
Abstract
A congenital melanocytic nevus is a benign melanocyte proliferation, that may be complicated by malignant transformation. We are reporting a three-year-old girl, who had a giant congenital melanocytic nevus on her back, that was treated by serial surgical excisions with tissue expander insertion. Histopathological examination confirmed the diagnosis of congenital melanocytic nevus with ganglioneuroma. Out of approximately 250 case reports on congenital melanocytic nevus, we identified only two reports of medium/large congenital melanocytic nevus with cutaneous ganglioneuroma. Due to the potential malignant transformation of congenital melanocytic nevus, reporting the features and characteristics of such rare findings may help in further understanding congenital melanocytic nevus, its associations, and prognosis.
Introduction
A congenital melanocytic nevus is a benign melanocyte or nevus cell proliferation that usually presents at birth or develops within the first six months of life. 1 It is apparently caused by one or more identified mutations that result in defective proliferation or differentiation of melanoblasts, the precursor cells of melanocytes. 2 It usually presents as a brown to black skin lesion with well-demarcated borders and flat or mamillated surface, with or without hair.2,3 Congenital melanocytic nevus widely varies in size, ranging from a small size of less than 1.5 cm to a giant lesion, which has at least >20 cm projected adult size. 4 While the incidence of congenital melanocytic nevus is relatively frequent (1%), giant congenital melanocytic nevus is very rare and is probably seen once every 20,000–50,000 live births.3,5 The clear disfiguring nature of the congenital melanocytic nevus lesion and the associated painful treatments may have significant impacts on the psychological, social, and quality of life of the patient and family. 6 Congenital melanocytic nevus may be associated with several diseases/syndromes, including neurocutaneous melanosis, neurofibromatosis, epidermal nevus syndrome, and Carney syndrome. 7 The most serious complication of congenital melanocytic nevus is the possibility of malignant transformation, such as cutaneous melanoma and rhabdomyosarcoma.4,8,9 Congenital melanocytic nevus are treated by surgical excision or conservative treatments, according to size, location, and other risk factors.4,6 Here we are reporting a rare case of a giant ganglioneuroma arising in congenital melanocytic nevus in a patient with cardiac anomalies.
Case Report
A one-day-old baby girl was delivered with an emergency cesarean section at 43 weeks of gestation due to uteroplacental insufficiency (prolonged deceleration on cardiotocograph). Antenatal care records showed a history of symmetrical intrauterine growth restriction (IUGR), anhydramnios, and cardiac defects including ventricular and atrial septal defects. The baby had a good Apgar score after birth. Echocardiogram showed a double-outlet right ventricle, large unrestrictive sub-aortic ventricular septal defect, unrestrictive pulmonary blood flow, and large patent ductus arteriosus.
On the day after delivery, the baby was referred to dermatology to assess a skin lesion over the back. On examination, the patient had a giant congenital melanocytic nevus on her back extending from the level of the scapula down to the coccyx and from end to end laterally, measuring around 16 × 12 cm. Additionally, there were satellite nevi over the rest of the back, the occipital area of the scalp, and the upper and lower limbs (Figure 1). The giant lesion was flat but some of the satellite lesions were raised. All lesions were not hairy. Further, the patient has low-set ears, a depressed nasal bridge, a picked nose, and micrognathia, with no facial asymmetry. The parents had a positive history of consanguinity without similar lesions in both families. Whole exome sequencing test was done to rule out leptomeningeal disease and the result was negative. Magnetic resonance imaging of the brain and spine was suggestive of leptomeningeal melanosis and intraparenchymal melanosis.

A photo taken at the age of 3 months before the cardiac surgery, showing the congenital melanocytic nevus and some of the satellite lesions, as well as two soft subcutaneous nodules suggestive of subcutaneous hemangiomas.
Cardiac defects were repaired at the age of 3 months. However, the patient developed a 3 cm long, horizontal superficial laceration over the lumbar area at the congenital melanocytic nevus site, noticed after surgery, with no active bleeding but with on/off oozing. MRI showed two subcutaneous soft tissue lesions at the lumbar area, the largest one was measuring 6.9 × 26 × 23 mm, more likely to be hemangiomas rather than subcutaneous melanosis due to lack of the high T1 signal expected to be seen with melanin.
Treatment of congenital melanocytic nevus was started at the age of 3 years when the patient underwent the first surgery of serial excisions with tissue expander insertion in the parascapular area. The first excision was done through a mid-back elliptical incision, with full-thickness excision until the back superficial fascia. An excisional specimen was sent for histopathological examination, which revealed a benign dermal melanocytic lesion occupying the superficial and part of the mid dermis. The superficial components are arranged in nests and the deeper parts reveal smaller single cells. Underneath the melanocytic nevus, there are nodular aggregates of mature ganglion cells intermixed with fascicles of Schwan cells. No atypia, mitoses, or necrosis were seen (Figure 2). The diagnosis of congenital melanocytic nevus with ganglioneuroma was confirmed. The patient was last seen at the age of 4 years, when she was admitted for removal of previous tissue expander and surgical excision of back lesion. The patient was healthy and fine at the time of admission.
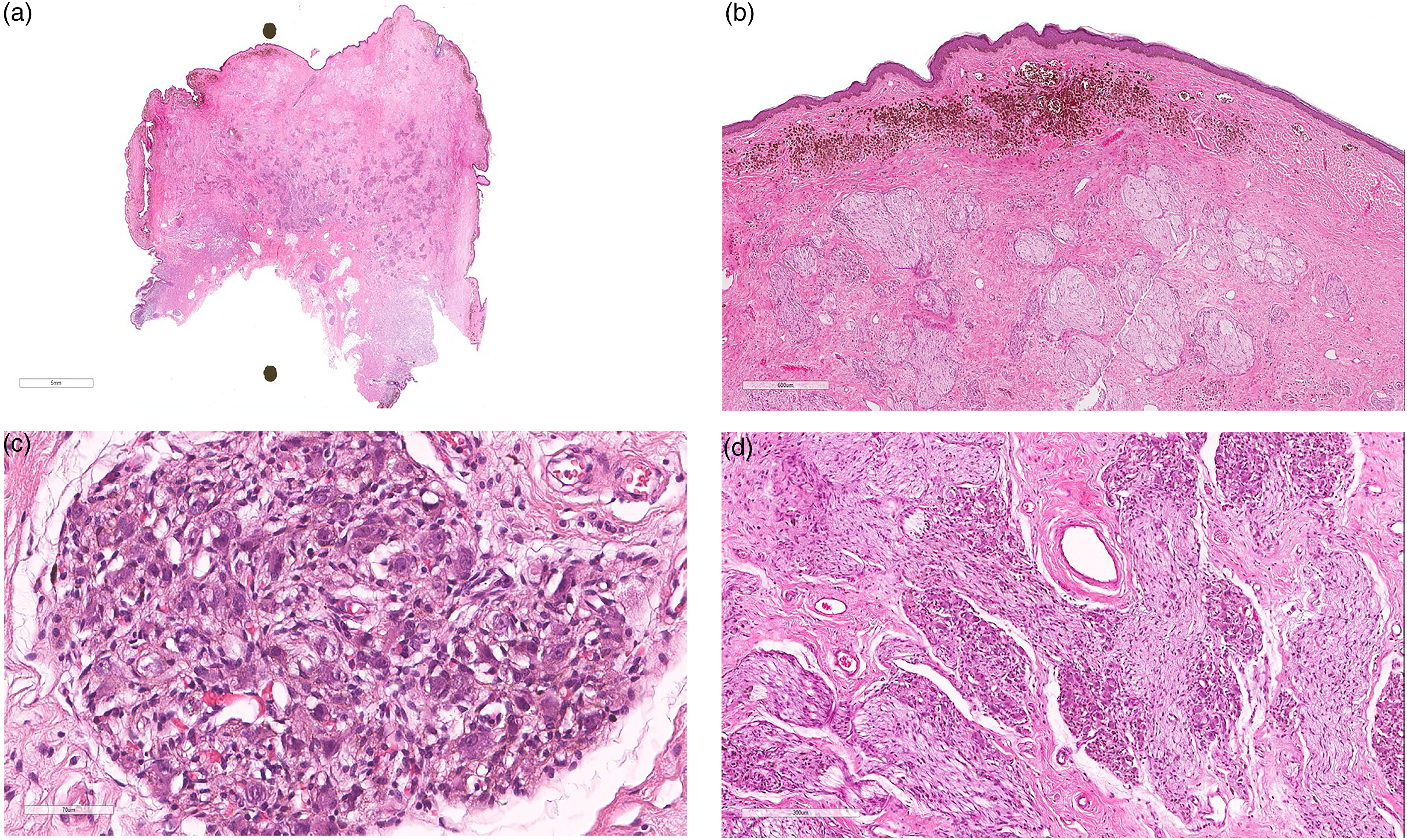
Histopathology of a congenital melanocytic nevus with ganglioneuroma. (a) Panoramic view of hematoxylin and eosin (H&E) stained lesion showing the superficial component of nevus and the underlying component of ganglioneuroma. (b) 2× magnification of H&E stained lesion showing dermal melanocytic nevus and underlying nerve bundles. (c) 40× magnification H&E stained lesion showing a group of ganglion cells (large cells with enlarged eccentric nuclei and eosinophilic cytoplasm). The nuclei harbor prominent nucleoli. (d) 10× magnification H&E stained lesion showing the two components of ganglioneuroma; the fascicles of nerve bundles and the nests of mature ganglion cells.
Discussion
We are reporting a very rare case of giant ganglioneuroma arising in congenital melanocytic nevus in a patient with cardiac anomalies. Congenital melanocytic nevus is frequently associated with neurological anomalies, including neurocutaneous melanosis, and neurofibromatosis, because both conditions are caused by multiple post-zygotic mutations in the neuroectoderm.7,10 Similarly, the current baby had signs of leptomeningeal melanosis and intraparenchymal melanosis on MRI of the brain and spinal cord. Giant congenital melanocytic nevus represents only one in every 200 to 500 congenital melanocytic nevus.1,5 Additionally, the combination of giant congenital melanocytic nevus with ganglioneuroma is extremely rare. Out of approximately 250 case reports on congenital melanocytic nevus, we were able to only identify two reports of medium/large congenital melanocytic nevus with cutaneous ganglioneuroma.11,12 Moreover, the cardiac anomalies are not among recognized syndromes associated with congenital melanocytic nevus, 7 adding further rarity to this case. It should be noted that these cardiac anomalies could be just a coincidence.
The positive history of consanguinity in the baby's parents is likely unrelated, as the disease is not hereditary and the responsible mutations occur during embryogenesis.7,10 The responsible multiple post-zygotic mutations in the neuroectoderm were not identified in the current baby. It has been reported that the clinical outcome of congenital melanocytic nevus is not variable in different genotypic groups. 13 Around 74% of the children diagnosed with congenital melanocytic nevi have at least three typical characteristic facial features. 14 The current baby has a peculiar facial appearance, such as low-set ears, depressed nasal bridge, picked nose, and micrognathia. These were not typical of the facial appearance that was frequently seen in patients with congenital melanocytic nevus syndrome. 14 Additionally, facial appearance does not correlate with the severity of the disease. 14
In addition to congenital melanocytic nevus, the current baby had cutaneous ganglioneuroma, which is a benign tumor derived from neural crest cells which later differentiate into the sympathetic nervous system.12,15 Unlike congenital melanocytic nevus, cutaneous ganglioneuroma is unlikely to have a malignant transformation. 15 However, it should be differentiated from neural crest malignant tumors such as neuroblastomas. 12 Approximately 20 cases of cutaneous ganglioneuroma have been reported worldwide, 15 including only two cases diagnosed in association with congenital melanocytic nevus. 12 Consistent with the current finding, cutaneous ganglioneuromas are commonly seen on the back (30%) and abdomen (20%) and are more common in females than males (65% vs 35%). 15 It usually presents as a round, firm nodule of small size of few millimeters to few centimeters. However, cutaneous ganglioneuromas are less likely to affect neonates and children (20%) compared with adults and older age (80%). 15
When examining a congenital melanocytic nevus, physicians should pay attention to the clinical features of melanoma using the ABCDEF rule that include: Asymmetry, Border irregularity, Color variation (both intralesional color variation as well as a color that is different from the patient's other nevi), Diameter greater than 6 mm, Evolving (a new or changing lesion), and Funny looking “ugly duckling sign.” 16 Furthermore, there is a 7-point checklist that can be used in clinics for urgent referral. This include three major signs; size, shape, or color and four minor signs that are inflammation, crusting/bleeding, sensory change, and diameter ≥7 mm for suspected malignant melanoma; the scoring was weighted (2 for major, 1 for minor signs), and again, any lesion scoring ≥3 warranting referral. 17 Moreover, a systematic review for melanoma risk in congenital melanocytic nevi reported that risk of melanoma is strongly associated with the size of congenital melanocytic nevi, which is greater in garment nevi. 18
Histologically, well-delimited spindle cell proliferation of axon and Schwan cells with scattered mature ganglion cells. 12 Immunohistochemistry studies using antibodies such as Sox10, glial fibrillary acidic protein, neurofilament, or synaptophysin will be helpful to show expression patterns in the nevus and the ganglioneuroma. It was reported that the tumoural spindle cells are vimentin and S-100 protein positive, while they are skeletal muscle-specific actin (HHF-35) negative. Whereas ganglion cells were stained positive for glial fibrillary acidic protein and neurofilaments. 12 The histopathological differential diagnosis for ganglioneuroma includes a well-differentiated cutaneous metastasis of neuroblastoma or ganglion cells entrapped by a plexiform neurofibroma in neurofibromatosis and the malignant neuroblastoma. The current baby has been successfully treated by serial surgical excisions starting from the age of 3. Surgical excision in the current baby is could be the best therapeutic option to avoid the risk of malignant transformation. Additionally, histopathological examination of the excised lesion is the best method to confirm the diagnosis and rule out malignant transformation. It has been reported that the risk of melanoma is much higher in infants with giant congenital melanocytic nevus located on the trunk and congenital melanocytic nevus associated with multiple satellite nevi; both were evident in the current baby. 10 When surgical excisional is decided, it should be started early as the risk of developing melanoma is highest during infancy and early childhood. 19 While surgical excisions cannot eliminate the risk of malignant transformation, it remains the most effective treatment option in patients at high risk of developing melanoma.4,6
Conclusions
We are reporting a very rare case of giant ganglioneuroma arising in congenital melanocytic nevus in a patient with cardiac anomalies. As the patient's presentation met high-risk criteria for malignant transformation, the patient started serial surgical excisions at an earlier age. Since malignant transformation is a life-threatening complication of congenital melanocytic nevus, the patient should be subjected to frequent evaluations of the lesions to assess the risk for malignant transformation and to develop a management plan based on dermatologic, histopathologic, radiologic, and surgical consultations. 19 Due to the potential malignant transformation of congenital melanocytic nevus, reporting the features and characteristics of such rare findings may help in further understanding congenital melanocytic nevus, its associations, and prognosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
Informed consent was obtained from the parents of the patient to publish the case report.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported via funding from Prince Sattam bin Abdulaziz University project number (PSAU/2023/R/1444).