
Abstract

IgG4-related disease (IgG4-RD) is an autoimmune-mediated disease that can effectively involve every organ system, with limited data on genitourinary tract involvement.1–7 Detailed findings of IgG4-RD involving the prostate consist of mostly single case reports, with the largest known study of histologically confirmed prostatic involvement by IgG4-RD including 9 patients, 2 which comprised a targeted retrospective review of patients with known autoimmune pancreatitis. In order to emphasize that IgG4 prostatitis may be underappreciated among pathologists, herein we report detailed findings from a series of patients with histologic evidence of IgG4-RD identified during routine work-up of urologic symptoms.
We recently encountered 5 specimens of IgG4-RD (the largest known histologic series to date not associated with pancreatitis; all patients meeting diagnostic histologic criteria of highly suggestive of or probable IgG4-RD with additional clinical evidence supporting IgG4-RD based on 2012 pathology consensus criteria 3 ) involving the prostate identified either on prostate biopsy or transurethral prostatic resection, performed for benign prostatic hyperplasia symptomology or clinically nodular prostate. All patients had a prior clinical diagnosis of IgG4-RD and 3 of 5 had a prior (extraprostatic) tissue diagnosis of IgG4-RD. In only 2 patients was the clinical history of IgG4-RD provided at the time of urologic procedure. Additionally, in only 2 patients was the urologist aware of the patient's history of IgG4-RD before the biopsy. Serum IgG4 levels were elevated in all patients at the time of urologic biopsy, with 3 patients taking therapeutic pharmacotherapy for disease at the time of biopsy. All prostatic specimens showed markedly increased IgG4:IgG ratios (>50%) by immunohistochemistry, with 3 of 5 patients showing both storiform fibrosis and obliterative phlebitis (Figure 1). One patient (specimen 5) also showed florid admixed eosinophils almost obscuring the plasma cell population. Light chain analysis by in situ hybridization was performed on 1 patient (specimen 1) and showed polyclonal plasma cells. This same patient also showed high-grade prostatic adenocarcinoma within the targeted magnetic resonance imaging lesion as well as concurrent IgG4-RD in the same biopsy. Follow-up available showed 3 patients with an improvement in symptoms from steroid treatment adjustment after IgG4-related prostatitis was diagnosed. Table 1 depicts clinicopathologic features of study patients.
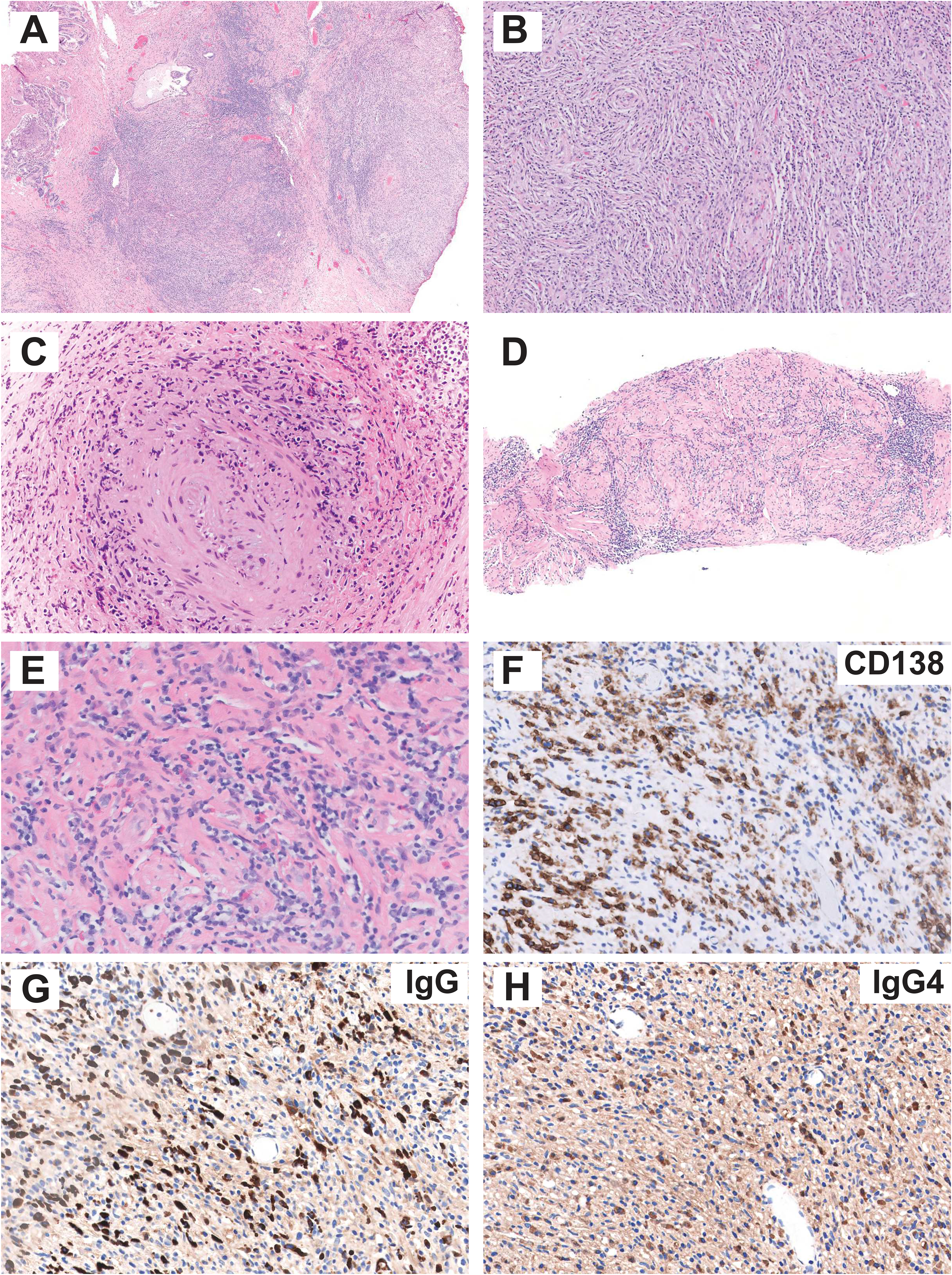
Representative morphologic and IHC findings in prostatic IgG4-RD. (A-B) Low and high-powered images from TURP specimen demonstrating dense chronic lymphoplasmacytic inflammatory infiltrate with storiform fibrosis (specimen 2). (C) Obliterative phlebitis (specimen 5) and also unusual finding of florid eosinophils. (D-E) Low and high-powered images from biopsy specimen with dense chronic lymphoplasmacytic inflammatory infiltrate but otherwise nonspecific histologic findings (specimen 2). (F-H) CD138, IgG, and IgG4 IHC (specimen 2). Abbreviations: IgG4-RD, IgG4-related disease; IHC, immunohistochemical; TURP, transurethral resection of prostate; IgG4-RD, IgG4-related disease.
Clinicopathologic features of IgG4-related prostatitis patients.
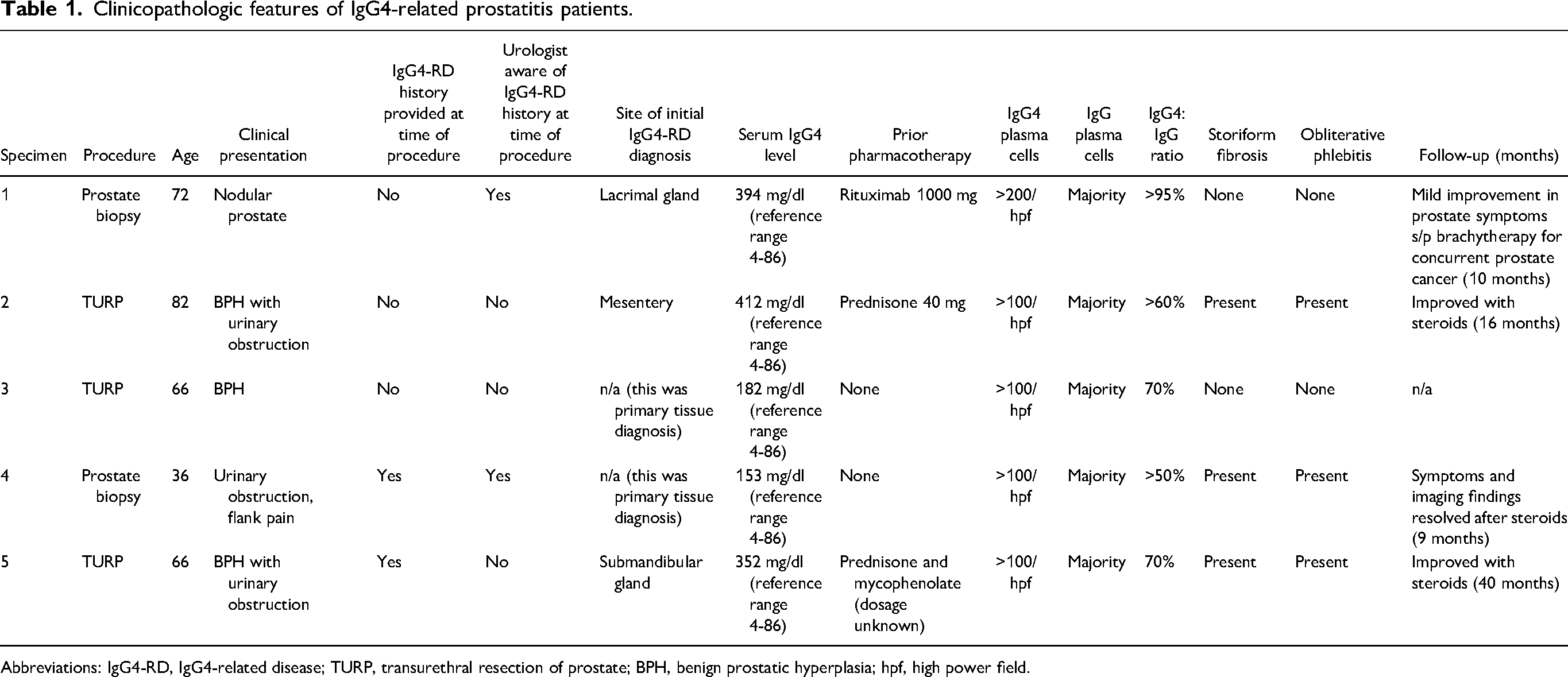
Abbreviations: IgG4-RD, IgG4-related disease; TURP, transurethral resection of prostate; BPH, benign prostatic hyperplasia; hpf, high power field.
Despite the findings depicted from this report, it may be neither cost-effective nor practical for pathologists to employ IgG/IgG4 immunostains as a screening tool on all prostatic specimens with marked inflammation (a fairly commonly encountered scenario) for a putative diagnosis of IgG4-related prostatitis. Rather, some of the histologic clues that should prompt further clinical inquiry into a possible explanation (e.g., prior urologic procedure, presence of a stone, prior history of lymphoma or autoimmune disorder) include a prominent plasma cell component to the chronic inflammation with either storiform fibrosis and/or obliterative phlebitis. However, it should be noted that the latter 2 findings which are well-described histologic features in IgG4-RD3,7 were only present in 3 of 5 (60%) our study patients. Moreover, in the other IgG4-associated prostatitis studies beyond single case reports, storiform fibrosis was identified in only 25% of their patients with only 17% showing obliterative phlebitis,2,5 although it should be noted that in some instances scant tissue as often in needle biopsies might preclude adequate assessment for these features (the single specimen showing obliterative phlebitis was from a radical prostatectomy specimen 2 ). However, specimens can lack the full histological spectrum associated with IgG4-RD, and other organ involvement or serum IgG4 > 135 mg/dL can help confirm the diagnosis of IgG4-RD, 3 the latter which was seen in all 5 of our patients. Nonetheless, despite an absence of the patient's history of IgG4-RD being provided to pathology at the time of urologic biopsy, clinical inquiry (namely chart review, not necessarily asking the urologist) in most instances should provide the most useful managerial information to stratify those patients warranting formal IgG/IgG4 immunohistochemical testing, as the vast majority of patients with prostatic involvement also showed other sites of organ involvement (96% 5 ). In 2 of 5 of our patients, the prostate gland was the primary tissue diagnosis, though both showed increased plasma serum IgG4 levels; therefore inquiry into the patient’s chart may be the first step in the setting of probable or highly suggestive histologic features. While prostatic involvement by IgG4-RD has been estimated at 15% of all IgG4-RD patients, 5 based on the paucity of reports in the genitourinary pathology literature, we suspect IgG4-related prostatitis is an under-appreciated finding for pathologists, which in some instances can have therapeutic and symptomatic implications.1,2,4,5
Footnotes
Author Contribution
ARS and EC established the study design and ARS wrote the original draft of the manuscript. ARS, FM, EM, and EC collected specimens, analyzed immunohistochemistry and histopathology, and provided critical revision and final approval of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This was a retrospective study not interfering with diagnosis and patient management.