1-stage arthrodesis is an effective method for treating TB of the foot and ankle. Debridement, involving eliminating necrotic, infected tissues, combined with ATT can effectively remove TB. Meanwhile, drainage culture assists diagnosis and helps to determine the drugs needed for treating the infection. More importantly, biopsy is essential to confirm TB if the diagnosis is doubtful. In the presence of a large bone defect or joint dysfunction, bone grafting and arthrodesis need to be performed. According to Chen et al, 3 21 of the 28 patients in their study who received surgery achieved a satisfactory outcome. Nevertheless, talar bone collapse with flatfoot or rocker-bottom foot subsequently occurred in 6 patients. In addition, 1-stage arthrodesis for patients with active tuberculosis has a potential risk of TB reactivation. The presence of sinus tract drainage usually indicates pyogenic infections. Sinus tracts can also increase the difficulties of thorough debridement. In the absence of thorough control of the infection, not only can internal fixation increase the possibility of fixation infection, which results in deterioration and instability, but the fusion failure rate also increases. Under these conditions, staged surgery could be a potential method.
Since Masquelet et al 22 introduced the induced membrane technique (Masquelet technique), it has been widely used for bone defects. 23 For instance, good efficacy was also obtained for treating infected long bone defects.25,31 In the Masquelet technique, the 2 main stages are separated: debridement and antibiotic bone cement implantation in the first stage and bone cement removal and bone reconstruction several weeks afterwards in the second stage. Recently, the Masquelet technique was also used for treating osteoarticular tuberculosis. For hip tuberculosis, Yoon et al 34 suggested that if thorough debridement could not be achieved, a 2-stage total hip arthroplasty should be considered. Liangjun Li et al 20 described a 2-stage total hip arthroplasty in detail and achieved good outcomes. 2 In terms of TB of the foot and ankle, Zou et al 35 suggested a 2-stage operation in the midfoot, in which debridement and antibiotic cement placement in the cavity were performed in the first stage, and subsequently bone grafting and arthrodesis were performed when the infection was controlled completely. Their study reported good outcomes with no complications in 14 cases. J. H. Lee et al 17 demonstrated that streptomycin bone cement, with its rapid, enduring, and efficient isolated concentration, had effective elution characteristics and antimycobacterial effects during a 30-day period and can be a potential implant to eliminate osteotuberculosis. In addition, a previous paper described that with antibiotic bone cement, not only can rigid internal fixation be used at the second stage but the infection risks also do not increase after first-stage control. 35 Moreover, it can shorten the period of anti-TB drug therapy and has a satisfactory prognosis. However, their cases only refer to the midfoot.
The VSD technique, used for removing infectious and necrotic substances and promoting the presence of various growth factors in wounds, can facilitate wound recovery and is widely used as an assistive therapy combined with surgery for various infections and open trauma.21,24,26 In addition, several surgeons applied it to TB infections in deep tissue and TB infections with sinus tracts.13,32 In Jia’s study, 13 the median healing time was 19.6 days for 38 patients in the experimental group, which was apparently shorter than for the control group, indicating that VSD is conducive to wound healing and controlling TB with sinus tracts.
Because of the complex anatomy of the foot and ankle, bacteria can easily attach to tissue and diffuse so that 1 debridement is often not complete even with the 2-stage Masquelet technique, resulting in failure of surgery. 9 Inspired by the successful application of VSD and antibiotic bone cement for osteoinfection, the 3-stage Masquelet technique was used in the authors’ previous 19 cases for infected bone defects at the beginning and acquired excellent outcomes. 19 Additionally, the 3-stage Masquelet technique was applied to 5 cases of TB of the foot and ankle with destructive bone or sinus tract, and 3 of them had additional bacterial infections. Four of the 5 patients achieved bone union and obtained an AOFAS score of 75.3 ± 7.0. One patient developed a distal tibia fracture, indicating that there is a possibility of bone fracture after bone cement implantation and that gradual and proper weightbearing is necessary. Notably, this patient’s TB of the ankle was completely controlled, although he rejected the third-stage operation. No reinfection was present in any of the 5 patients.
According to our experience and the results of our cases, the 3-stage Masquelet technique reveals several advantages and disadvantages compared with other methods. First, it enables antituberculous drugs and antibiotics to have a rapid effect when most necrotic, infected tissues and sinus tracts are removed, thereby avoiding failure of the first-stage operation in which bacterial biofilm produced by uncontrolled bacteria can result. Second, VSD involves eliminating necrotic, infected tissues and accelerating the union of soft tissue after debridement so that bacterial infection and TB can be better controlled. 13 In addition, culture results and biopsy are essential to define diagnosis and guide effective antibiotic or antituberculosis drugs to control localized infection, and they also offer proof for which kind of antibiotic bone cement should be implanted at the next stage. Fourth, local, efficient, long-lasting chemotherapy can increase the drug concentration, and it is beneficial to control the residual tubercular and mixed infectious nidus.2,33,35 Fifth, the efficacy of debridement, antibiotics, and ATT can be tested by monitoring ESR and CRP during the debridement stage. Moreover, after eradicating tuberculosis and other pathogens, rigid internal fixation combined with bone implants can provide an excellent condition for arthrodesis, with a rare instance of infection or reinfection, achieving satisfactory function of the foot and ankle. Last, to some extent, if there is vast soft tissue coloboma, skin flap transposition can also be performed after complete elimination of the infection. However, an increased severity of infection will increase the number of operations, prolong the time needed for therapy, and increase the cost of treatment. Despite these disadvantages, no reinfections occurred, and 4 of the 5 achieved bone union, which suggests that the 3-stage Masquelet technique is a potentially reliable method for treating foot and ankle TB mixed with sinus tract and bacterial infections.
Importantly, there are some notes for the 3-stage Masquelet technique:
In the first stage, debridement holds the key to the whole surgery. Debridement must be performed thoroughly, including necrotic tissue, inflammatory granulation tissue, and soft tissue with sinus tract, until normal bone and soft tissue with active blood flow remain. The application of irrigation and drainage of VSD can further decrease the concentration of bacteria and TB and promote the growth of fresh granulation tissue. Properly repeated debridement should be performed so as to control the local infection.
In the second stage, the choice of antibiotic and antituberculosis drugs for the antibiotic cement spacer is undoubtedly important. The drug or fixed drugs should contain some basic characteristics such as good thermal and chemical stability, durable release, and little disturbance for the mechanical properties of bone cements etc. 16 In addition, good antibacterial and antituberculosis capacity when combined with bone cement is essential, with little mutual negative effect between each element. Mixed with bone cement, the long-lasting release of vancomycin, gentamicin, rifampicin, moxifloxacin, and streptomycin can be achieved over 30 days, but the mechanical properties of rifampicin-loaded bone cement are poor. A total of 1-2 g of streptomycin to 40 g bone cement can reach the effective concentration in 30 days, and its mechanical properties are relatively good such that patients can perform partial weight-bearing exercise at the second stage to avoid osteoporosis.11,17 Although the combination of streptomycin with amoxicillin/potassium clavulanate in bone cement can promote efficacy for antituberculosis in skeletal muscle, their antibiotic efficacy is not often enough, especially for MRSA. 17 Therefore, we often choose vancomycin and streptomycin mixed with bone cement for foot and ankle TB with sinus tract, but this choice is actually in accordance with the cultures as well. However, according to the authors’ experience, when directly mixing vancomycin and streptomycin with bone cement, the mechanical strength is not very good. To address this problem, streptomycin is mixed with bone cement at first, and then vancomycin-loaded cement covers it when it is not yet solidified. Furthermore, if soft tissue is severely destroyed, flap surgery can be performed at this stage. 19
As for the choice of bone reconstruction surgery in the third stage, adjacent bone tissue and joints are often destroyed by tuberculosis, and mixed infections in the foot and ankle, arthrodesis, and simultaneous repair of bone defects are choices for the majority of infectious bone defects of the foot and ankle. Before the surgery, the wound should have been sterile for more than 6 months, and ESR and CRP should be normal. Under these conditions, the wound can be considered an aseptic wound, and internal fixation for arthrodesis is secure. In the authors’ study, no skin necrosis or infection occurred. Several papers also support the application of internal fixation at this stage.2,19,20,35
In the present study, 9 of 10 patients achieved relatively good efficacy by both 1- and 3-stage operations. The argument is that there is no criterion standard of methods for TB of the foot and ankle. In the 5 cases treated with a 1-stage operation, 1 was stage II, 3 were stage III, and 1 was stage IV TB, in which no sinus occurred, indicating that 1-stage operation is effective for treating foot and ankle TB. The 5 patients treated with the 3-stage Masquelet technique were all stage IV, and 3 of the 5 presented with bacterial infections. Zou et al 35 recommended that stage III or IV TB be treated with a 2-stage operation regardless of the presence of a sinus tract. However, according to the authors’ experience, 1-stage operation can be used for early-stage foot and ankle TB no more than stage III, without sinus tracts or mixed infections. Once stage IV is reached—when sinus tracts usually occur—or there are sinus tracts or mixed infection, the 3-stage Masquelet technique should be applied to better control the TB and mixed infections and achieve better bone reconstruction (Figure 5).
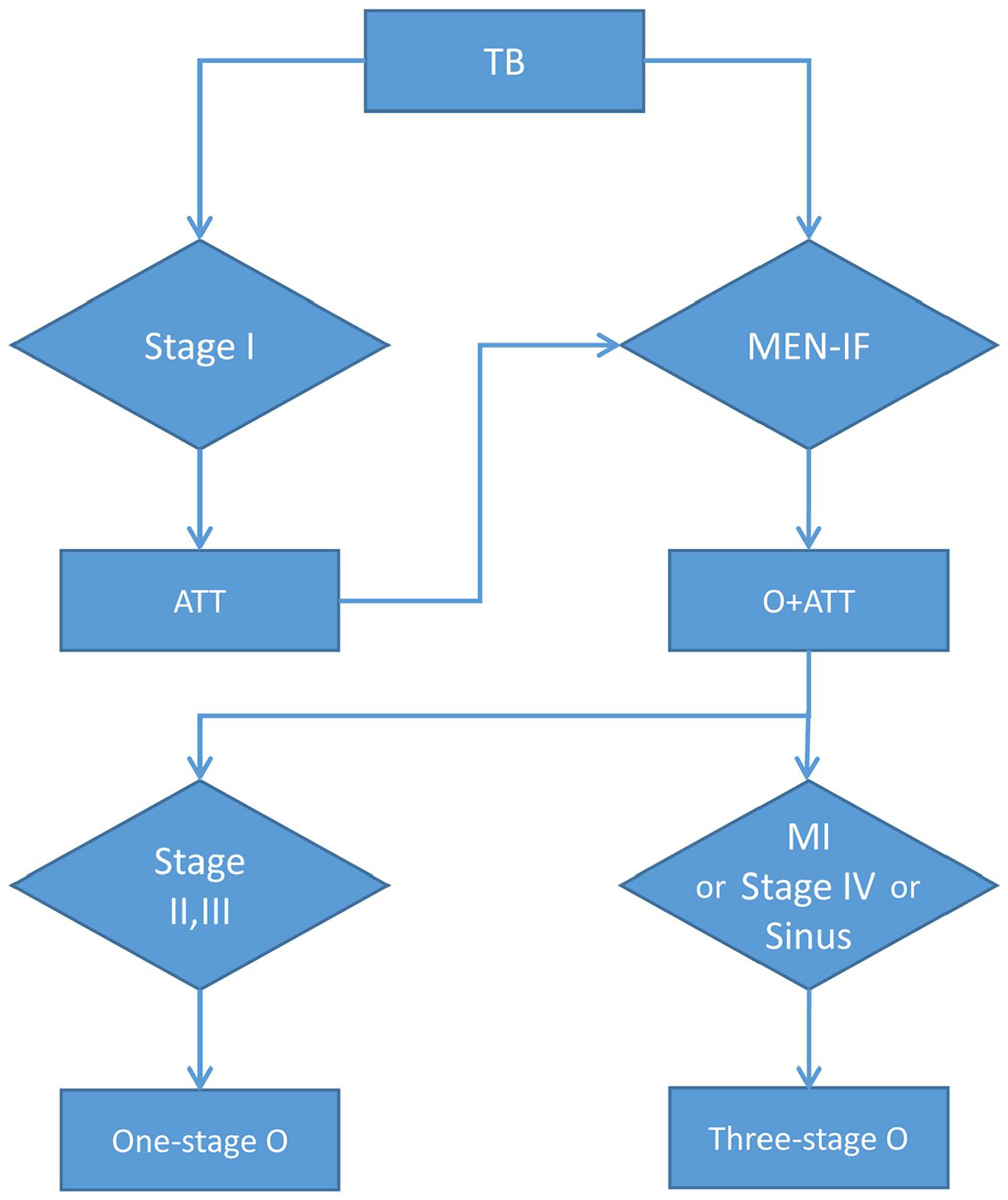
The flowchart of the choice for the treatments of foot and ankle TB. ATT, antituberculosis treatment; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; MEN-IF, any of the following 5 conditions—Marked erosions above stage I on radiologic imaging, Erosions accompanied by sinus or mixed infections, No healing or deterioration after appropriate ATT, Inability to trend ESR/CRP to normal levels despite ATT, or Failure to identify TB or other diseases; MI, mixed infections; O, operation; TB, tuberculosis.
There are several limitations in the present study. For instance, the sample undergoing both operations was small, and there was no comparison of operations for the same stage of foot and ankle TB. Further studies with a large sample size and a longer follow-up need to be performed. In addition, it is not clear whether the staged Masquelet technique is suitable for treatment of the early stages, regardless of its ability to eliminate tuberculous and mixed infections for the destruction of foot and ankle, especially when accompanied by sinus tracts. Moreover, undergoing several surgeries is stressful for the body and relatively costly.
Conclusion
Although single ATT and 1-stage or 2-stage operations are traditionally considered safe procedures for most patients with TB of the foot and ankle, our practical experience indicates that 3-stage operation is preferable for destructive TB of the foot and ankle with stage IV or sinus tracts or other infections and that 1-stage reconstruction is preferable for early stages such as stages II and III. With antituberculous medications and VSD, we believe the 3-stage protocol offers the greatest chance for the eradication of infection while achieving better bone reconstruction.
Supplemental Material
FAI890854_ICMJE_Disclosures – Supplemental material for Three-Stage Masquelet Technique and One-Stage Reconstruction to Treat Foot and Ankle Tuberculosis
Supplemental material, FAI890854_ICMJE_Disclosures for Three-Stage Masquelet Technique and One-Stage Reconstruction to Treat Foot and Ankle Tuberculosis by Wenqiang Qu, Chi Wei, Li Yu, Yu Deng, Panfeng Fu, Zhe Kang and Shaobo Zhu in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.