
Abstract
Introduction
Telomerase reverse transcriptase (TERT) promoter mutations is a relatively novel mutation that has been linked with thyroid cancers. This study examines the frequency, cytology and histo-morphologic features, and clinical outcomes of TERT-mutated indeterminate thyroid nodules.
Methods
A retrospective review of Bethesda III and IV thyroid cytology specimen sent for ThyroSeq® testing (2019-2022) was performed, selecting those with TERT mutations. Demographics, cytologic features, surgical diagnoses, and follow-up data were analyzed.
Results
Among 567 specimens tested, 12 (2%) harbored TERT mutations; 4 had TERT alone, and 8 had additional mutations. Average age of patients was 69 years (92% > 50 years). Eight had surgical follow-up: 50% were malignant, 25% were benign and 25% were of uncertain malignant potential. Additionally, 62% were oncocytic nodules. Clinical follow-up showed all evaluated patients were alive without recurrences or metastases at last contact.
Conclusion
In our cohort, TERT promoter mutations were rare in indeterminate thyroid nodules (2%) and frequently accompanied by additional molecular changes. It is more frequently detected in older patients. Unlike prior reports describing TERT mutations exclusively in malignant thyroid tumors, our findings encompassed a broader histological spectrum, including benign, uncertain malignant potential and malignant lesions.
Keywords
Introduction
Thyroid cancers have been known to harbor various molecular alterations. Telomerase reverse transcriptase (TERT) promoter mutations is a relatively novel mutation that has been linked with thyroid cancers such as papillary thyroid carcinoma (PTC), follicular thyroid carcinomas (FTC), poorly differentiated thyroid carcinoma, and anaplastic thyroid cancers but not in medullary thyroid carcinoma. 1 The most common TERT promoter mutations are C228T and C250T, with C228T being more common in thyroid cancers. Clinically, TERT-mutated thyroid cancers tend to have poor outcomes and aggressive disease courses, including tumor metastasis, recurrences, and early mortality.2,3 TERT promoter mutations may be seen with other gene mutations, particularly BRAF V600E and RAS mutations, with studies showing a higher incidence of TERT mutation in BRAF-mutated lesions compared to BRAF-wild type. 4 There have been reports of TERT promoter mutations being associated with increased mortality in patients with differentiated thyroid cancer independently. 5 Additionally, few studies have shown that TERT promoter mutations, especially in PTC, have been known to be associated with extrathyroidal extension, 6 vascular invasion, 7 lymph node metastasis, 8 and distant metastasis. 9 TERT promoter mutations have also been associated with advanced TNM stages in both PTC as well as in FTC compared to those that did not demonstrate a TERT mutation.2,3
In this case series, we aim to understand the frequency of TERT promoter mutations in cytologically indeterminate thyroid nodules (Bethesda III and IV), any cytomorphologic feature associated with the presence of TERT, its histologic characterization, and clinical outcomes.
Methods
Our cytology database was searched to identify thyroid cytology specimens categorized as Bethesda Category III or IV that were reflexed to ThyroSeq molecular testing between 2019 and 2022. Of them, specimens that resulted in having a TERT mutation were selected for our study. Demographic details, including age and gender, size of the thyroid lesion, location of the lesion, surgical follow-up, and diagnosis, as well as clinical follow-up was obtained from chart review. The cytology and surgical slides were evaluated by a pathologist to confirm the diagnosis. This study received approval from the institutional review board.
Results
A total of 567 indeterminate thyroid cytology specimens were reflexed to ThyroSeq molecular testing, of which 235 (41%) demonstrated a positive molecular finding. Among the specimens demonstrating positive results, 5% (12/235) harbored a TERT mutation. Of the 12 TERT-mutated lesions, 4 had TERT as the sole molecular alteration, while 8 exhibited TERT mutations along with additional molecular findings (see Table 1).
Demographic Details, Cytology Diagnosis, Surgical Follow-Up, and Clinical Follow-Up of TERT-Mutated Thyroid Nodules in Our Study Cohort.
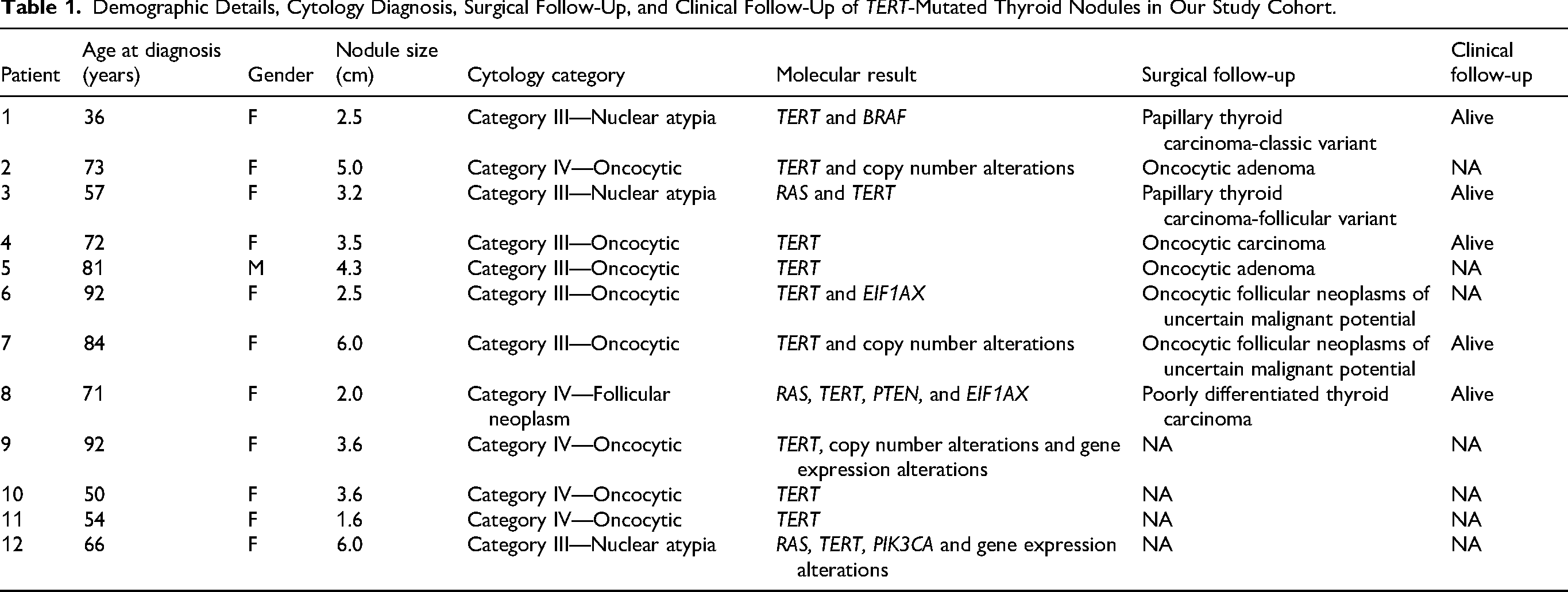
Patient ages ranged from 36 to 92 years, with a mean age of 69 years; 11 of 12 patients were older than 50 years. Regarding gender distribution, there was a preponderance of female patients (92%; 11 of 12). Lesion sizes varied from 1.6 cm to 6 cm, with an average size of 3.6 cm; 4 of 12 had lesions larger than 4 cm. Lesion locations included the right lobe (n = 5), left lobe (n = 4), and isthmus (n = 3).
Surgical follow-up was available in 8 of 12 (67%). The surgical diagnoses in these 8 specimens were PTC (n = 2), oncocytic adenoma (n = 2), oncocytic follicular neoplasm of uncertain malignant potential (n = 2), oncocytic carcinoma (n = 1), and poorly differentiated thyroid carcinoma (n = 1). Two of these 8 specimens showed TERT as the sole mutation, which, on surgical follow-up, were oncocytic adenoma (Figure 1) and oncocytic carcinoma. Another oncocytic adenoma in the cohort demonstrated both copy number alterations and TERT mutations. Of the two PTCs in the cohort, one was a classic variant, demonstrating BRAF and TERT mutation, while the other specimen was a follicular variant of PTC demonstrating RAS and TERT mutations. The poorly differentiated thyroid carcinoma exhibited a complex molecular profile with TERT, RAS, PTEN, and EIF1AX alterations. Focal angioinvasion was observed in 3 out of 8, including poorly differentiated thyroid carcinoma, oncocytic carcinoma, and follicular variant PTC. Lymphatic invasion was identified only in the poorly differentiated thyroid carcinoma; however, lymph node dissection was not performed. Only one had lymph node metastasis, the lesion being a classic variant PTC. Within our cohort, perineural invasion or extrathyroidal extension was not identified. Clinical follow-up was available for 5 of the 8 surgically treated patients, all of whom were alive at last follow-up, with no reported recurrences or distant metastases.

Representative images of follicular neoplasm-oncocytic on cytology and oncocytic adenoma on surgical resection. (A) Smear showing sheets and clusters composed exclusively of oncocytic cells (Pap stain, 4X). (B) Oncocytic cells with enlarged nuclei, occasional prominent nucleoli, and abundant granular eosinophilic cytoplasm (Pap stain, 40X). (C) Resected oncocytic adenoma with adjacent compressed normal thyroid follicles (lower left). FNA-related changes are present in the upper right, with scar tissue and hemosiderin-laden macrophages (H&E stain, 4X). (D) Follicles lined exclusively by oncocytic cells (H&E stain, 20X).
Discussion
Thyroid cancer develops and progresses through the gradual accumulation of early and late genetic and epigenetic changes that activate the MAPK and PI3K-AKT signaling pathways. 10 TERT promoter mutations in thyroid cancer are considered late genetic events, and their presence marks dedifferentiation and is known to contribute to the development of a more aggressive disease.11,12
In our case series, 2% of all indeterminate thyroid nodules tested, which constituted 5% of all those with a positive molecular finding, harbored TERT mutations. This is concordant with studies, including smaller studies including 1000 specimens and larger studies such as ones analyzing over 50,000 ThyroSeq® v3-tested nodules that found TERT mutations in 1.7% of indeterminate lesions.13,14
Generally, TERT mutations are known to be more common in the older age group.11,15 Our findings were in keeping with this with 92% being above 50 years of age. Within our study cohort, TERT mutations with other complex molecular alterations (51%) were much more common than sole TERT mutations (33%) and TERT with RAS (8%) and TERT with BRAF mutations (8%). Coexistence of TERT with BRAF mutations has been reported in the past and is known to be associated with aggressive histopathological features, such as tall cell variant PTC, and also confers a higher risk of recurrence. 7 The TERT- and BRAF-mutated thyroid lesion demonstrated classic PTC, and the patient is alive on follow-up with no recurrences or metastasis.
The cytologic findings varied and consisted of oncocytic cell predominance (8 of 12 specimens), cytologic atypia with nuclear changes (3 of 12 specimens), and architectural atypia with micro follicles (1of 12 specimens). Oncocytic cell predominance was the most common cytologic finding in our study (67% of all specimens). Similarly, oncocytic nodules were the most common surgical diagnosis (5 out of 8 specimens). In the literature, RAS family mutations are the most common molecular alterations identified in oncocytic nodules, with TERT being far less frequently described.16–21 In our cohort, none of the 8 specimens with oncocytic cell predominance were associated with RAS family mutations. The two specimens that showed nuclear atypia and had surgical follow-up were associated with BRAF or RAS mutations in addition to TERT mutations and, as expected, were classic and follicular variant of PTC, respectively.
The majority of the studies have shown that TERT mutations are usually associated with malignant thyroid lesions and not detected in benign entities.1,6,22 However, in our study, of the resected lesions, 50% were malignant, 25% were benign, while 25% were of uncertain malignant potential. The two benign lesions were oncocytic adenomas. A study by Pinto et al that investigated 77 TERT-mutated indeterminate thyroid nodules revealed that 84% of their cohort were malignant, while 16% were benign. 23 A recent study by Alzumaili et al demonstrated that in a cohort of 52 specimens that had TERT mutations without concomitant BRAF mutation, 35% were either benign or low-risk thyroid neoplasms. 24
Within our study cohort, the management TERT-mutated nodules was variable with no surgical resection in 4, total thyroidectomies in 5, and lobectomies in the remaining 3. The molecular finding of only TERT mutations or TERT mutations with additional molecular aberrations did not determine whether the nodule was resected (total or lobectomy) or not resected. TERT mutations did not seem to influence management. Single TERT-mutated lesions underwent total thyroidectomies if the patient had substernal goiters clinically. On the other hand, nodules with TERT mutations with additional molecular findings were not all resected; only some with additional cytologic atypia were resected.
TERT-mutated lesions have been known for their aggressive disease course, including recurrences and distant metastasis.2,3 However, clinical follow-up of our study cohort did not demonstrate early mortality or tumor recurrences and metastasis. This is probably due to an intense, advanced targeted surgical approach or probably due to a short follow-up interval based on our study years.
Conclusion
Our study highlights that TERT promoter mutations, while relatively infrequent in indeterminate thyroid nodules (2% in our cohort), occur predominantly in older patients and often coexist with other molecular alterations. Our study findings contradict the well-known and published facts regarding the occurrence of TERT mutations solely in malignant thyroid lesions as our study has a wide spectrum of histologic outcomes, including both benign and malignant entities. Similarly, although TERT mutations have been linked to aggressive disease, our cohort did not demonstrate early recurrences or metastases on follow-up, suggesting that molecular context, histologic subtype, and clinical management all play critical roles in patient outcomes. These findings support the need for multidisciplinary approaches to risk stratification and treatment planning in patients with TERT-mutated thyroid nodules.
Footnotes
Ethical Approval and Informed Consent Statements
This study received approval from the institutional IRB with waiver of informed consent.
Author Contributions
SDG: project design, project supervision, data collection, data analysis, and manuscript writing. NS: data collection and image acquisition. KC: data collection. KD: project design, project supervision, slide review, and manuscript editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available only upon request due to ethical considerations.