
Abstract
Trauma work involves intervening with others enduring acute pain and suffering, often with heavy psychological and physical health impacts. An important question is whether dispositional empathy helps or hurts trauma workers in their occupational functioning. The current study addresses this gap in the research literature by using a person-centered approach to examine the empathy profiles and professional outcomes of a broad sample of trauma workers (n = 315). We measured their trait empathy and organizational outcomes (occupational burnout, person-job fit, turnover intentions, job performance), and found three distinct empathy profiles which differed significantly in their occupational functioning. A ‘self-focused’ empathy profile (dominated by high personal distress responding) reported the worst functioning; an ‘other-oriented’ profile (high on perspective taking and empathic concern) had more positive functioning, and an unexpected ‘low reactivity’ profile (a full SD below the general population on empathy facets) showed the lowest exhaustion. Exploratory analyses revealed that first responders (e.g., police, firefighters, EMTs, paramedics) were overrepresented in the ‘low reactivity’ profile, while psychology-related professions (e.g., psychologists, counsellors, social workers) were underrepresented in that profile. The significance of these results, as well as their implications for empathy research and vocational counselling in the field of trauma work, are discussed.
Keywords
Introduction
Trauma workers are professionals and paraprofessionals who have been trained to work with victims in the prolonged aftermath of traumatic events (Dutton & Rubinstein, 1995). The ‘prolonged aftermath’ includes things such as the recounting and revivification of the event by the client, the survivor’s reactions to the trauma (via intense emotional pain, rage, despair, etc.), and the institutional or social responses that may re-victimize the client (Dutton & Rubinstein, 1995). Emergency personnel (e.g., paramedics, firefighters, police, emergency medical technicians, etc.) also fall under the umbrella of trauma work, as they are exposed to human pain and suffering on almost a daily basis. Specifically, they “work to rescue individuals trapped in crashed vehicles, they extricate people from fires, they collect the remains of suicide victims, they care for victims of assault” (Regehr et al., 2002, p. 505).
Trauma workers perform an invaluable service to society, yet also bear a heavy personal burden as a result of this work. For example, alcohol abuse and suicide ideation have been associated with trauma-related professions, with 34% of firefighters reporting binge-drinking alcohol in the previous month (Piazza-Gardner et al., 2014). Career prevalence estimates for suicide ideation and suicide attempts are estimated at 46.8% and 15.5% for current and retired firefighters, respectively (Stanley et al., 2015). Similarly, Milner and colleagues (2017) found that suicide rates for a sample of Australian emergency and correctional workers was 22.4 for men and 7.8 for women (out of 100,000); this was in contrast to only 15.5 out of 100,000 for men and 3.4 out of 100,000 for women in other occupations.
Beyond these serious lifestyle and physical health risks, trauma workers are also at an elevated risk to acquire psychological injuries, such as secondary traumatic stress (STS; Figley, 1995). STS is characterized by intrusion (e.g., unintended thoughts and/or disturbing dreams about one’s work with clients), avoidance (e.g., feeling emotionally numb or discouraged about the future; having little interest in being around others), and arousal (e.g., trouble sleeping, feeling jumpy or annoyed, and trouble concentrating) (Bride et al., 2004). Trauma workers can experience disruptive and painful psychological effects months or years after their initial work with victims (McCann & Pearlman, 1990). For example, Peled-Avram (2017) found that nine percent of Israeli social workers reported a high average level of secondary traumatization, while 14% reported very high or extremely high levels.
Empathy in Trauma Work: A Help or Hindrance?
An intriguing and important question is whether higher empathy in trauma workers serves as a buffer or an escalator of stress responses in their work. As a psychological construct, empathy is proposed to consist of four broad elements: (1) understanding, (2) feeling and (3) sharing another person’s world, while also (4) maintaining self-other differentiation (Eklund & Meranius, 2021). The escalation hypothesis has been put forward by theorists on the basis that high empathy would escalate the transmission of trauma from the primary victim to the trauma worker, invoking STS (Figley, 1995; MacRitchie & Leibowitz, 2010). As Figley (1995) so aptly stated, “the process of empathizing with a traumatized person helps us to understand the person’s experience of being traumatized, but, in the process, we may be traumatized as well” (p. 15).
The prevalence of STS among trauma professions such as social work (Bride, 2007), emergency nursing (Duffy et al., 2015; Morrison & Joy, 2016) and policing (Hyman, 2004) has been well-documented. In a meta-analysis, Cieslak and colleagues (2014) found that STS was also related to job burnout in trauma workers. Interestingly, a peripheral line of research found fMRI evidence for greater burnout among medical professionals with higher dispositional empathy levels (Tei et al., 2014).
However, in apparent contrast to such findings is a substantive body of evidence that suggests that empathy actually buffers or prevents burnout in trauma-relevant professions. Occupational burnout is “a syndrome of emotional exhaustion and cynicism that occurs frequently among individuals who do ‘people-work’ of some kind” (Maslach & Jackson, 1981, p. 99). A scoping review of 26 studies of physicians and nurses found that the vast majority showed an inverse relationship between greater empathy and lower occupational burnout (Williams et al., 2017). The buffering hypothesis is also supported by a study by Turgoose and colleagues (2017), who found that higher trait empathy was correlated with lower burnout among police officers who assist victims of rape and sexual assault. Finally, a review of eight studies conducted with nurses and other medical professionals reported that most studies found higher empathy to be related with lower burnout (Wilkinson et al., 2017).
Researchers have explained the buffering effect as related to other-concern coupled with clear differentiation of self and other, citing that helping behaviour buffers the impact of stressful life events (Gleichgerrcht & Decety, 2013). This explanation, if accurate, would clarify the apparent contradiction in the literature on whether empathy escalates versus buffers burnout in trauma workers, as it depends on the type of empathic response measured.
In social psychology, a consensus has emerged that dispositional empathy is multi-faceted, and the most widely utilized framework is Davis’ (1980, 1983) Interpersonal Reactivity Index (IRI). This scale measures four distinct dispositional empathy facets that differentially predict work-related outcomes (Gilin et al., 2013). Empathic concern involves experiencing feelings of warmth, compassion and concern for other people; perspective taking involves anticipating the behavior and reactions of others; personal distress involves experiencing feelings of anxiety and/or discomfort in emotional settings; and fantasy involves transposing oneself into the feelings and actions of other characters (such as in books, movies and plays). Empathic concern and perspective taking constitute the ‘other-oriented’ aspects of empathy while personal distress constitutes the ‘self-oriented’ aspect (Davis, 1983).
Studies using the IRI to measure dispositional empathy have shown that it is only the personal distress dimension that consistently escalates occupational burnout, with the inherent lack of self-other differentiation seeming to promote transfer of client/patient trauma to the professional (Tei et al., 2014). For example, among psychiatry residents it was only the personal distress dimension that related to burnout and every measured symptom of STS (Fülöp et al., 2012). Similarly, in a large-scale survey of board-certified physicians, burnout and STS correlated with personal distress only, while the perspective taking and empathic concern facets correlated with compassion satisfaction (Gleichgerrcht & Decety, 2013).
The Current Study: Dispositional Empathy Profiles Among Trauma Workers
In organizational and occupational psychology, person-environment interactionist models conceptualize an employee’s stress, performance, and longevity in their work role as determined by the level of fit between their personal characteristics and the job environment (Sonnentag & Frese, 2013). Our study draws on person-environment fit (PE Fit, Kristof-Brown et al., 2005) and conservation of resources (COR, Hobfoll, 1989) theories to develop research questions about how the unique demands of trauma work and the empathy traits of trauma workers may interact to produce a match – or lack thereof (Kristof-Brown et al., 2005). We posit that the level of demand-ability match of individuals to trauma-related jobs contributes to both attraction and selection into trauma-related jobs (Schneider, 1987), as well as occupational outcomes once in the role (Sonnentag & Frese, 2013; Wen et al., 2023).
Our first research question concerns the extent to which a person-centered approach focused on profiles of empathic traits will discover distinct types of trauma workers in their combination of Davis’ (1983) four unique empathic dimensions. From a theoretical point of view, the unique demands of trauma work—for example, reducing the emotional connection with an emergency victim so as to remain cognitively sharp (Regehr et al., 2002)—represent a unique occupational environment that could be expected to signal attraction, and encourage selection, to groups of individuals with compatible coping abilities (Schneider, 1987). Further, Davis’ IRI empathy subfacets occur relatively independently (Davis, 1983), such that “a variety of ‘empathy constellations’ are possible” (Davis, 1980, p. 15). Empirically, the behavioral divergence (opposite prediction) of the IRI facets across a range of outcomes (Gilin et al., 2013; Longmire & Harrison, 2018), and the fact that professional groups can differ markedly in their mean facet scores from the general population (Bellini et al., 2002) add to the theoretical arguments for why person-centered analysis may be especially enlightening in advancing our understanding of dispositional empathy in trauma workers.
Person-centered analyses seek to find categories or subgroups of individuals who are both similar within groups and different between groups, based on their patterns of association among specific outcome variables (Laursen & Hoff, 2006; Pastor et al., 2007; Spurk et al., 2020). Person-centered approaches like latent profile analysis (LPA) are thus ideal for addressing research questions involving qualitatively different configurations of variables within a single population distribution (Spurk et al., 2020), as the focus is on relationships among individuals rather than variables (Muthén & Muthén, 2000). Taking a person-centered approach can therefore further advance our understanding of trauma worker resilience due to the unique individual combinations of different empathic traits themselves.
Occupational research in this area is scant and has not sampled professions exposed to human trauma on a regular basis (Schneider, 1987). Two previous person-centered studies with non-traumatic jobs illustrate how taking this approach could further elucidate our understanding of this unique population. Laverdière and colleagues (2019) conducted an LPA using the IRI (Davis, 1983) on a sample of psychotherapists and found evidence for four distinct empathy profiles. An ‘insecure self-absorbed’ profile emerged which was high on personal distress and low on perspective taking, in contrast with others such as a ‘rational empathic’ profile (characterized by the highest perspective taking, average empathic concern, and low fantasy and personal distress). The researchers speculate that clinicians in the ‘insecure self-absorbed’ profile “may be at risk of becoming overwhelmed by patients’ problems, likely failing to work in the service of therapeutic progress” (Laverdière et al., 2019, p. 41).
Meanwhile, Wang and colleagues (2019) conducted a similar LPA on a sample of Chinese preschool teachers and found evidence for three distinct empathy profiles, including a ‘high cognitive empathy–moderate affective empathy’ profile that had significantly lower levels of emotional exhaustion than profiles in which cognitive empathy was not relatively higher. These studies illustrate how LPA can illuminate types of workers who respond differently to the demands of the occupation, but no previous study has explored the unique profiles that may exist among trauma workers who have self-selected into work in which they must perform while being exposed to substantial human pain and suffering (Regehr et al., 2002; Stanley et al., 2015; Turgoose et al., 2017).
To our knowledge, no published research studies have examined whether meaningful and distinct dispositional empathy profiles exist among a broad sample of trauma workers. Similarly, no studies appear to have examined whether such empathy profiles could be differentiated on occupational performance and well-being outcomes.
While the exact nature of the profiles that will emerge is exploratory, the strong connection between elevated personal distress and negative outcomes in past literature (e.g. Gleichgerrcht & Decety, 2013; Tei et al., 2014) suggests that profiles characterized by higher levels of personal distress will exhibit greater occupational burnout (e.g., Fülöp et al., 2012), while those with high or moderate levels of perspective taking and/or empathic concern will exhibit less burnout (e.g., Wang et al., 2019). Our second research question investigates how empathy profiles provide an “ability” that then fits (or does not) with the emotional demands of trauma work (Kristof-Brown, 2005; Sonnentag & Frese, 2013), conferring resilience versus risk for distress and poor occupational outcomes among trauma workers. Addressing this research gap will not only provide much needed clarity on the nature of empathy profiles and work outcomes in trauma workers, it will also provide greater insights into how organizations might better recruit and counsel their trauma workers. Conservation of Resources (COR) theory (Hobfoll, 1989) posits that individuals strive to build, protect and retain resources they value, and the potential to lose such resources ultimately poses a threat to the individual. According to the COR theory, “resources” can include personal characteristics (Hobfoll, 1989) and people who lack resources fit to their role are ultimately more vulnerable to future resource losses (e.g., “loss spirals”), which we propose can involve escalated strain responses and resultant burnout over time (Halbesleben & Buckley, 2004; Hobfoll, 1989). Viewed through the lens of COR theory, we argue that one’s empathic profile constitutes a resource as defined by Hobfoll (1989) and some profiles may be better fit to working with victims of trauma than others (Kristof-Brown et al., 2005). Indeed, past research has linked both perspective taking and empathic concern to positive outcomes in trauma workers (Gleichgerrcht & Decety, 2013), while personal distress has been consistently linked to negative outcomes (Fülöp et al., 2012; Tei et al., 2014). In other words, perspective taking and empathic concern would be a personal resource, while personal distress is the antithesis (or lack of) a resource. The present study’s focus on person-centered analysis asks whether the interaction of these positive and negative resources will combine to impact trauma workers’ overall fit (or lack thereof) with their chosen line of duty (Kristof-Brown et al., 2005). Person-job fit is an important occupational outcome in its own right, due to being an antecedent and correlate of physical and mental health (Wen et al., 2023), burnout (Zeng & Hu, 2024), strain, job performance, tenure, and intentions to quit (Kristof-Brown et al., 2005). We explore how empathy profiles may differ on these important outcomes. For example, the cognitive engagement element of the perspective taking empathy facet may provide emotional regulation skills to a trauma worker with higher personal distress or fantasy levels to down-regulate any potential over-identification with clients or patients (thus improving their overall fit with their calling). Alternately, while high empathic concern tends to correlate overall with lower burnout in trauma professions, a trauma worker who also has high levels of personal distress and fantasy (e.g., affective over-identification) might show a higher burnout and turnover risk. If meaningful empathy profiles do exist, they may relate to unique resilience outcomes in trauma-related professions and, by extension, serve to inform vocational counselling and coping resources to prevent undesirable work outcomes such as burnout and turnover intentions.
Given the past literature, we expect that profiles characterized by high personal distress and low perspective taking or empathic concern may have worse work outcomes than other profiles. Our third research question capitalizes further on the strengths of person-centered analysis to understand distinct groups of people, and explores whether trauma worker profiles differ on demographic characteristics as well.
Laverdière and colleagues (2019) found that psychodynamic clinicians and less experienced psychotherapists were more likely to be members of the ‘empathic immersion’ and ‘average’ empathy profiles rather than the ‘rational empathic’ profile, and Bellini and colleagues (2002) found that medical residents differed on mean empathy facets from the general population; thus, it is conceivable that different empathy profiles might end up being over-represented and/or under-represented in certain trauma professions.
Method
Participants
Participants were recruited via two different techniques. First, snowball sampling involved e-mailing the researchers’ personal contacts in trauma-related professions and asking them to participate and promote the study within their own networks. The second technique consisted of posting the study information on various social media platforms including Facebook, Twitter and LinkedIn. Targeted posts were also made in specific trauma profession communities on Reddit. To be eligible, participants had to: (1) be currently working, or had previously worked in, a field that is exposed to human pain and suffering on a regular basis; (2) be at least 18 years of age or older; and (3) be living or working in the United States or Canada. Participants were screened out of the study if they listed a non-trauma work profession, did not report any instances of trauma as part of their job, and/or did not pass specific attention-check items. This resulted in an initial sample of 315 cases.
Of these 315 participants, 54% were women, 42.8% were men, and 3.2% identified as ‘other’. Ages ranged from 18 to 67 (M = 33.5, SD = 9.3), with participants residing/working in the United States (76.2%) or Canada (23.8%). Participants identified predominately as White (84.4%), but also Hispanic (4.4%), Asian (1.6%), Black (1%), Indigenous (1%), mixed race (3.5%) and ‘other’ (4.1%). Most participants were either married (46.3%) or single (38.7%), while others were divorced (7.3%), common-law (6.7%) or separated (1%). Professions included nurses (21.3%), paramedics (20.6%), firefighters/EMTs (18.1%), social workers (16.5%), police/corrections (11.1%), medical professionals (6%) and psychologists/counselors (6.4%). Job tenure ranged from six months to 41 years (M = 7.9, SD = 7.4), with the total number of highly traumatic events (e.g., death, sexual assault, gruesome injury, etc.) witnessed on the job ranging from one to 2000. Participants also reported that, on average, 32% (SD = 27.9) of their shifts involved witnessing or experiencing some type of trauma.
Procedure
All invitations to participate in the study contained a hyperlink that took participants directly to an online survey hosted by Qualtrics. After giving their consent, participants first had to answer a screening question where they confirmed that they worked or had worked in a trauma-related profession (i.e., a job where they were exposed, either directly or indirectly, to human pain or suffering). If participants stated that their job did not meet the criteria for trauma work, they were prevented from completing the rest of the survey. Participants who confirmed that they were a trauma worker then completed several demographic questions and the psychological measures described in the next section. In exchange for their participation, all participants were offered the opportunity to enter a draw to win one of five $100 gift cards.
Measures
Demographics
Specific demographic questions were posed to capture participants’ age, gender, ethnicity, profession, country of residence, marital status and job tenure, as well as the total number of trauma experiences at work and the percentage of work shifts involving trauma.
Empathy
Empathy was measured using the Interpersonal Reactivity Index (IRI; Davis, 1983). This 28-item questionnaire contains four 7-item subscales measuring participants’ levels of perspective taking (α = .78), empathic concern (α = .79), personal distress (α = .69) and fantasy (α = .82). Participants responded to each item using a 5-point Likert scale (1 = “does not describe me well”; 5 = “describes me very well”). Items include: “I try to look at everybody’s side of a disagreement before I make a decision” (perspective taking); “when I see someone being taken advantage of, I feel kind of protective towards them” (empathic concern); “being in a tense emotional situation scares me” (personal distress); and “I really get involved with the feelings of the characters in a novel” (fantasy).
Burnout
Occupational burnout was measured using the Maslach Burnout Inventory General Survey (MBI-GS; Maslach et al., 1996), a 16-item tool that measures individuals’ levels of emotional exhaustion (α = .91), cynicism (α = .85) and professional efficacy (α = .76). Participants respond to items inquiring about their feelings about their job using a 7-point Likert scale, with values ranging from zero (“never”) to 6 (“every day”).
Person-Job Fit
Person-job fit (α = .90) was measured using a single-construct measure (Brkich et al., 2002). This scale assesses the degree to which an individual’s knowledge, skills, abilities, needs and values match their job requirements. Items include “all things considered, this job suits me” and “I feel like this is not the right type of work for me”. Responses are given using a 7-point Likert scale (1 = “strongly disagree”; 7 = “strongly agree”).
Turnover Intentions
Participants’ turnover intentions (α = .86) were measured using three items from a scale developed by Kelloway and colleagues (1999). The three turnover items were: “I plan on leaving my job within the next year”; “I have been actively looking for other jobs”; and “I want to remain in my job”. Responses are recorded using a 5-point Likert scale (1 = “strongly disagree”; 5 = “strongly agree”).
Job Performance
Job performance (α = .85) was measured using a 3-item scale developed by Gilin Oore and colleagues (2016). Respondents report how their supervisor or boss would rate their quality of work, amount of work, and overall job performance within the past month. Responses are captured using a 5-point Likert scale (1 = “poor”; 5 = “excellent”).
Results
IRI Means of Trauma Workers Compared to Norms.
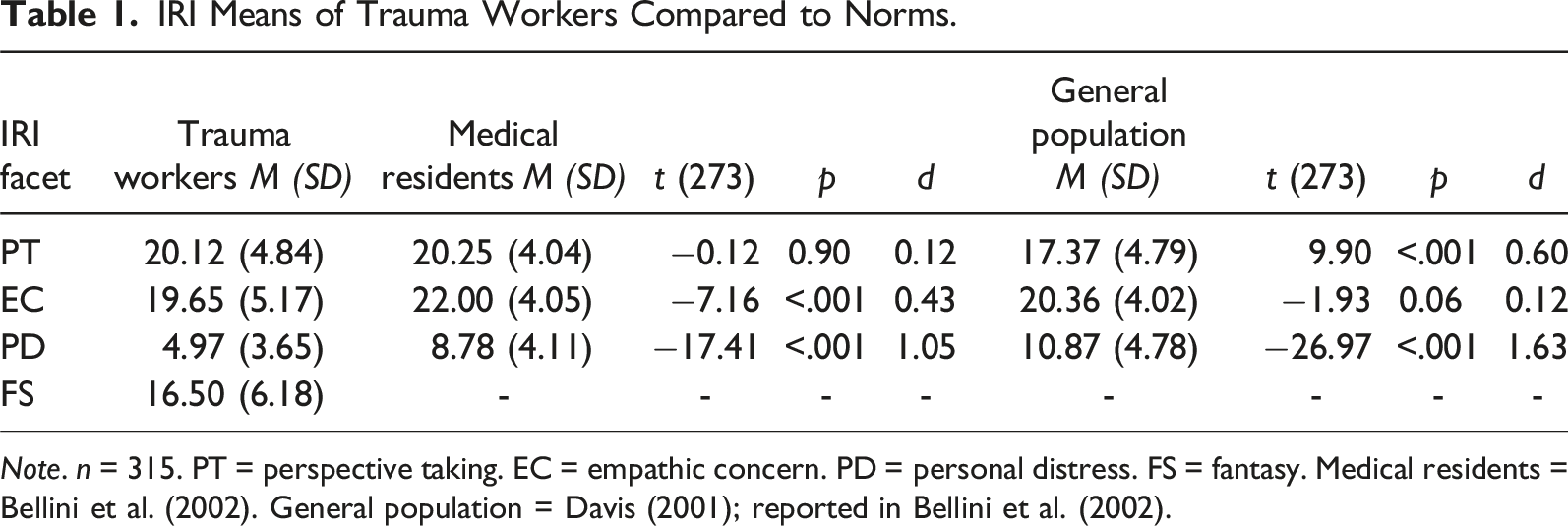
Note. n = 315. PT = perspective taking. EC = empathic concern. PD = personal distress. FS = fantasy. Medical residents = Bellini et al. (2002). General population = Davis (2001); reported in Bellini et al. (2002).
While similar to medical residents on mean PT, our sample was lower on both EC (with a small to medium effect) and PD (with a large effect), indicating trauma workers are less affectively reactive than other medical professionals. Compared to the general population, our sample was significantly higher on PT (with a medium effect), similar on EC, and dramatically lower on PD (very large effect), indicating trauma workers are both more cognitively empathic and much less affectively reactive than the general population.
Latent Profile Analysis
The LPA was conducted using Mplus Demo (Version 8; Muthén & Muthén, 1998-2017). The overall process was iterative, meaning that it first began with estimating a one-profile solution and continued by increasing the number of profiles by one in a stepwise fashion until a best-fitting solution was found (Muthén & Muthén, 2000; Williams & Kibowski, 2016). The indicator variables were the four subscales of the IRI (perspective taking, empathic concern, personal distress and fantasy). We specified a robust maximum likelihood estimator of 7000 random starts and 200 best solutions retained, as recommended by Spurk and colleagues (2020).
LPA Model Fit Summary.
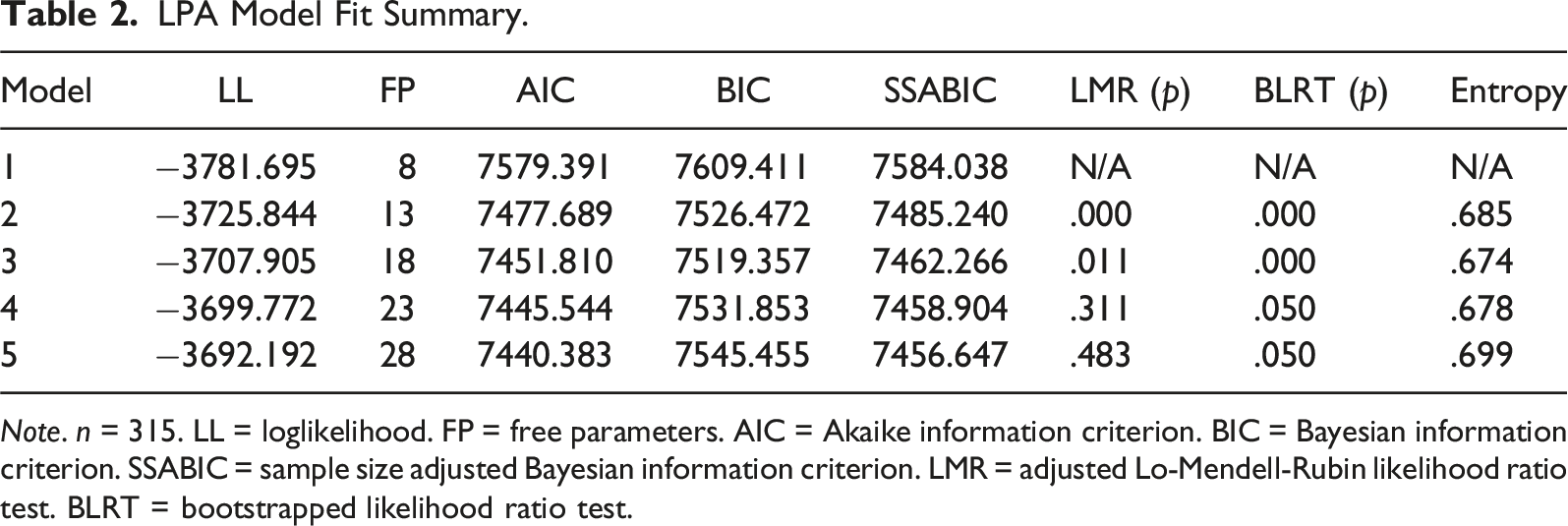
Note. n = 315. LL = loglikelihood. FP = free parameters. AIC = Akaike information criterion. BIC = Bayesian information criterion. SSABIC = sample size adjusted Bayesian information criterion. LMR = adjusted Lo-Mendell-Rubin likelihood ratio test. BLRT = bootstrapped likelihood ratio test.
Other fit statistics considered are the adjusted Lo-Mendell-Rubin likelihood ratio test (LMR) and bootstrapped likelihood ratio test (BLRT). A statistically significant LMR or BLRT value (p < .05) indicates that a model with one less profile, k – 1, should be rejected in favour of the current estimated model, k (Nylund et al., 2007). Entropy, or the probability of properly classifying participants into a latent class, is also considered (Williams & Kibowski, 2016). Values closer to 1 represent a greater probability, however Spurk and colleagues (2020) note that values between 0.60 and 0.80 are considered to be within an acceptable range.
In our LPA, the lowest BIC value occurred at Model 3, indicating that a three-profile solution was a strong candidate for the best-fitting solution. Model 3 also had significant LMR and BLRT values (indicating that we should reject k – 1, or Model 2), and the entropy value (0.67) fell within the accepted range. Additionally, the LMR and BLRT values for Model 4 were both nonsignificant, indicating that we should accept the k – 1 model (Model 3).
In addition to the statistical fit indices, LPA also affords researchers the ability to consider qualitative issues such as parsimony, theoretical consistency, past research and profile descriptions when considering the optimal number of profiles (Bauer & Curran, 2003; Ram & Grimm, 2009). Previous research found evidence for both three (Wang et al., 2019) and four (Laverdière et al., 2019) empathy profiles, and since our hypothesized number fell within this expected range, we decided to retain the three-profile solution for further exploration.
IRI Means, Profile Names and Class Counts for the Three-Profile Solution.
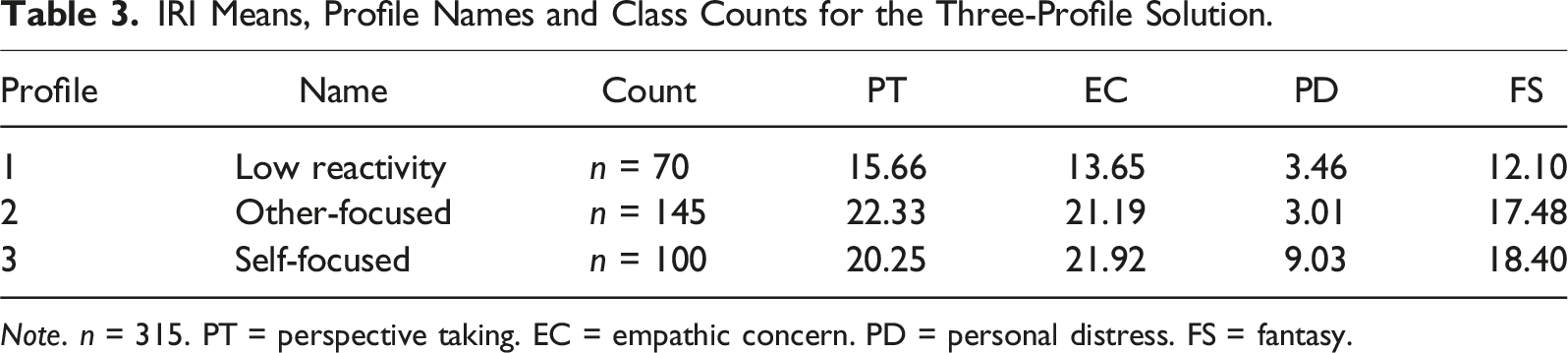
Note. n = 315. PT = perspective taking. EC = empathic concern. PD = personal distress. FS = fantasy.
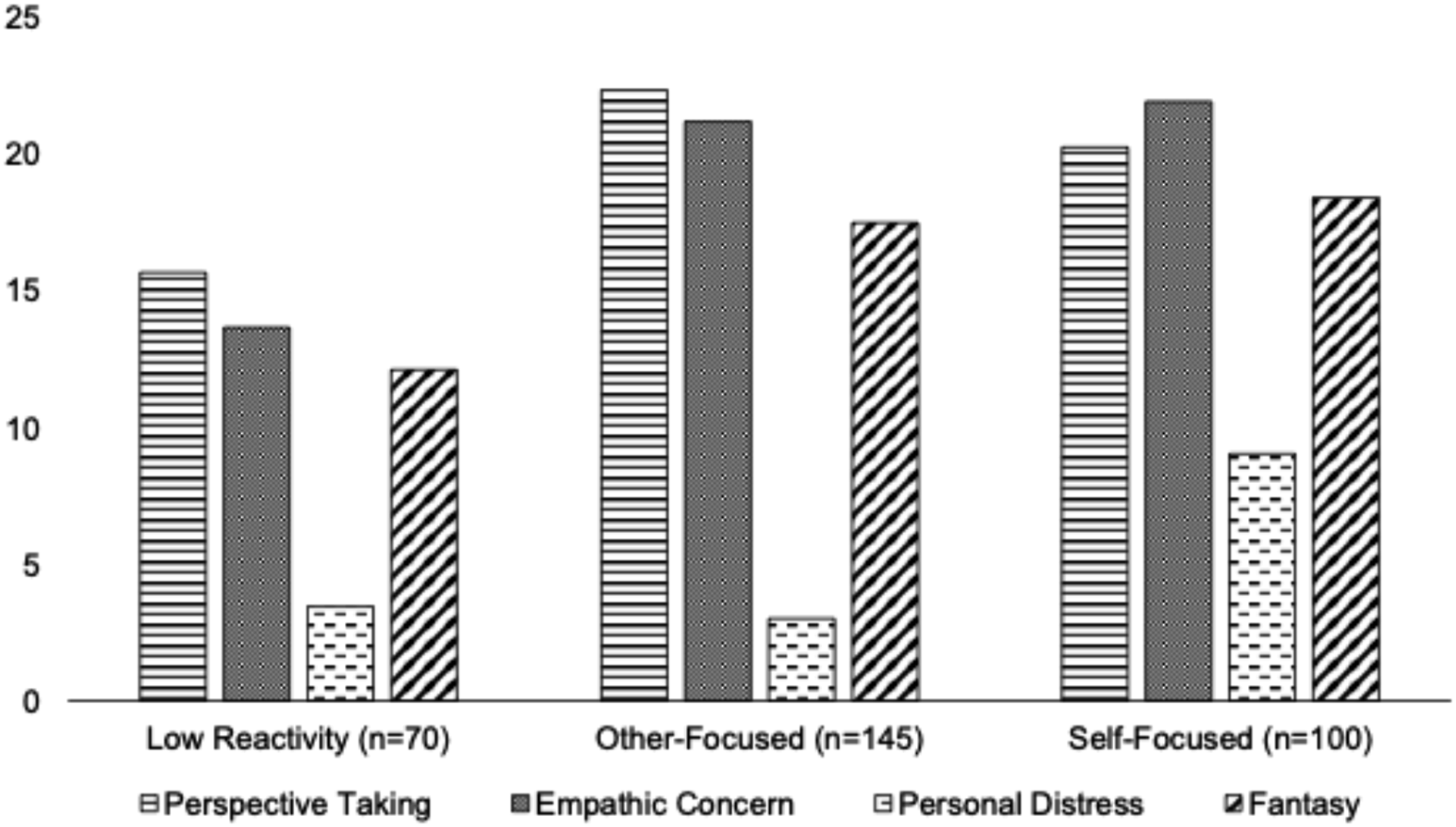
A visual representation of the three empathy profiles and their Interpersonal Reactivity Index (IRI) means.
Empathy Profiles and Work Outcomes
Descriptive Statistics and Intercorrelations for the Main Study Variables.
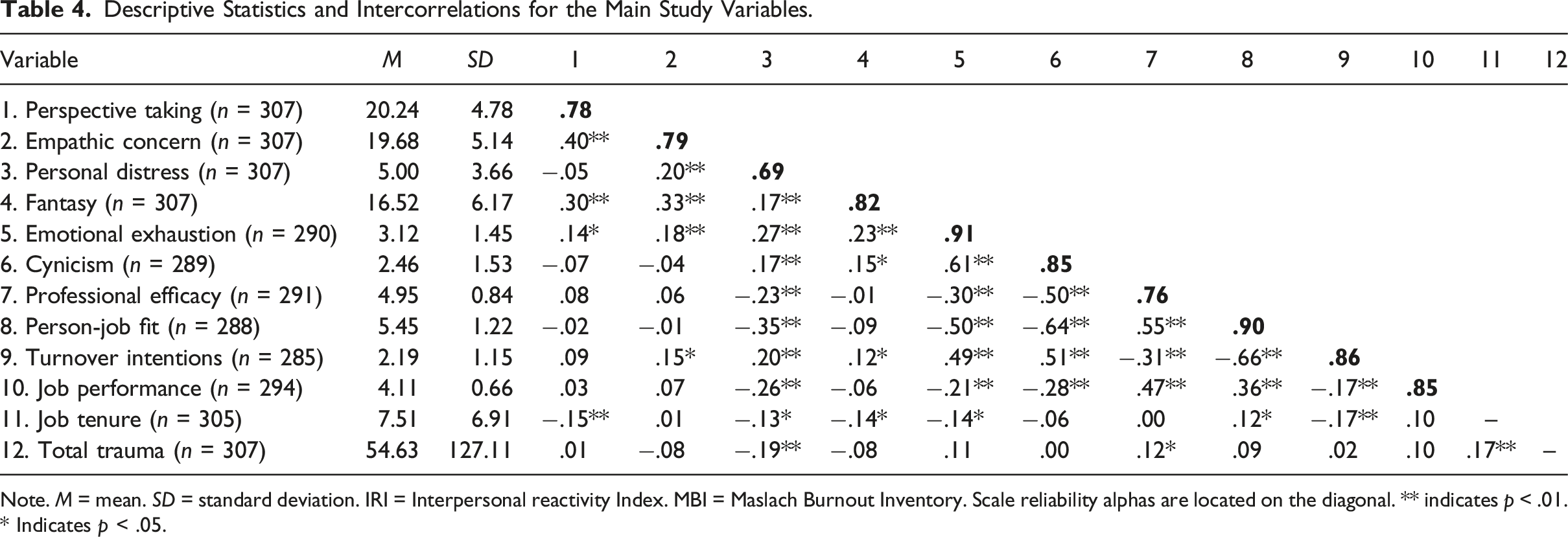
Note. M = mean. SD = standard deviation. IRI = Interpersonal reactivity Index. MBI = Maslach Burnout Inventory. Scale reliability alphas are located on the diagonal. ** indicates p < .01. * Indicates p < .05.
Research Question 2 anticipated that profiles high on personal distress would have relatively worse work outcomes. By extrapolation, the ‘self-focused’ profile – with comparatively very high personal distress – was anticipated to be functioning significantly worse than the other two profiles. Research Question 2 also anticipated that profiles with lower perspective taking and/or empathic concern would have relatively worse work outcomes, so we further expected the ‘other-focused’ profile would be functioning significantly better than the ‘low reactivity’ profile.
Means and Standard Deviations of the Empathy Profiles According to Work Outcome.
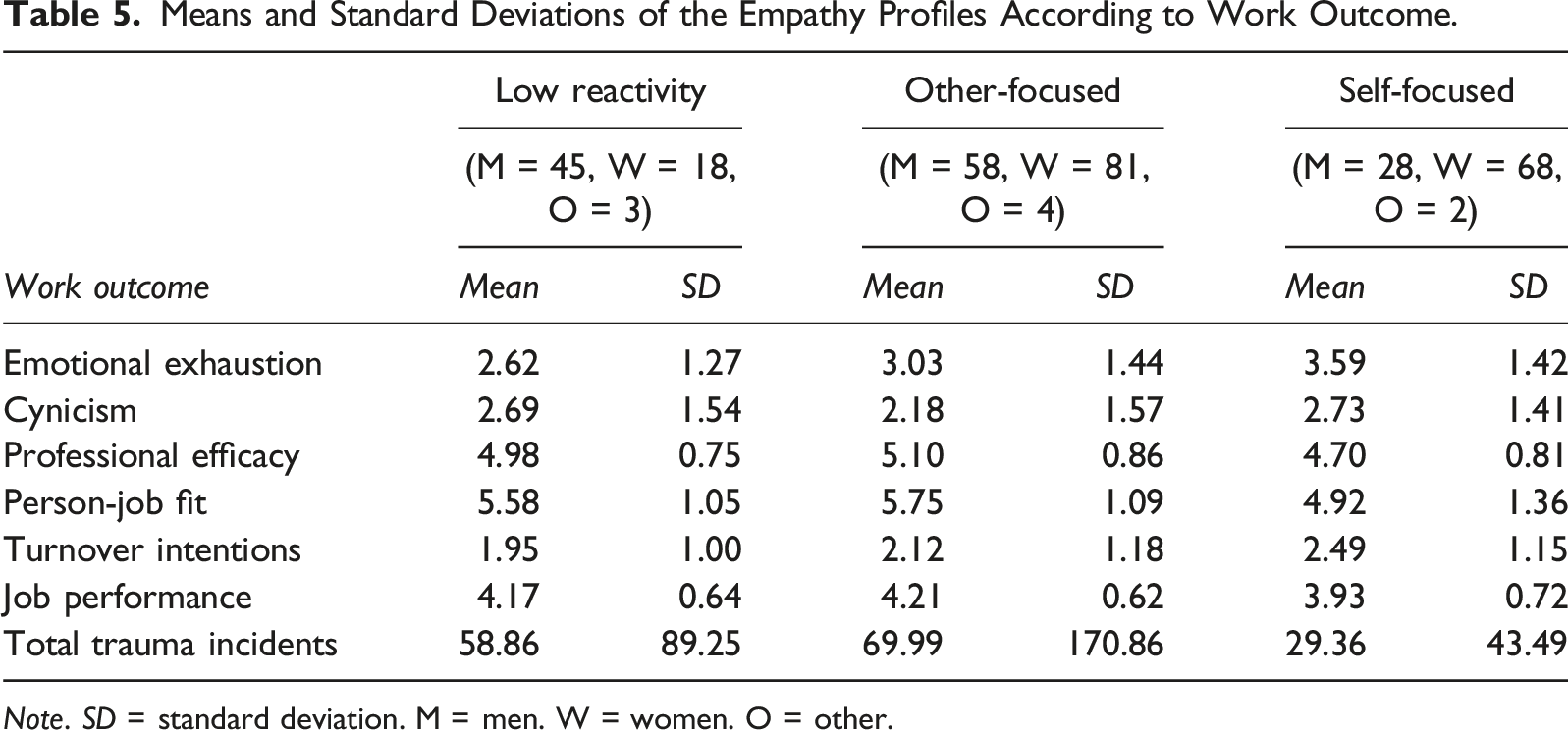
Note. SD = standard deviation. M = men. W = women. O = other.
Burnout
First, on emotional exhaustion, there was a significant main effect for profile membership, F (2, 289) = 9.20, p < .001, ηp2 = .060. Contrast (1) revealed that the ‘self-focused’ profile reported significantly higher emotional exhaustion than the ‘low reactivity’ and ‘other-focused’ profiles combined (t (166.25) = 4.20, p < .001, Cohen’s d = −1.08, large effect). Contrast (2) revealed that the ‘other-focused’ profile reported significantly higher emotional exhaustion than the ‘low reactivity’ profile (t (136.27) = 2.04, p = .043, Cohen’s d = .30, small to medium effect). These results partially support our expectations derived from Research Question 2, as we did not anticipate that the ‘low reactivity’ would fare better than the ‘other-focused’ profile.
Second, on cynicism, there was also a significant main effect for profile membership, F (2, 288) = 4.49, p = .012, ηp2 = .030. Contrast (1) revealed that the ‘self-focused’ profile did not differ on mean cynicism compared to the ‘low reactivity’ and ‘other-focused’ profiles combined (t (178.86) = −1.55, p = .123, Cohen’s d = −.39, small to medium effect), whereas Contrast (2) revealed that the ‘low reactivity’ profile was significantly more cynical than the ‘other-focused’ profile (t (125.30) = −2.18, p = .031, Cohen’s d = −.33, small to medium effect).
Again, on professional efficacy, there was a significant main effect for profile membership, F (2, 290) = 6.59, p = .002, ηp2 = .044, with Contrast (1) showing the ‘self-focused’ profile having lower professional efficacy (t (170.79) = 3.31, p = .001, Cohen’s d = .84, large effect). However, Contrast (2) revealed no significant difference between the ‘low reactivity’ and ‘other-focused’ profiles (t (139.35) = 0.97, p = .340, Cohen’s d = .14, small effect).
Our results for exhaustion and professional efficacy support our expectations from Research Question 2 that a high-personal distress profile would fare worse, but only partially support the notion that the ‘other-focused’ profile would function better than the ‘low reactivity’ profile, with the other-focused profile faring better in terms of cynicism and low-reactivity profile faring better in terms of exhaustion. For the rest of the work outcomes below, the significant distinction is that the ‘self-focused’ profile fares worse than the remaining profiles.
Person-Job Fit
There was a significant main effect for profile membership on person-job fit, F (2, 287) = 14.03, p < .001, ηp2 = .090. Contrast (1) showed that the ‘self-focused’ profile had worse job fit than the other profiles (t (144.38) = 4.53, p < .001, Cohen’s d = 1.27, very large effect), but Contrast (2) showed no difference between the ‘other-focused’ and ‘low reactivity’ profiles (t (125.77) = 1.06, p = .294, Cohen’s d = .16, small effect).
Turnover Intentions
A significant main effect was also found for profile membership on turnover intentions, F (2, 284) = 4.82, p = .009, ηp2 = .033. Contrast (1) showed that the ‘self-focused’ profile had significantly higher turnover intentions than the other profiles (t (156.04) = −3.12, p = .002, Cohen’s d = −.82, large effect), but Contrast (2) showed no difference between the ‘other-focused’ and ‘low reactivity’ profiles (t (140.78) = 1.06, p = .290, Cohen’s d = .15, small effect).
Job Performance
Finally, a significant main effect was found for profile membership on job performance, F (2, 293) = 5.49, p = .005, ηp2 = .036. Contrast (1) showed that the ‘self-focused’ profile had lower self-reported job performance than the other profiles (t (157.58) = 2.95, p = .004, Cohen’s d = .80, large effect), but Contrast (2) showed no difference between the ‘other-focused’ and ‘low reactivity’ profiles (t (118.78) = 0.47, p = .642, Cohen’s d = .07, small effect).
Empathy Profiles and Demographic Variables
We conducted additional exploratory analyses to determine if certain demographic variables (e.g., job tenure, total trauma incidents, type of profession) also differed among the three empathy profiles. A one-way ANOVA for job tenure was not significant, however the ANOVA for total trauma incidents was significant, F (2, 306) = 3.06, p = .048, ηp2 = .020. Contrast (1) showed that the ‘self-focused’ profile had fewer trauma incidents than the other profiles (t (279.15) = 3.50, p < .001, Cohen’s d = .56, medium effect), but Contrast (2) showed no difference between the ‘other-focused’ and ‘low reactivity’ profiles (t (203.87) = 0.62, p = .538, Cohen’s d = .07, small effect).
Likewise, a chi-square test of association revealed significant differences when it came to types of professions, χ2 (12, n = 307) = 42.86, p < .001. An inspection of the crosstabulations revealed that the majority (72.7%) of the participants in the ‘low reactivity’ profile were first responder-type professions: paramedics (22.7%), police/corrections (19.7%), firefighters/EMTs (30.3%). A follow-up chi-square test of association with four simplified profession categories (first responders, nurses, psychology professionals and medical professionals) confirmed the difference between first responders (72.3%) and non-first responders (27.7%) for this profile, χ2 (2, n = 305) = 21.64, p < .001. Comparatively, the proportion of first responders was much lower in the ‘self-focused’ profile (35.1%) and the ‘other-focused’ profile (49%). There was also a significant chi-square test for psychology-related professions (e.g., psychologists, counsellors, social workers) versus non-psychology related professions, χ2 (2, n = 305) = 21.43, p < .001, as this group (3.1%) was vastly underrepresented in the ‘low reactivity’ profile compared to the ‘self-focused’ (34%) and ‘other-focused’ (24.5%) profiles. Thus, Research Question 3 was also answered affirmatively, in that the profiles differed on demographic variables.
Discussion
Our study capitalized on person-centered analysis to address the important question of whether dispositional empathy helps versus hinders trauma professionals in terms of their wellness and efficacy. While some theorists (Figley, 1995; MacRitchie & Leibowitz, 2010) have speculated that high dispositional empathy may escalate the transmission of trauma from patient/client to the trauma worker, the trend across many studies is a buffering effect of high dispositional empathy for trauma professionals (Turgoose et al., 2017; Wilkinson et al., 2017; Williams et al., 2017), associated with lower burnout (Gleichgerrcht & Decety, 2013). Studies that have measured dispositional empathy multi-dimensionally (such as using the IRI scale by Davis, 1983) have shed light on this apparent contradiction, in that it seems the interplay or combination of empathic traits determines the fit of professionals to their work (Gleichgerrcht & Decety, 2013; Wang et al., 2019).
Our study furthers past research by providing novel insights into the relationship between trauma workers’ empathy and theoretically relevant work outcomes (e.g., burnout, person-job fit, job performance and turnover intentions). This population, which has been historically understudied, is unique in that it consists of a broad spectrum of occupations (e.g., physicians, nurses, firefighters, EMTs, police, social workers, counsellors) – all of whom are exposed to some degree of human trauma through the course of their professional responsibilities.
Empathic Profiles of Trauma Workers
Generally speaking, we found that the workers in our sample were substantially higher on perspective taking and markedly lower on personal distress responding than in the general population (Bellini et al., 2002). Within our trauma worker sample, three distinct profiles emerged, which appear to capture a broad range of empathic responding styles (e.g., relatively low empathy or reactivity, other-focused responding, and self-focused responding).
The empathic profiles we found among trauma workers have some consistency but also significant uniqueness compared to empathy profiles found in other occupational populations. For example, there is evidence for a similar self-focused profile (high personal distress, low perspective-taking) also among psychotherapists (Laverdière et al., 2019). The authors theorized this to be a high-risk profile for therapists, and our study confirms this proposition. Every well-being and efficacy work outcome we measured was significantly worse for trauma workers with the self-focused empathic profile. This further confirms the widespread finding that a high level of personal distress responding, when unmitigated by other empathic tendencies, results in over-identification with client and patient trauma (Fülöp et al., 2012; Gleichgerret & Decety, 2013; Tei et al., 2014) and confers a risk of burnout, low job efficacy, and intentions to quit.
Further, past research has found a cognitively other-focused profile among both psychotherapists and preschool teachers (Laverdière et al., 2019; Wang et al., 2019). However, the trauma workers in our study had a more balanced other-focused profile that was equally strong on cognitive (perspective-taking) and affective (empathic concern) resonance with clients and patients. This combination of altruistic helping orientation and self-other distinction promotes emotional regulation and protection against burnout (Gleichgerrcht & Decety, 2013). Our results also show that this empathic profile is thriving professionally, with relatively high job performance and person-job fit, and relatively low intentions to quit.
In terms of unique profiles to the trauma worker population, our ‘low reactivity’ group was an unexpected discovery. The ‘low reactivity’ or low empathy profile was markedly lower across the board on all empathy facets – including for those that tend to correlate with positive and with negative outcomes. In fact, our ‘low reactivity’ profile averaged a full standard deviation lower than medical residents (Bellini et al., 2002) on perspective taking, empathic concern, and personal distress responding. Further, first-responder type trauma workers (e.g., police, fire, paramedics, EMTs) were significantly overrepresented in this ‘low reactivity’ empathy profile.
While very low levels of empathy tend to be a marker of ‘dark’ personality traits such as Machiavellianism, narcissism and psychopathy (Wai & Tiliopoulos, 2012), low empathy trauma workers appear to thrive while helping victims and their families in highly distressed circumstances. The ‘low reactivity’ profile experienced similarly favorable job performance and person-job fit as the ‘other-focused’ profile, and even had significantly lower emotional exhaustion than the ‘other-focused’ profile as well as the lowest mean level of turnover intentions overall.
Theoretical Implications
There are theoretical implications of our work for person-environment fit models in occupational and vocational psychology. First, it is novel to construe empathy profiles as an “ability” to adapt to the emotional demands of trauma work (Kristof-Brown et al., 2005; Sonnentag & Frese, 2013). We suggest that empathic profiles can confer a range of dispositional reactivity (vs. resilience) to certain job stressors, escalating or buffering how stressor appraisals become strain (Sonnentag & Frese, 2013). As an example from our data, the ‘self-focused' profile had the worst occupational outcomes across the board, and yet they reported markedly fewer traumatic work incidents on average than the other two profiles. That is, they react with greater strain to fewer incidents of human suffering.
Second, the fact that trauma workers in our sample showed such unique empathic profiles compared even to medical residents (Bellini et al., 2002) suggests that the unique stressors of trauma work attract a self-selected group with more compatible coping styles (Schneider, 1987). Indeed, all three empathic types of trauma workers show substantially lower personal distress responding than comparison groups (Bellini et al., 2002). This suggests self-selection into trauma work of those less reactive to others’ distress, and among those, the least well-fit (the ‘self-focused’ group) show highest intentions to quit. Further, almost no ‘low reactivity’ trauma workers are employed in psychotherapy, and relatively few ‘other-’ and ‘self-focused’ trauma workers are employed as first responders, suggesting self-selection based on stressor-profile match.
The current study therefore helps to answer the larger theoretical question about the relationship between empathy and trauma work (i.e., does having empathy help or hurt?). The answer, it seems, is that it really boils down to the facet combinations, with one specific aspect of empathy – personal distress – conferring an especially escalated risk of burnout.
For example, our ‘other-focused’ and ‘self-focused’ profiles had very similar levels of perspective taking, empathic concern and fantasy, but the differing levels of personal distress resulted in the existence of two very different groups of trauma workers – both in terms of descriptive names and in work outcomes. Conversely, the ‘low reactivity’ and ‘other-focused’ profiles had dissimilar levels of empathic concern and perspective taking, but had similar levels of personal distress and thus comparable work outcomes. This is an enlightening discovery that would not have been possible had we not adopted a person-centered approach to data analysis.
Additionally, the deleterious effect of personal distress not only confirms past research in this area (Fülöp et al., 2012; Tei et al., 2014), it suggests that this empathic trait is likely the antithesis of a personal resource as conceived in the Conservation of Resources theory (Hobfoll, 1989). As such, future research studies may wish to explore how other individual characteristics (e.g., personality traits, general mental ability) may work together (or against each other) to ultimately influence outcomes (Clark et al., 2019).
Applied Implications
The current study has several implications for vocational guidance and intervention. First, the identification of the problematic ‘self-focused’ profile (characterized by a high level of personal distress) should be viewed as a major benefit to guidance counsellors and human resource professionals who are responsible for recruiting, selecting and advising trauma workers. Specifically, trauma workers and first responders who exhibit this profile should be made aware of their tendency as soon as possible so they can work with their organizations to mitigate the negative occupational consequences of their psychological propensities. Similarly, guidance counsellors and human resource professionals who identify this problematic profile in prospective applicants may wish to advise them that their temperament confers a higher risk of burnout in their chosen vocation that will take active mitigation to support them in their career. Additionally, guidance counsellors and human resource professionals may wish to team up with organizational researchers to develop interventions that view empathy as a multidimensional concept that can be manipulated in field settings, for example, using known techniques to boost perspective taking (Clark et al., 2019).
Recently, we (Gilin et al., 2023) developed a six-module burnout reduction intervention course for health care leaders, and one module provides feedback and coaching on the four IRI empathy facets. Leaders who have high personal distress unmitigated by high perspective taking are made aware that using the burnout prevention tools in the course—including vigilant work stress recovery—would be especially critical to protect their energy for their calling. The course was shown to reduce burnout and increase off-work recovery in home nursing leaders immediately post-course (Foote et al., 2022; Gilin et al., 2021) and prevent resting heart rate escalation in physician leaders (Gilin et al., 2023). However, this does not provide evidence of targeted impact on those with the self-focused style. Longitudinal intervention studies with large samples including a broad spectrum of empathic styles could inform whether such coaching can indeed be preventive of poor well-being and work outcomes especially for this group. Doing so could save both applicants and hiring organizations time and potential hardships in the future.
Second, while individuals with a profile of very low empathy across all facets seem to be especially resilient to coping with the emotional rigours of trauma work, some researchers have called for first responder agencies such as police to recruit and select more empathetic officers (Bloksgaard & Prieur, 2021). While our results indicate that lower empathy can mean less emotional exhaustion and turnover intentions in trauma professions, we must also acknowledge that our study was self-report data and did not consist of more objective measures of job performance or even patient/client-rated empathic concern. In other words, just because the ‘low reactivity’ trauma workers were the least distressed subgroup of trauma workers in our sample, we cannot conclude that they are “better” at their jobs. Future research involving objective institutional work data and other-rated measures of job performance would need to be conducted before such a claim could be made.
In the meantime, we can say that having a ‘low reactivity’ profile does seem to offer some self-protective features and resilience in very challenging professions. This finding is important, because past research shows that firefighters (Piazza-Gardner et al., 2014; Stanley et al., 2015), emergency and correctional workers (Duffy et al., 2015; McCann & Pearlman, 1990; Milner et al., 2017; Morrison & Joy, 2016), paramedics (Regehr et al., 2002) and social workers (Bride, 2007; Peled-Avram, 2017; Wagaman et al., 2015) have higher rates of substance use, STS and suicidality. Thus, low-reactivity trauma workers, who appear to self-select at a high rate into these professions, may be protected from such destructive outcomes.
Limitations
Several important limitations must be noted for the current study. First, we note that our study was cross-sectional in nature, so the replicability of our profiles should be confirmed with similar samples. For example, Laverdière and colleagues (2019) found four distinct empathy profiles using a sample of psychotherapists, and their ‘insecure self-absorbed’ profile appears to match quite well with our ‘self-focused’ profile. But because our other two profiles do not directly map onto any of theirs, future replication studies should utilize a broad sample of trauma workers rather than specific occupations (such as psychotherapists).
Second, our sample size was slightly small for latent profile analysis (Spurk et al., 2020), so certain occupations were ultimately underrepresented in the sample. Future studies should try to increase representation for these types of occupations in order to confirm whether our findings (specifically, that the ‘low reactivity’ profile is underrepresented in psychology-related occupations) are also applicable for larger samples of trauma workers.
Third, although our sample was relatively evenly split between genders (e.g., 54% women), it is possible that a gender bias exists in terms of both empathy profile composition and occupational representation. For example, we found that the ‘low reactivity’ profile was predominantly male (68%), and in turn was also overrepresented in the first responder type professions (72.7%). These findings do comport with past research – Davis (1980) found that men tend to score lower on all four facets of empathy, and Frazer and colleagues (2021) remind us that first responder professions tend to be male-dominated in general – however it would still be worthwhile for future studies to over-sample minority gender groups (e.g., men in nursing, women first responders) to confirm our results in such samples.
Finally, longitudinal intervention studies with large samples of trauma workers could be analysed with different statistical approaches such as latent profile transition analysis (Muthén & Muthén, 2000; Ram & Grimm, 2009) to test whether empathic styles can change over time as a result of organizational intervention attempts, such as being mitigated or modified to a lower-risk style with vocational coaching or training.
Conclusion
The current study surveyed workers who face others’ trauma regularly on their work shifts, and extracted three distinct empathy profiles of trauma workers. A ‘self-focused’ empathic style (dominated by high personal distress responding) was associated with worse work wellness, efficacy, and fit. An ‘other-focused’ empathic style (dominated by perspective taking and empathic concern) was associated with better outcomes for trauma workers, and a novel ‘low-reactivity’ profile (characterized by markedly low empathy on all four IRI facets) had the most positive work outcomes of all three groups. We therefore conclude that the answer to the quandary of dispositional empathy and trauma work is that “the full profile matters”. Dispositional empathy should be measured at the holistic profile level to appropriately guide prospective trainees in these professions and to help them avoid burnout, turnover, and the psychological and physical distress from negative coping strategies reported in previous literature.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canada Graduate Scholarship – Master’s and Nova Scotia Graduate Scholarship – Master’s programs.
Ethical Statement
Data Availability Statement
The data that support the findings of this study are not publicly available as they are subject to participant privacy and confidentiality.