
Abstract
The COVID-19 pandemic has led to the introduction of unprecedented safety measures, one of them being physical distancing recommendations. Here, we assessed whether the pandemic has led to long-term effects on two important physical distancing aspects, namely interpersonal distance preferences and interpersonal touch behaviors. We analyzed nearly 14,000 individual cases from two large, cross-cultural surveys – the first conducted 2 years prior to the pandemic and the second during a relatively stable period of a decreased infection rate in May-June 2021. Preferred interpersonal distances increased by 54% globally during the COVID-19 pandemic. This increase was observable across all types of relationships, all countries, and was more pronounced in individuals with higher self-reported vulnerability to diseases. Unexpectedly, participants reported a higher incidence of interpersonal touch behaviors during than before the pandemic. We discuss our results in the context of prosocial and self-protection motivations that potentially promote different social behaviors.
Keywords
As the SARS-Cov-2 virus is mainly transferred via the droplet route (Jin et al., 2020), person-to-person transmission occurs primarily through close interpersonal contact and depends on social contact patterns (McGrail et al., 2020; Sorokowska, Saluja, Kafetsios, et al., 2022). Hence, health organizations and governments worldwide followed the recommendation of the World Health Organization (WHO, 2021) to restrict this risk by the so-called “social distancing” policy involving, among others, increased interpersonal distance and reduced touch behaviors (ECDCfor, 2020a, 2020b; Pedersen & Favero, 2020; WHO, 2021). Although many research articles point to the potential risks of insufficient interpersonal contacts and touch deprivation for private life (e.g., Durkin et al., 2021; Field et al., 2020) and for both mental and physical health (e.g., Deliktas Demirci et al., 2021; Rosen et al., 2020) it is yet to be explored whether the COVID-19 pandemic has led to a long-lasting reduction in interpersonal touch and an increase of interpersonal distance.
Both interpersonal distance and interpersonal touch are essential elements of our daily social lives. An interpersonal distance preference marks the space at which two people are comfortable talking to one another. This preferred distance varies greatly across individuals, social relationships, and cultures (Sorokowska et al., 2017). For example, early research showed a range between 0.46 to 3.7 m for non-intimate contexts, and this range depended on the interaction partner, with a smaller distance for family or close friends than for strangers (Hall, 1966). A worldwide study conducted several years before the COVID-19 pandemic revealed a mean distance of 1.35 m for strangers, 0.92 m for acquaintances, and 0.32 m for close friends (Sorokowska et al., 2017). In the context of the pandemic (ongoing at the time of writing this article), it should be noted that the distances for friends and acquaintances are considerably lower than the 1.0 (WHO, 2021) to 1.5 m (RKI, 2021) social distancing guidelines. Studies suggest that the SARS-CoV-2 infection risk gradually increases with social distances below 1 m (Chu et al., 2020), and less social distancing predicts a higher likelihood of a COVID-19 infection in 4 months (Fazio et al., 2021).
Interpersonal touch is a prevalent behavior in social interactions which involves a direct contact between the bodies of two individuals, and thus a considerable reduction in interpersonal distance. Touch behaviors vary in the degree to which they convey intimacy and consequently can be classified as affectionate (such as an embrace or a stroke) or non-affectionate (a handshake or a casual, non-intentional touch). Our Global Survey showed that 80% of individuals used affectionate forms of touch at least once a week prior to the COVID-19 pandemic to interact with their friends (Sorokowska, Saluja, Sorokowski, et al., 2021). For strangers, touch is more prevalent in non-affectionate forms. Before the COVID-19 outbreak, between 51% and 97% of participants (depending on the country of origin) reported using such types of touch at least once a week (Sorokowska, Saluja, Kafetsios, et al., 2022). The latter result is important in the context of the COVID-19 pandemic, because variation in the early dynamics of the SARS-CoV-2 spread is, among other factors, significantly and positively related to non-affectionate touch behaviors between strangers (Sorokowska, Saluja, Kafetsios, et al., 2022). Thiebaut et al. (2021), for instance, showed that people vulnerable to diseases avoided social touch more than those less vulnerable to diseases and that this association was stronger during the COVID-19 pandemic than a few months before.
Mirroring social patterns of interpersonal distancing, interpersonal touch varies with relationship closeness, with higher touch frequency toward close versus other interaction partners (Beßler et al., 2020). This result fits the enhanced risk of contamination with new pathogens when interacting with people outside the core group. To counteract the risk of disease, humans have a set of innate tendencies that motivate them to behave more carefully towards unknown, and potentially infectious people. This behavioral immune system (BIS) is motivated by disgust and includes protective behaviors, such as increasing interpersonal distance, washing hands, or avoiding touch (Schaller & Park, 2011; Thiebaut et al., 2021). One’s individually perceived vulnerability to disease (PVD; Duncan et al., 2009) moderates the activation of BIS. For instance, the feeling of being ill at a given time point predicts infection-preventative behavior for several weeks (Miller & Maner, 2011). During the COVID-19 pandemic, disgust sensitivity and PVD increased (Stevenson et al., 2021) and were related to individual concerns about COVID-19 (Shook et al., 2020) and to contact with information about the pandemic (Ackerman et al., 2021).
Currently, the COVID-19 pandemic has persisted for almost 3 years, as have attempts to mitigate its extent and the contagion speed in community settings. Hence, it is plausible that the official social distancing recommendations observed in almost every country during this pandemic and the immediate disease threat arising from ignoring these recommendations may have changed habitual, social distancing-relevant behaviors in humans. We assumed that this change of habits would be observable even in periods of relatively low global numbers of reported COVID-19 incidents. Our previous Global Survey conducted between 2016 and 2018 allowed us to capture a certain “baseline level” of interpersonal behaviors, and thus we recollected comparable data on social distancing behaviors in various countries during the pandemic, i.e. in May/June 2021.
We hypothesized that a) touch prevalence would decrease and preferred interpersonal distance would increase in 2021 compared to reports collected before the COVID-19 outbreak, and b) that this difference would be especially salient for behaviors towards more distant social relations. Furthermore, we hypothesized that c) self-assessed vulnerability to disease would negatively predict touch frequency and positively predict interpersonal distance preferences during the COVID-19 pandemic, and that these effects would be stronger for behaviors toward more distant social relations.
Materials and Methods
The project was preregistered on the AsPredicted website (https://aspredicted.org/PAI_VSM) and all data for this project are available at https://osf.io/cz2pv/?view_only=0ba613b14216432ead3cc3019b20afb4.
Participants
Our research comprised two studies. During study/wave I (referred to as the Global Survey), participants from 45 countries took part in a large, cross-cultural research project comprising studies on interpersonal distancing and touch behaviors (Sorokowska, Saluja, Kafetsios, et al., 2022; Sorokowska, Saluja, Sorokowski, et al., 2021) as well as on several other psychological concepts (Conroy-Beam et al., 2019; Kowal, Sorokowski, et al., 2020; Sorokowska, Saluja, Sorokowski, et al., 2021). As the touch part was not completed in every country and the analysis of this survey part was only performed for participants who reported having met their respective interaction partner in the week preceding data collection, the total sample in the current research included 8147 individuals (age range = 15–75, M = 28.85, SD = 10.80, 45.4% females) from 24 countries.
The second study/data collection wave (hereafter referred to as the COVID-19 Survey), was conducted between May and June 2021. We invited each researcher who contributed to the previous touch study to take part in this new data collection, resulting in data collected from 5716 individuals (age range = 15–96, M = 34.28, SD = 13.13, 66.5% females) from 24 countries.
Materials
Interpersonal Distance Preferences
We surveyed interpersonal distance preferences with a scale designed for the purpose of our previous cross-cultural studies (Sorokowska et al., 2017; Sorokowska, Saluja, Sorokowski, et al., 2021). In short, participants are asked to rate the physical distance from another person at which they feel comfortable during various interactions in a task comprising two silhouettes and a visual scale ranging between 0 and 220 cm (0–86.6 in). In both data collection waves, we asked participants about their preferred distance to male and female strangers, male and female acquaintances, and to male and female close persons (friends or relatives). The COVID-19 Survey additionally included a question about preferred distance to a romantic partner, but this was not analyzed in the current study to ensure that data from the two data collection waves were comparable.
Touch Questionnaire
We surveyed interpersonal touch behaviors using a Touch Questionnaire designed for this purpose in our Global Survey (Sorokowska, Saluja, Sorokowski, et al., 2021). This questionnaire contains six icons presenting four affectionate (embrace, caress/stroke, kiss, and hug) and two non-affectionate touch behaviors (casual physical touch, handshake), as guided by (Hall, 1966). Verbal descriptors for each touch behavior aid the icon interpretation. For each touch behavior, participants answer the question, “have you performed this type of touch in the last week?”, referring in each case to six different interaction partners (male and female strangers, male and female friends, romantic partner, and youngest child). We used a “yes-no” answering format in both data collection waves because of its simplicity, cross-cultural understandability and salience in memory.
Perceived Vulnerability to Disease Scale (PVD)
In the COVID-19 Survey, the participants additionally answered the Perceived Vulnerability to Disease Scale (Duncan et al., 2009), a brief 15-item scale comprising questions on self-assessed proneness to diseases (Infectability subscale) and willingness to avoid various pathogens (Germ Aversion subscale) (for psychometric properties please compare Díaz et al., 2016). The responses are provided on a scale ranging from 1 – “strongly disagree” to 7 – “strongly agree”.
Procedure
As mentioned above, our research comprised two separate data collection waves – the Global Survey (wave I), and the COVID-19 Survey (wave II), both described in more detail below.
The Global Survey
The Global Survey was conducted between 2016 and 2018 in 45 countries. Researchers in the respective countries invited participants to take part in a study on several psychological constructs. This paper-and-pencil survey was distributed among community members and university students (with a maximum of 50% students per sample per country) aged between 15 and 75 years. The survey was presented in local languages, translated and back-translated from the original English version by local researchers.
COVID-19 Survey
Researchers from the Global Survey who took part in the study on interpersonal touch were invited to a follow-up study on interpersonal behaviors during the COVID-19 pandemic. They received the English version of the questionnaire and translated it into their native language using the translation – back-translation procedure. Afterwards, we implemented the local language forms in an online research platform (Qualtrics) and the local researchers tested and approved the final version prior to data collection. Thereafter, every researcher received a personalized link to be locally distributed to participants. The requirement was to work primarily with community samples (mirroring the Global Survey procedure, the total percentage of students in each country was not to exceed 50%).
The Ethics Committee of the Institute of Psychology, University of Wroclaw, approved both data collection waves and the local researchers also obtained additional permits wherever this was legally required. The participants were informed about the anonymity and voluntary nature of the study and provided informed, written consent before data collection. The study was preregistered on the AsPredicted website (https://aspredicted.org/PAI_VSM).
Statistical Analyses
Data Preprocessing
We merged the COVID-19 Survey dataset with the already pre-processed Global Survey dataset (Sorokowska, Saluja, Sorokowski, et al., 2021). In order to provide a valid basis for data analysis, we removed all data from countries with less than 70 valid overall cases. We compared the sex and age distribution between both datasets and found that the population in the COVID-19 Survey was older than in the Global Survey (Global Survey: 28.7y+/−10.8; COVID-19 Survey: 34.3y+/−13.1y; t [119,668] = 69.4: p < 0.001; d = 0.48). We also observed a significantly different sex distribution (p < 0.001). Age and sex were thus controlled for in mixed models (see Data analysis).
Variables
Interpersonal Distance Preference
We first computed a mean preferred interpersonal distance index collapsing across all interaction partners for each data collection wave. Overall internal consistency was found to be α = .942 for interpersonal distance preference (6 items).
Affectionate Touch Behavior
We analyzed affectionate touch behavior separately for each of the affectionate touch types (embrace, stroke, kiss, hug) with each interaction partner (partner, male friend, female friend, male stranger, female stranger, youngest child). On an individual-level this variable had only two values – “yes”, meaning that a person performed a given touch type, or “no”, meaning that a person did not perform the given touch behavior type in a given relationship. These values were re-coded to percentages (0% or 100% for a certain touch type in a given relationship). Overall internal consistency was found to be α = .880 for affectionate touch behavior (24 items).
Non-Affectionate Touch Behavior
Furthermore, we analyzed non-affectionate touch behaviors separately for the two non-affectionate touch types (casual physical contact, handshake) with each interaction partner (partner, male friend, female friend, male stranger, female stranger, youngest child). Mirroring the affectionate touch behavior assessment, non-affectionate touch behavior had only two responses – “yes”, meaning that a person performed a given touch behavior, or “no”, meaning that a person did not perform the given touch behavior in a given relationship. These values were re-coded to percentages (0% or 100% for a certain touch type in a given relationship). Overall internal consistency was found to be α = .784 for non-affectionate touch behavior (12 items).
Affectionate and Non-Affectionate Touch Diversity
We also analyzed a more fine-tuned index of touch behaviors focusing on the range of used touch behavior types, i.e., Affectionate Touch Diversity Index. Affectionate and non-affectionate Touch Diversity was operationalized as a percentage of the possible touch behavior types used by an individual in each interaction. Thus, values for this index for the affectionate touch could be 0% (no touch in the last week within the respective relationship type), 25%, 50%, 75% (one, two, or three types of touch behavior, respectively) to 100% (i.e., an individual used all types of touch behavior – hug, stroke, embrace and kiss – in the last week within the respective relationship type). For the non-affectionate touch diversity the values of this variable could be 0% (no non-affectionate touch behavior used), 50% (one type of touch behavior used), or 100% (both casual physical contact and handshake used – in the last week within the respective relationship type; see Sorokowska, Saluja, Sorokowski, et al., 2021). Overall internal consistency was found to be α = .783 for affectionate touch diversity (6 items) and α = .785 for non-affectionate touch diversity (6 items).
Perceived Vulnerability to Disease
Perceived Vulnerability to Disease was operationalized as a mean score in the PVD Scale (Duncan et al., 2009).
Data Analysis
To test hypotheses a and b on the possible increase in all social distancing aspects during the COVID-19 pandemic, we conducted three separate analyses using SPSS version 27. Two generalized linear mixed (GLM) models were computed separately for affectionate touch behaviors and non-affectionate touch behaviors. These models included interaction partner (6 levels: partner, male friend, female friend, male stranger, female stranger, youngest child), time of data collection (2 levels: the Global Survey, the COVID-19 Survey), sex and age as fixed factors, and each of the affectionate touch types (4 subscores: embrace, stroke, kiss, hug) or the non-affectionate touch types (2 subscores: casual physical contact, handshake) as dependent variables, respectively. As the touch was indicated as an alternative variable (yes, no), we computed a binary logistic regression model. All main effects and the two way interaction wave-by-interaction-partner were modeled. The participant`s country was added as a random effect. The residual method was used with model based covariances.
This approach deviates from the preregistration in two cases: First, we did not analyze the general touch prevalence and touch degree indices, which are both computed out of the alternative answer to each of the 4 affectionate or 2 non-affectionate touch types (see Sorokowska, Saluja, Sorokowski, et al., 2021). Instead we decided to include the answers to each affectionate and non-affectionate touch type of those items separately into the GLM to make full use of the data. Second, we decided to run the GLM instead of t-tests. This was needed as the t test does not allow for the inclusion of potential covariates. As our samples from the two surveys differed in age and sex distribution, this correction was needed. We tested whether the results between the pre-registered (t test) and the new statistical approach (GLM) differ and we did not observe a significant result in one approach that did not hold in the other.
Further, a two-way ANOVA was computed to examine interpersonal distance preferences. The ANOVA included interaction partner (6 levels: close female/close male/female acquaintance/male acquaintance/female stranger/male stranger) and wave of data collection (2 levels: pre-/during COVID-19) as factors, and interpersonal distance preference as the dependent variable. In all analyses, interaction effects were assessed between interaction partner*time of data collection.
To test hypothesis c, we focused on the Perceived Vulnerability to Disease (PVD) scores. Therefore, we computed Pearson’s correlation coeffcients to assess the relationship between interpersonal distance preference and PVD across the whole sample. We then computed Pearson’s correlations between the mean country values of interpersonal distance preference and mean country values of PVD. Furthermore, we computed Spearman’s correlations between affectionate and non-affectionate touch diversity with PVD. Correlations were performed for each interaction partner. Bonferroni correction was used for all comparisons.
Results
Changes in Interpersonal Distance Preference, Affectionate Touch, and Non-Affectionate Touch Behaviors During the COVID-19 Pandemic
Across all interaction partners, interpersonal distance preferences increased by an average of 54.27% during the COVID-19 pandemic (Global Survey: 61.21 cm, SD = 38.08; COVID-19 Survey: 94.43 cm, SD = 52.31). This result was observed in all participating countries (Supplementary Table S7). Hence, there was a significant main effect of data collection wave (F(3,21,340) = 1214.7; p < 0.001). The interaction effect of interaction partner*data collection wave was not significant (F(3,21,340) = 0.2; p = 0.90), implying the differences between collection waves were similar for close and more distant social interactions (Figure 1). Interpersonal distance preferences increased during the COVID-19 pandemic. Differences in interpersonal distance preferences between the Global Survey, conducted between 2016 and 2018, and the COVID-19 Survey, conducted in 2021. Means and standard deviations are displayed.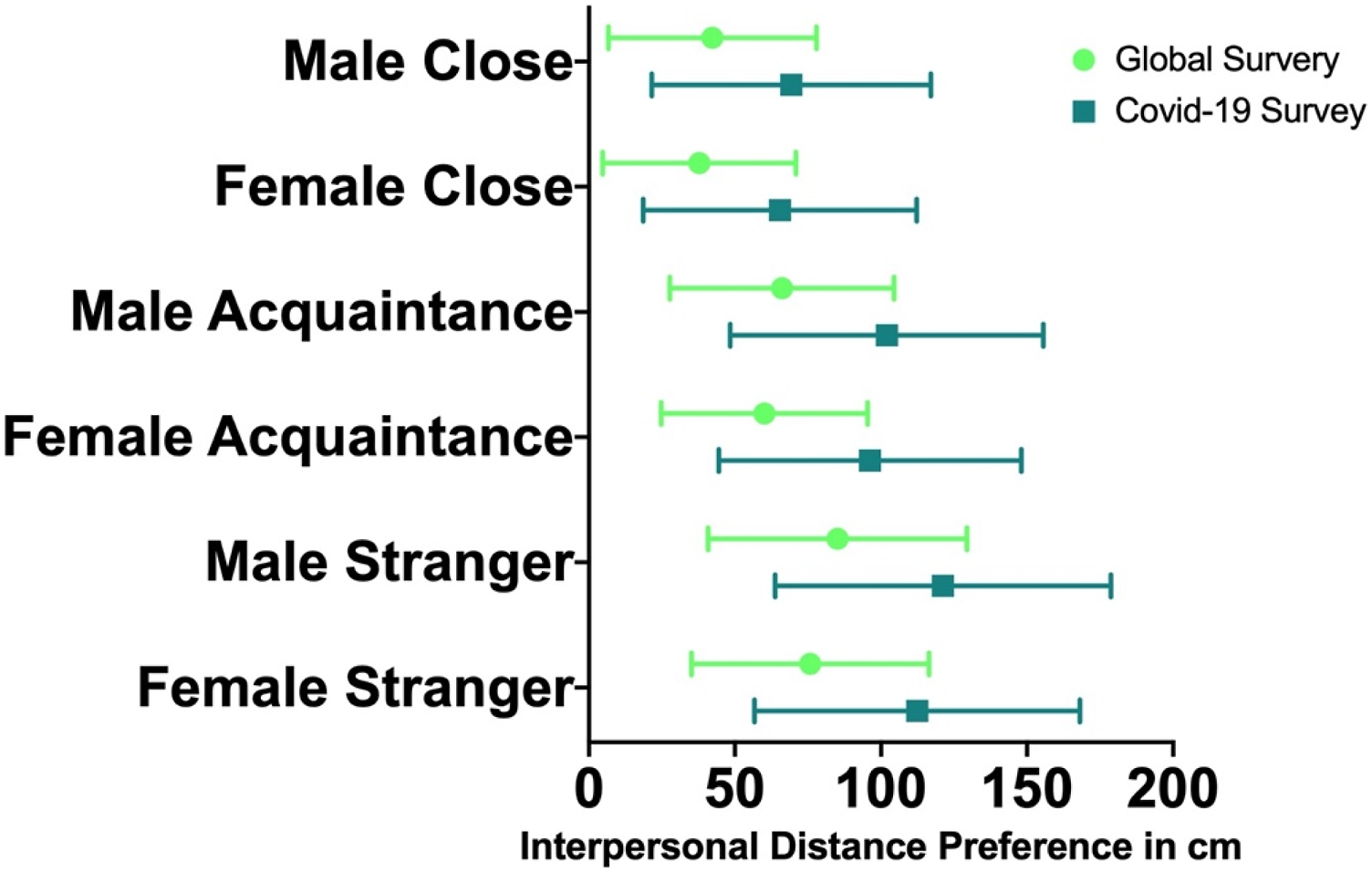
Unexpectedly, across all interaction partners, affectionate touch behaviors increased by 16.2% and non-affectionate touch behaviors increased by 13.9% during the COVID-19 pandemic. Hence, there were significant main effects in both affectionate and non-affectionate touch behaviors for data collection wave (affectionate touch: F(1,160,723) = 839; p < 0.001; non-affectionate touch: F(1,71,368) = 1056; p < 0.001, Figure 2, Supplementary Tables S1-S4). Affectionate and non-affectionate touch behaviors both increased during the COVID-19 pandemic. Differences in affectionate (embrace, stroke, kiss, hug) and non-affectionate touch behaviors (casual physical contact, and handshake) between the Global Survey conducted between 2016 and 2018 and the COVID-19 Survey conducted 2021. Means and standard deviations are displayed. Touch behavior is displayed in %.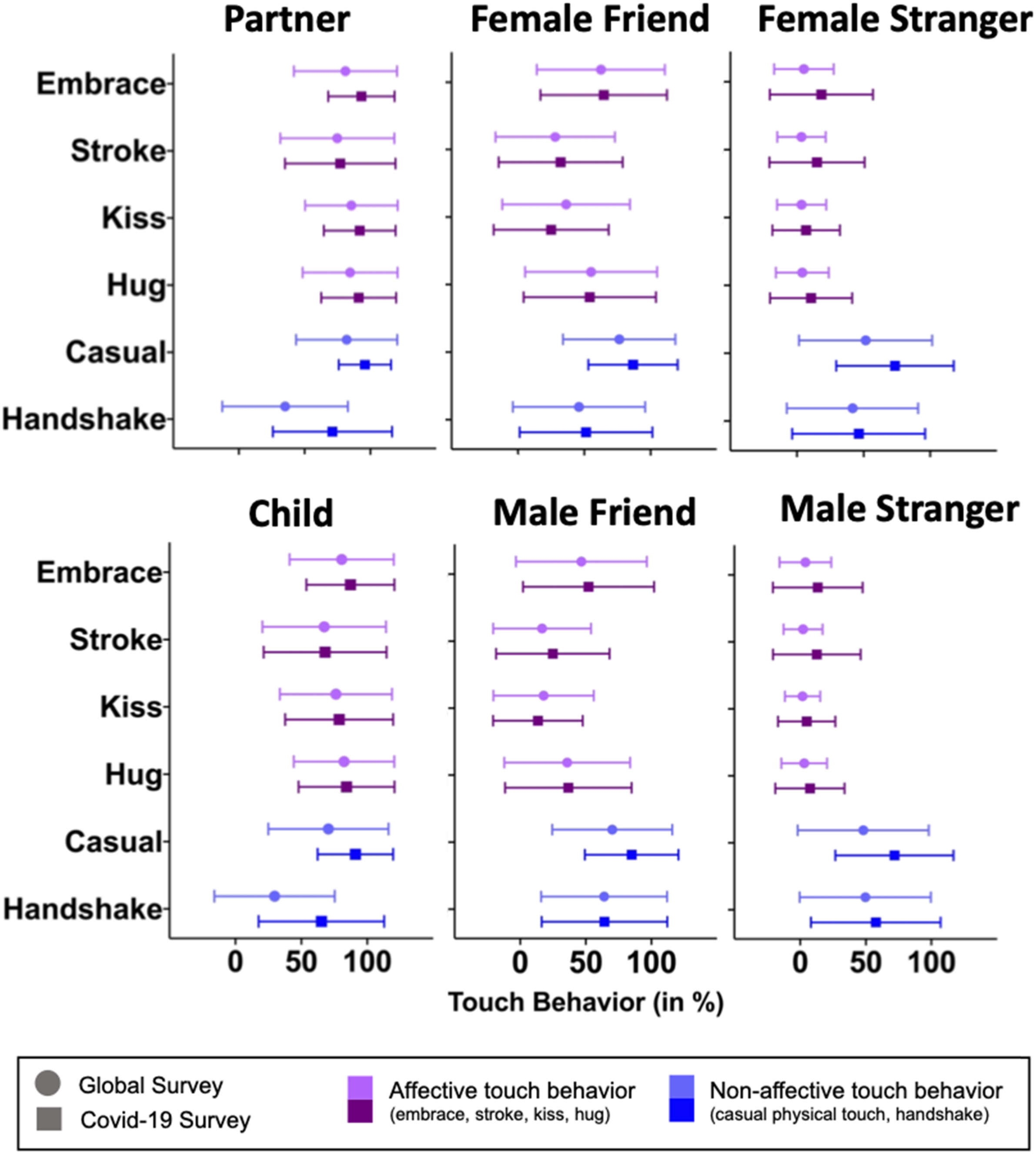
A significant interaction effect of interaction partner*data collection wave suggests that the COVID-19 pandemic may have influenced the behaviors of both affectionate as well as non-affectionate touch differently, depending on interaction partners (affectionate touch: F(10,160,723) = 3784; p < 0.001; non-affectionate touch: F(10,71,368) = 57; p < 0.001). While the increase in affectionate touch behaviors was most pronounced for the partner (CI: 7.5–10.1) and those interaction partners who had a very low prevalence in the Global Survey data collection, namely for male strangers (CI of size of increase: 4.5–7.1%) and female strangers (CI: 6.2–9.4%), it was not as pronounced in the male friend (CI: 1.9–4.1%) and the child (CI: 2.3–4.8%) and not significant in the female friend (CI: −1.3-1.1%). For non-affectionate touch behaviors, the increase was very pronounced for the child (CI: 22.0–28.0%), male strangers (CI: 14.1–20.1%), female strangers (CI: 10.2–16.2%) and partner (21.6–27.5%) categories, and also strong for the male friend (CI: 5.8–9.7%) and the female friend (CI: 6.1–9.7%) categories.
We observed pronounced differences also between individual countries (for detailed results regarding each country and each touch type see Supplementary Tables S1–S6 and S11). For affectionate touch, the effect of country explained a difference of 17.4% (CI:9.3–32.8%, p = 0.002). As indicated in Supplementary Table S11, indices of affectionate touch variability toward partners and strangers mostly increased, whereas decreases were found only in Colombia, India, Sweden and Slovenia. Touch to partner increased in most countries, most pronouncedly in Nigeria, Uganda, Pakistan, Russia and Slovakia. The differences in affectionate touch to friends were more heterogenous. For example, touch to friends decreased in India, Turkey, Brazil and Algeria, while it increased in Russia, Ukraine, Poland and Lithuania. For non-affectionate touch the effect of country explained a difference of 18.8% (CI:10.3–34.4%, p = 0.001). Non-affectionate touch indices were mostly higher during the pandemic as compared to the first measurement. For example, non-affectionate touch to the partner decreased only in India and increased in all other countries. To friends, non-affectionate touch decreased in India and Germany and Algeria and increased for instance in Russia, Slovenia and Slovakia.
Social Distancing and Perceived Vulnerability to Disease
For all interaction partners, PVD positively predicted interpersonal distance preferences (each p < 0.001) across the whole sample (see Supplementary Table S9). This indicates that individuals with higher perceived vulnerability to disease preferred larger distances between themselves and other individuals than did people with lower perceived vulnerability to disease. Similar results – but with an even stronger effect size – were observed when correlations were performed between mean country values of interpersonal distance preferences and PVD (each p < 0.001; see Figure 3 and Supplementary Table S9). In countries with high PVD, such as Brazil and Turkey, higher interpersonal distances were preferred as compared to countries with lower PVD, such as Norway or Austria. All correlations between interpersonal distance preference and PVD on individual country levels are found in Supplementary Table S10. Associations between interpersonal distance and PVD. Scatterplots of associations between interpersonal distance preference and perceived vulnerability to disease (PVD) during the COVID-19 pandemic by country are displayed. Mean values of interpersonal distance preference and PVD by country are used. The gray lines represent the best linear fit to the data.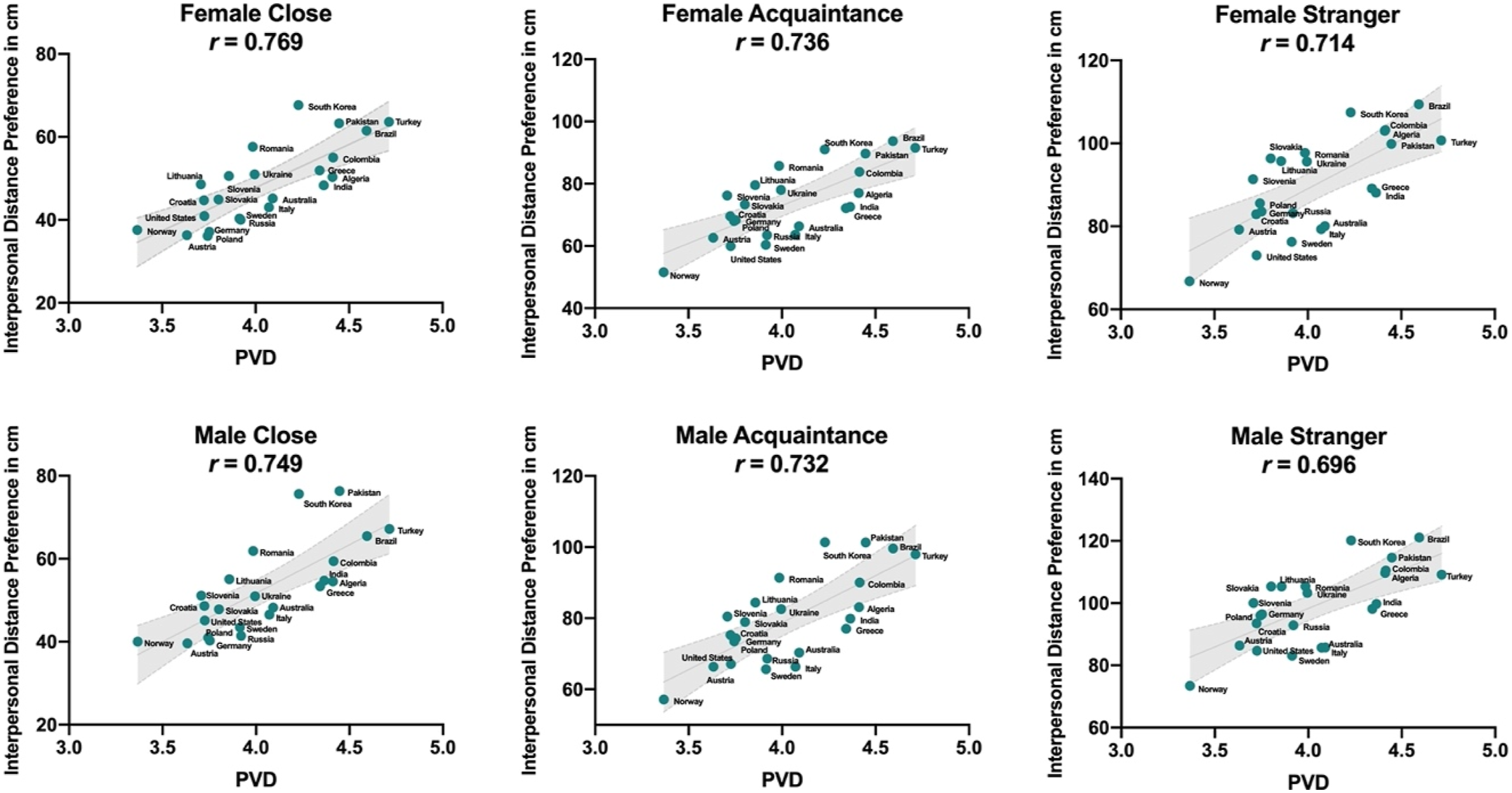
Spearman correlations between perceived vulnerability to disease (PVD) and diversity of affectionate and non-affectionate touch.
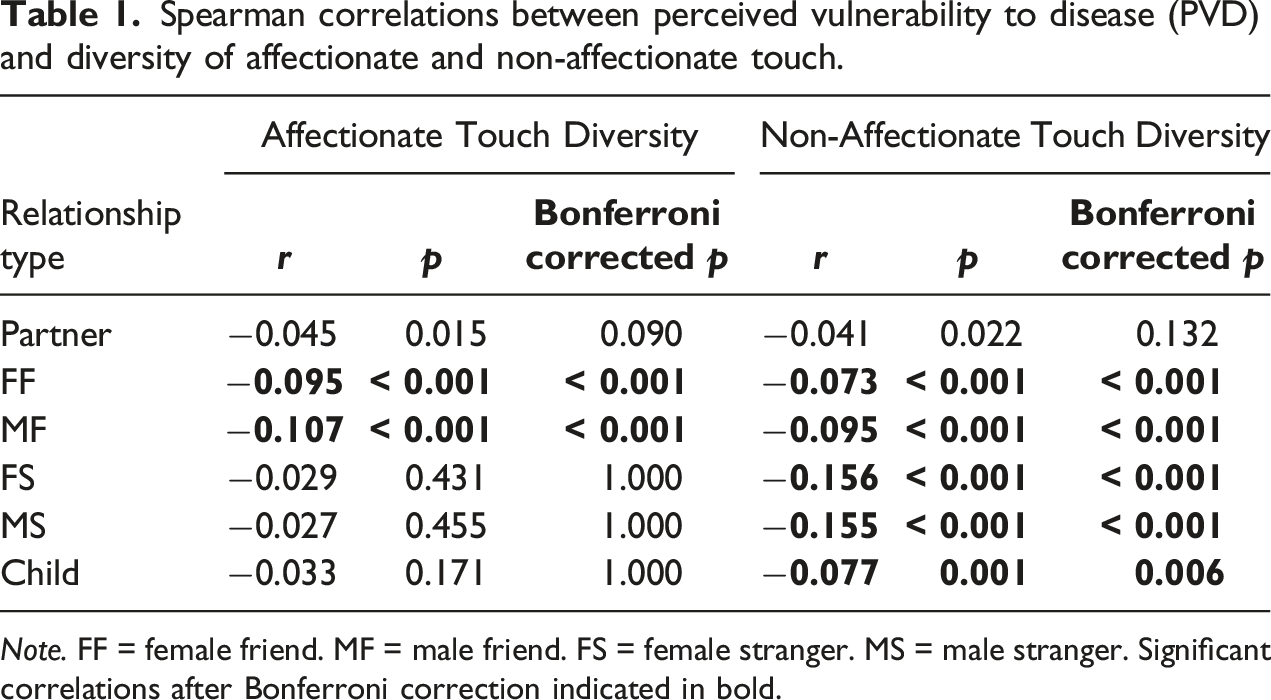
Note. FF = female friend. MF = male friend. FS = female stranger. MS = male stranger. Significant correlations after Bonferroni correction indicated in bold.
Discussion
The unusual scope of the SARS-Cov-2 global transmission has led to the worldwide introduction of unprecedented safety measures, including world-wide physical distancing recommendations (WHO, 2021). Our analysis of self-reports from two large cross-cultural surveys suggests that these recommendations have exerted a significant effect on social distancing worldwide, notably increasing the preferred interpersonal distances by nearly 55% on average. This increase was observable across all included countries and all interaction partners, and was more pronounced in individuals with higher self-reported vulnerability to diseases. The pattern of results concerning affectionate and non-affectionate touch behaviors is definitely less uniform and clear, pointing to possible, underlying variables and mechanisms driving these differences.
It is worth exploring what drives the universal increase in preferred interpersonal distances during the COVID-19 pandemic as compared to the pre-pandemic period. Our study showed that this outcome was observed globally, even in countries that are much different from each other – a finding quite rare in cross-cultural analyses. In the context of the existing literature on social distancing during the pandemic (and interpersonal distance in particular), one of the crucial factors may be human prosocial and self-preservation motivations, exhibited regardless of the cultural background. For example, Lunn et al. (2020) found that physical distancing is encouraged by fears of infecting vulnerable people or large numbers of people. Similar findings were reported by Oosterhoff and colleagues (2020). Adolescents in their study were most commonly motivated to apply physical distancing for prosocial reasons (i.e., social responsibility and not making others sick), and a higher level of this motivation predicted higher engagement in social distancing. The effects we report in our study may also possibly be driven by individual self-protection tendencies in people who are anxious about their own health. Accordingly, our study revealed that higher perceived vulnerability to diseases predicted even larger preferred distances from other individuals during the pandemic (Thiebaut et al., 2021). Here, regardless of the universally observed trend we documented, it may be noted that the culture-level PVD was positively associated with interpersonal distance preferences also on the country-level and preferred distances were notably higher in countries with high mean PVD, such as Brazil and Turkey, as compared to countries with lower PVD, such as Norway or Austria. These results confirm the notion that adoption of precautionary behaviors against COVID-19 crucially depend on the perceived risk of becoming severely ill from the virus – and this holds true for individual beliefs as well as group-level knowledge transfer (Allcott et al., 2020; Harper et al., 2021; Wise et al., 2020).
Contrary to our expectations, however, across many countries included in our research, the participants reported a higher incidence of interpersonal touch behaviors during, rather than prior to the COVID-19 pandemic – and this was also true for touching strangers. We propose two possible explanations for this finding. First, data for the second wave of the study were collected in May/June 2021, during a time of relatively low or decreasing viral incidences in most countries we surveyed, and thus people may have used the opportunity provided by relatively low SARS-CoV-2 infections to engage in touch behaviors. For example, affectionate touch behaviors were reported considerably more often in interactions with strangers in the COVID-19 Survey, while in the pre-pandemic Global Survey they were quite rare. This is plausible as touch is not only a potential risk for transmission of disease, but also a beneficial “glue” for social interactions with positive effects on well-being (Field, 2010) and stress alleviation (Cong et al., 2021; Ditzen et al., 2007). People have been largely deprived from physical contact during pandemics and as a result their desire for interpersonal touch could have increased (Meijer et al., 2022). More touch could be a compensation strategy to reduce stress (Kowal, Coll-Martín, et al., 2020), depression, and anxiety (Qiu et al., 2020; Torales et al., 2020) generated by the pandemic. This explanation may be particularly plausible in the case of – mostly uniform – higher values of touch indices for partners and children reported during the pandemic.
Alternatively, a generally enhanced touch awareness during the COVID-19 pandemic may have led to a certain memory bias, where touch occasions became more salient and were therefore better remembered and more often reported during, than before the pandemic. Nevertheless, touch diversity indices still correlated negatively with self-reported vulnerability to diseases, especially in the case of non-affectionate touch toward strangers. Furthermore, individuals of higher perceived vulnerability to diseases were slightly less likely to use interpersonal touch in relationships with their friends. In this context, it is noteworthy that physical distancing behaviors triggered by the motivation to avoid personal illness are known to be associated with a higher risk of mental health problems (Lieberoth et al., 2021; Oosterhoff et al., 2020).
The increases in interpersonal touch and preferred distance may seem contradictory. However, this divergence might result from a discrepancy in preferences (for interpersonal distances) and behaviors (actual touch incidences). For instance, in a recent study, when participants were asked to pass by a virtual agent in a supermarket, they only maintained the recommended 1.5 m distance when this could be done without any further effort (Kroczek et al., 2022). It is also possible that one has certain preferences, but is forced to behave otherwise, since one’s behaviors depend also on the behaviors of others. For instance, Biehl et al. (2021) showed that elderly persons have difficulties maintaining the recommended interpersonal distance when they are approached by other people (despite their preferences). The same may be true for touch. It may be hard not to shake an outstretched hand during a business meeting, or avoid casual touch in an elevator. Regardless of the potential dangers associated with interpersonal touch during the pandemic, the average prevalence of handshakes with strangers exceeded 50% among our participants, and the percentage of people declaring they shook hands with strangers during the preceding week was as high as 70% in 7 countries.
Compliance with social distancing rules and guidelines (i.e., the behavioral index of actual touch used by our participants) may also be affected by cultural attitudes and behavioral norms (Welsch et al., 2020). As illustrated in our supplementary tables, the differences between two surveys in reported touch behaviors were far from uniform across the countries we included. This opens numerous questions as to the variables that may have driven this diversity. We may assume that enforcing a physical distance of 1.5–2 m and promoting the absence of interpersonal touch can represent a particularly serious challenge in some regions, especially in those highly valuing close social contacts (Creighton et al., 2022). On the other hand, the body of literature in this area generally finds that collectivism, which is also associated with a high value of interpersonal closeness, generally predicts greater COVID-19 protection compliance (Cho et al., 2022; Im & Chen, 2022; Leong et al., 2022; Lu et al., 2021), and higher self-importance/expectation to engage in behaviors known to prevent the COVID-19 spread (Cho et al., 2022). This trend may be driven by collectivism being associated with a belief that other members of a community consider it important to engage in preventive behaviors (Cho et al., 2022). Actually, even messages focusing on individualistic gains and collectivistic losses can increase people’s intention to adopt such behaviors (Yu & Shen, 2013). Such studies and their complexity provide an interesting combination with a heterogenous pattern of our findings, and open new questions and research directions in the area of cultural factors underlying the magnitude of effects the COVID-19 pandemic has had on social behaviors.
With regard to COVID-19 policies compliance, it should be remembered that there are also some situational constraints that are more extreme in regions with a higher population density. Such a case of impossible compliance with COVID-19 protection policies was reported by Wasdani and Prasad (2020), who showed that among the most socially vulnerable inhabitants of a poor and overcrowded part of an Indian city, social distancing rules were unfortunately “more an aspiration than any attainable reality”. The state-enforced policy could also affect interpersonal behaviors. Even the type of message used to promote physical distancing (Legate et al., 2021) and the political leaders of each country could impact the perceived importance of, the diffusion of, and the compliance with social distancing measures during the current pandemic (Luoto & Varella, 2021). This may be reflected in outcomes we observed in some individual countries analyzed in our studies. For example, in Germany, preferred interpersonal distance to strangers was higher during the pandemic and – coherently – the touch behaviors to strangers were less frequent. Such outcomes may be explained by the strict COVID-19 avoidance policies enforced by the state, with – among others – the recommendation of 2m interpersonal distance to strangers. However, this recommendation seems not to be reflected in affectionate touch behaviors to family (partner, child), or friends. Here, individuals seemed to not comply with the state rules. The governmental regulations, particularly strict in Germany throughout the more difficult phases of the pandemic, may have thus been reflected in the easily observable social distancing in relation to strangers, but less meaningful for close, affectionate interactions.
Such explanations as those presented above remain, however, hypothetical at this stage of research, since the current study did not investigate the distal associations of interpersonal touch or distancing with outcomes like mental health, or COVID-19 policies. Understanding the processes we hypothesize upon may be even more difficult because the cultures are not uniform, and study sites even within one country can be much different from one another in terms of important factors such as religion. What should be highlighted is that the data we presented in our manuscript can be used to generate new hypotheses on culture-level variables that drive the trends we observed in the interpersonal behaviors, or other changes associated with the COVID-19 pandemic. In addition to the factors and proposed future research directions discussed or listed above, one such variable could be social network structure, that is, weak-ties (avoidant attachment) versus strong-ties (anxious attachment) (Yamagishi & Hashimoto, 2016). As shown by an exploratory analysis presented in Supplementary File 2, there is some evidence for meaningful cross-cultural patterns in interpersonal distance and affectionate touch variation as a function of these variables.
With respect to our study, despite the use of convenient non-representative sampling it is critical to note that we did not use objective measures of distance or touch, but rather based our results on self-reports. Such self-reports are prone to bias by various confounding effects, such as memory bias, estimation error, or social desirability (van de Mortel, 2008). We consider social desirability unlikely to explain our findings, because this effect should not only lead to the reported increased social distancing preference, but also to decreased reporting of touch behaviors. However, the latter was not the case. Effects of estimation errors are also unlikely to explain our results as those should affect both survey waves equally. Memory bias, on the other hand, might differ between the survey waves because the recommendations of physical distance might have led to a higher salience of memories of touching.
Despite the irregular, wave-like increases in COVID-19 rates, SARS-CoV-2 has been actively affecting human lives around the world for several years now, and so have the attempts to mitigate the extent and the speed of the pandemic in community settings. Our two cross-cultural surveys, separated only by a few years, show that the pandemic could have meaningfully affected social distancing preferences and touch behaviors across the globe. Some of the limitations of our survey studies can be addressed in future work by using other methodologies such as videos from security cameras in public places or cell phone location data with user permissions. After global vaccination has increased and the threat of the pandemic has greatly decreased, studies may also test whether interpersonal space preferences and touching behaviors returned to pre-pandemic levels or remained at the new, elevated levels. The unprecedented social distancing guidelines during the pandemic have opened new opportunities for investigating and understanding interpersonal spacing and touching on a global scale.
Supplemental Material
Supplemental Material - COVID-19 and Social Distancing: A Cross-Cultural Study of Interpersonal Distance Preferences and Touch Behaviors Before and During the Pandemic
Supplemental Material for COVID-19 and Social Distancing: A Cross-Cultural Study of Interpersonal Distance Preferences and Touch Behaviors Before and During the Pandemic by Ilona Croy, Carina Heller, Grace Akello, Afifa Anjum, Chiemezie Atama, Andreja Avsec, Boris Bizumic, Ricardo Borges Rodrigues, Mahmoud Boussena, Marina Butovskaya, Seda Can, Hakan Cetinkaya, Jorge Contreras-Garduño, Rui Costa Lopes, Marcin Czub, Slavka Demuthova, Daria Dronova, Seda Dural, Oliver Ifeanyi Eya, Mokadem Fatma, Tomasz Frackowiak, Farida Guemaz, Ivana Hromatko, Konstantinos Kafetsios, Tina Kavčič, Imran Khilji, Magdalena Kruk, Cătălin Lazăr, Torun Lindholm, Amanda Londero-Santos, Conal Monaghan, Anam Mughal, Bojan Musil, Jean Carlos Natividade, Elisabeth Oberzaucher, Anna Oleszkiewicz, Ike E. Onyishi, Charity Onyishi, Ariela Francesca Pagani, Miriam Parise, Katarzyna Pisanski, Nejc Plohl, Camelia Popa, Pavol Prokop, Muhammad Rizwan, Mario Sainz, Rūta Sargautytė, Shivantika Sharad,ORCID, Olha Uhryn, Jaroslava Valentova, Marco Varella, Belkacem Yakhlef, Gyesook Yoo, Gaja Zager Kocjan, Maja Zupančič and Agnieszka Sorokowska in Cross-Cultural Research
Supplemental Material
Supplemental Material - COVID-19 and Social Distancing: A Cross-Cultural Study of Interpersonal Distance Preferences and Touch Behaviors Before and During the Pandemic
Supplemental Material for COVID-19 and Social Distancing: A Cross-Cultural Study of Interpersonal Distance Preferences and Touch Behaviors Before and During the Pandemic by Ilona Croy, Carina Heller, Grace Akello, Afifa Anjum, Chiemezie Atama, Andreja Avsec, Boris Bizumic, Ricardo Borges Rodrigues, Mahmoud Boussena, Marina Butovskaya, Seda Can, Hakan Cetinkaya, Jorge Contreras-Garduño, Rui Costa Lopes, Marcin Czub, Slavka Demuthova, Daria Dronova, Seda Dural, Oliver Ifeanyi Eya, Mokadem Fatma, Tomasz Frackowiak, Farida Guemaz, Ivana Hromatko, Konstantinos Kafetsios, Tina Kavčič, Imran Khilji, Magdalena Kruk, Cătălin Lazăr, Torun Lindholm, Amanda Londero-Santos, Conal Monaghan, Anam Mughal, Bojan Musil, Jean Carlos Natividade, Elisabeth Oberzaucher, Anna Oleszkiewicz, Ike E. Onyishi, Charity Onyishi, Ariela Francesca Pagani, Miriam Parise, Katarzyna Pisanski, Nejc Plohl, Camelia Popa, Pavol Prokop, Muhammad Rizwan, Mario Sainz, Rūta Sargautytė, Shivantika Sharad,ORCID, Olha Uhryn, Jaroslava Valentova, Marco Varella, Belkacem Yakhlef, Gyesook Yoo, Gaja Zager Kocjan, Maja Zupančič and Agnieszka Sorokowska in Cross-Cultural Research
Footnotes
Author’s Note
The project was preregistered on the AsPredicted website (https://aspredicted.org/PAI_VSM) and all data for this project are available at ![]() .
.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Scientific Excellence Incubator Being Human Lab, University of Wroclaw. The work of Andreja Avsec and Gaja Zager Kocjan was supported by the Slovenian Research Agency, research core funding no. P5-0110. The work of Tina Kavčič and Maja Zupančič was supported by the Slovenian Research Agency, research core funding no. P5-0062.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.