
Abstract
Extramedullary hematopoiesis is the physiological process of hematopoiesis occurring outside of the bone marrow and is an extremely rare occurrence in the prostate, with only 1 previously documented report in the English literature. We present a specimen from a 56-year-old man who was found to have a palpable nodule on digital rectal examination and visible findings on ultrasound, confirmed to be extramedullary hematopoiesis on the prostate core.
Introduction
Extramedullary hematopoiesis is the physiological process of hematopoiesis occurring outside of the bone marrow. In pathological states with bone marrow infiltration, extramedullary hematopoiesis occurs as a compensatory mechanism to correct ineffective erythropoiesis. Common causes include myelofibrosis, sickle cell disease, thalassemia, and other hematological disorders such as leukemia and lymphoma. 1 Given the role the spleen and liver play in fetal hematopoiesis, they are also the most common sites of extramedullary hematopoiesis that occur due to reactivation of these fetal hematopoietic centers.2,3 Other common sites include the lymph nodes, while more rare sites include but are not limited to the paraspinal, presacral, retroperitoneal, mediastinal, nasopharyngeal, and para-nasal regions, as well as other organs such as the lung, heart, kidneys, adrenal tissues, skin, breast, and thyroid glands.2,4,5
Here, we report an occurrence of extramedullary hematopoiesis in the prostate. A patient with no significant medical history was found to have a prostatic calcification on ultrasound which was diagnosed as extramedullary hematopoiesis post biopsy. To our knowledge, there has only been 1 other report of prostatic extramedullary hematopoiesis to date, highlighting the rarity of this unique pathological condition. 6
Patient History
During a routine physical examination of a 56-year-old man with no history of hematologic malignancy but factor V deficiency carrier status, a prostatic nodule was identified on digital rectal examination in the left lobe extending to the apex. Prostate-specific antigen was low (0.4 ng/mL), but due to irregular morphology on palpation, further investigations were ordered. On ultrasound, the prostate volume was 31 cc, the peripheral zone was unremarkable, and the transition zone was enlarged, in keeping with benign prostatic hyperplasia. There was also a 0.6 cm calcification within the left transition zone at the mid gland, felt to represent the palpable nodule. A 12-core systematic biopsy was performed, which demonstrated all benign cores. However, in the left apex, there was extramedullary hematopoiesis (Figure 1) within the core associated with osseous metaplasia, including trilineage hematopoiesis. Staining for CD61 confirmed the presence of megakaryocytes (Figures 2 and 3). The presence of benign prostate tissue on either side of the lesion (not shown, but seen at low power) supports the process being within rather than adjacent to the prostate. Being within the prostate makes the possibility of a floater or contamination unlikely.
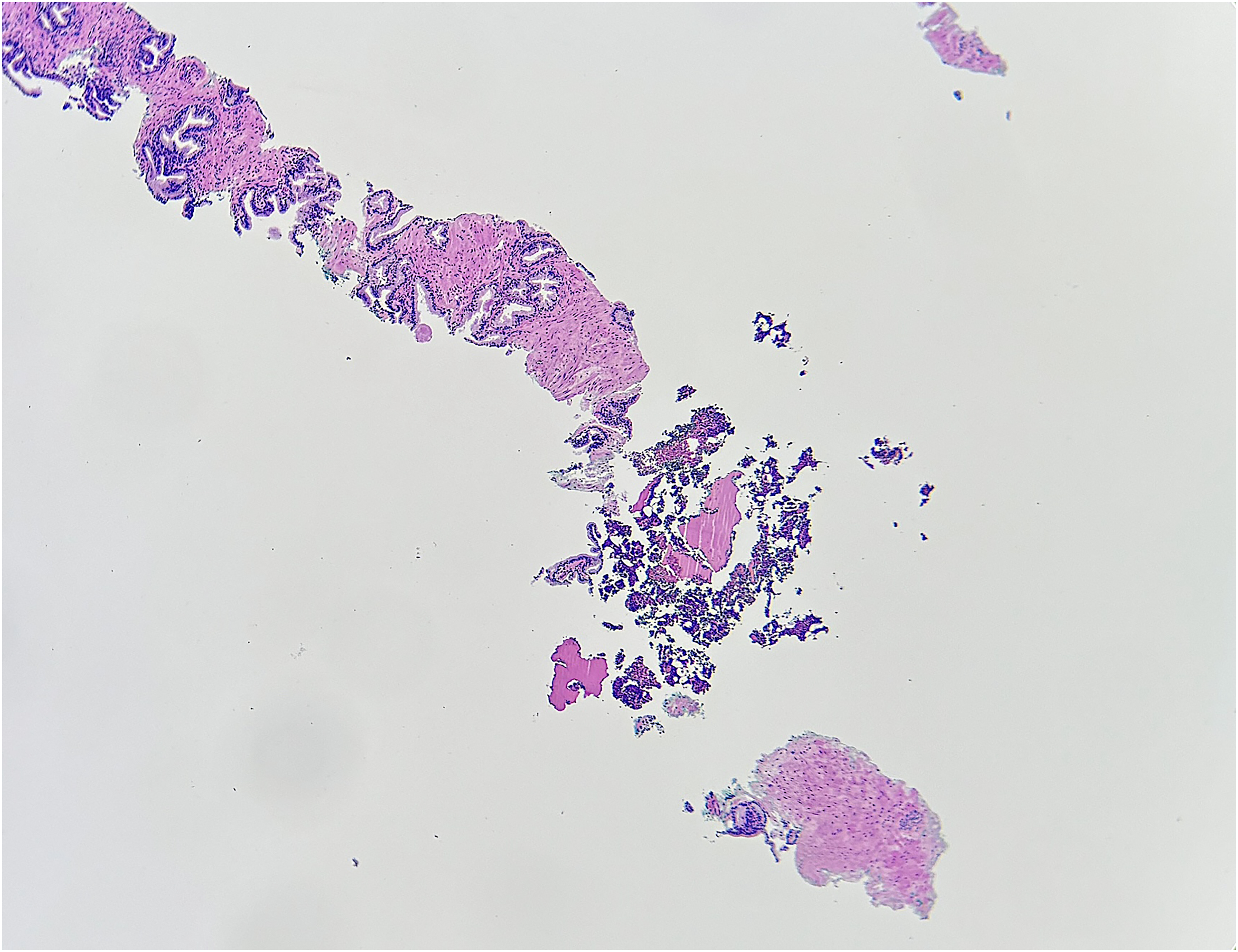
Low power (40×) magnification showing the focus of extramedullary hematopoiesis within the benign prostate core.
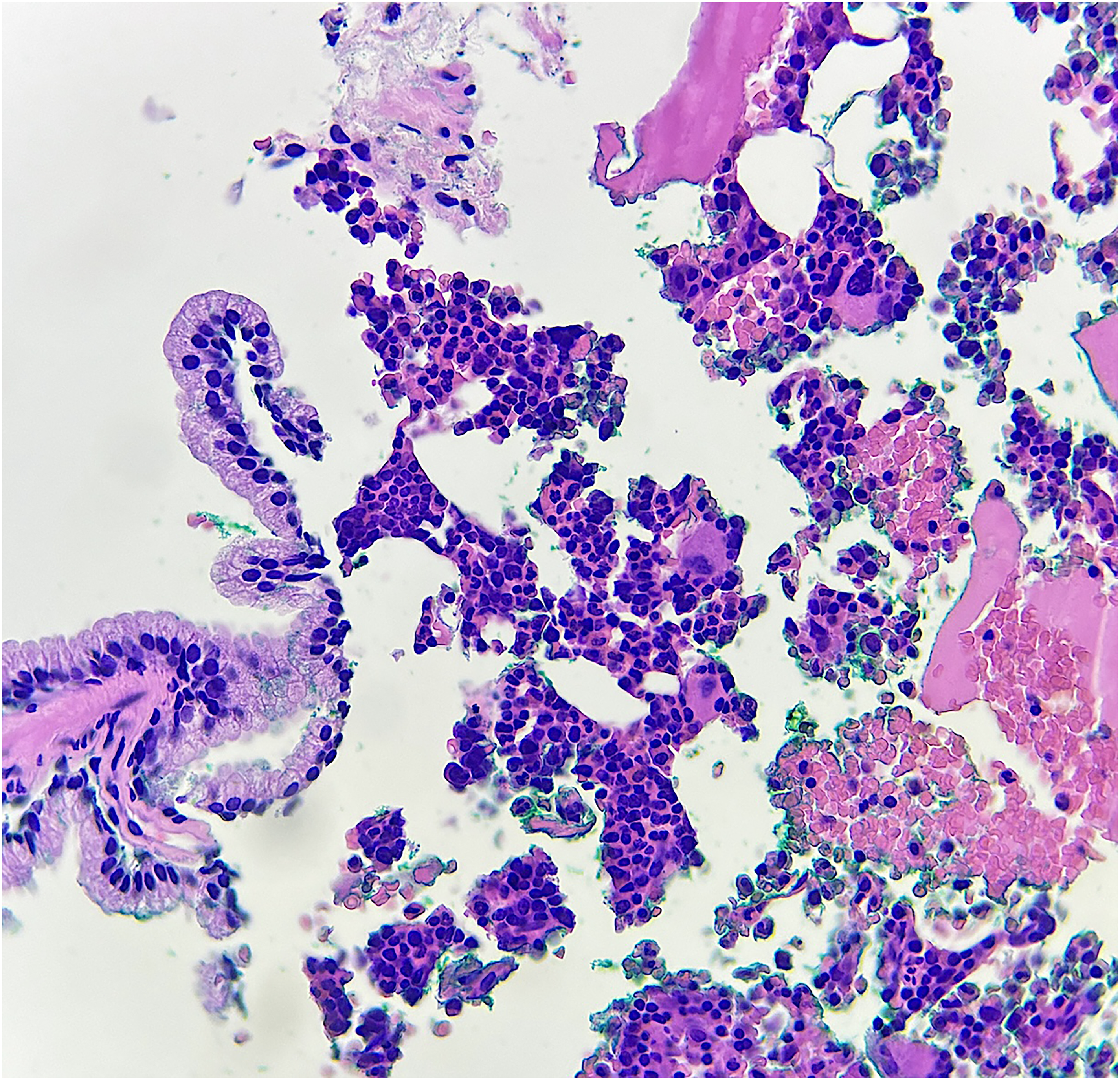
High power (400×) magnification showing hematopoietic elements, including megakaryocytes.
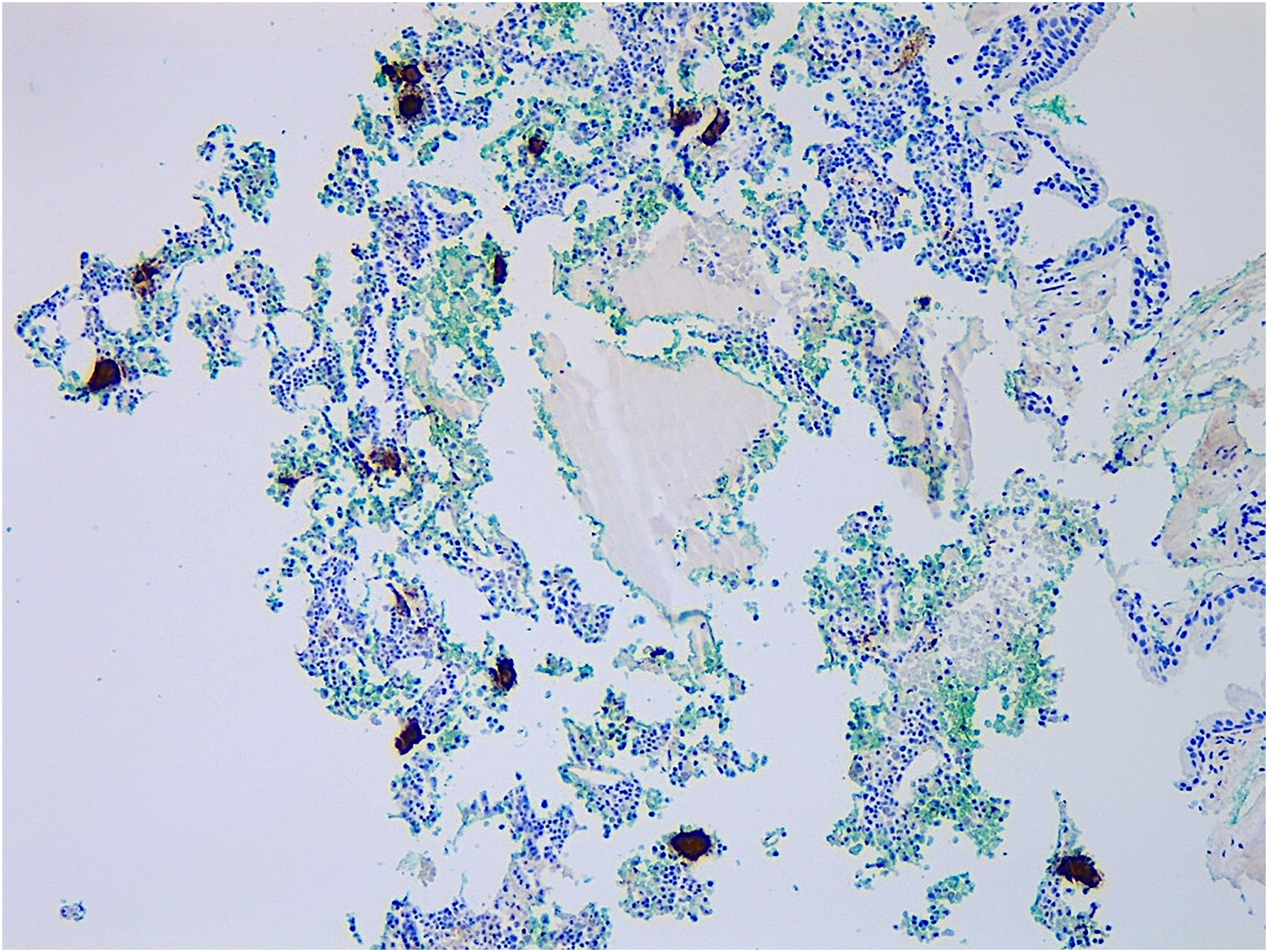
Positive CD61 staining of megakaryocytes.
Discussion
This is the second report of extramedullary hematopoiesis in the prostate. 6 However, there are differences between this patient and the first. For one, in Humphry and Vollmer's (1991) specimen, the patient had a known 8-year history of myelofibrosis. The patient initially presented with hepatosplenomegaly and complete blood count abnormalities suggestive of myelofibrosis. Over the years, he developed worsening asymptomatic anemia. Later in his disease course, the patient acquired obstructive urinary symptoms leading to an eventual transurethral resection of the prostate which demonstrated extramedullary hematopoiesis. The authors of this report stated that the patient's hepatosplenomegaly suggested extramedullary hematopoiesis was also likely present in these sites. Conversely, in our patient, there was no history of hematological, or any other, malignancy.
Although it cannot be stated with 100% certainty that the nodule on ultrasound and palpation corresponds to the area of bone formation and extramedullary hematopoiesis, we feel this is the most likely scenario since the digital rectal exam described the lesion in the left lobe extending toward the apex, which is the same location the specimen was targeting. In addition, the ultrasound report concluded that the calcification identified was felt to represent the palpable nodule. In addition, the presence of benign prostate tissue on either side of the lesion (not shown but seen at low power) supports the process being within rather than adjacent to the prostate. Being within the prostate makes the possibility of a floater or contamination unlikely.
In a Mayo Clinic case series examining 309 examples of extramedullary hematopoiesis in the absence of myeloproliferative neoplasms, 4% (12) of the examples were found to have no attributable cause and therefore were termed idiopathic in nature. 4 Most of these patients presented with nonspecific symptoms or as an incidental discovery. Additionally, the median follow-up for the 12 patients was 7 years, and none of these patients were ever found to harbor occult malignancies nor went on to develop myeloproliferative neoplasms or myeloid malignancies. Idiopathic extramedullary hematopoiesis is therefore an uncommon diagnosis that is often found incidentally which was the circumstance for our patient.
Although exceedingly rare in the prostate, extramedullary hematopoiesis does occur more commonly in other genitourinary organs. There are numerous documented examples of extramedullary hematopoiesis in the kidney,7–14 with some studies demonstrating renal extramedullary hematopoiesis rates almost as high as lymph nodes and liver extramedullary hematopoiesis rates. 15 More rarely it can present in the bladder16–18 and ureters.18,19
Extramedullary hematopoiesis is an uncommon, benign, compensatory mechanism for ineffectual erythropoiesis. In this report, we illustrate a rare form that is extramedullary hematopoiesis in the prostate, the second recorded specimen of prostatic extramedullary hematopoiesis to date.
Footnotes
Author Contributions
Lucas A.B. Fisher contributed to writing of original draft and editing. Nicholas Baniak contributed to writing, editing, clinical work, and project administration.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Case report and review are exempted from formal ethics as per our institutional review policies.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable, because this article does not contain any studies
with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical
trials.