
Abstract
Hibernoma is a relatively uncommon benign neoplasm of brown adipose tissue which usually affects head and neck region, thigh and rarely breast. There are different subtypes of hibernoma with the spindle cell-type is the least common one. Herein, we are reporting a case of this rare spindle cell hibernoma in a location which has not been previously reported: perinephric adipose tissue. This tumor was presented as a renal mass on imaging.
Keywords
Introduction
Hibernoma is an uncommon benign neoplasm of brown adipose tissue. The most common sites of hibernoma include head and neck region and thigh. Few reports have shown this neoplasm in unusual sites such as breast tissue and intrabdominal cavity. So far, there are no published reports of a hibernoma arising in the perinephric adipose tissue and presenting as a renal neoplasm. In this case report, we are sharing a subtype of hibernoma—spindle cell hibernoma arising in a very unusual location—perinephric adipose tissue. This case report is unique regarding the location of this uncommon tumor.
Case
A 74-year-old man with medical comorbidities (hypertension, hyperlipidemia, and tubular adenomas of the colon) came for an annual physical checkup. He denied fever, abdominal pain, altered bowel habits, dysuria, hematuria, or unintentional weight loss. A routine urine examination revealed microhematuria. Subsequent computed tomography (CT) of the abdomen found a homogeneously enhancing exophytic right inferior pole nodule (2.2 × 2.0 × 2.1 cm). No lymphadenopathy or other lesions were noted. The patient worked in a hardware store and was an ex-smoker (15 pack-years, quit 10 years ago). No family history of renal carcinoma was present. A repeat CT (Figure 1) of the abdomen performed 6 months later showed a minimal increase in the size of the renal nodule (2.4 × 2.1 × 2.1 cm) without lymphadenopathy or any other lesions. The patient denied abdominal pain or gross hematuria and did not report any new complaints. The increase in the size of the nodule became clinically concerning for a neoplastic process. With the patient's consent, a robot-assisted laparoscopic partial right nephrectomy was planned and performed (Figure 1).
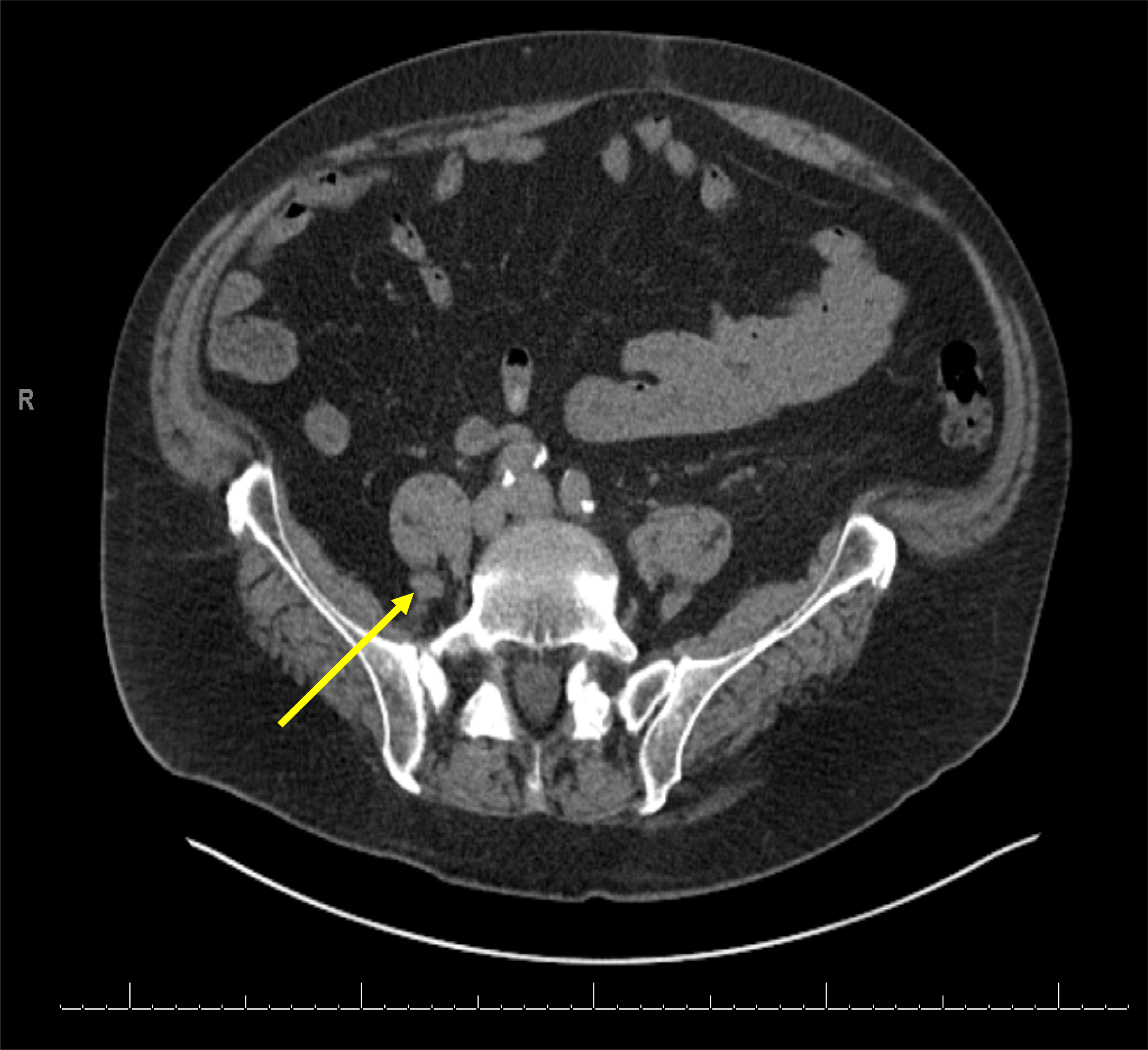
Computed tomography (CT) of the abdomen. CT image of the abdomen shows a homogeneously enhancing exophytic right inferior pole renal nodule (highlighted by a yellow arrow).
The specimen was received as a tan-gray-yellow fragment of tissue with a shiny, membranous surface (Gerota's fascia). The tissue measured 4.8 × 3.9 × 3.6 cm. Sectioning of the tissue revealed an ill-defined firm gray tumor (2.4 × 2.0 × 1.0 cm) at the right lower pole of the kidney, which was extending to the perinephric fat. Sectioning of the specimen revealed grossly unremarkable renal parenchyma with the tan-gray cut surfaces of the tumor mostly confined to the perinephric fat with no involvement of the renal parenchyma.
By histology, the tumor is composed of a mixture of three different elements: bland spindle cells with wiry collagen, myxoid stroma, and polygonal, multivacuolated cells containing eosinophilic foamy cytoplasm and small nuclei with rare nucleoli (Figure 2). The polygonal multivacuolated cells have an increased capillary network around them. Chronic inflammatory cells are present within the tumor. The presence of polygonal multivacuolated cells with foamy cytoplasm is most suggestive of a brown fat tumor- hibernoma. In the background of spindle cells with wiry collagen and myxoid stroma, this finding is suggestive of a spindle cell hibernoma. The other differential for this microscopic finding includes spindle cell lipoma and rarely low-grade fibromyxoid sarcoma. Our case does not fit well with either of these differential diagnoses primarily due to the presence of a hibernomatous component as well as the absence of curvilinear branching vessels in the myxoid area, which is a hallmark feature for low-grade fibromyxoid sarcoma. To further confirm our preliminary diagnosis, we sent the case for an expert consultation at The Joint Pathology Center (Silver Spring, MD, USA). MDM2 FISH study was performed and was reported as negative. Their expert consultant agreed with our preliminary diagnosis of hibernoma with areas of spindle cells and myxoid stroma, consistent with spindle cell hibernoma. Thus, this is an example of spindle cell hibernoma involving perinephric adipose tissue.
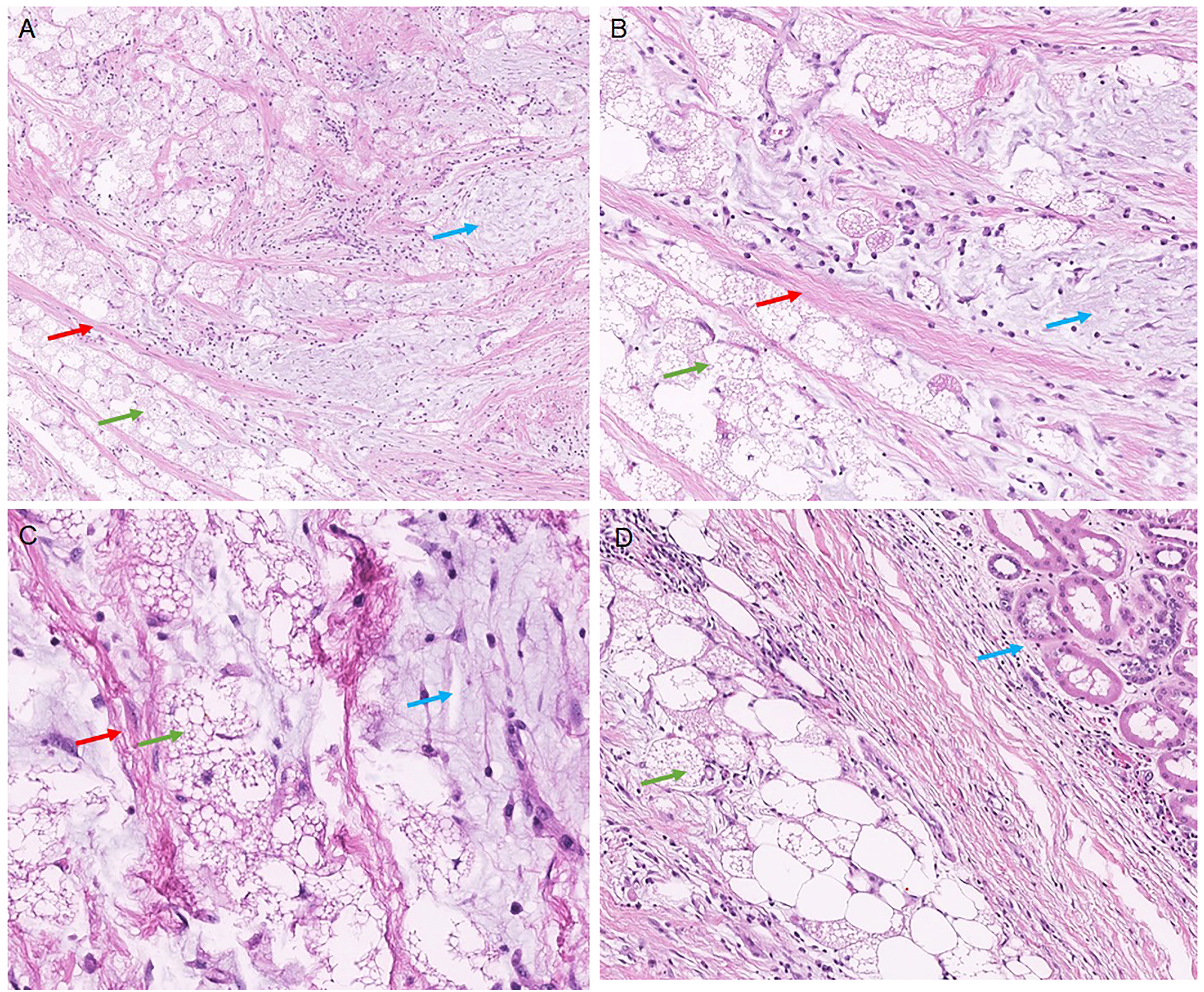
Histology of spindle cell hibernoma. (A-C) Histology of perinephric tumor showing three components of spindle cell hibernoma-polygonal cells with eosinophilic granular cytoplasm (green arrow), myxoid stroma (blue arrow), and ropy/wiry collagen (red arrow) (A: 20×; B: 100×; C: 200×). (D) Hibernoma (green arrow) is separated from the adjacent normal renal parenchyma (blue arrow, 100×).
The patient is doing well without any signs of metastasis or tumor recurrence in a 12-month follow-up.
Review of Literature and Discussion
Hibernoma is a relatively uncommon benign neoplasm of brown adipose tissue and presents as a slow-growing, painless mass, usually at 30–40 years of age. Most neoplasms are found incidentally during imaging. The most common sites for hibernomas are the soft tissues of the thigh, shoulder, back, neck, chest, arm, and abdominal cavity, which can represent areas of brown adipose tissue remnants in adult life. 1 Rare case reports of hibernoma affecting mammary gland tissue have been reported. The malignant variant of hibernoma is very rare. 3–6 The prognosis of hibernoma, irrespective of the site, is excellent.
There are four subtypes of hibernoma reported in the literature: typical, lipoma-like, spindle, and myxoid. The histologic features of typical hibernoma include polygonal cells with granular eosinophilic cytoplasm and multivacuolated adipocytes. The lipoma-like hibernoma has an abundance of univacuolated adipocytes and sparse polygonal cells with eosinophilic granular cytoplasm resembling lipoma. This type commonly affects the thighs. The spindle hibernoma is a very rare entity with a male predilection and is usually found in the posterior neck, scalp, and groin. The spindle cell component is usually CD34 positive. It comprises polygonal cells with eosinophilic granular cytoplasm, thick collagen bundles, and mast cells. The myxoid variant is more common in males and usually affects the head and neck region. It is comprised of polygonal cells with eosinophilic granular cytoplasm, and cells are separated by acellular myxoid stroma. Among these histologic variants, spindle cell hibernoma is considered the rarest one, ∼2% of all hibernomas. 4 Mitosis and cellular atypia are extremely rare in hibernomas. The diagnosis of hibernoma is chiefly based on the classical histologic appearance of hematoxylin and eosin-stained tissue as described above. Hibernomas other than the classical type may include a differential diagnosis of lipoblastoma, atypical lipomatous tumor (ALT), granular cell tumor, and myxoid liposarcoma. Immunostains and molecular studies are performed to rule out these differential diagnoses [PLAG gene rearrangement for lipoblastoma; MDM2 amplification for atypical lipomatous tumor; diffuse S100 positive cells in granular cell tumor in absence of multivacuolated cells; t(12:16) or t(12:22) for myxoid liposarcoma].
To date, the largest registry for hibernoma 1 reported 10 examples of hibernoma in the abdominal cavity/retroperitoneum out of 170 in that study. The study has not mentioned the exact location of this tumor in the abdominal cavity or retroperitoneum. Moreover, spindle cell hibernoma has been shown to be more common in the head and neck region, and thigh. In our case, the perinephric tumor was thought to be a renal cell neoplasm based on imaging findings. On histologic examination, it is most consistent with a spindle cell hibernoma. This case demonstrates that spindle cell hibernoma can represent as a retroperitoneal renal mass. Thus, pathologists should keep hibernoma in their differential when dealing with a perirenal adipocytic mass.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
No patient related information is used in this article. Neither was the patient's management changed. This is a retrospective observation.
Trial Registration
This is not a clinical trial.