
Abstract
Background:
Rheumatoid arthritis (RA) can cause significant forefoot disorders. If forefoot deformity and pain are severe, surgical treatment can be considered. The aim of this study was to analyze the long-term outcomes of surgical forefoot correction per Tillmann, which involves resection of the metatarsal heads through a transverse plantar approach for the lesser toes and a dorsomedial approach to the great toe.
Methods:
This retrospective study used patient-based questionnaires to analyze the revision rate, pain, use of orthoses, walking ability, forefoot function, and patient satisfaction of patients with RA who had undergone a complete forefoot correction of metatarsophalangeal (MTP) I to V. The study only included participants with RA before the era of biological agents and who were at least 20 years postoperatively. A total of 60 patients who had undergone 100 complete forefoot operations according to Tillmann 24.6 ± 3.5 years ago were included in this study.
Results:
The data collected showed that 35 reoperations were performed on 26 of the patients. Deformity relapses were often documented for the hallux valgus. More than 60% of the patients were able to wear conventional shoes. The distances the participants were able to walk were significantly increased by wearing shoes when compared with walking barefoot (P < .01).
Conclusion:
While forefoot function remained difficult to assess, the majority of patients were able to use conventional shoes. This long-term follow-up study of patient-reported questionnaires completed more than 20 years after the Tillmann procedure showed that more than 80% of the patients remained satisfied with the outcome.
Level of Evidence:
Level IV, retrospective cohort study.
Keywords
Introduction
Rheumatoid arthritis (RA) is a disease with an inflammatory process of the synovial membrane in joints, tenosynovial sheaths, and bursae. Despite major improvements in drug therapy over the last decades,9,17 the inflammatory process can lead to severe destruction of joints, causing substantial deformities, particularly if the drug therapy fails. 10 Tendons can deteriorate or even rupture and cause a loss of function. 26 Additionally, the bursae below the metatarsal heads are often severely inflamed and painful with pronounced swelling. This inflammatory and destructive process is often simultaneously found in all 3 parts of the foot. 21 Thus, patients with RA and a failure of antirheumatism medication (disease-modifying antirheumatic drugs [DMARDs]) can have a significant forefoot deformity with pain, and loss of mobility and function. Such patients will likely need to wear orthopedic shoes as normal shoes can no longer be tolerated. 28
In order to correct the deformity and reduce pain, several surgical techniques have been used over the last decades, including arthrodesis.4,13,15,20,27,28 One method commonly used is the Clayton-Hoffmann technique on the lesser toes, which is often concurrently used with a fusion of the first metatarsophalangeal (MTP) joint. 8 Another method is a complete forefoot correction according to Tillmann, which is the standard procedure at the authors’ institution for such forefoot disorders and which is a well-described procedure by Karl Tillmann.6,29,31,32 The operation includes a Hueter-Mayo procedure with a dorsomedial approach for the hallux valgus (HV) and a plantar approach to the lesser toes for resection of the metatarsal heads with some particular modifications. 29 The main goal of this surgical treatment is to reduce forefoot pain, increase the ability to wear conventional shoes, and maintain forefoot function.29,30
This study analyzes data from patients with RA with severe forefoot deformities who, before the era of biological treatment, underwent a complete forefoot correction per Tillmann. The study only included participants who were at least 20 years postoperatively.
Methods
Surgical Procedure
Complete forefoot arthroplasty as described by Tillmann of the rheumatoid foot includes a modification of the resection arthroplasty of the MTP I joint by Hueter 15 and Mayo,20,32 in combination with a modified resection arthroplasty of MTP joints II to V according to Hoffmann.13,31 Tillmann’s forefoot arthroplasty consists of a metatarsal head resection from a plantar approach, plantar capsulorrhaphy, tenolysis, and rerouting of the tendons. For the MTP I joint, a dorsomedial approach is used, before a sparse metatarsal head resection adjusted to the length of the second MTP joint is performed to create the proper position of the first digit. If needed for alignment and length adjustments, Tillmann recommends adding a resection of the proximal phalangeal base. Furthermore, the sesamoids are resected (Figure 1). After resection, the reshaped metatarsal head is covered by a dorsal capsular flap including the short extensor tendon. Arthroplasty of MTP joints II to V requires a transverse plantar approach using an elliptical excision of skin calluses and subcutaneous tissue including bursae. The distal aspect of the plantar incision curves in line with the natural metatarsal head cascade. The proximal incision is created to adequately excise any plantar calluses but may be irregularly shaped in order to maximize the length of the flap.
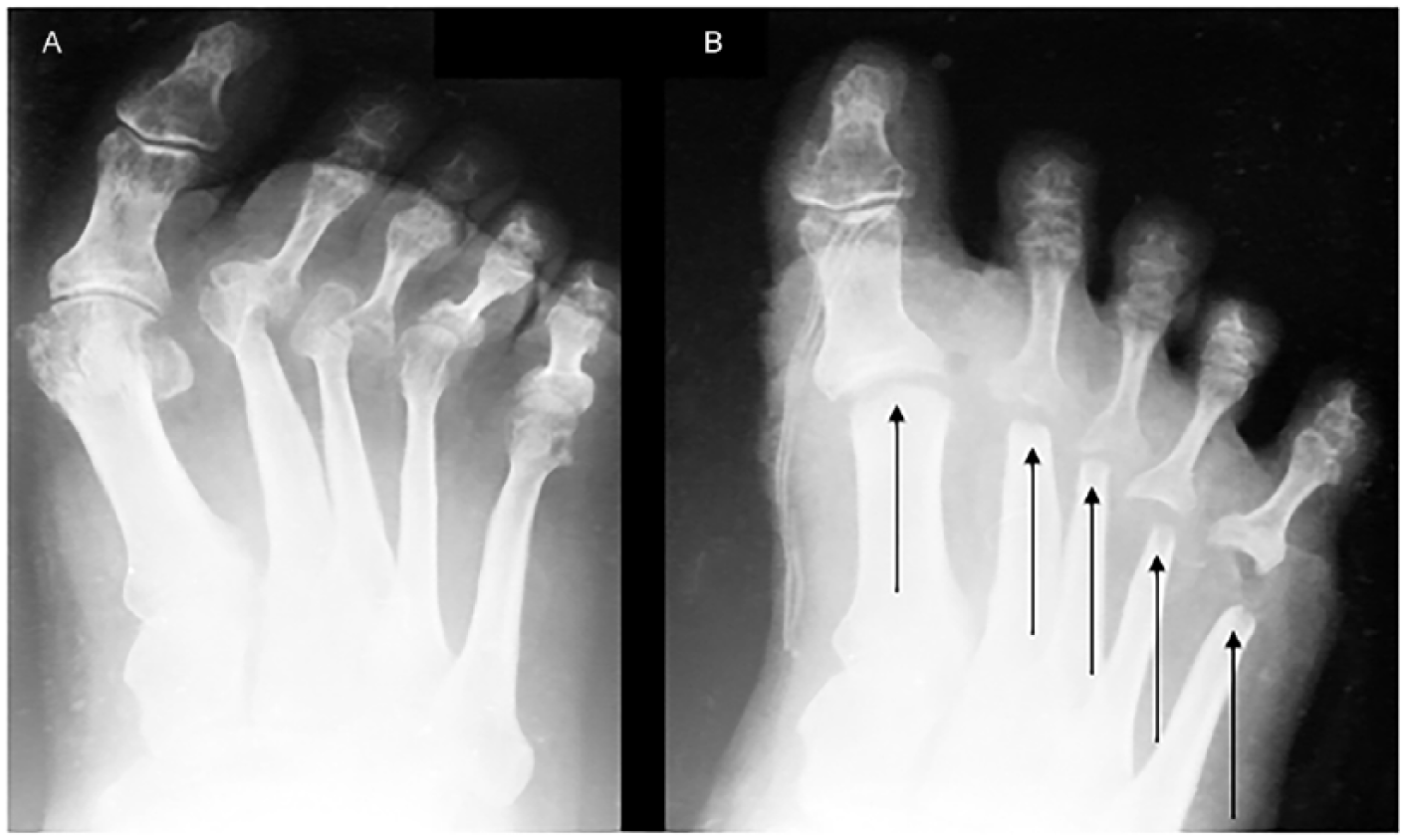
Pre- and postoperative radiographs demonstrating a forefoot. (A) The preoperative radiograph shows a severe forefoot deformity with hallux valgus and subluxation of the lesser toes, particularly digits 2 and 3. (B) The postoperative radiograph was taken in the operation room immediately after the Tillmann procedure and shows a corrective elastic dressing with a slightly intended overcorrection of the first digit for the first days. The arrows point to the resected metatarsal areas. The metatarsal head of digit 1 shows a sparse resection and anatomic position. The sesamoid bones are resected. Furthermore, it illustrates the resected metatarsal heads of digits 2 to 5 with length adjustments. The latter radiograph of the forefoot was taken with wound dressings including a radiopaque marker along digit 1.
Resection of the metatarsal heads is performed with correct alignment and length relative to each other, allowing correction of deformity and soft tissue contractures. The metatarsal stumps are rounded off, and the plantar capsule is then tightened. Thereafter, plantar tibial tightening of the capsule of the lesser toes is performed for additional alignment positioning. For lasting correction and good mobility, the arthroplasty needs to resist elastic distraction of 6 to 8 mm between the remodeled metatarsal heads and the proximal phalanges without losing the suture fixation and correction. In cases of flexion contractures of the proximal or more seldomly of the distal interphalangeal joints, manipulation of the contracted joints is often needed; sometimes, temporary Kirschner wire fixation is needed to preserve alignment.28,29,32
Patients
To be accepted into this study, patients had to have RA and had to have undergone a complete forefoot correction according to Tillmann due to a severe forefoot disorder before January 1, 1995. From the hospital database and according to the inclusion criteria, 234 patients were eligible to be included in the retrospective study (Figure 1). Data from 165 patients were archived in the electronic database. The data from 69 patients had to be assessed in film archives. Eighteen patients had to be excluded due to lack of files. Contact details for the remaining 216 patients were provided by the registration office. Of the 216 patients, 78 had already died. Letters enclosing a patient-based questionnaire were therefore sent out to 138 eligible participants. Of those 138 eligible participants, 46 did not want to participate in the study and 32 others were no longer at their registered address and consequently were untraceable for the purposes of this study. Ultimately, a total of 60 patients who had collectively undergone 100 forefoot operations agreed to participate in the study and returned the completed questionnaire. All patients were offered an appointment for a follow-up visit. However, none of the patients accepted this offer.
After applying the inclusion criteria and identifying participant locations, 60 patients who had undergone 100 forefoot reconstructions according to Tillmann had returned the questionnaire (Figure 2). Most of the participants were female (58 vs 2 male). On 7 occasions, only the left foot was operated on, while in 13 cases only the right foot was operated on. In 40 cases, both feet underwent surgery. The average age of the patient when the forefoot operation was carried out was 48.9 ± 8.7 years. The average age of those completing the follow-up questionnaire was 72.6 ± 8.3 years. All participants had a minimum follow-up time of 20 years postoperatively, averaging a total of 24.6 ± 3.5 years.
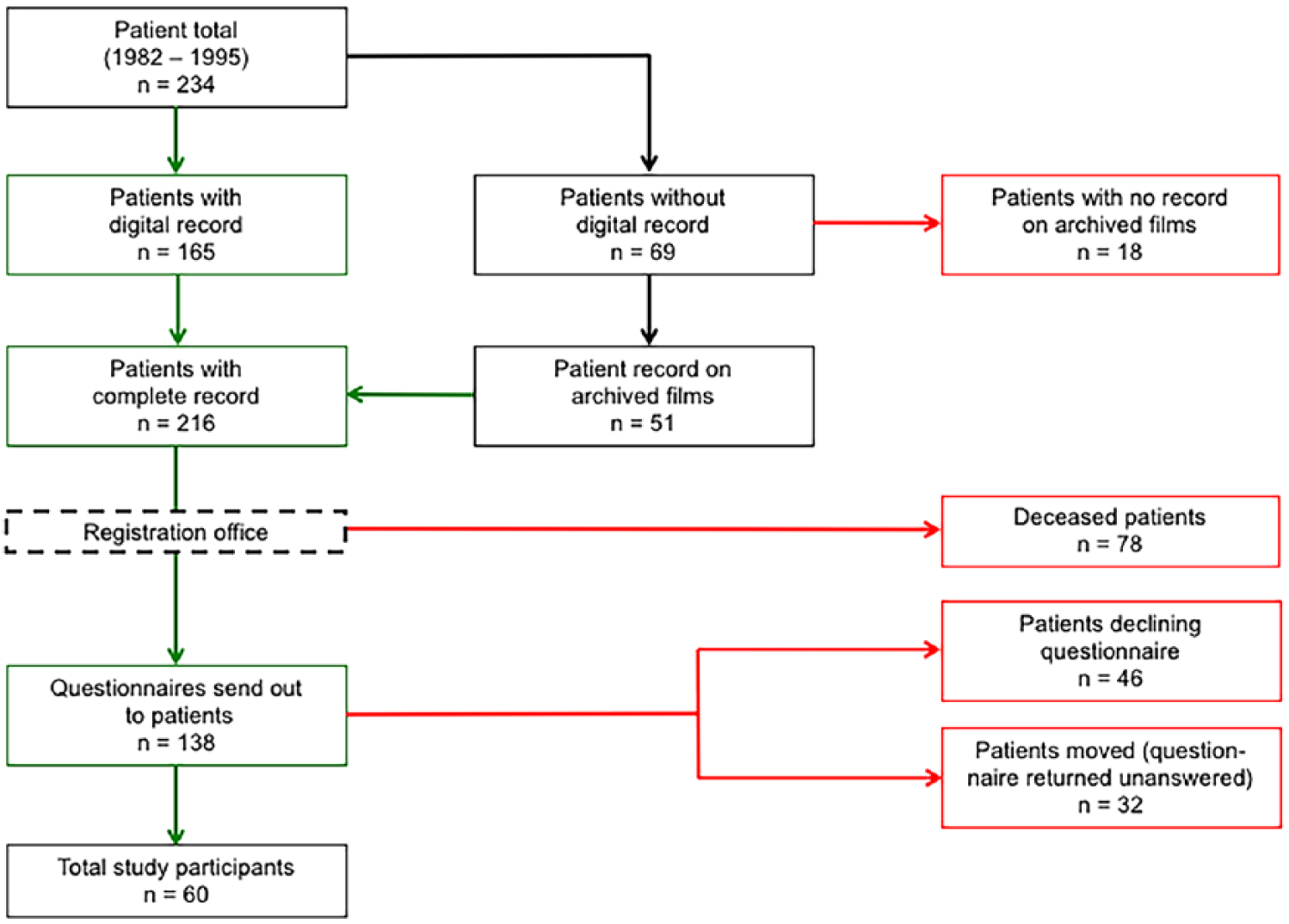
The flowchart illustrates the number of patients who had the forefoot operation (n = 234), the dropout reasons (eg, no records in archive, deceased, etc), and the total number of patients included in the current study (n = 60).
Questionnaire
The patient-based questionnaire was a self-constructed RA- and forefoot-specific outcome instrument that covered 6 survey areas: revision surgery, pain, use of orthoses, walking ability, foot function, and satisfaction with surgery (Appendix A). Secondary outcome parameters were the development of recurrent deformities such as hammertoes and HV, as well as plantar callosities. Information on revision surgery was based on information provided by the participant in the questionnaire, and the participant’s health records for the revision surgery, if available. Pain was measured on a nominal scale consisting of 3 categories: no pain, pain under strain, and rest pain. Participants were asked about their use of orthoses, particularly whether conventional shoes with or without modifications by shoemakers, custom-made orthopedic shoes, insoles, or toe pads were used in their daily life. For measurements of walking ability, participants were asked about their walking distance with and without shoes on a 4-point rating scale from “not at all” to “over 100 meters.” Foot function and balance were measured via the ability to perform a 2-legged tiptoe stand, a plantar 1-legged stand, and a 1-legged tiptoe stand for 5 seconds each. Deformity recurrence for HV, hammertoes, and plantar swelling was evaluated by each patient based on photographic examples given in the questionnaire. At the end of the survey, patient satisfaction was measured with a 4-point Likert scale.
The study was performed in accordance with the Declaration of Helsinki of 1975, as revised in 2000, and with ethical approval obtained from the local ethics committee of the Hamburg Medical Association. All participants in the study gave written informed consent.
Statistical Analysis
Statistical analysis was performed using the statistics package SPSS version 23.0 (IBM Corp., Armonk, NY). The values of descriptive statistics are expressed by means with a standard deviation (SD) as well as frequencies and percentages for nominal data. The Kendall rank correlation coefficient (rφ) was used to test the association between pain, recurrence deformities, and patient satisfaction. The Wilcoxon signed rank test for nonparametric data was applied to measure the difference between the barefoot walking distance and the walking distance with shoes. In accordance with accepted standards, statistical significance was set to a 2-tailed P value of .05.
Results
For 35% of the participants, no forefoot pain was present at the time they completed the follow-up questionnaire (Supplemental Figure 1). In approximately 40% of cases (23 participants), pain under strain was recorded. Approximately 23% of participants had pain at rest (2 patients declined to answer). Pain medication (eg, NSAIDs) was regularly taken by one-third of the participants.
Patients were asked whether they wear conventional shoes, conventional shoe wear modified by the shoemaker, custom-made orthopedic shoes, insoles, or toe pads. As multiple answers were possible, an average of 2.2 ± 0.97 combinations of orthoses were used in 60 patients. Furthermore, due to multiple selections and an individual emphasis for each category, each orthosis category was analyzed and demonstrated separately (Figure 3). Thirty-four patients (56.7%) were able to wear conventional shoes. Upon questioning, 15 patients (25%) declared using conventional shoe wear with minor modifications. Custom-made orthopedic shoes were worn by about one-third (22 patients, 36.7%) of the questioned participants. Many patients required additional orthoses like toe pads (11 patients, 18.3%) or insoles (47 patients, 78.3%). The use of proper footwear is essential for most patients to increase their mobility (Figure 4). More than 68% of participants were not able to walk unshod for more than 10 m. However, over 70% of participants were able to walk more than 100 m while wearing shoes (P < .001).
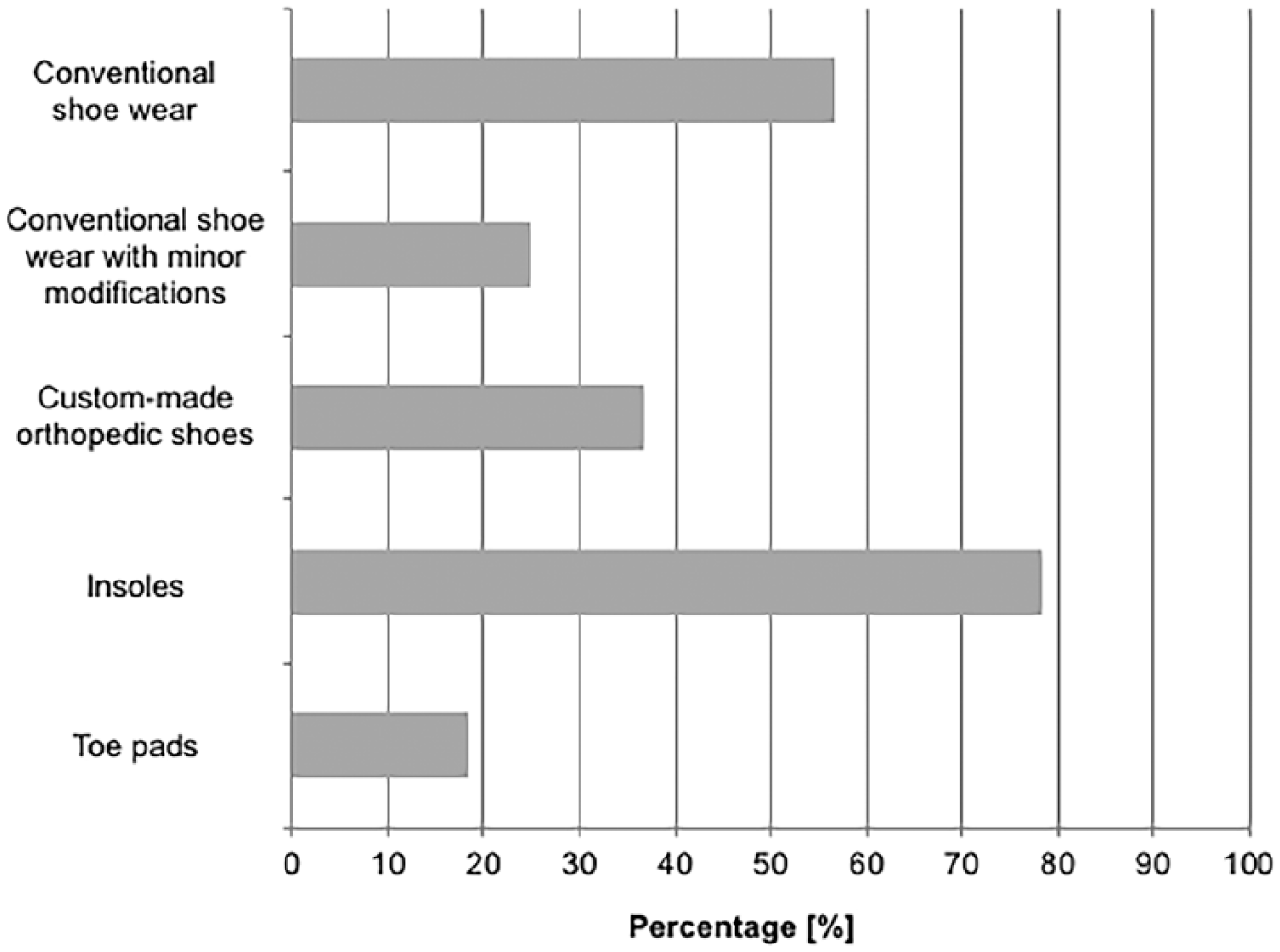
Illustration showing the use of shoe wear (conventional shoes with or without modifications by the shoemaker, custom-fabricated orthopedic shoes) and other orthoses (insoles, toe pads). Multiple answer choices were possible. Therefore, values reach more than 100% in total, as some patients require different orthoses depending on the situation in the operated foot.
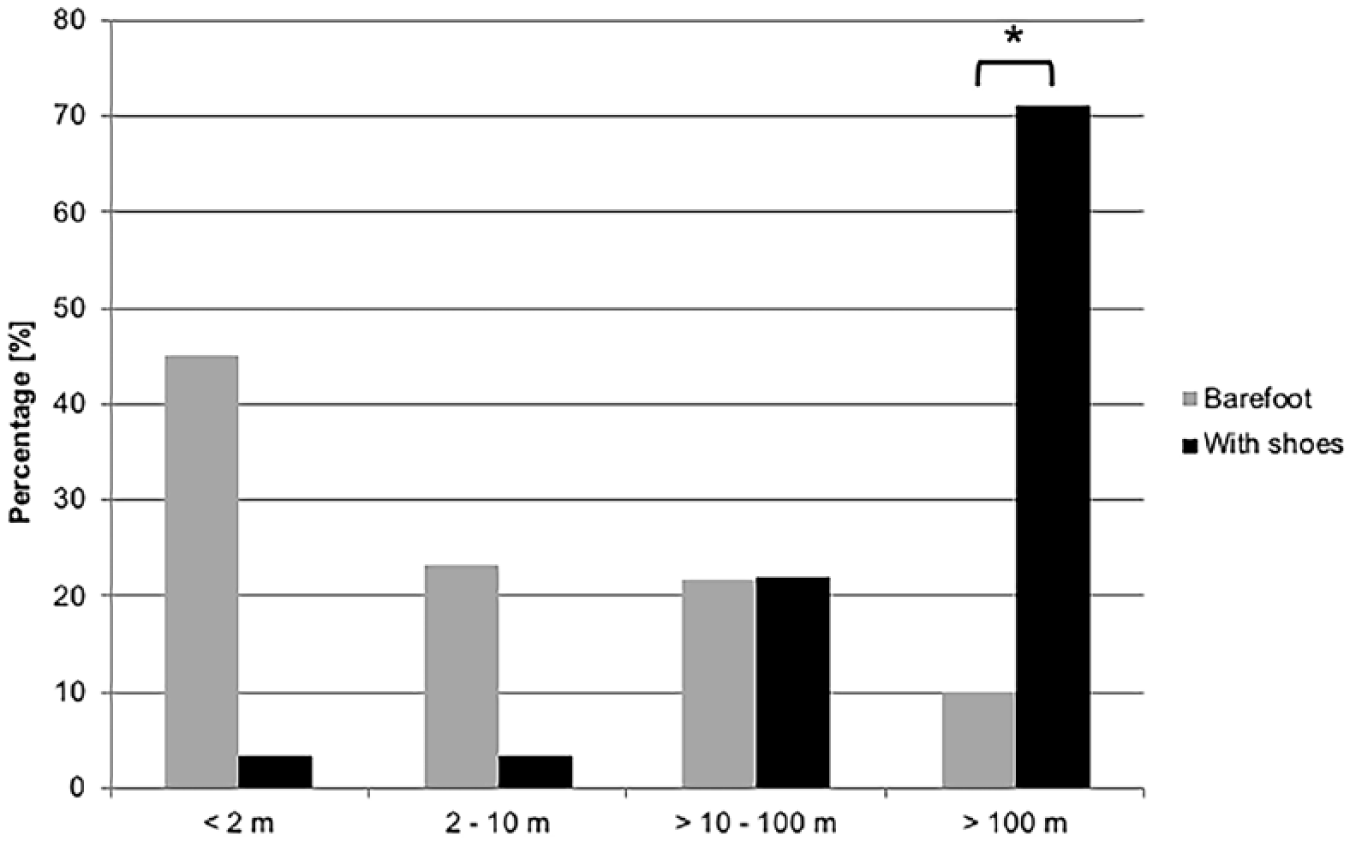
Bar graphs demonstrating the percentage of patients able to walk a specified distance (less than 2 m, 2-10 m, more than 10 m but less 100 m, and more than 100 m) barefoot or with shoes. A reciprocal significance for barefoot and shoed walking for a distance of more than 100 m is shown (*P < .001).
Functional outcomes were assessed with a 2-legged tiptoe stand, 1-legged tiptoe stand, and, the most difficult task, a 1-legged tiptoe stand (Figure 5). Fifty percent of participants were not able to perform the 2-legged tiptoe stand. However, more than a quarter of the operated feet (26.7%) could hold the position for more than 5 seconds. The 1-legged stand was possible in 60 operated feet (63.2%), but only 29 feet could bear the position for more than 5 seconds (30.5%). The 1-legged tiptoe stand was the most difficult position to perform, with only 18 operated feet being able to keep the position for more than 5 seconds (18.4%). For the majority (64.3%), the 1-legged tiptoe stand was not possible. Data for 5 feet are absent with regard to the 1-legged stand and for 2 feet for the 1-legged tiptoe stand.
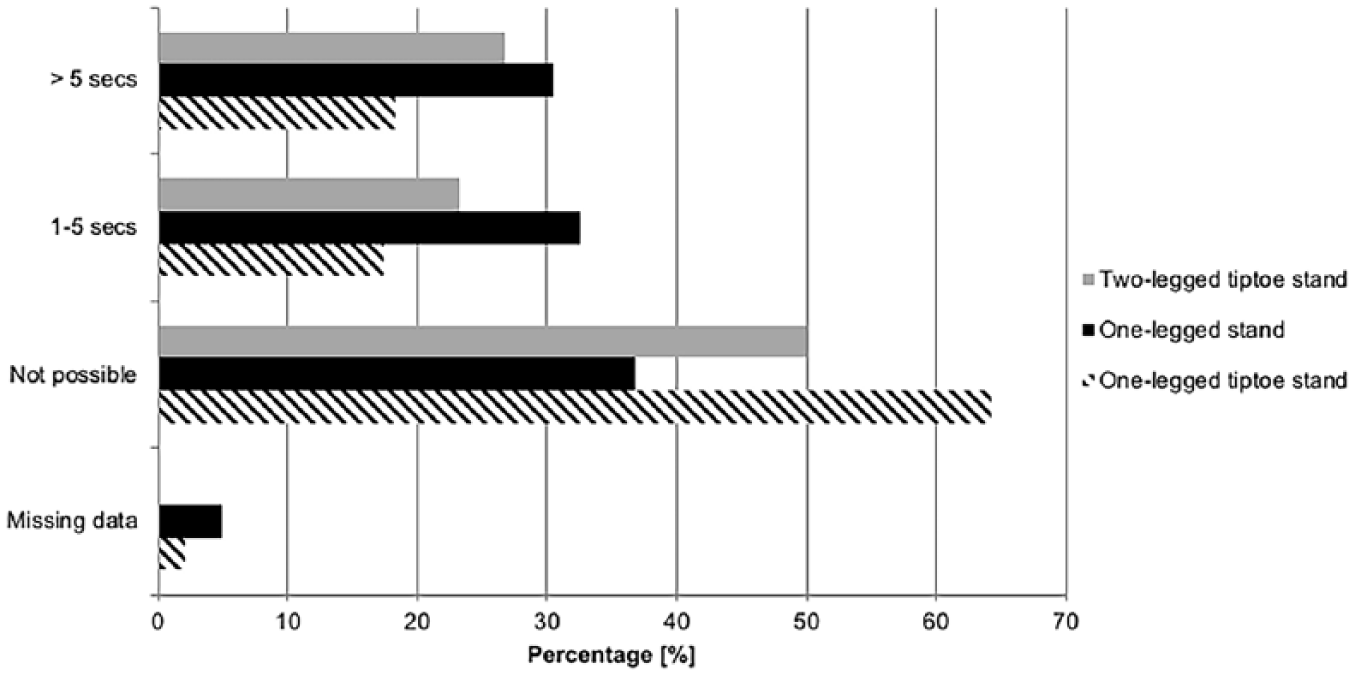
Forefoot function of the patients is demonstrated as a percentage via the 2-legged tiptoe stand, the 1-legged stand, and, the most advanced form, the 1-legged tiptoe stand. If patients were able to perform these stands, they were asked to specify whether it was possible to hold the position for 1 to 5 seconds or longer.
There were no recurrences for hammertoes or plantar swelling in 64 and 65 feet (66.0% and 68.4%), respectively (Figure 6A). Only 10 feet (10.3%) had a severe relapse of hammertoes, and only 8 feet (8.4%) had a severe relapse of plantar swelling. Recurrent HV was documented as mild to moderate in 30 feet (31.25%), and severe in 29 feet (30.2%). Information is lacking for 4 HV, 3 hammertoes, and 5 feet with plantar swelling.
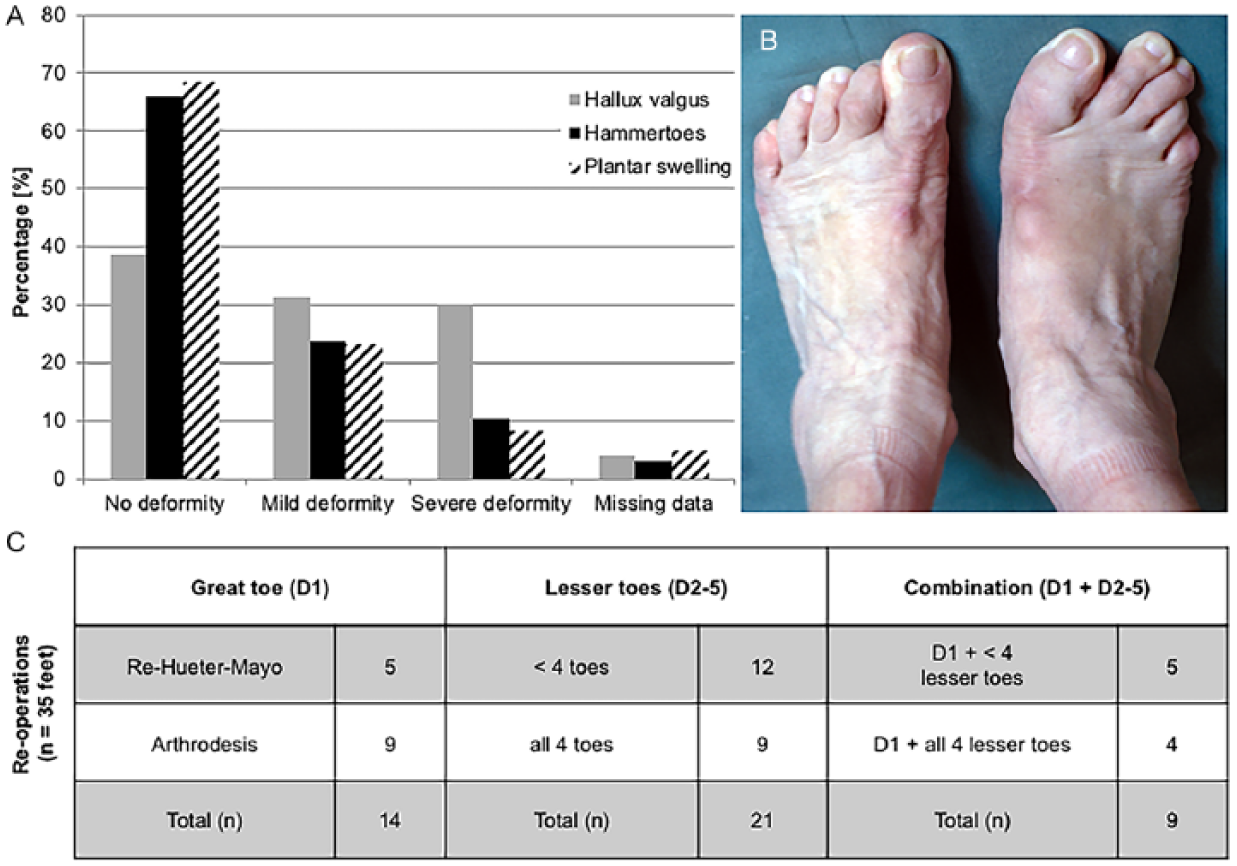
(A) Deformity relapses of the forefoot are demonstrated with bar graphs. No significant differences are identified. However, the fewest deformity relapses were documented for hammertoes and plantar swelling. Most mild and severe deformity cases were seen for the hallux valgus (hallux valgus angle 20 to 40 degrees and more than 40 degrees, respectively). (B) Image demonstrating a severe hallux valgus relapse with hammertoes for digits 4 and 5. (C) Table demonstrating the number of reoperations (n = 35 feet) of the great toe (D1) and the lesser toes (D2-D5), including their combinations in a total of 26 patients. Some patients underwent a revision Hueter-Mayo procedure for the great toe (n = 5), whereas 9 others had a metatarsophalangeal I arthrodesis due to the relapse. The operations for the lesser toes are separated according to whether they involved all 4 or fewer than 4 lesser toes. The combinations of great and lesser toes (D1 and D2-D5) take into account both previous groups.
A total of 35 reoperations (35%) were necessary in 26 patients (43.3%) (Figure 6C). Reoperations were performed on average 10.5 ± 7.3 years after the primary operation. There were no significant differences in terms of patient satisfaction, pain, orthosis use, walking distances, or standing abilities in patients who had undergone reoperations, when compared with patients who had not required secondary surgery. The only significant difference recorded in the study was increased plantar swelling in cases of reoperations (P < .05). Breakdown of the reoperations demonstrated that the great toe needed it 14 times (revision Hueter-Mayo or MTP I arthrodesis). The lesser toes required further surgical therapy in 21 cases. These reoperations mostly addressed the remaining distal metatarsal bone (n = 19) and, to a lesser extent, the surrounding soft tissue (n = 6). Only 4 cases required a complete reoperation of the entire forefoot.
Twenty-five percent of the participants were very satisfied with the operation. Fifty-nine percent (50 participants) were satisfied with the operation. Six percent (4 participants) were not satisfied with the operation, and 10% (6 participants) selected the category “dissatisfied” on the 4-point Likert scale (Supplemental Figure 1).
Discussion
With an average follow-up time of 24.6 years, this study of forefoot reconstructions per Tillmann is the longest follow-up study of its kind. The main surgical aim of the Tillmann procedure for RA-associated forefoot disorder is pain reduction, regaining the ability to use conventional shoe wear, and maintaining the forefoot function. Although joint protection and/or maintaining interventions are now more frequently successful after the introduction of DMARD therapy, the metatarsal head resection of the lesser toes II to V remains the gold standard therapy for the severely deformed rheumatoid forefoot. 22 In contrast to the Tillmann procedure, the Stainsby operation uses a dorsal approach with several longitudinal incisions. 27 Instead of resecting the metatarsal heads, the Stainsby operation resects the base of the proximal phalanges and repositions the dislocated plantar plate beneath the metatarsal heads.1,3 It has been reported that the Stainsby operation results in good satisfaction rates, with 50% of participants in the study by Hassan et al being completely satisfied, and 34% of participants being satisfied with some reservations, while 20% of the participants still reported significant forefoot pain in a midterm follow-up of 32 months. 11 These respectable results were confirmed by other authors in short- to midterm follow-up studies. For example, Dodd et al, Matthews et al, and Queally et al concluded that the Stainsby operation provides effective pain relief, a reduction of skin callosities, correction of claw toe deformations, and overall improved forefoot function.7,19,24 However, long-term studies for this dorsal approach are currently not available.
The plantar approach of Tillmann with resection of the metatarsal heads investigated here might have a high revision rate of 35% but has an overall satisfactory outcome of 84% for all patients. The surgical plantar approach was well tolerated, even 20 or more years after the operation. 29 The reoperations mainly addressed relapses for recurring HV and, to a lesser extent, hammertoes or plantar callosities. Only minor bone issues (eg, edge smoothening, resections) regarding the lesser toes had to be readdressed, similar to previous evaluations by Tillmann himself. 29 Furthermore, the surgical procedures for HV and for the lesser toes have to be assessed separately, as the deformity of the great toe appears to be the least well-addressed part in the Tillmann procedure. Others, like Hassan et al, showed similar problems in addressing the HV by osteotomy and soft tissue reconstruction. 11 Others, such as Bass et al and Kadambande et al, advocate strongly for a primary arthrodesis of the MTP I joint due to increased stability of the MTP I joint and weightbearing possibility plus increased protection of the lesser toes after reconstructive surgery.1,16 In contrast, others support a combined osteotomy and soft tissue reconstruction and have had good results with that.1,16,18 In the authors’ experience, a mere osteotomy and soft tissue reconstruction should be limited to mild HV angles of less than 40 degrees with good redressing intraoperatively. However, in cases of severe joint deviations of 40 degrees or more of the HV angle, the authors suggest, with regard to the current results, primary arthrodesis of the MTP I joint in order to avoid deformity relapse. This opinion aligns with Bass et al and Whitt et al, who used a primary fusion technique for all HV in forefoot deformity surgery.1,34
The use of conventional shoes not only is important for patients but also is one of the surgical goals. This follow-up study shows that only about one-third of participants (36.7%) needed custom-made orthopedic shoes after the Tillmann forefoot procedure. Often, the need for special shoes is significantly increased after an operative correction of the rheumatoid forefoot. This happens especially after a resection arthroplasty of the first MTP joint, where between 45% and 91% of patients require special shoes. 5 In this study, the majority of patients (>60%) were able to wear conventional shoe wear. Bitzan and his colleagues had more than 90% of patients wearing ordinary shoes, but their follow-up was conducted only up to 90 months after surgery. 2 The ability to use a conventional shoe is important for patients’ quality of life, as it significantly improves their walking distances compared with barefoot walking.
Postoperative pain improvement is also addressed by other procedures.1,3,7,24 This follow-up study shows that 35% of patients were pain-free while approximately 40% of patients had pain under strain. This is most probably the limiting factor for the reduced barefoot walking distances for the larger part of the group. Even Tillmann described pain relief lasting only for a few years before the intensity increased again. 29 Therefore, the current results show even longer pain relief than expected. Other groups with similar surgical techniques have demonstrated a higher percentage of pain-free patients due to better plantar pressure distribution and deformity correction,2,33 but long-term follow-up results, such as those here, are not available. Other groups recently demonstrated good outcomes for joint-preserving arthroplasties similar to resection techniques, but likewise, long-term follow-ups are lacking.14,25,34 Nevertheless, HV and the lesser toes have to be properly addressed and positioned with each operative procedure in order to achieve long-term satisfactory outcomes.
One of the less satisfactory outcomes after Tillmann’s forefoot surgery is decreased forefoot function. Only a few patients were able to perform a 1-legged stand or even a 1-legged tiptoe stand, the latter even being challenging for a healthy, nonoperated patient. One reason may be progressive stiffness in the first MTP joint, which was already identified by Tillmann. 29 He not only described its stiffness, but also documented an increase in correction loss and a reduced walking capacity. In addition, the authors further believe that reduced gripping function of the lesser toes is a major cause of reduced forefoot functionality. The study has no data to support this claim, but surgical intervention of the lesser toes with osteotomies and soft tissue reconstructions, regardless of the surgical approach or method, reduces the length of the digits and hence the initial tension of the flexor tendons, which can cause loss of strength. Thus, forefoot function is the most difficult part to reestablish with any type of forefoot arthroplasty. Other techniques like modified metatarsal shortening offset osteotomies might achieve some improved clinical scores, but this technique also has some limitations, as seen in the range of motion. It is also lacking long-term follow-up.12,23 However, it seems a good option particularly in the time of newer RA therapeutic agents.
This study has some limitations. First, it is a retrospective study with a self-constructed patient-based questionnaire. This questionnaire specifically addressed the key points of forefoot reconstruction surgery, but it is not validated. The already-established questionnaires (eg, the Foot Function Index or the Foot and Ankle Disability Index) do not look at shoe wear, forefoot deformities, or the gripping/standing function of the toes. However, the authors attempted in a second step to retrieve validated outcome measures, but the attritional loss of patients precluded inclusion of the data in the final paper. Second, the study did not collect information regarding specific RA treatment regimens. Today, RA therapeutic agents are much more effective, and deformity of the forefoot is seldom as severe as it was 20 or more years ago. Nonetheless, there is an urgent need to identify long-term results of surgical treatments, particularly in the event of decreased numbers of deformities in RA cases, in order to keep surgical options and outcomes in mind for patients with poor responses to current drug treatments. Third, the postal survey resulted in a selection bias as only patients who had returned a questionnaire could be considered. As a result, a specific dropout analysis cannot be carried out. Trying to increase the participation level by contacting patients by telephone and/or offering to schedule an appointment at the hospital to complete the questionnaires did not raise participation numbers. For the majority of eligible participants, completing the questionnaire was too tiring or complicated due to various factors (eg, dementia, increased age—45 out of 46 patients were over the age of 80 years), and several patients simply showed no interest in participating in any sort of questionnaire. None of the eligible participants who were spoken to expressed any sort of general dissatisfaction with the operation. Also, the study lacks clinical follow-up examinations. However, the answers that were given by the relatively large sample size (having regard to the time that has elapsed since the surgeries) so long after the surgery was performed provide crucial and hitherto unknown insight for patients and surgeons alike who are considering this type of surgery.
Conclusion
In conclusion, this follow-up study of patients with RA more than 20 years after they had undergone forefoot reconstruction surgery as described by Tillmann demonstrates compelling long-term outcomes from the surgery. For instance, the procedure reduced pain at rest in more than 70% of patients, and more than 60% of patients could wear conventional shoes. Furthermore, patients had significantly increased walking distances with shoes compared with without shoes. The forefoot function remained difficult to assess, but the Tillman procedure continued to yield long-term satisfying results for basic standing functions in this particular group of patients. Overall, 20 years after having the Tillmann procedure, the overall patient satisfaction level remained high, with more than 80% of participants in this study being satisfied. These findings are of paramount importance as the Tillmann procedure remains a solid surgical option today for patients who are refractory to newer treatments.
The study was performed in accordance with the Declaration of Helsinki of 1975, as revised in 2000, and with ethical approval obtained from the local ethics committee of the Hamburg medical association (registration no. PV4826). All included patients gave written informed consent. No animal experiments were performed.
Supplemental Material
DS_10.1177_1071100719840814 – Supplemental material for Forefoot Reconstruction Following Metatarsal Head Resection Arthroplasty With a Plantar Approach—A 20-Year Follow-Up
Supplemental material, DS_10.1177_1071100719840814 for Forefoot Reconstruction Following Metatarsal Head Resection Arthroplasty With a Plantar Approach—A 20-Year Follow-Up by Maciej J. K. Simon, André Strahl, Haider Mussawy, Tim Rolvien, Robert F. Schumacher, Marcel Seller and Wolfgang Rüther in Foot & Ankle International
Supplemental Material
FAI840814-ICMJE – Supplemental material for Forefoot Reconstruction Following Metatarsal Head Resection Arthroplasty With a Plantar Approach—A 20-Year Follow-Up
Supplemental material, FAI840814-ICMJE for Forefoot Reconstruction Following Metatarsal Head Resection Arthroplasty With a Plantar Approach—A 20-Year Follow-Up by Maciej J. K. Simon, André Strahl, Haider Mussawy, Tim Rolvien, Robert F. Schumacher, Marcel Seller and Wolfgang Rüther in Foot & Ankle International
Footnotes
Acknowledgements
In honor of Professor Karl Tillmann (March 3, 1932-March 19, 2017), who established this surgical procedure in the rheumatoid deformed forefoot.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.