
Abstract
Background:
Localized nerve pain in the foot and ankle can be a chronic source of disability after trauma and has been identified as the most common complication following operative interventions in the foot and ankle. The superficial location of the injured nerves and lack of suitable tissue for nerve implantation make this pain refractory to conventional methods of neuroma management. We describe a novel strategy for management using processed nerve allografts to bridge nerve gaps created by resection of both end neuromas and neuromas-in-continuity.
Methods:
A retrospective review of a prospectively maintained database was performed of all patients who received a processed nerve allograft for treatment of painful neuromas in the foot and ankle between May 2010 and June 2015. Patient demographic and operative information was obtained, as well as preoperative and postoperative pain assessments using a conventional ordinal scale and PROMIS (Patient Reported Outcomes Measurement Information System) Pain Behavior and Pain Interference assessments. Twenty-two patients were identified, with postoperative pain assessments occurring at a mean of 15.5 months after surgery.
Results:
Neuromas of the sural and superficial peroneal nerves were the most common diagnoses, with 3-cm nerve allografts being used as the interposition graft in the majority of cases. Eight patients had end neuromas and 18 patients had neuromas in continuity. Analysis of paired data demonstrated a mean ordinal pain score decrease of 2.6, with 24 and 31 percentage-point decreases in PROMIS Pain Behavior and Pain Interference measures, respectively. All changes were significant (P < .002).
Conclusion:
The painful sequelae of superficial nerve injuries in the foot and ankle was significantly improved with complete excision of the involved nerve segment followed by bridging of the resulting nerve gap with a processed nerve allograft. This approach limits surgery to the site of injury and reconstitutes the peripheral nerve anatomy.
Level of Evidence:
Level IV, retrospective case series.
Introduction
Injury to superficial nerves in the foot and ankle can lead to painful sequelae that have a profound impact on patient quality of life. These nerve injuries are often the consequence of trauma or iatrogenic injury during operative interventions. In a recent report, Deng et al found neurologic injury to be the most common complication following ankle arthroscopy. 9 Despite the relative prevalence of these injuries, there is no clear consensus with regard to management. Operative strategies range from neurectomy or neurolysis to neuroma excision with mobilization and burial of the proximal nerve.5,6,22,23,28 Neurectomy and neurolysis have failed to yield durable pain relief, and extensive nerve mobilization for transposition and burial necessitates greater operative morbidity.6,19,29 An ideal approach would limit the operative field to the site of injury, simplify intraoperative decision making, provide durable pain relief, and offer the potential to restore sensation.
Experience with the use of nerve transfers to decrease neuroma pain in amputees has encouraged a novel approach to pain caused by injured nerves in the intact lower extremity. 25 We attempted to repair injured nerves rather than to hide the painful neuroma, based on the concept that a reinnervation target is the key to achieving reduced sprouting and increased axon size—hallmarks of a healed nerve. 15 As a second building block of this strategy, we resisted the sacrifice of an uninjured sensory nerve to serve as a donor graft. We hypothesized that pain associated with chronic neuromas and neuromas-in-continuity in the lower extremity could be effectively managed with resection of the involved nerve segment followed by nerve allograft reconstruction of the resulting gap. The purpose of this study was to evaluate the efficacy of this approach based on a comparison of prospectively collected pain assessments.
Methods
Patient Preoperative Evaluation
After obtaining a complete history and review of any prior operative reports, physical examination consisted of a peripheral pulse exam and documentation of all prior operative scars. Inclusion criteria for this study included lower extremity patients with a physical examination consistent with the point tenderness of localized nerve pain. Typically, patients had decreased sensation distal to the area of greatest tenderness, though the extent and character of this sensory loss was variable. All patients in this series responded to a 1 mL injection of lidocaine just proximal to the area of greatest tenderness. Temporary improvement of localized pain would obviate the need for any further tests. Lack of improvement would lead to a repeat office examination for reinjection in the area of the same nerve or the injection of an adjacent nerve with overlapping territory. Exclusion criteria for the study included a lower extremity without documented pulsatile blood flow or lack of symptom improvement with local anesthetic injection. Imaging with ultrasound or magnetic resonance imaging was not a critical component of the diagnostic evaluation.
Overall, 26 patients met inclusion criteria for the study. Mean age in the cohort was 46 (range 18-75). Mean follow-up time was 66±31 weeks.
Operative Technique
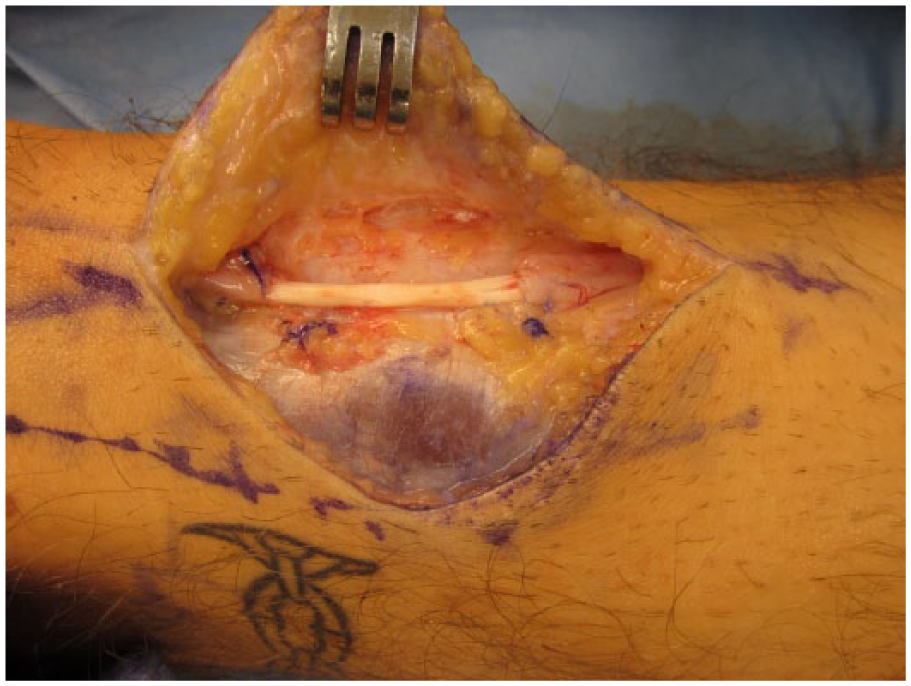
The area of greatest tenderness was marked carefully in the preoperative holding area. Typically, with the aid of a tourniquet, a 4- to 5-cm long incision was made to identify the target nerve. Palpation was critical for the procedure. Neuromas had a rounded feel like a soft marble, whereas neuromas-in-continuity were palpable as a mildly swollen and firm change in the character of the nerve immediately under the area of greatest tenderness. Dissection typically began a few centimeters proximal and distal to the area of greatest tenderness, and then went in each direction toward the damaged nerve segment (Figure 1). The neuroma was sharply resected back to healthy fascicles both proximally and distally. In most cases, the gap created was under 3 cm, with the nearest joint positioned in full extension. The gap was then reconstructed using an appropriately sized nerve allograft (Avance nerve graft, AxoGen Inc, Alachua, FL). The allograft was placed as an interposition graft and coapted end-to-end in a tension-free manner using 2 to 3 epineurial 7-0 polypropylene sutures placed under loupe magnification (Figure 2). The nerve repair was typically performed after any associated orthopedic procedures such as ankle arthroscopy, hardware removal, or Achilles tendon lengthening.

Neuroma-in-continuity of the sural nerve at the level of the lateral malleolus.
Nerve allograft placed as an interposition graft following complete resection of the involved sural nerve segment.
Postoperative Care
A splint was used to immobilize the nerve allograft in its soft tissue bed for 2 weeks. Temporary immobilization served to shield the repair from tension and encourage inosculation. Leg elevation, joint mobilization, and gentle compression were emphasized on splint removal. Preoperative neuroma pain was typically improved shortly after neuroma resection, and instead replaced with operative pain that was readily controlled with oral narcotics. After the initial 2 weeks, the patient could ambulate as tolerated.
Data Collection and Manuscript Preparation
The Northwestern University Institutional Review Board approved this retrospective review of a prospectively maintained database of consecutive patients who underwent reconstruction with a processed nerve allograft for management of a painful lower extremity nerve by the senior author (G.A.D.) between May 2010 and June 2015. Patient demographic and operative information was reviewed with particular emphasis on identification of the involved nerve, location of the neuroma, and the length of nerve allograft used. The electronic medical record was queried for preoperative information, medication use, complications, and follow-up information.
A standardized pain assessment was obtained for all patients on their initial presentation to the clinic with pain as a predominant symptom. The pain assessment included both an evaluation of maximum pain intensity on an accepted 0-10 ordinal scale (0 is no pain and 10 is the worst), as well as a validated assessment of pain behaviors and pain-related impairment of social and physical function (pain interference) using PROMIS (Patient Reported Outcomes Measurement Information System) instruments. The pain score and PROMIS assessments were performed at each postoperative visit. For patients with multiple postoperative pain reports, the postoperative pain scores obtained at the longest duration since surgery were used for comparison with preoperative scores.
PROMIS is a validated, NIH-supported set of instruments for measuring health status. The PROMIS Physical Function item bank has previously been reported to be superior to conventional outcome measurements for assessment of physical function in the foot and ankle patient. 13 In the case of the PROMIS Pain Behavior and Pain Interference item banks, questions delivered via an iterative algorithm rapidly assess the effect of pain on a patient’s behavior and daily function, respectively. PROMIS outcomes are reported as T-scores, which have a population mean of 50 and standard deviation (SD) of 10. Importantly, the raw score can be easily translated into a percentile corollary, which enables comparison between the subject’s score and those harvested from a 21 000-person control population representative of the US general population. As such, the PROMIS tools provide an easy means for comparison not only across an intervention, but also against age and sex-matched controls. While the minimum clinically important difference (MCID) for the pain behavior and interference instruments have not been determined, the MCID for the majority of PROMIS instruments has been set at 0.5 SD or T-score value of 5.3,21,26 PROMIS is not a disease-specific outcomes tool.
The 2 instruments utilized in this study determined different aspects of pain on a patient’s life. The PROMIS Pain Behavior instrument is designed to assess behaviors that would indicate to others that a patient is experiencing pain, such as wincing, crying, or verbal reports of pain. The Pain Interference instrument assessed the effect of pain interfering with social and recreational activities, as well as sleep.
Data analysis was performed with SPSS Statistics (IBM Corp, Armonk, NY). Pre- and postoperative PROMIS behavior and interference scores, as well as ordinal pain scores, were compared using the Wilcoxon rank-sum test. Regression analysis was performed to determine if there were any significant predictors of decreased pain score of any type.
Results
Preoperative Data
Mean preoperative pain score on the ordinal pain scale was 7.5. In terms of the PROMIS pain assessment, the mean preoperative pain behavior T score was 63, with a mean pain interference T score of 68. This translates to mean population percentile scores of the 88th and 92nd percentiles, respectively. It follows that these patients had multiple interventions for pain. At the time of the preoperative pain assessment, 22 patients (85%) were actively seeing a pain specialist for management of their pain. Seventeen patients (65%) were taking over-the-counter pain medications and 13 patients (50%) were taking prescription medications for pain control. Thirteen patients (50%) had undergone a previous operative procedure intended to address their pain, with 2 patients having undergone multiple procedures. Of these 13 patients, 4 underwent prior neurolysis and 2 underwent a previous neurectomy. The remaining 7 patients had undergone nonneurologic procedures in an attempt to address their pain.
Intraoperative Data
All patients in the study underwent excision of the involved nerve segment and immediate nerve repair with a processed nerve allograft. Nerves repaired were sural (10), superficial peroneal (9), common digital nerve (5), deep peroneal (1) and lateral plantar nerve (1) (Figure 3). There were 8 end-neuromas and 18 neuromas-in-continuity. The diagnosis of neuroma was confirmed histologically in all cases. Length of graft used was most commonly 3 cm (14 patients), with a mean length of 3.3 cm and a range of 1 to 6 cm. Concurrent procedures were performed in 9 patients, including a tarsal tunnel release in 3 patients, 3 ankle arthroscopies, 1 midfoot arthrodesis, 1 Achilles tendon lengthening, and 1 transposition flap for soft tissue coverage. Mean operative time for the neuroma treatment portion of the case was 95 minutes.
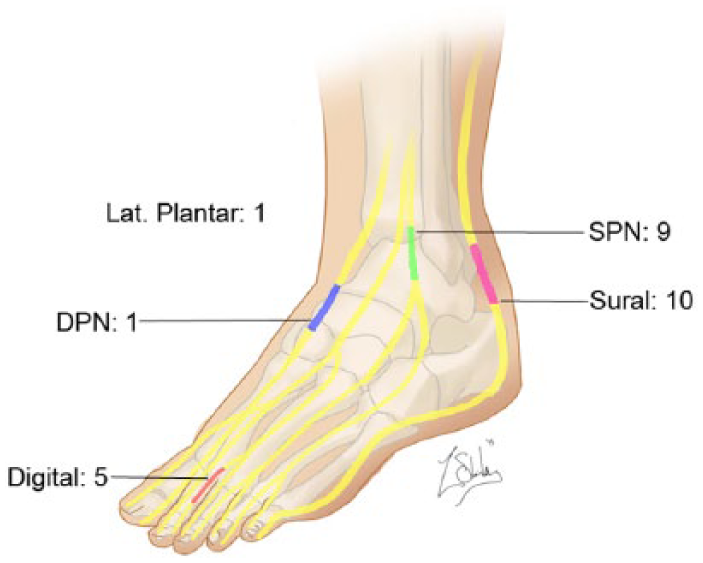
Distribution and number of nerves treated. Twenty-six nerves were treated, but only the 22 patients had follow-up data sufficient to be included in the final analysis.
Postoperative Data and Operative Outcomes
There were no operative site complications. Overall, 22 patients had adequate follow-up (defined as 6 months or more) for postoperative ordinal and PROMIS pain assessments (Table 1). Postoperatively, there were significant decreases in ordinal pain scores (Figure 4), as well as pain behavior and interference scores (Figure 5). Ordinal pain scores decreased by a mean of 2.6 points (range +2 to −8). Pain behavior T score decreased by 7.3 (range +2 to −22), a mean percentile decrease of 24%. Pain interference T score decreased by a mean of 11.3 (range +2 to −27) with a mean percentile change of 30.7% (Figure 5). All changes were significant with P < .003. No single variable was a significant predictor of decrease in any type of pain score on regression analysis. There were no significant differences in the treatment of end neuromas and neuromas-in-continuity. There were no differences in outcomes between the different nerves treated. There were also no differences in outcomes between patients who had prior operative treatment or no previous surgeries. Mean postoperative pain scores were an ordinal pain score of 5, behavior raw score of 56 (64th percentile), and interference raw score of 57 (percentile 62th).
Individual Patient Data: Nerve Location, Neuroma Type, Prior Nerve Surgery, Graft Length, and Change in Pain Outcomes.
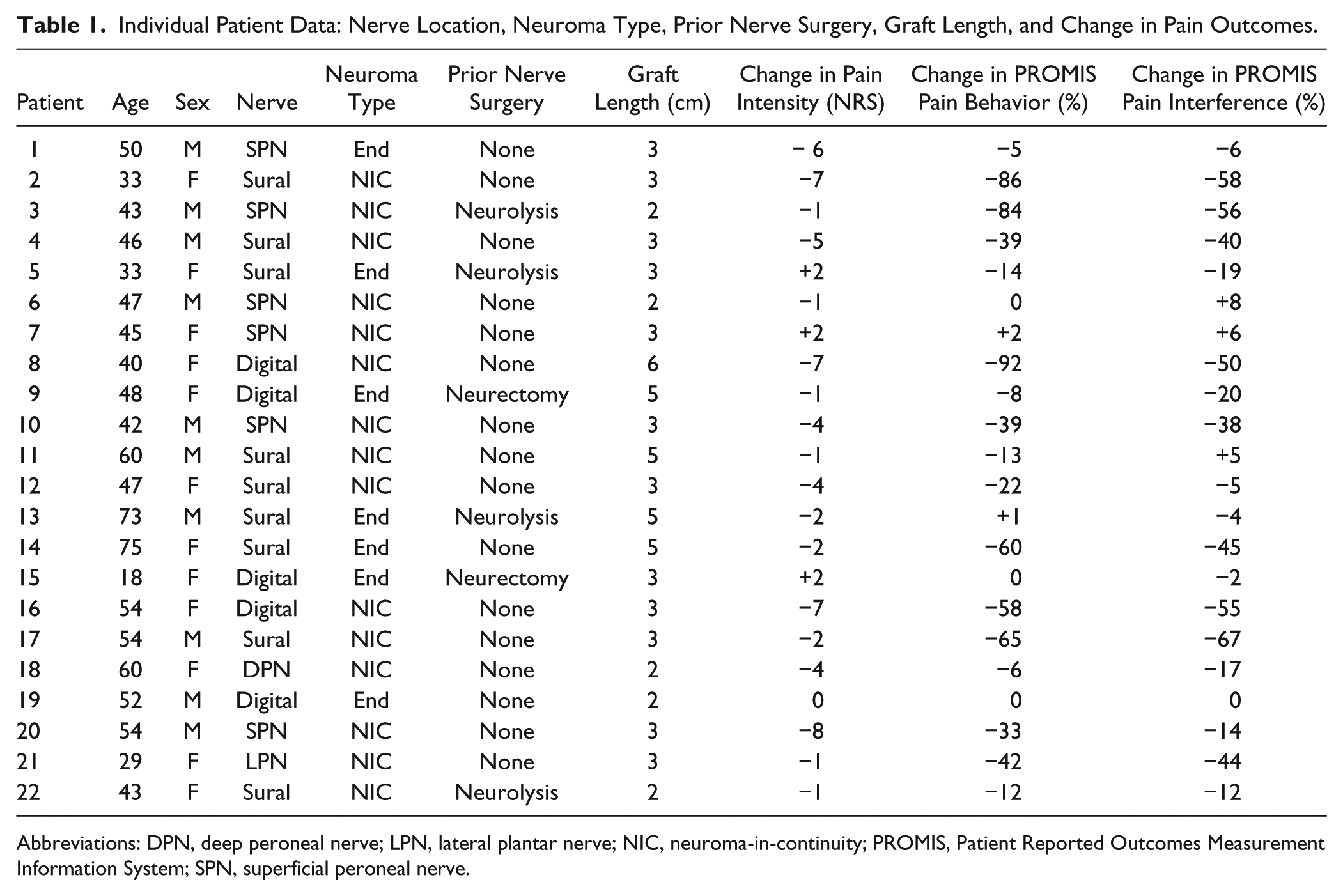
Abbreviations: DPN, deep peroneal nerve; LPN, lateral plantar nerve; NIC, neuroma-in-continuity; PROMIS, Patient Reported Outcomes Measurement Information System; SPN, superficial peroneal nerve.
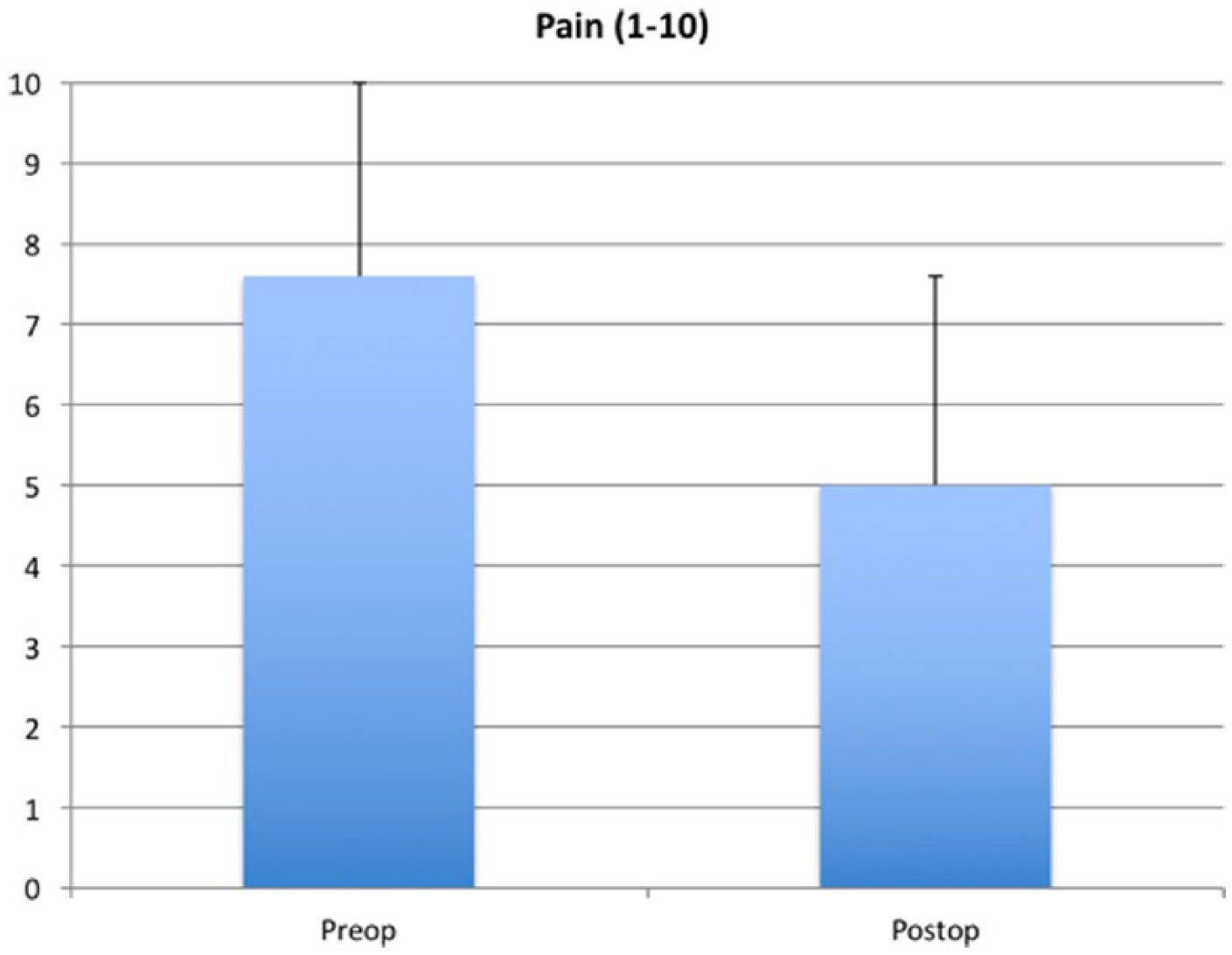
Change in mean ordinal pain score after neuroma excision and gap repair with processed allograft (P = .016; N = 22 patients).
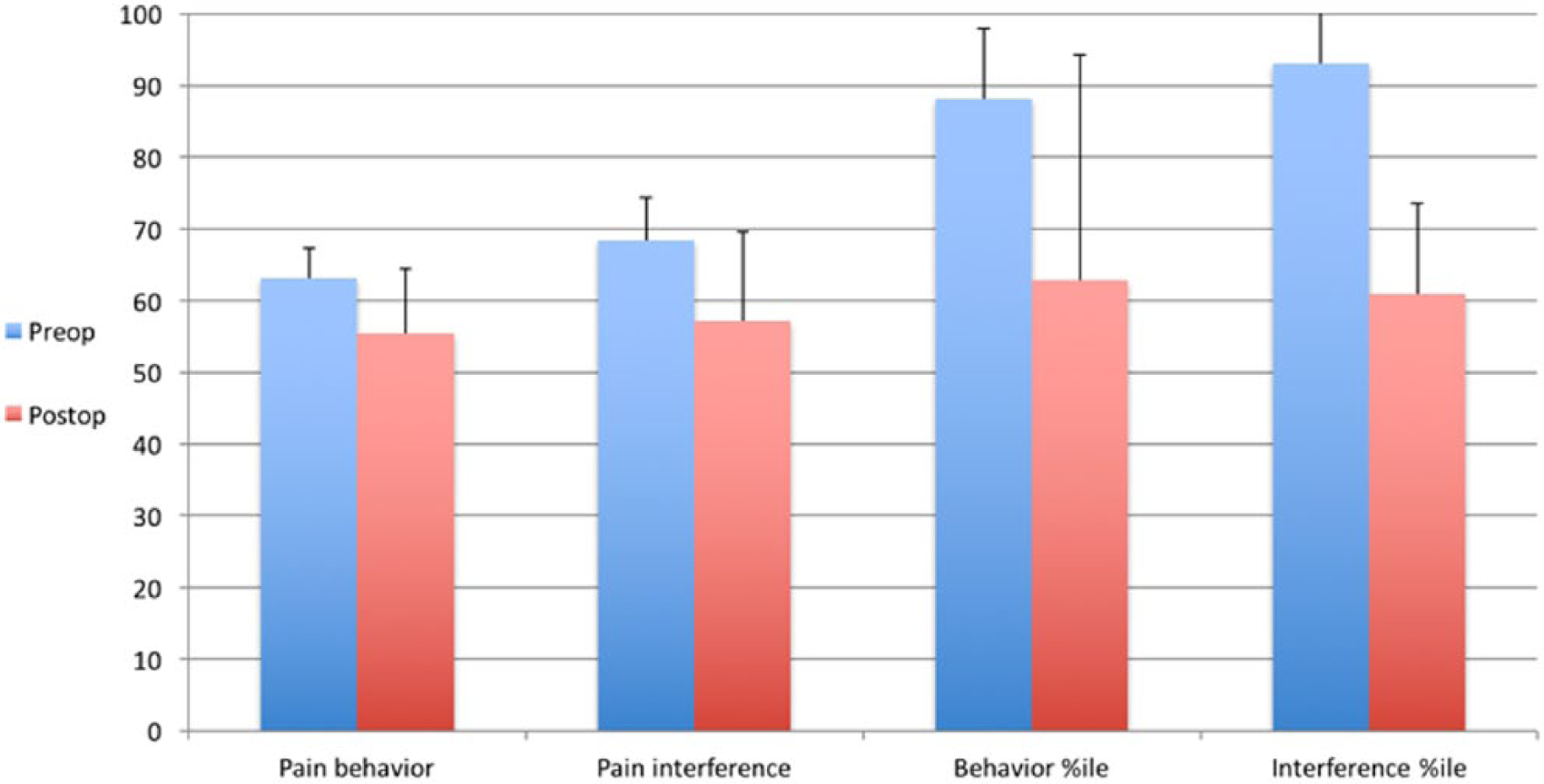
Change in PROMIS pain behavior and interference T scores after neuroma excision and gap repair with processed allograft. Percentile ranks are compared to total population. All differences significant, P < .006; n = 22 patients.
Repeat Procedures
One patient, with a neuroma-in-continuity of the tibial side digital nerve of the great toe had a repeat procedure to treat a recurrence of local neuroma pain. In this patient, a new neuroma developed at the proximal allograft coaptation site, and no nerve fascicles were found on histology within the allograft. It was suspected that the previous neuroma resection had not extended sufficiently proximal to enable allograft coaptation with healthy nerve fascicles. In the revision, an autogenous motor nerve branch to the vastus lateralis muscle was used as a graft to span the 5-cm gap of the re-resected neuroma and failed nerve allograft. Follow-up in this patient was not sufficient to be included in this manuscript.
Discussion
Localized nerve pain has received increased attention as a source of chronic disability after trauma. It has also been identified as the most common complication following orthopedic and podiatric interventions in the foot and ankle. 9 The mixed training backgrounds of providers managing these conditions and the lack of a single reliable treatment method has led to significant variability in management. All management strategies are challenged by the superficial location of the injured nerves and the constant pressure applied by shoe wear. The lack of a simple and standardized treatment algorithm has often relegated these patients to pain management clinics.
End neuromas have traditionally been treated with excision and burial of the nerve ending in tissues thought to either inhibit new neuroma formation or to render the recurrent neuroma less susceptible to movement and pressure.7,8,17 In comparison, neuromas-in-continuity represent a quandary in management, as resection requires sacrifice of any residual distal innervation. Many advocate neurolysis or nerve wrapping in these situations, but neither technique effectively ameliorates dysfunction due to intraneural scarring.2,10,11,18,22-24
The treatment of painful neuromas outlined in this study is guided by laboratory evidence demonstrating cessation of sprouting and evidence of coordinated regeneration when the proximal nerve is provided with a reinnervation target. 15 In contrast, there is histologic evidence of neuroma recurrence with techniques that fail to provide the proximal nerve with “somewhere to go and something to do.”8,16 This management strategy was also encouraged by a recent clinical report demonstrating improved pain outcomes when nerve grafting was performed in favor of neurectomy or nerve burial. 12 Unlike other treatments for foot and ankle neuroma pain, only nerve graft repair offers the potential for coordinated axon regeneration into a denervated bed. Although there have been sporadic case reports citing favorable pain outcomes after autologous nerve grafting, our use of nerve allografts avoids the potential for new painful loci from autogenous nerve graft harvest.2,14 To simplify intraoperative decision making and effectively eliminate intraneural scarring, neuromas in continuity are resected back to healthy nerve fascicles, in comparable fashion to the management of end neuromas. Comprehensive resection is justifiable, on account of the “non-critical” nature of the involved nerves. Though sensory outcomes were not recorded in this study, the available evidence suggests that allograft reconstruction yields reliable sensory recovery when performed for small to moderate nerve gaps.4,20,30 Likewise, the morbidity of resection is further diminished by sensory recovery because of collateral sprouting from adjacent nerves.1,27
The reconstructive component of this approach required an additional direct cost for the nerve allograft material. However, this cost was largely offset by avoidance of the additional operating room time, physician time, and anesthesia time that accompany techniques that require more extensive dissection or nerve autograft harvest. Resection of the scarred nerve segment with allograft reconstruction was fast and straightforward, as evidenced by a mean operative time of 95 minutes. The procedure did not require special instrumentation or the use of a microscope. Furthermore, preoperative evaluation minimized the use of costly imaging and relied chiefly on patient history, physical examination, knowledge of anatomy, and the use of diagnostic nerve blocks.
This review of prospectively collected pain data suggests that use of the described nerve allograft technique yields a statistically significant and clinically important improvement in pain symptoms. The PROMIS data collected also provides important insights into the degree of impairment experienced by patients with neuroma pain in the foot and ankle. It is noteworthy that at the time of presentation to our clinic, the patients in this cohort experienced a degree of impairment that ranked in the 88th percentile for pain behavior and 92nd percentile for pain interference. As a point of comparison, patients presenting to the same senior surgeon for carpal tunnel surgery over a similar time period exhibited a mean pain behavior score in the 64th percentile and pain interference score in the 62nd percentile. On presentation to our outpatient clinic, most foot and ankle patients were actively followed by a pain specialist. The majority of patients were taking prescription pain medications, and half had previously undergone at least 1 operative procedure for management of their pain.
Pain is frequently an elusive outcome to measure. Given the relative novelty of the PROMIS pain assessments, we included a commonly used ordinal scale to serve as a legacy measure of pain intensity. Our technique yielded a significant improvement in pain intensity, which lends credence to the benefits identified by PROMIS. While PROMIS offers many insights, it is not a disease-specific instrument. As a result, pain outcomes can be negatively affected by confounding sources of pain that are unrelated to the nerves managed with this procedure. All of the patients in this series sustained nerve injuries as a result of trauma or iatrogenic causes, and thus had a high incidence of additional lower extremity pathology. The fact that PROMIS provides a holistic measure of pain, rather than isolating nerve-related pain, makes the significant reduction in pain behaviors and pain-related impairment in this group of patients all the more impressive.
This study is not without its limitations. Although the data were collected prospectively, the study design and chart review were retrospective and thus susceptible to the inherent biases introduced by a retrospective study. Likewise, the retrospective design of this study means that potentially useful preoperative data, such as a standardized preoperative sensory evaluation, could not be performed. Early in the study period, the senior surgeon’s efforts to measure sensory thresholds yielded such marked variability that thorough sensory examination was abandoned as a component of the preoperative evaluation. As a result, the extent of sensory recovery following allograft reconstruction was not studied. As mentioned above, collateral sprouting from adjacent nerves would further confound any objective measurement of sensory recovery. Still, it cannot be excluded that pain improvement is in some way related to the material properties of the nerve allograft rather than to coordinated nerve regeneration, as we hypothesized. Additionally, while lengthy follow-up duration is the ideal, the moderate size of the nerve gaps reconstructed in this series make a mean follow-up of almost 16 months sufficient to enable identification of neuroma recurrence. Perhaps the greatest limitation of this study is the absence of an alternative technique for comparison. However, our prior experience with conventional techniques was marked by unfavorable pain outcomes. Unfortunately, these patients pre-dated the standardized pain assessments used in this study.
Conclusion
In summary, in properly selected patients, painful sensory nerve neuromas of the lower extremity were improved with excision of the damaged nerve and grafting using processed nerve allograft. We found a statistically significant decrease in patient-reported pain at an average of 15.5 months after operative intervention.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.