
Abstract
Idiopathic granulomatous mastitis (IGM) is a chronic inflammatory breast disease. Patients typically present with a painful or painless mass and signs of inflammation. While IGM is already rare in women, only a few male patients have been reported in the literature. In this article we present the case report of a 63-year-old male patient with IGM, which clinically and radiologically mimicked male breast cancer. Radiological findings in the patient were nonspecific. Definitive diagnosis was made by histopathological evaluation. Surgical excision was performed as a treatment modality. No recurrence or residual lesion was detected in postoperative follow-up.
Introduction
Granulomatous mastitis is a chronic inflammatory breast disease first described by Kessler and colleagues in 1972. 1 Without any specific infectious cause are classified as idiopathic granulomatous mastitis (IGM). Patients typically present with a painful or painless mass and signs of inflammation, which can often mimic breast cancer. A definitive diagnosis requires biopsy, with non-caseating granulomas being the characteristic finding. 2
Clinical presentations may vary. Severe examples of IGM can lead to abscess formation, sinus tracts or fistulas, and ulcerative lesions in the breast. 3 Treatments include antibiotics, oral or intralesional corticosteroids, non-steroidal immunosuppressive agents, and surgical excision. However, optimal treatment modality remains debated. 4
Although IGM is more commonly seen in women of reproductive age, with onset typically in the 30 s, there are striking regional differences in its prevalence, with it being more common in Middle Eastern countries. 5 While IGM is already rare in women, only a few male patients have been reported in the literature.6,7,9,12–18 This study presents the case report of 63-year-old male patient with IGM who presented with a breast mass complaint.
Patient Presentation
A 63-year-old male patient presented with a palpable mass in his right breast. His symptoms had begun 15 days earlier, without accompanying pain, redness, or warmth. His medical history was significant only for hypertension. On physical examination, a 1 cm, immobile, well-defined, smooth-surfaced, painless mass was palpated in the 1 o’clock position of the right breast. Axillary examination was normal.
Considering the patient's age and the palpable mass, a mammography was performed. It revealed no gynecomastia in either breast but identified a sharply defined 9 × 8 mm mass with moderate density and coarse calcifications in the upper inner quadrant of the right breast (Figure 1). Ultrasonography showed a circumscribed isoechoic 6.5 × 5 mm mass at the same location, with slightly increased echogenicity around the mass. No pathological lymph nodes were detected in either axilla. The lesion was categorized as BI-RADS 4, and core needle biopsy was planned. Ultrasound-guided core needle biopsy was performed using a 14G tru-cut needle (Figure 2). Histopathological analysis confirmed the diagnosis of nonspecific granulomatous mastitis (CD68(+), keratin (AE1/AE3)(-)) (Figure 3).
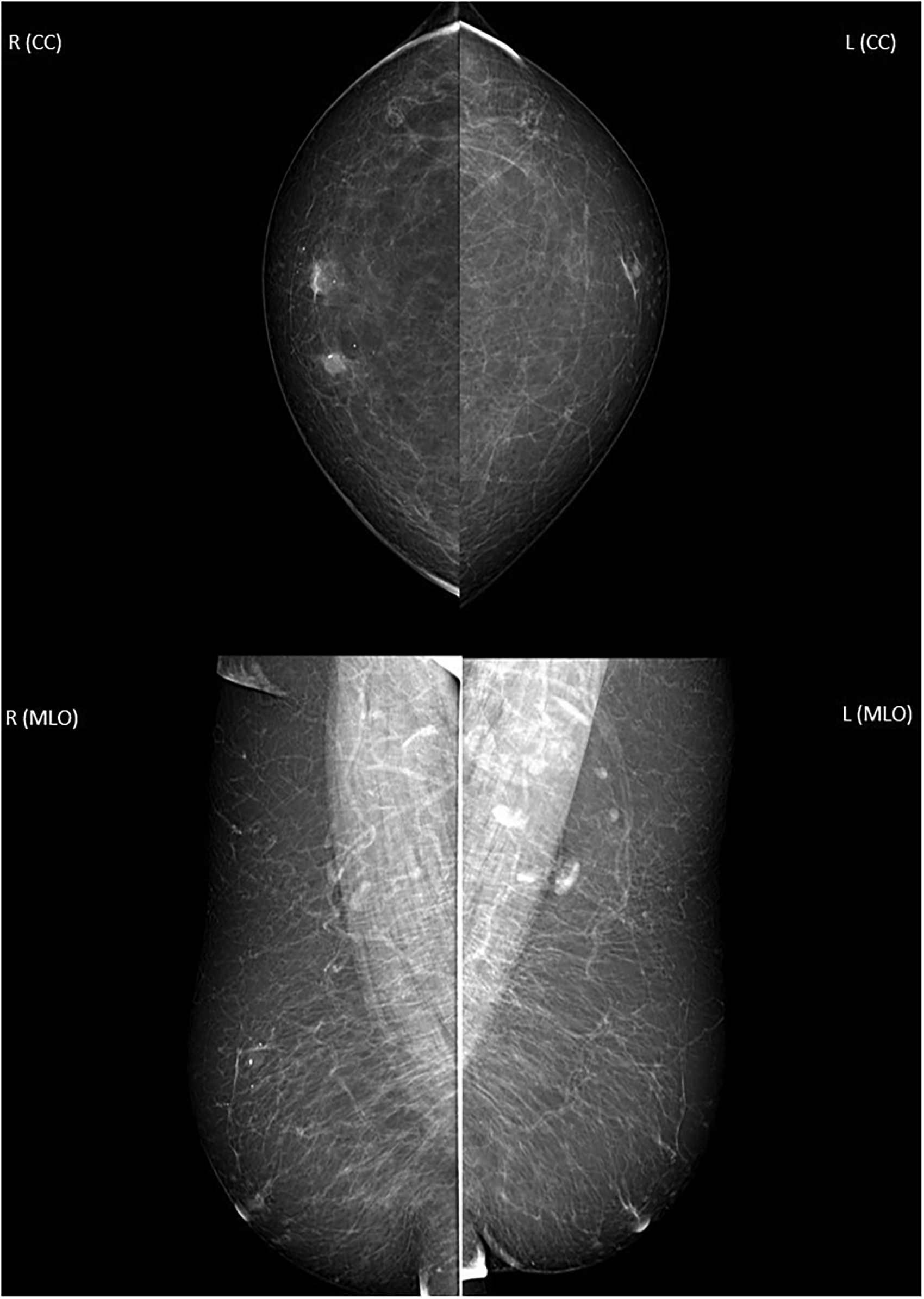
In mammography, a well-defined mass measuring 9 × 8 mm is observed in the upper inner quadrant of the right breast. Isodense mass contains coarse calcifications.
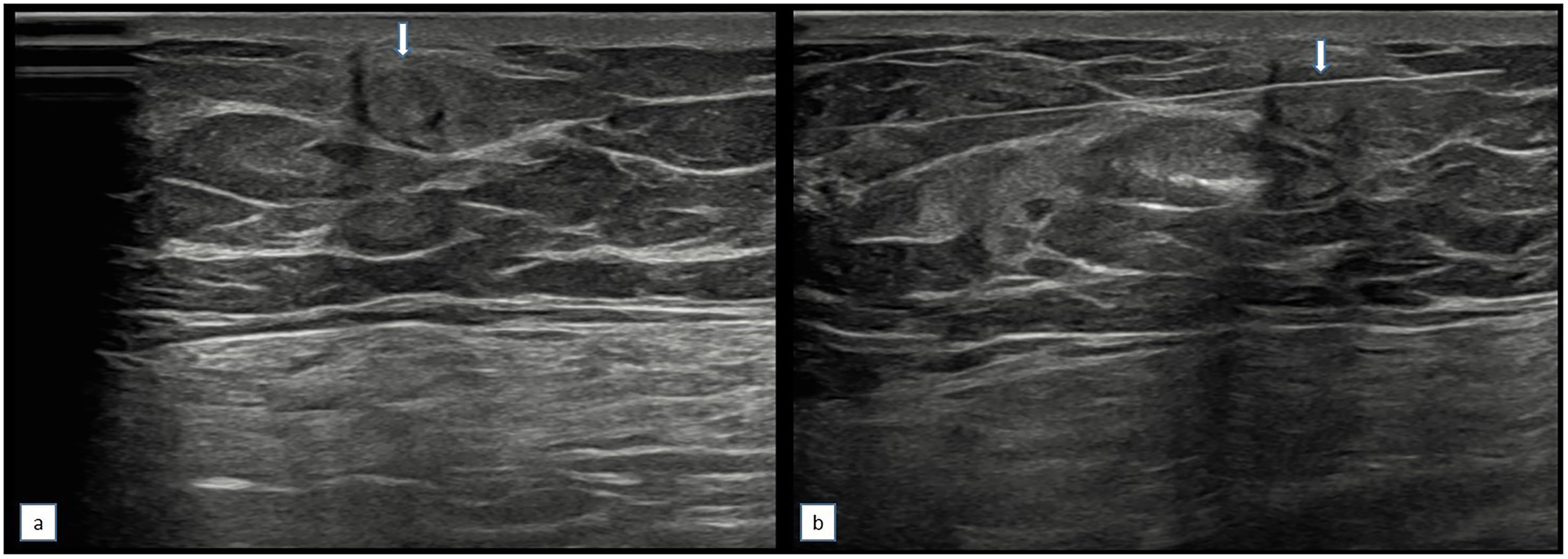
(a) On ultrasonography, a circumscribed iso-echoic mass with slight peripheral increased echogenicity is observed (arrow). (b) In the ultrasound-guided biyopsy the needle is shown (arrow).
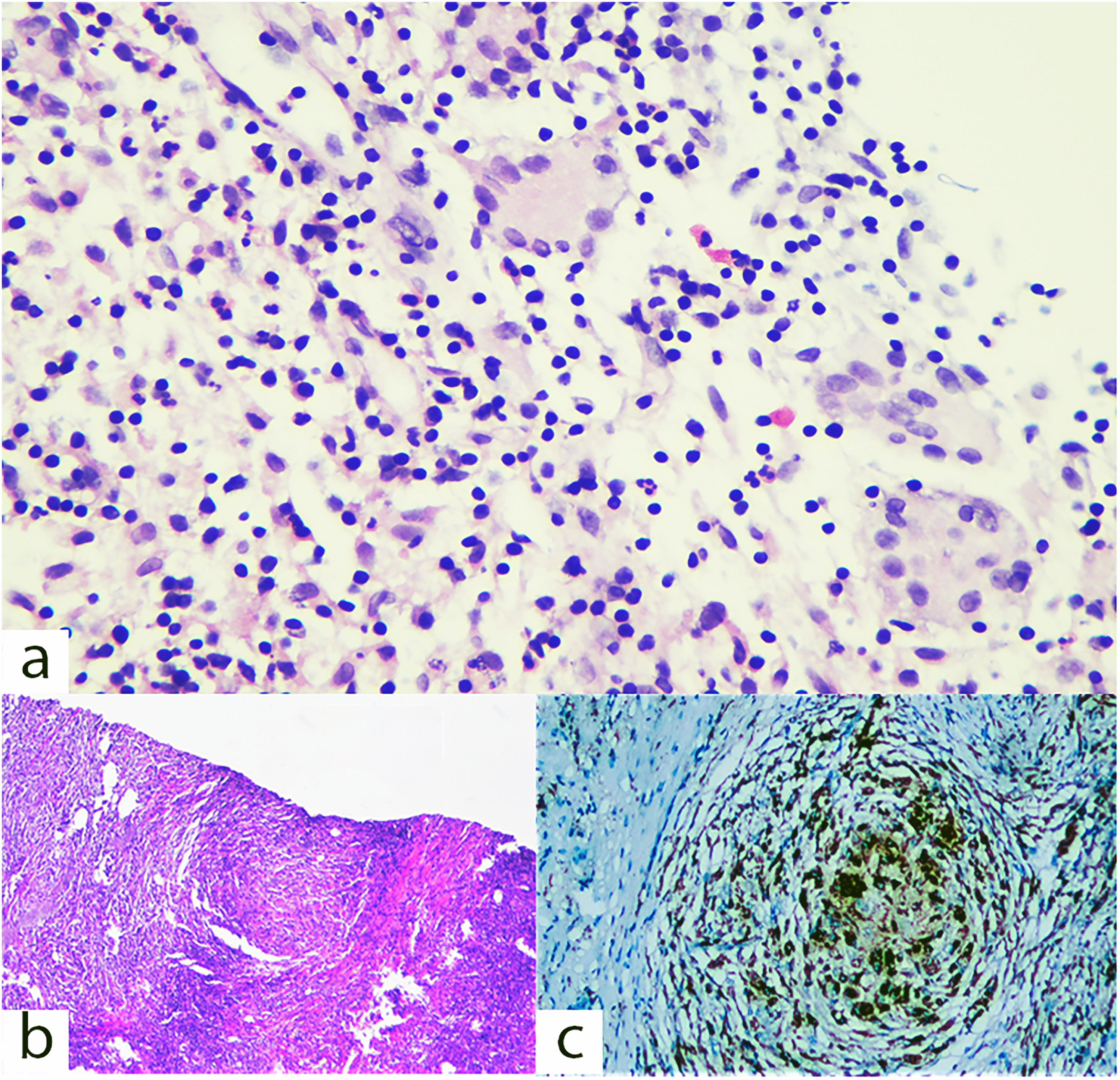
(a) x200 close-up view of giant cells within granulomas, (b) x40 granuloma structures composed of epithelioid histiocytes and lymphocytes stained with HE, (c) x100 immunohistochemical staining showing CD68(+) histiocytes.
Laboratory tests revealed slightly elevated white blood cell counts (11.29 μg/L), neutrophils (6.57 μg/L), and monocytes (0.90 μg/L). The percentage of immature granulocytes was five times the upper limit of normal range (0.3%, reference range: 0-0.06%). Purified protein derivative skin test, quantiferon test, anti-Toxoplasma IgG/IgM, Brucella coombs gel test and anti-syphilis antibody test were all negative. C-reactive protein and sedimentation rate were normal.
Despite the nonspecific radiological findings, a mismatch between radiology and pathology raised the suspicion of male breast cancer, leading to surgical excision of the lesion. Pathology report confirmed granulomatous mastitis (dimensions of excised tissue: 4.4 × 3 × 2.8 cm). It was observed that no specific microorganism grew in the culture sample sent from the excision material. In addition, negative results were obtained with histochemically applied Giemsa and Ziehl-Nelson staining. Postoperative follow-ups showed no additional pathological findings. At the one year postoperative ultrasound, no recurrence or residual lesion was detected.
Discussion
Although granulomatous mastitis is typically considered a disease of women, it can, albeit rarely, present in males. What makes this case report notable is that it is among the few male patients documented in the literature.6,7,9,12–17 Clinically, IGM often mimics breast cancer, with most patients presenting with a painful or painless palpable mass.6–18 Similarly, in this patient, presenting symptom was a painless palpable mass that clinically resembled male breast cancer. Radiological findings were nonspecific, and a definitive diagnosis was only made through histopathological evaluation.
The age range for IGM in males is variable. In a recent review of case reports between 2003 and 2022, the age range was found to be between 17 and 63. 7 Patients as young as 17 years, associated with hidradenitis suppurativa, 6 have been reported. It is noteworthy that our patient was also 63 years old and was diagnosed at an advanced age.
Histopathologically, IGM is characterized by granulomas consisting of histiocytes, lymphocytes, and neutrophils. These findings are nonspecific. Differential diagnoses include cystic neutrophilic granulomatous mastitis, tuberculosis, sarcoidosis, and foreign body reactions. 8 In our patient, no underlying condition was identified as a potential cause of the clinical entity.
The etiology of the disease remains idiopathic. Some studies suggest that hyperprolactinemia or hormonal imbalances in sex hormones may play a role. In male patients with IGM associated with gynecomastia, prolactin levels have been found to be elevated.9,10 However, in our patient, there was no radiological evidence of gynecomastia, nor was there a history of exogenous hormone use.
IGM in men may present as asymmetric density, irregularly shaped masses resembling breast cancer, or as density indistinguishable from gynecomastia on mammography. On ultrasonography, it typically appears as a hypoechoic mass with a heterogeneous internal structure. 11 In our patient, mammography revealed a sharply defined, isodense mass, while ultrasonography showed an isoechoic, circumscribed lesion. Radiological findings in male IGM are nonspecific and can closely mimic breast carcinoma. For this reason, biopsy and histopathological evaluation are necessary for diagnosis. 12
Treatment approaches for IGM vary and include observation, surgical excision, corticosteroids, and immunosuppressive drugs. No standard treatment protocol has been established yet. In male IGM patients, local excision has been reported as an effective treatment option.13–15 Corticosteroid therapy is also a significant treatment alternative,16,17 while some patients have been managed with observation alone. 18 In this patient, surgical treatment was performed, and the patient's postoperative examination at 1 year revealed no recurrence or residual lesion.
There is no specific blood test for the diagnosis of IGM. However, high inflammation parameters may be significant. A recent study emphasized that blood IgA and C reactive protein levels are high in IGM patients. 19 In our patient, C-reactive protein level was found to be normal. However, the percentage of immature granulocytes was found to be 5 times higher than the upper limit.
Conclusion
IGM is exceedingly rare in male patients. It can clinically and radiologically mimic breast cancer. Definitive diagnosis is established through histopathological evaluation following a core biopsy. Early diagnosis is critical to avoid delays in treatment, which directly impacts therapeutic success.
Footnotes
Acknowledgments
We would like to thank Andaç Can for his contributions to this study
Ethical Approval
Written informed consent was obtained from the individual for the publication of any potentially identifiable images or data included in this article.
Author Contributions
Funding
This study received no outside funding.
Conflict of Interest Statement
Authors have no conflicts of interest to declare.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Statement of Ethics
Ethical approval from the Ethical Review Board was not applicable for this study. Ethical approval was not required for this study in accordance with local/national guidelines. Written informed consent was obtained from the patient for publication of this case report and any accompanying images.