
Abstract
Appendiceal neoplasms are an incidental finding in <1% of all appendicectomy specimens. Their incidence rates are largely based on appendectomies performed for appendicitis. Appendicectomy is often performed as part of cytoreductive surgery for gynecological malignancies. This is to reduce the risk of occult metastatic disease and to mitigate the morbidity of acute appendicitis in patients undergoing chemotherapy for cancers. The objective of this study was to investigate the incidence of primary lesions of the appendix in 2 cohorts of patients who underwent appendicectomy: patients who had surgery for mucinous neoplasms of the ovary and patients who had cytoreductive surgery for gynecological malignancies. This study looked at the histopathology reports of 581 patients covering both cohorts. Appendicectomy in the setting of mucinous neoplasms of the ovary was done in 187 patients and as part of cytoreductive surgery for gynecological malignancies in 182 patients. We used the updated 2019 WHO nomenclature to classify the appendiceal lesions. The 2 cohorts had an incidence of 13% (25/187) and 7% (12/182) of appendiceal lesions. The appendix was noted to be the frequent primary site of extraovarian mucinous tumor metastasis to the ovary with a frequency of 56% (14/25) in patients with mucinous ovarian tumors; the highest cited in literature to date. We also noted poor correlation between gross and microscopic confirmation of appendiceal lesions with 7% of all macroscopically normal appendices harboring an appendiceal pathology. The study highlights the importance of appendicectomy during surgery for ovarian mucinous neoplasms and as part of cytoreductive surgery for gynecological malignancies. It also signifies the importance of microscopic examination of the whole appendix, especially when no gross abnormality is detected.
Introduction
The incidence of appendiceal cancer is low and it is predominantly an incidental diagnosis 1 found in less than 1% of all appendicectomy specimens.2–4 Because of their rarity, they also pose a challenge for clinicians and radiologists alike. An appendicectomy in the setting of a gynecological malignancy is often performed as part of cytoreductive surgery because of the risk of occult metastatic disease and to mitigate the morbidity of acute appendicitis in patients undergoing chemotherapy for ovarian cancers. Moreover, in the setting of mucinous ovarian neoplasms, an appendicectomy can help in ascertaining or excluding the appendix as the site of primary cancer.5,6
There have been recent advances in the understanding and the nomenclature of appendiceal neoplasms. For instance, the goblet cell carcinoid is renamed as goblet cell adenocarcinoma in view of the potential aggressive behavior of this entity. 7 Moreover, previously benign entities like hyperplastic polyps are considered neoplastic in view of emerging mutation found in these lesions. 7 Hence, keeping abreast with these changing terms is ever more important for gynecological pathologists to not only accurately diagnose and timely refer to the gastrointestinal team but also for better management of these patients with concomitant appendiceal pathologies. Further surgeries, like right hemicolectomies, may be mandated depending on the size and the stage of tumor and the clearance of margins.7–9
The role of appendicectomy in the setting of malignant ovarian neoplasms is well studied and hence submission of appendix at the time of such surgery is a frequent occurrence. The rate of appendiceal pathology has ranged from 4.97% to 24% in women undergoing appendicectomy for mucinous ovarian neoplasms.10–12 However, the role of an appendicectomy in gynecological cancers other than mucinous lesions of the ovary is not well reported in the literature.
The literature is divided when it comes to performing appendicectomy as part of primary gynecological surgery. Most studies advocate looking at the macroscopic appearance of the appendix at the time of primary surgery to ascertain the need for removal.13–15 Some studies also add weightage to frozen section diagnosis of the ovarian pathology and believe that this in combination with the macroscopic appearance of the appendix are significant predictors of coexisting appendiceal pathology. 5 However, the presence of significant appendix pathology in around 6% of the macroscopically normal appendix is also a statistic that cannot be ignored. 16 This coupled with the fact that an appendicectomy does not increase morbidity in patients undergoing cytoreductive surgery, is another argument in support of appendicectomy. 16
Primary cytoreductive surgeries are performed with the aim of complete debulking and no residual disease remaining, thereby allowing for accurate FIGO staging.17,18 Studies that have looked at removal of the appendix and the incidence of metastasis in ovarian carcinoma have found that high stage (III-IV) tumors have increased incidence of appendiceal metastasis.19–21 Moreover, older age (>50 years) and omental involvement, which confers a higher stage, have been cited as significant risk factors for appendiceal involvement by metastasis. 22
Mucinous tumors in the ovary may be primary or metastatic, and immunostains may be helpful in distinguishing primary ovarian mucinous tumors from metastatic mucinous tumors, in some but not all tumors. A keratin immunoprofile of keratin 20 positive and keratin 7 negative suggests a lower gastrointestinal tract origin. Ovarian mucinous tumors usually express both Keratin 7 and Keratin 20, but some, such as mucinous tumors arising in a teratoma may show a keratin profile similar to that seen in tumors of lower gastrointestinal tract origin. Moreover, ovarian mucinous tumors can also express CDX2, known to be expressed in gastrointestinal tumors. 23 However, the expression of PAX8 supports a primary ovarian origin, but PAX8 is expressed in only a subset of primary ovarian mucinous tumors. 24 As the confirmation of a primary ovarian origin is not possible on the basis of morphology and immunoprofile in some tumors, removal of the appendix, which is a potential site of origin is a consideration in patient presenting with mucinous tumors in the ovary. A study looking at the role of appendicectomy in the setting of mucinous adenocarcinoma of the ovary advocated removal of the appendix. Despite a normal looking appendix in a minority of the specimens, there was disease on microscopy, thereby upstaging the tumor, which portends poor survival. 25
In this study, we investigated the incidence and types of lesions of the appendix in 2 cohorts of patients, including patients undergoing surgery for mucinous lesions of the ovary (Cohort 1) and patients undergoing cytoreductive surgery for other gynecological malignancies (Cohort 2). The primary objectives of the study were to identify the frequency of preforming appendicectomy for patients undergoing surgery for mucinous ovarian tumors, to identify the frequency of appendiceal lesions in patients undergoing surgery for mucinous tumors and in patients undergoing extensive cytoreductive surgery for different types of ovarian lesions, and the correlation between the gross appearance of the appendix and the presence of an appendiceal lesion.
Methods
Cohort 1
We reviewed the data of all surgeries performed for mucinous ovarian neoplasms from the database of the Department of Histopathology, Hammersmith Hospital, London, United Kingdom, over an 18-year period. All patients diagnosed with mucinous ovarian tumors were included as the aims of studying this cohort were to identify the frequency of performing appendicectomy in these patients and the frequency of appendiceal lesions identified in these patients. Data collected for these patients included age, appendicectomy (not performed, performed, if performed whether at the time of surgery for the ovarian tumor) subsequent or previous, macroscopic data including presence and type of appendiceal abnormality, embedding of the entire appendix, and type of appendiceal lesion confirmed on microscopic examination.
Cohort 2
Our second cohort comprised of patients who underwent appendicectomy as part of cytoreductive surgery for gynecological malignancies including but not limited to mucinous lesions of the ovary, over the course of 6 years. The aim of studying this cohort was to identify the frequency of appendiceal lesions identified in these patients. Data collected for these patients included age, macroscopic data including presence and type of appendiceal abnormality, and if a tumor deposit was noted on gross inspection of the appendix and whether this was confirmed microscopically.
Results
Cohort 1
For Cohort 1, 399 patients were identified. The median age of the patients was 53 years (range 17-94 years), of these, 187 patients had appendicectomy (47%), and of these 25 (13%, 25/187) patients had concomitant appendiceal lesions. The median age of patients with concomitant appendiceal lesions was 57 years (range 24-84 years).
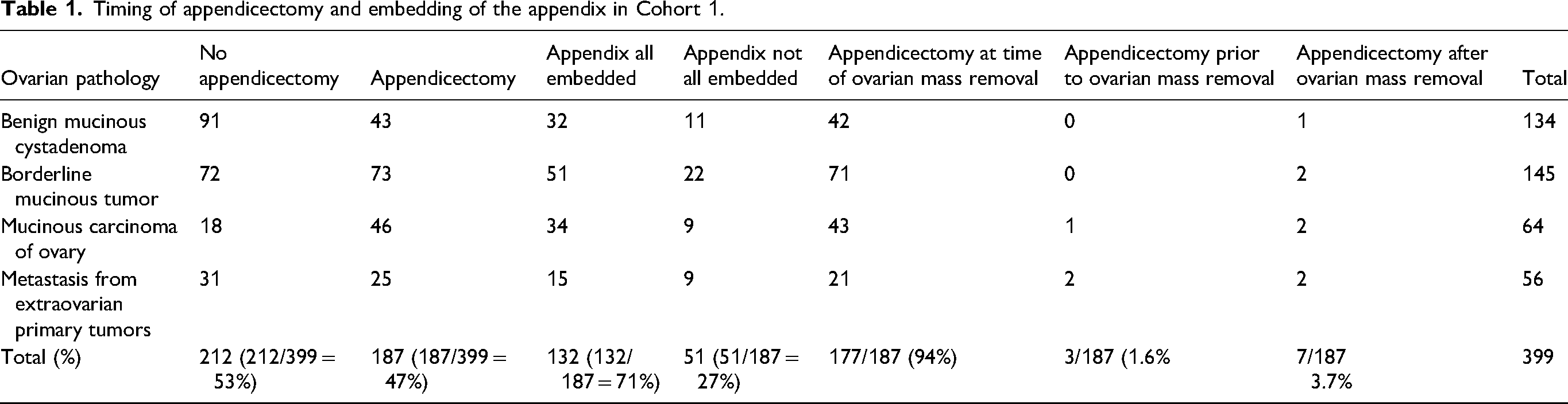
The mucinous ovarian neoplasms included benign mucinous cystadenoma; 134 (34%), borderline mucinous tumors; 145 (36%), primary mucinous carcinomas of the ovary; 65 (16%) and metastatic tumors to the ovary from extraovarian primary sites; 55 (14%). The timing of appendicectomy and processing of the appendix is presented in Table 1.
Timing of appendicectomy and embedding of the appendix in Cohort 1.
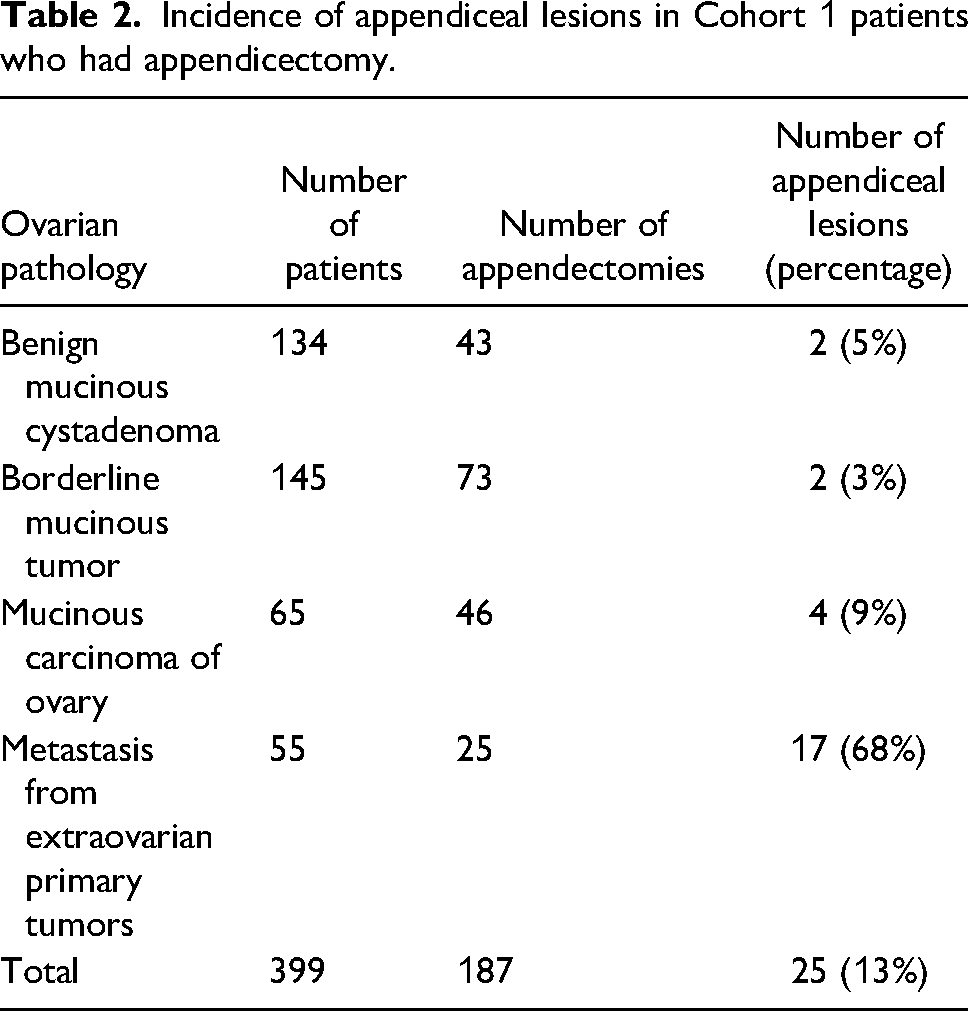
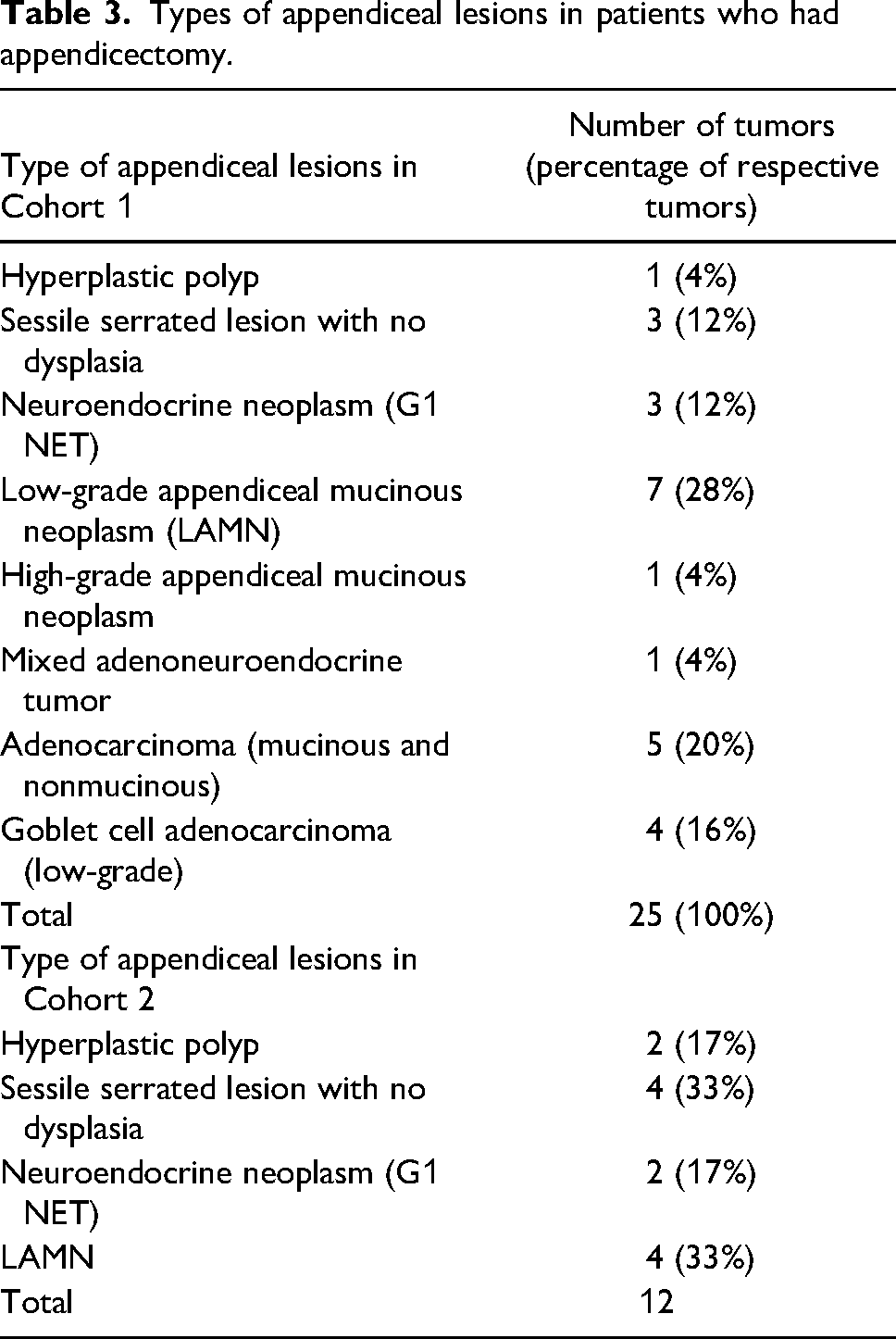
The incidence of appendiceal lesions in Cohort 1 patients who had appendicectomy was 13% (Table 2) with the majority of the appendiceal lesions being low-grade appendiceal mucinous neoplasm (LAMN) (28%) followed by adenocarcinoma (20%) (Table 3).
Incidence of appendiceal lesions in Cohort 1 patients who had appendicectomy.
Types of appendiceal lesions in patients who had appendicectomy.
Of the 56 patients where the mucinous lesion seen in the ovary was not considered primary, 17/25 (68%) patients who had an appendicectomy done had an appendiceal lesion. There were 14 primary appendiceal lesions, including LAMN, high-grade appendiceal mucinous neoplasm (HAMN) and adenocarcinoma including low-grade goblet cell adenocarcinoma that metastasized to the ovary. In 3 of these patients, the appendiceal lesion was not considered the primary site, as shown in Table 4. Figure 1 shows examples of metastatic tumors in the ovary.
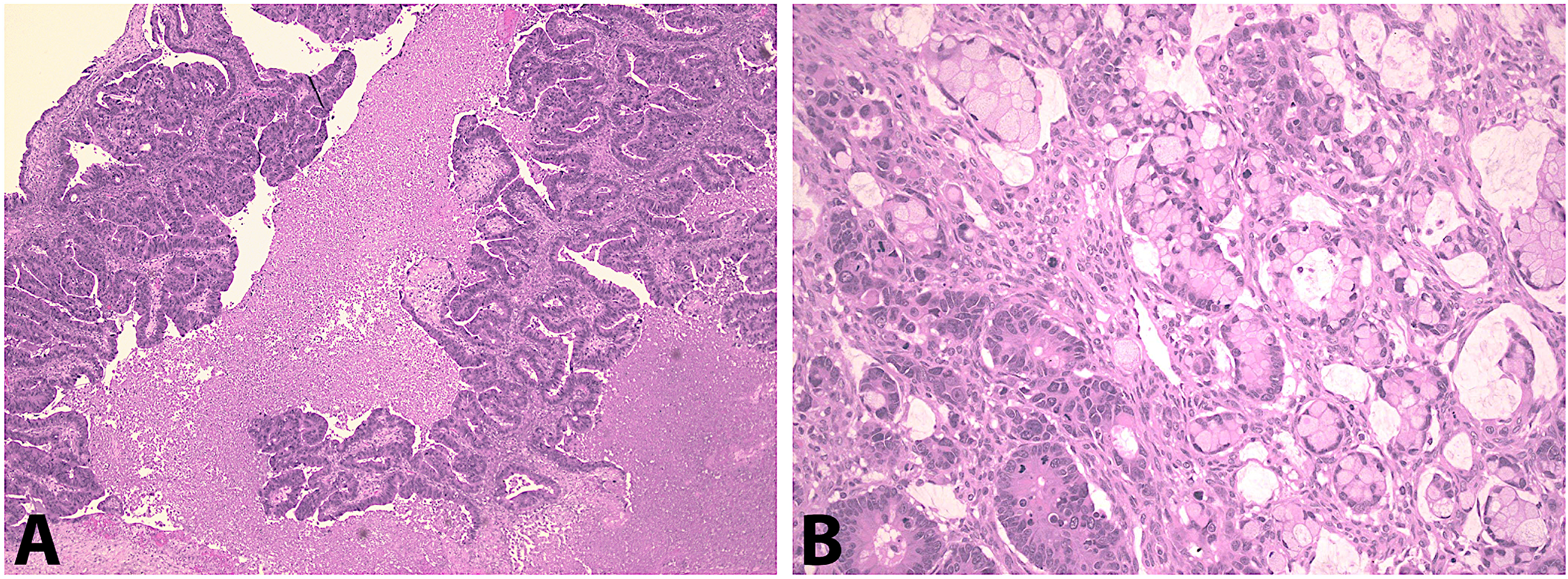
Metastatic tumors to the ovary: (A) metastatic adenocarcinoma, (B) metastatic goblet cell adenocarcinoma.
Distribution of appendiceal pathology in Cohort 1 and correlation with age, primary ovarian pathology, appendiceal pathology, macroscopic appearance of appendix, and site of primary tumor (where applicable and ascertained).
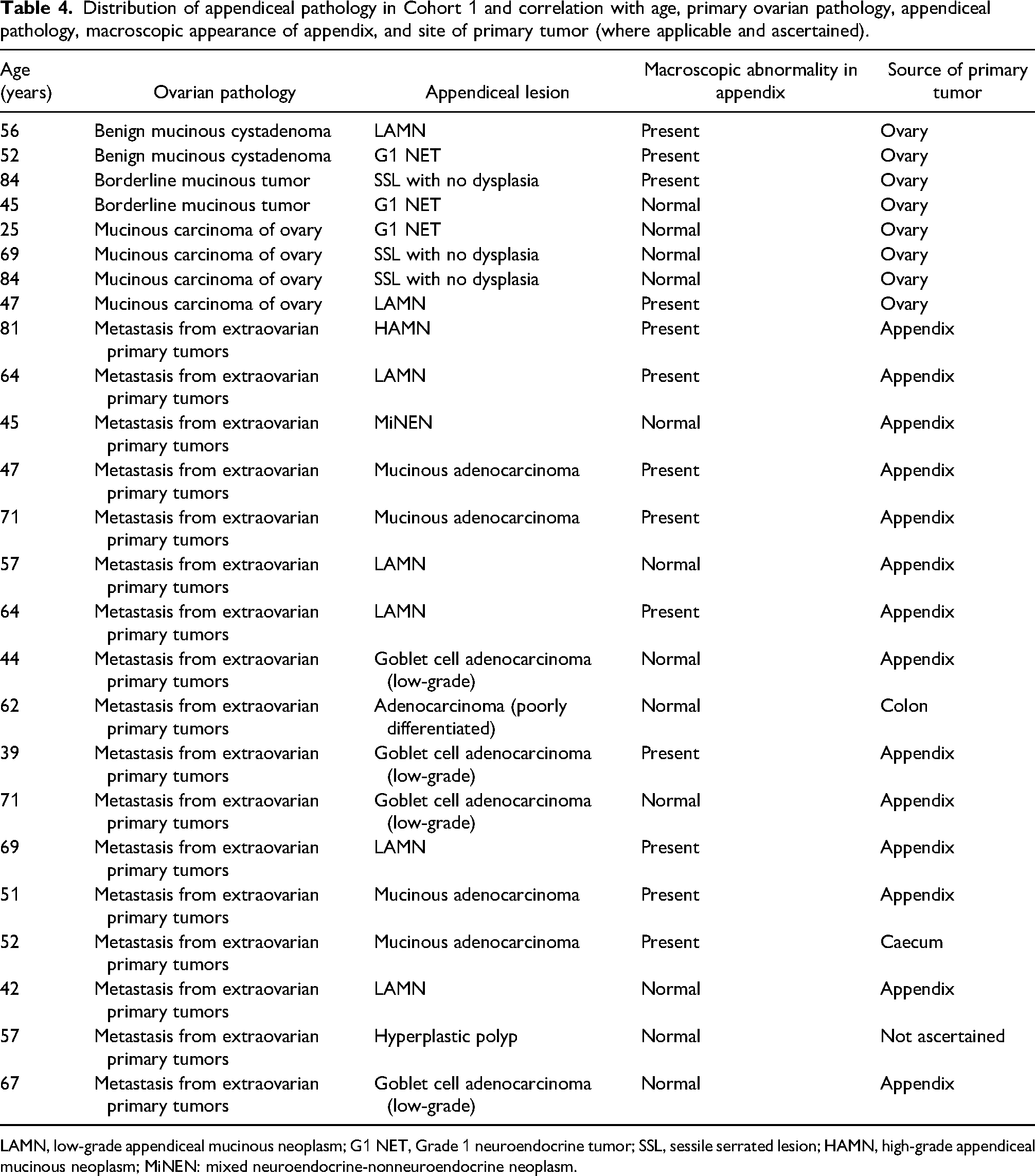
LAMN, low-grade appendiceal mucinous neoplasm; G1 NET, Grade 1 neuroendocrine tumor; SSL, sessile serrated lesion; HAMN, high-grade appendiceal mucinous neoplasm; MiNEN: mixed neuroendocrine-nonneuroendocrine neoplasm.
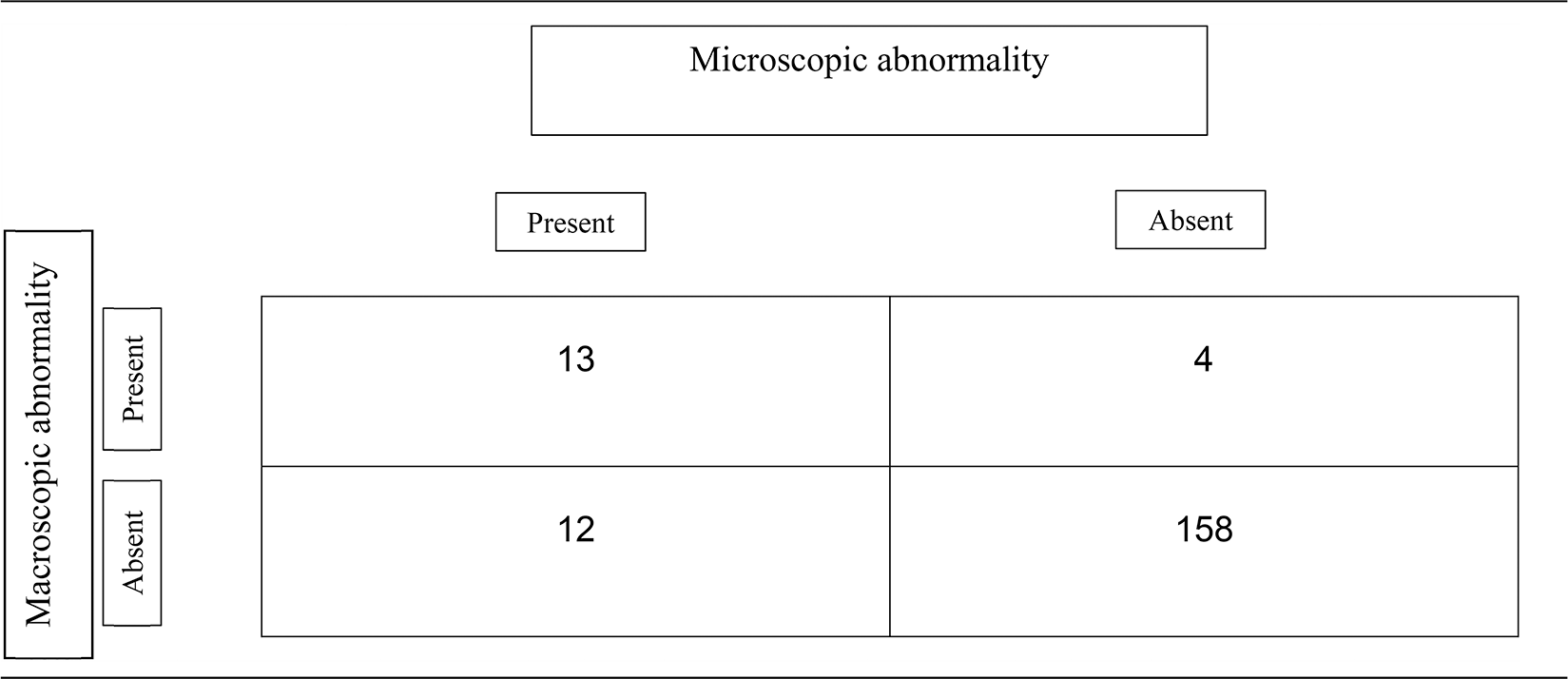
Despite a frozen section or radiological diagnosis of at least a borderline mucinous tumor of the ovary, an appendicectomy was performed in only 47% of the patients. It is also worth noting that when an appendicectomy was performed, the entire appendix was not submitted for histological assessment in 27% of the specimens. Table 5 illustrates the relation between macroscopic detection of an abnormality and microscopic confirmation; and in our series the sensitivity was only 52%.
Correlation between macroscopic detection of abnormality and microscopic confirmation of lesions in appendicectomies of Cohort 1 patients.
Cohort 2
For Cohort 2 a total of 182 patients were identified. The median age of the patients was 54 years (range 17-83 years). All patients had appendicectomy. An appendiceal lesion was identified in 12 patients (6.5%), whose median age was 61 years (range 48-77 years).
The appendiceal pathology included LAMN in 4/12 (33%), well differentiated (Grade 1) neuroendocrine tumor in 2/12 (17%), sessile serrated lesion with no dysplasia in 4/12 (33%) and hyperplastic polyp in 2/12 (17%) patients (Table 6).
Distribution of appendiceal pathology in Cohort 2 and correlation with age, primary gynecological cancer type, appendiceal pathology, macroscopic appearance of appendix, and microscopic confirmation of tumor deposit.
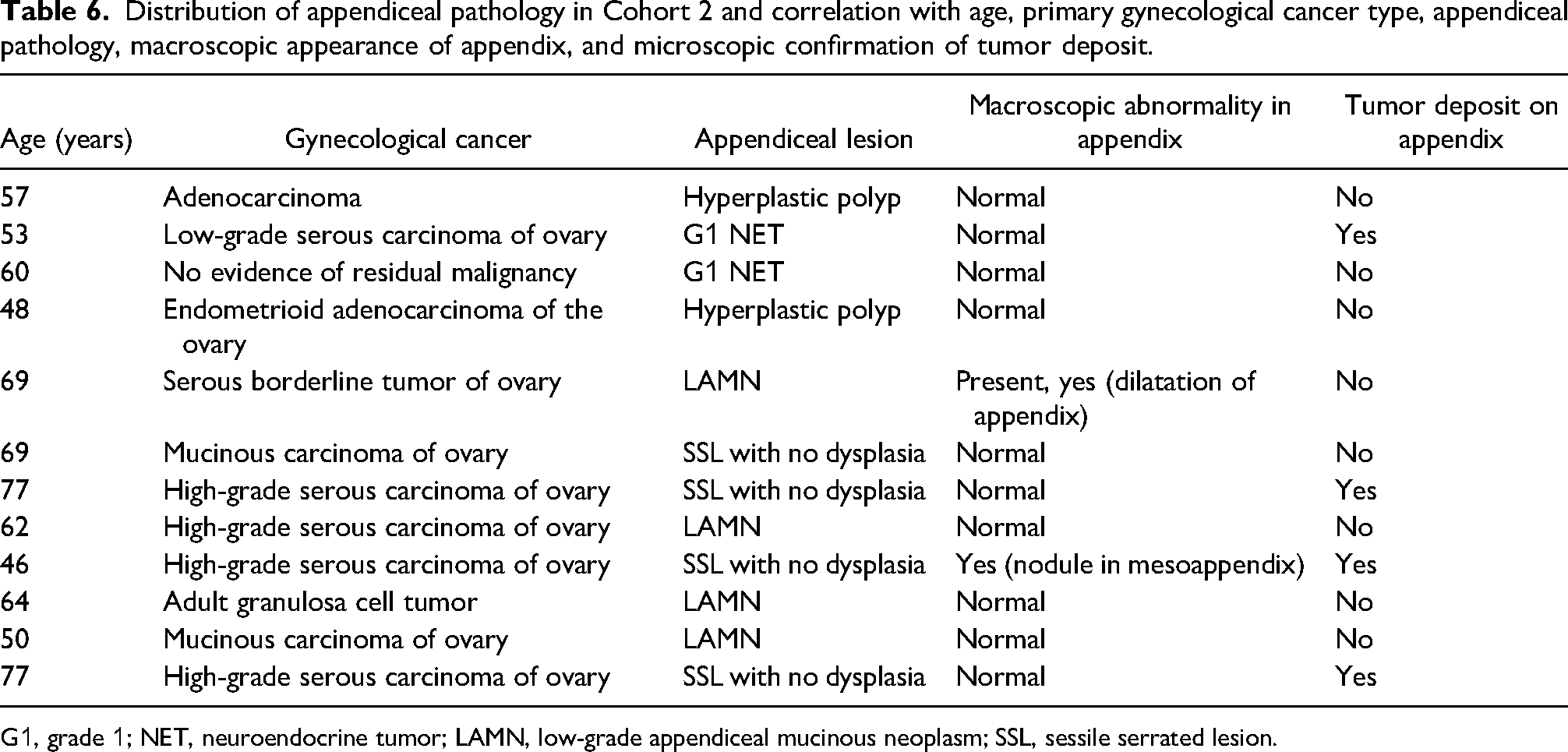
G1, grade 1; NET, neuroendocrine tumor; LAMN, low-grade appendiceal mucinous neoplasm; SSL, sessile serrated lesion.
In Cohort 2, a macroscopic abnormality in the form of dilatation of the appendix was only noted in one of the 12 specimens (8%). A tumor nodule was identified grossly in another specimen, while tumor deposits were confirmed microscopically in 4 out of the 12 specimens (33%). There was no association of any particular gynecological cancer type with the presence of appendiceal lesions (Table 6).
Appendicectomy was performed in all patients of Cohort 2. The whole appendix was submitted for histological assessment in only 53% of the patients. Of the 12 patients with the appendiceal pathology, only 4 had their entire appendix submitted for histological assessment.
In addition to the finding of primary appendiceal lesions, a metastatic deposit of primary gynecological cancer was noted in the appendiceal wall or the mesoappendix in only 36% (66/182) of the patients.
Discussion
Our study, with a total cohort size of 581 patients, is one of the largest of its kind, looking specifically at the incidence of primary lesions of the appendix in the setting of surgery performed for gynecological tumors. The incidence of appendiceal lesions in the 2 cohorts we studied was 13% and 7% respectively. This incidence of appendiceal lesions in both cohorts is above the figure of around 1% reported in the literature for appendectomies performed for appendicitis2–4 but similar to the incidence noted by Wong et al in their series of patients undergoing appendicectomy as part of cytoreductive surgery. 26 Our study hence provides a more accurate representation of the incidence of appendiceal neoplasms in patients presenting with gynecological neoplasms.
Cheng et al, in their metaanalysis, found that the malignant appendiceal pathology rate was only 1.4% in macroscopically normal appendix compared to 59% in the macroscopically abnormal appendix. 10 A report published from a U.K. center about outcome of appendicectomies in the setting of malignant mucinous ovarian neoplasms also found good correlation between detection of macroscopic abnormality and concordance with malignant microscopic lesions in 87.5% of the specimens. 27 However, in our study we found a poor correlation between gross appearance and detection of microscopic abnormality with 7% (12/170) of all the macroscopically normal appendices harboring an appendiceal pathology (Cohort 1) and detection of macroscopic abnormality reported in only 2 of the 12 appendices harboring appendiceal pathology (Cohort 2). There were also 3 appendices out of the 46 with macroscopic abnormality where no microscopic abnormality was seen on histological assessment (Cohort 2). The sensitivity of gross examination to determine appendiceal pathology was only 8% in Cohort 2, making it an unreliable method for disease detection. This, in part, could be explained by the small size of some of these lesions observed in our cohort.
According to the American Cancer Database, appendiceal cancer has increased over time, and the increase appears to be driven by a rise in carcinoids, most prevalent in patients 49 years of age or younger. 28 Bahmad et al have found in their institution, increased incidence of appendiceal neoplasms over a 10-year study period, which they attribute partly to better handling and thorough assessment of the appendix. 2 Hence, depending on gross examination to detect appendiceal lesions either intraoperatively or during specimen dissection is not a reliable method. This strengthens the argument of performing a primary appendicectomy as part of cytoreductive surgery and subsequent submission of the entire specimen in instances of no gross macroscopic abnormality.
Another important finding in our study of Cohort 1 was the appendix, being the most frequent site of origin of extraovarian metastasis to the ovary (56%), despite the rate of appendectomies being poor (47%). This is higher in comparison with rates of 7.3% found in a nationwide study in the Netherlands. 29 In fact, Moore et al noted the highest frequency of appendix as a primary site of metastasis, cited in literature, to be 20%. 30
The findings of normal looking appendices harboring malignant appendiceal pathology, the appendix being one of the most frequent sites of extra ovarian metastasis and inability to reliably delineate a tumor deposit from primary appendiceal lesion in cytoreductive surgeries are strong arguments in support of appendicectomy that are demonstrated by the results of our study. Moore et al also found a comparable incidence of 6% of significant appendiceal pathology in normal looking appendices, favoring routine removal of appendix at the time of primary surgery for all mucinous ovarian neoplasms. 11 This policy was also encouraged by Lavecchia et al who concluded in their study that a benign or borderline frozen section of an ovarian mucinous neoplasm and normal appearing appendix have limited predictive value for appendiceal pathology. Hence, they recommended appendicectomy with removal of the mesoappendix in all patients with mucinous ovarian neoplasms, regardless of intraoperative findings. 31
Studies advocating against removal of appendix extrapolate information based on normal microscopic findings in grossly normal appendices intraoperatively, but they fail to recognize the positive predictive value of gross inspection being only 56%. 15 Moreover, studies arguing for and against appendicectomy are limited by the small number of patients, limited cohort population13,30 and missing data 32 and hence conclusions drawn from such databases are not reliable.
It is also worth noting that many studies when they advise against removal of normal appendix, are also referring to absence of metastasis and pseudomyxoma peritonei, as presence of either of these in their studies mandate appendicectomy irrespective of the appearance of the appendix.14,33
The historic notion that the presence of an appendiceal primary in mucinous ovarian neoplasms did not lead to change in final stage, 14 as there was metastatic disease elsewhere, 34 has not withstood the test of time. Our growing understanding of appendiceal lesions together with emerging evidence-based management of appendiceal neoplasms,7,8 mandate concomitant if not separate management of these neoplasms with gynecological malignancies.
Appendicectomy is sometimes performed in patients undergoing major abdominal operations for trauma to prevent subsequent development of appendicitis. These patients are at high risk of developing dense adhesions, increasing the risk of future operations. Therefore, there is a potential benefit of appendicectomy for such patients. 35 The same concept can be applied to laparotomy for gynecological malignancies. Many studies recognized that there is no statistically increased risk of complications with this additional procedure as part of the gynecological surgery.14,30
However, infection is reported to be the main complication in appendicectomy during laparotomy. 35 More recently, Bernard et al, reported that appendicectomy at the time of surgery for suspected early-stage ovarian cancer was associated with significantly elevated odds of postoperative infection. However, this increased risk of infection was not associated with an increase in the length of hospital stay, readmission, return to the operating room, or postoperative death. 36
Moreover, appendicectomy of a grossly normal appendix was not an independent prognostic factor for overall survival and progression-free survival in patients with mucinous ovarian carcinomas. 37
Our study with a total cohort size of 581 patients is the largest of its kind looking at the incidence and type of appendiceal lesions encountered not just in the setting of mucinous lesions of the ovary but in all patients undergoing cytoreductive surgery for different types of gynecological malignancy. The study highlights a high incidence of primary appendiceal tumors in both cohorts.
There are very limited studies in the literature which segregate between colon and appendix as 2 separate sites of extraovarian metastasis and hence our study helps to hone in on this important distinction for future studies and subsequent management.
We have used the updated 2019 WHO nomenclature for classification of the appendiceal lesions 7 ensuring the findings of this study are relevant and have clinical utility and will serve as a benchmark for future trials and studies.
We have looked at the correlation between macroscopic abnormality and microscopic confirmation of appendiceal lesions and compared this with previous reports. We found appendiceal lesions even in normal looking appendix, particularly in the age group of over 45. We, therefore, propose that appendicectomy should be performed as part of cytoreductive surgery in these women, especially as it does not increase morbidity.14,20,21,30,34 It also provides an opportunity for better and holistic management of patients with concomitant appendiceal and gynecological malignancy.
Moreover, if an appendix is submitted for histological assessment, it should be examined very carefully macroscopically and embedded in its entirety if no macroscopic lesion is identified due to the small nature and size of some of the appendiceal lesions.
Our study highlights the importance of appendicectomy during surgery for ovarian mucinous neoplasms and as part of cytoreductive surgery for gynecological malignancies. It also signifies the importance of microscopic examination of the whole appendix, especially when no gross abnormality is detected.
Footnotes
Data Availability Statement
All data related to the study is included in the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
Ethics approval was obtained from the Institutional Review Board of the Tissue Bank of Imperial College Healthcare NHS Trust.
Funding
Professor El-Bahrawy is supported by the NIHR Imperial Biomedical Research Centre Funding Scheme.
Trial Registration
Not applicable, because this article does not contain any studies with human or animal subjects.