
Abstract
A 50-year-old man presented for evaluation of a periscapular mass. Biopsy suggested a low-grade chondrosarcoma; however, the resected specimen revealed a grade 2 chondrosarcoma with a low-grade dedifferentiated mesenchymal component. The mass multiply recurred as chondrosarcoma without a dedifferentiated component before the patient developed lung metastases of chondrosarcoma without a dedifferentiated component 11 years after the initial diagnosis and died of disease. This is one of the first reported cases of a dedifferentiated chondrosarcoma with low-grade dedifferentiated component. While overall prognosis may be better than in typical dedifferentiated chondrosarcoma, this tumor demonstrated numerous local recurrences as well as metastasis.
Keywords
Introduction
Chondrosarcomas are rare, cartilage-forming bone tumors with an estimated overall incidence of 1 in 200 000 cases yearly and are considered the third most common malignancy of bone behind multiple myeloma and osteosarcoma. 1 While a majority of chondrosarcomas originate from the medullary cavity of the appendicular skeleton, a small percentage of chondrosarcoma subtypes originate from soft tissue, including extraskeletal myxoid chondrosarcoma. 2 The most common presenting symptom is usually pain with or without localized swelling, and few cases will present with pathological fracture. Initial diagnosis typically relies on radiographic imaging and lesions most often appear in the metaphysis and diaphysis of long bones. Radiographic description includes calcifications that may be punctate, flocculent, or contain circumferential patterning. 3 Survival rates vary among histological subtypes as well as tumor grade. However, several studies suggest a 5-year survival rate north of 70% for conventional chondrosarcoma.2,4
Conversely, dedifferentiated chondrosarcomas are a subtype of chondrosarcoma with a far worse prognosis. Histopathological description of dedifferentiated chondrosarcomas mainly describes a well-circumscribed low-grade chondrosarcoma juxtaposed to a high-grade dedifferentiated spindle-cell sarcoma. 5 Comprising an estimated 10% of chondrosarcomas, dedifferentiated chondrosarcomas are extremely rare and offer a particularly poor prognosis. Rates of local recurrence have been reported up to 35%. 6 With a median survival of 5 to 16 months and a 5-year survival of 7%, early diagnosis and treatment are pivotal.7–12
Dedifferentiated chondrosarcomas present similarly to chondrosarcoma and other bony malignancies in anatomic location and presentation.7,10,13,14 Radiographic imaging depicts lesions with intraosseous chondroid matrix mineralization and cortical destruction with possible bimorphic features. 15 Addition of magnetic resonance imaging (MRI) and computed tomography (CT) can aid the diagnosis with the presence of soft tissue mass and evidence of chondroid matrix and cortical destruction.
Once the diagnosis is confirmed, surgical resection is imperative. En bloc resection with negative margins has been shown to decrease local recurrence and metastatic potential. 16 The benefit of adjuvant therapy with respect to chemotherapy and radiation remains debated among clinicians in its efficacy for use in dedifferentiated chondrosarcomas; however, a majority of centers will offer chemotherapy if the patient is able to tolerate the treatment.10,16,17
Following extensive literature review, we present what we believe to be an exceedingly rare case of a soft tissue dedifferentiated chondrosarcoma of the periscapular region remarkable for its low-grade dedifferentiated mesenchymal component and 11-year metastatic relapse. The patient was informed the data concerning the case would be submitted, and he provided consent.
Case Report
A 50-year-old male presented with a mass involving the posterior shoulder superior to the clavicle. At the time of referral to our orthopedic oncology practice, outside radiographs, MRI, and CT had revealed a heterogenous soft tissue lesion on the surface of the dorsal scapula. A needle biopsy was consistent with a low-grade chondrosarcoma. Several weeks later, the patient underwent en bloc resection. The final pathology revealed negative margins and was consistent with an 8.6 cm well-circumscribed grade 2 chondrosarcoma with 1 block containing a zone of skeletal muscle with 7 microscopic nodules of tumor with a low-grade dedifferentiated mesenchymal component spanning 1.3 cm (Figures 1-5). No adjuvant radiation or chemotherapy was administered following resection.
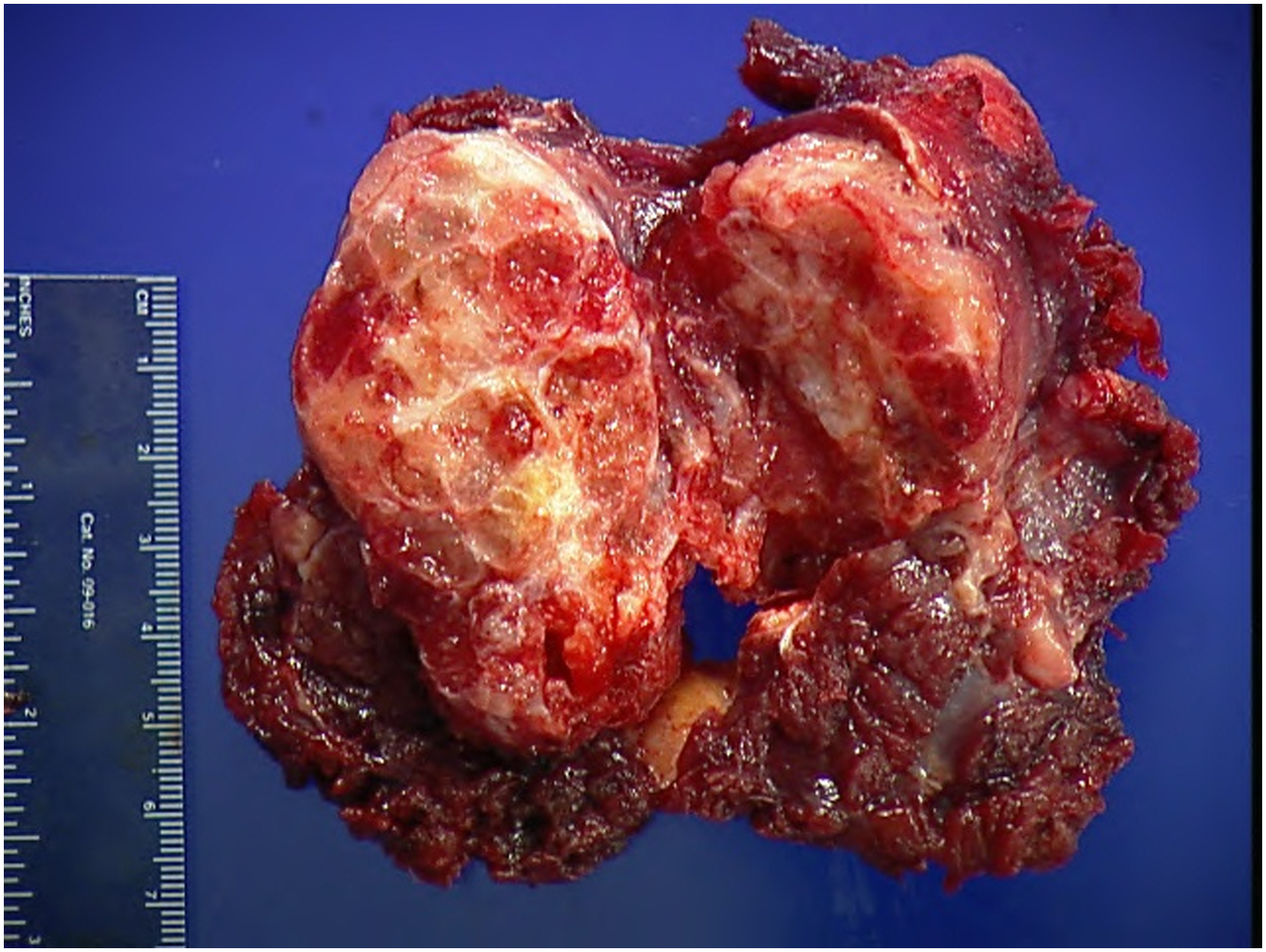
Gross photograph of resected chondrosarcoma with myxoid appearance surrounded by skeletal muscle.
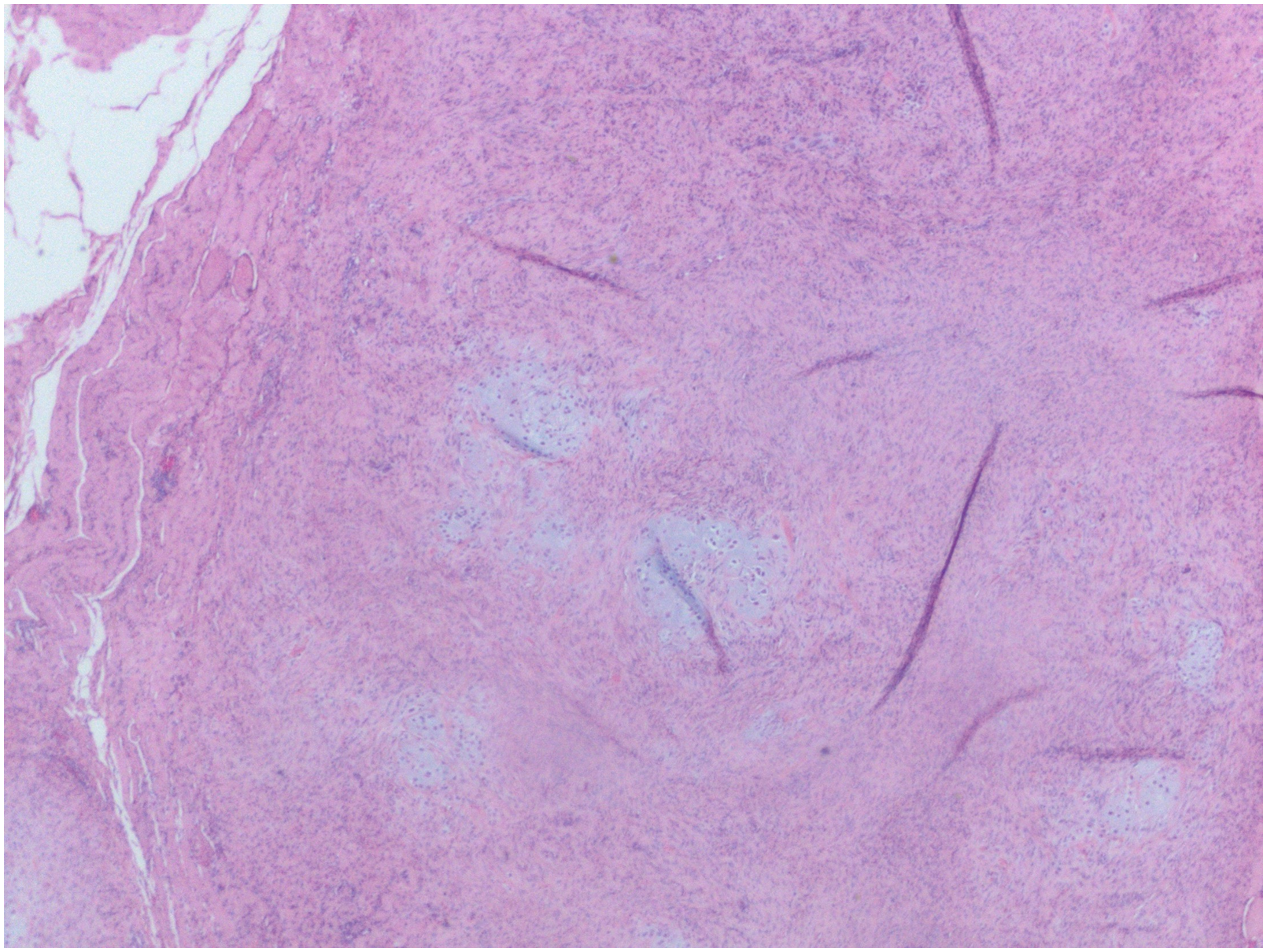
Photomicrograph at 20 × magnification demonstrating a proliferation of bland spindle cells with fibroblastic morphology forming fascicles in storiform pattern in largest microscopic tumor nodule.
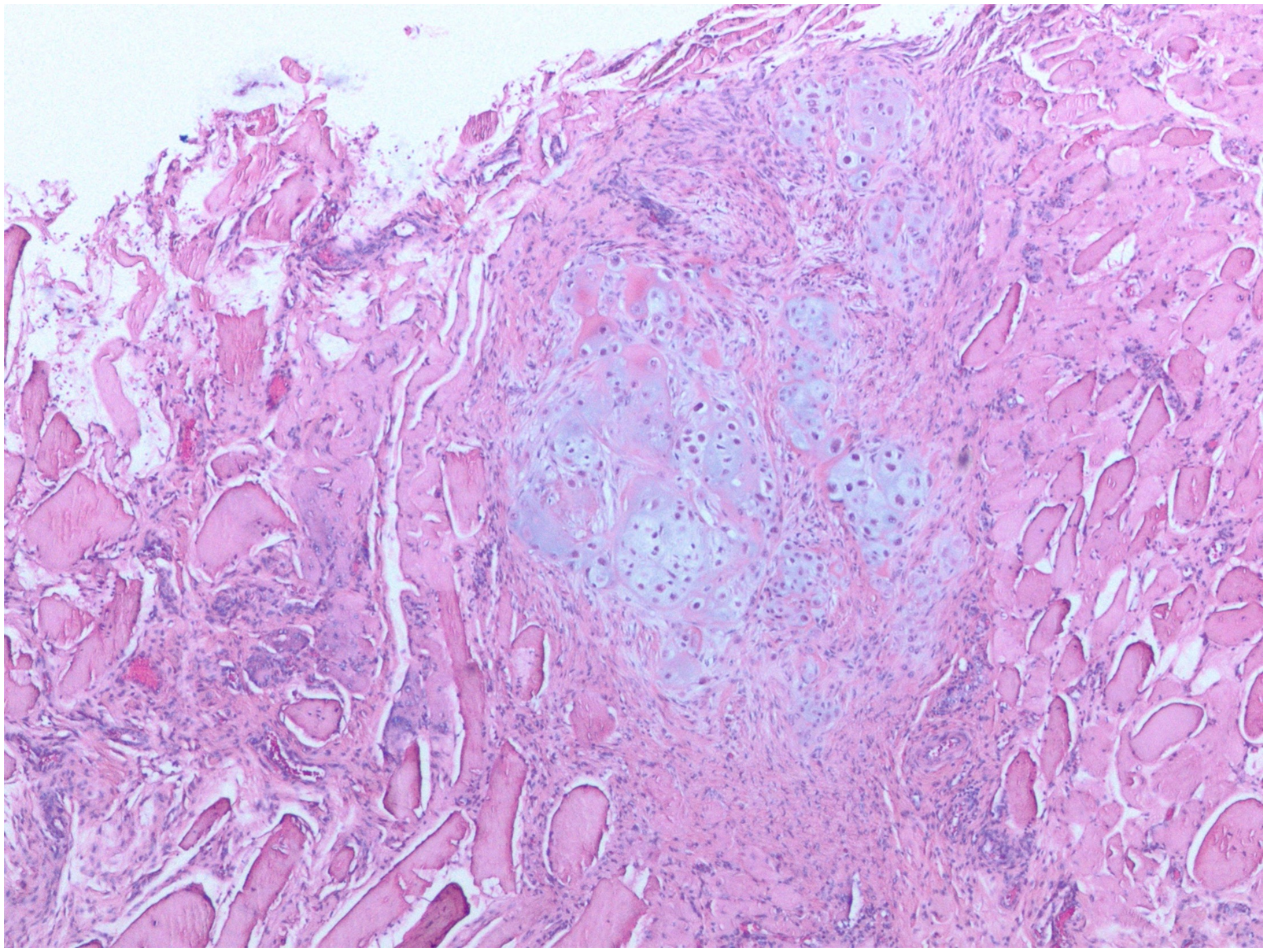
Photomicrograph at 40 × magnification demonstrating microscopic tumor nodule surrounded by skeletal muscle.
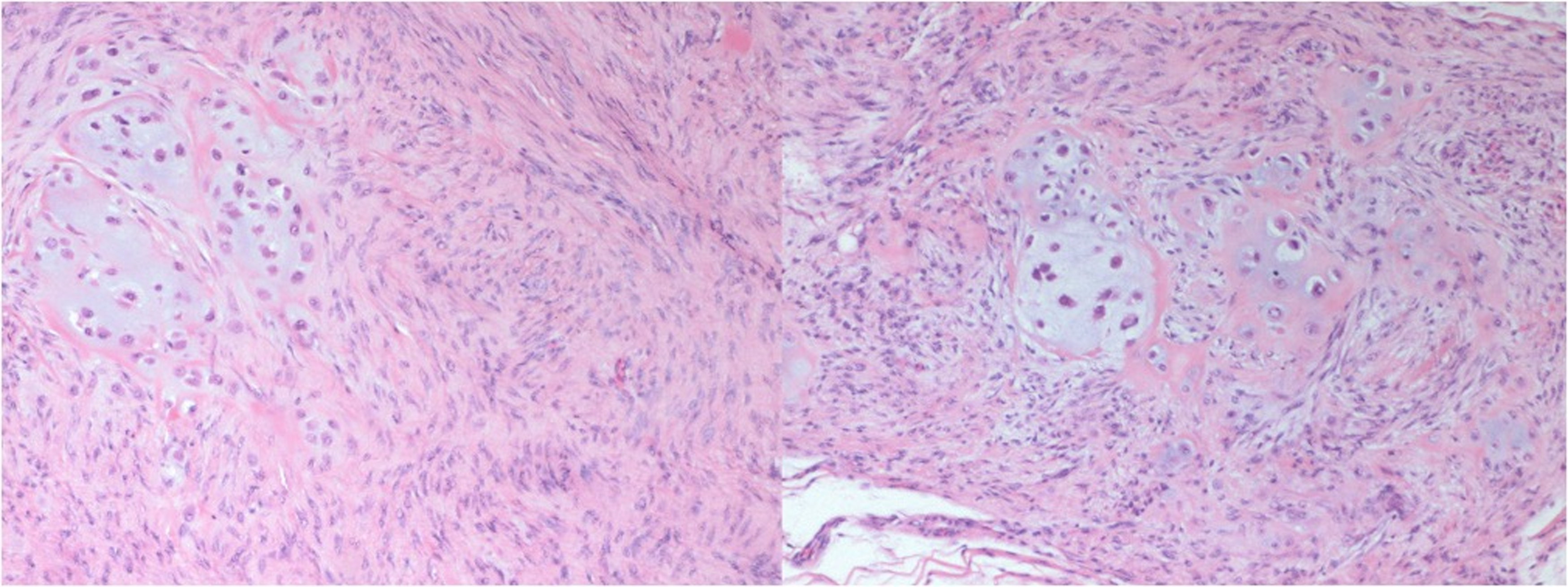
Photomicrograph at 100 × magnification demonstrating clusters of chondrocytes with mild atypia with occasional cells showing transitional morphology.
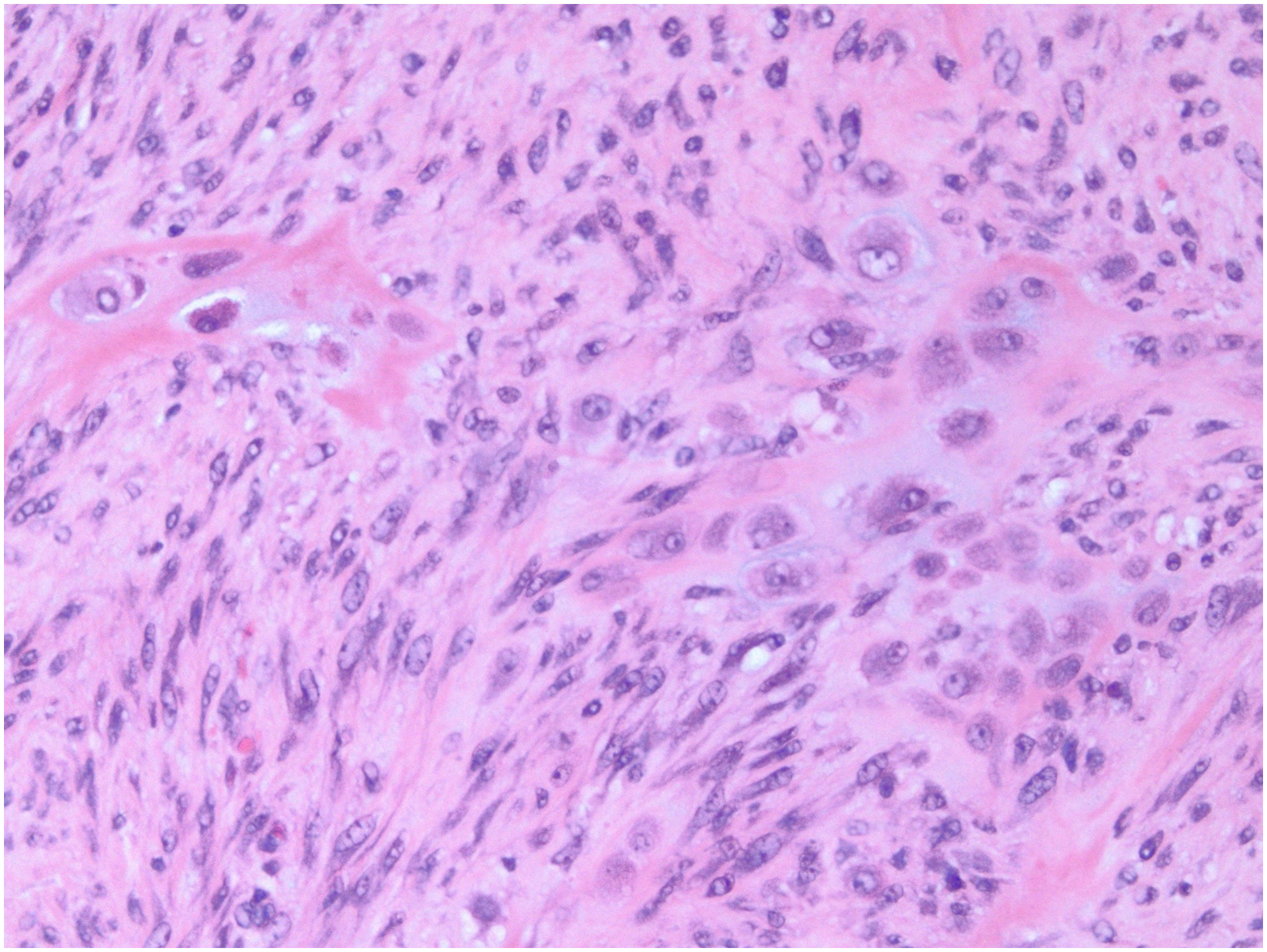
Photomicrograph at 200 × magnification demonstrating clusters of chondrocytes with mild atypia with arrows demarking transitional morphology.
Seven and a half months later, surveillance imaging was suggestive of local recurrence (Figure 3). The mass was resected with negative margins and histologically confirmed as recurrent grade 2 chondrosarcoma, though no dedifferentiated component was seen at this time. A third recurrence (Figure 6) was later treated at an outside institution and a fourth was treated with partial scapulectomy 60 months after the index procedure. Postoperatively, proton beam therapy was administered at an outside institution as the surgical margins were in question. Of note, no dedifferentiated component was seen following the partial scapulectomy.
A fifth recurrence was complicated with involvement of the chest wall and neurovascular structures in the axilla 3 years after partial scapulectomy. The patient was staged and confirmed to have localized disease. Limb-salvage was not an option due to the neurovascular involvement of the tumor and consequently, a forequarter amputation and chest wall resection involving rib hemicortex and neuroplasty of the brachial plexus were performed. Final pathology described a 16 cm recurrent grade 2 chondrosarcoma with negative margins, again with no evidence of dedifferentiated component.
Nine months after the forequarter amputation, biopsies from the superior scapular region, lateral thoracic wall, and interior lateral thoracic wall proved recurrent grade 2 chondrosarcoma. Still with localized disease, the sixth recurrence was treated with radical resection of the chest wall and placement of brachytherapy catheters. Negative margins were achieved again; however, lymphovascular invasion was noted on the final pathology report.
A seventh recurrence was treated 30 months later with radical resection of the medial chest wall and right shoulder. Pulmonary metastatic disease was revealed on imaging studies 2 months following this resection (Figure 7) and resected pulmonary nodules were consistent with metastatic grade 2 chondrosarcoma with lymphovascular invasion. The patient was started on pazopanib which he did not tolerate and then started on pembrolizumab. Ultimately, the patient died of disease 8 months after initiation of chemotherapy and 11 years after his initial diagnosis.
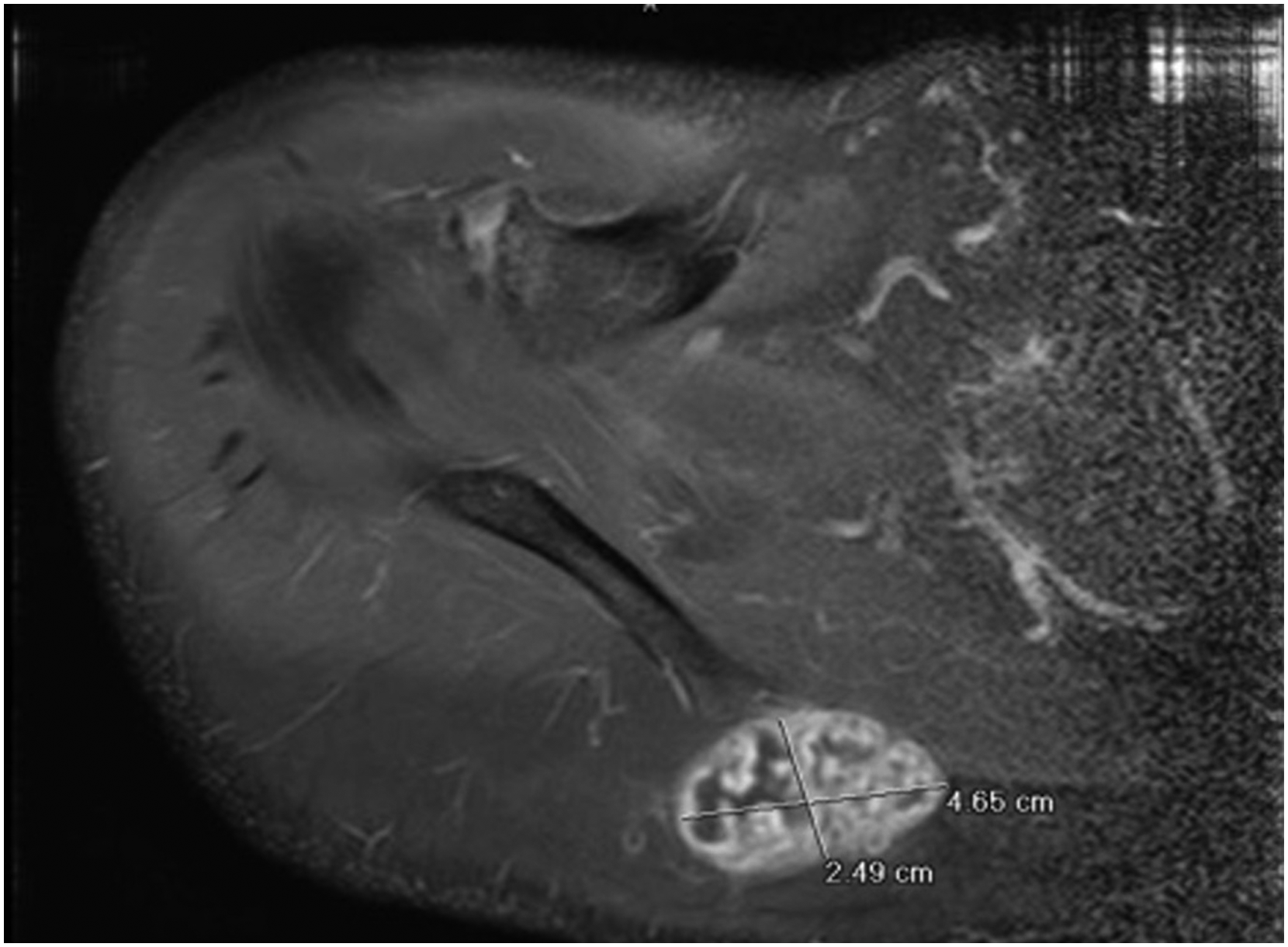
Axial MRI demonstrating a multilobulated, multicystic soft tissue mass along the scapular spine representative of recurrent soft tissue periosteal chondrosarcoma. Abbreviation: MRI, magnetic resonance imaging.
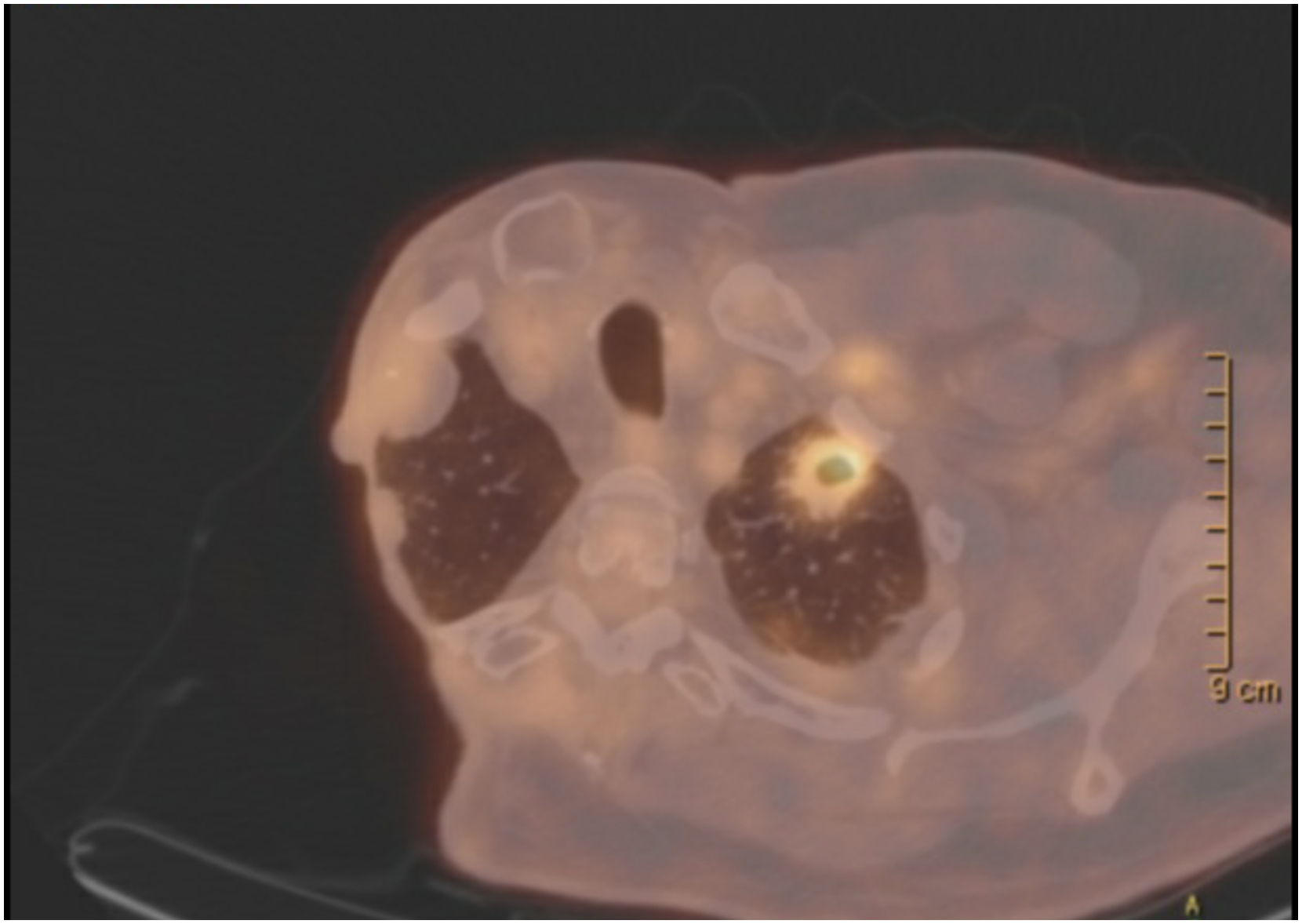
Axial PET-CT demonstrating FDG avid left anterior apical cavitary lesion measuring 2.3 × 2.0 cm, SUV max measuring 5.1. Abbreviations: FDG, Fluorodeoxyglucose; PET-CT, positron emission tomography-computed tomography; SUV, standardized uptake value.
Discussion
Dedifferentiated chondrosarcomas are described as well-circumscribed low-grade chondrosarcoma adjacent to a dedifferentiated high-grade sarcoma. 5 Histological composition of the high-grade component can be variable and has been documented as osteosarcoma, fibrosarcoma, histiocytoma, angiosarcoma, rhabdomyosarcoma, and spindle-cell sarcoma. Irrespective of the histology of the high-grade component, dedifferentiated chondrosarcomas are rare malignancies that grow rapidly, often metastasize, and have a dismal prognosis. 12 In the case presented, a 50-year old male presented with a grade 2 chondrosarcoma adjacent to a noncartilaginous mesenchymal component demonstrating low-grade dedifferentiation, suggestive of a dedifferentiated chondrosarcoma with a low-grade dedifferentiated component. This particular tumor has very rarely been described in the literature as dedifferentiated chondrosarcomas are understood to involve a high-grade dedifferentiated mesenchymal component. The low-grade dedifferentiation in this case is particularly unique and may explain the long overall survival with late metastasis of 11 years of the patient which is in stark contrast to the guarded prognosis in typical dedifferentiated chondrosarcoma.
The diagnosis of dedifferentiated chondrosarcoma can be complex due to its similarities to other bony malignancies on presentation. Imaging studies may offer insight; however, biopsy is needed to confirm the diagnosis of dedifferentiated chondrosarcoma. It should be noted that biopsies may mislead clinicians as the dedifferentiated component may not be contained within the specimen taken for biopsy.18,19 The case presented is analogous to previous reports as the initial biopsy had revealed only a grade 2 chondrosarcoma and the low-grade dedifferentiated component was only identified following tumor resection.
Treatment of dedifferentiated chondrosarcomas is centered around radical resection with a strong emphasis on negative margins as numerous studies have highlighted inadequate margin of resection as a negative prognostic factor for survival.6,9,16 With respect to adjuvant therapy, however, there is no consensus regimen for either chemotherapy or radiation therapy. Some studies have demonstrated no improvement in survival of dedifferentiated chondrosarcomas patients treated with neoadjuvant or adjuvant chemotherapy/radiation while Mitchell et al showed improved survival with the addition of doxorubicin and cisplatin though this group only consisted of 11 patients.10,14,16,17 Inadequate margin of resection has also been shown to increase risk of local recurrence, but it remains unclear whether radiation or chemotherapy can assist in preventing recurrence.6,9 In the case presented, the patient was initially treated with surgery alone and despite achieving negative margins, the tumor recurred within 1 year. Two of the 7 subsequent recurrences were treated with radiation in addition to surgery. In one of these instances, the surgical margins were in question, though surgical margins were negative in all other resections. The addition of radiation does not appear to mitigate recurrence, even in this dedifferentiated chondrosarcoma with low-grade dedifferentiated component.
The tumor presented in this case is exceedingly rare and consequently poorly documented in the existing literature. Additionally, this dedifferentiated chondrosarcoma with low-grade dedifferentiated component appears to behave in a starkly different manner to typical dedifferentiated chondrosarcomas which have a dismal prognosis with a 2-year survival of 20% and a 5-year survival of only 7%.7,12 Dahlin and Beabout 5 first defined dedifferentiated chondrosarcoma in 1971 and highlighted the poor prognosis in contrast to conventional low-grade chondrosarcoma. Later series confirmed this poor survival and recent studies have demonstrated similar survival.6,9,20,21 Of note, however, Johnson et al 8 reported a series of 26 patients with dedifferentiated chondrosarcomas, where 3 patients demonstrated a low-grade fibrosarcoma as the mesenchymal component adjacent to the chondroid region. In their series, only 5 patients survived longer than 1 year. All 3 patients with the low-grade fibrosarcoma component survived greater than 1 year with 1 patient alive at 18 months follow up and another alive at 21 months follow up. To our knowledge, the series by Johnson et al is the only previous documentation of the chondrosarcoma with low-grade dedifferentiated mesenchymal component histologically similar to the case presented herein. The clinical course of our case is similar to those presented by Johnson et al and demonstrates a starkly different survival from the typical dedifferentiated chondrosarcomas with a time to metastasis and overall survival of 11 years.
Although dedifferentiated chondrosarcomas are known to involve a high-grade dedifferentiated component, the case presented is one of few reports of a chondrosarcoma with low-grade dedifferentiated mesenchymal component. While the overall survival was significantly better than typical dedifferentiated chondrosarcomas, this tumor aggressively recurred and ultimately metastasized. Clinicians should be aware of this potential sarcoma subtype and counsel patients accordingly.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Informed Consent
The authors confirm that informed consent of the patient was taken for publication of this case report.
Trial Registration
Not applicable.