
Abstract

Brief Report
The Liesegang ring (LR) is a hollow, ring-shaped structure that varies in size from 7 to 800 μm. LRs are usually spherical but can appear in a variety of shapes and sizes. LRs occur as a consequence of periodic precipitation of subsaturation and supersaturation of insoluble products in a colloidal matrix. 1
They are commonly identified in vitro on agar plates, test tubes, and other laboratory gels, they are rarely recognized in human tissues. Most reports in human tissue occur in the kidneys, though rare cases have been found in the breast, female genitalia, or skin. LRs have been reported to be associated with benign cysts, inflammatory disease, fibrosis, and tissue necrosis. No report of this condition in the lung has been published. The observation of LRs in tissues is meaningful because it can be confused with parasite eggs and misdiagnosed. Fewer than 30 cases of LRs have been reported in the English literature.2–8 Herein, we describe an exceptional case of LRs associated with allergic bronchopulmonary aspergillosis and review the reported literature for histopathological features of LRs.
A 71-year-old female patient was admitted to the cardiothoracic surgery department because of increased consolidation in the right lung on chest computed tomography (CT) scan. She had a past medical history of rectal cancer (2003), pulmonary tuberculosis (2006), aneurysmal neck clipping (2015), and bronchopneumonia (2020). The patient was diagnosed with asthma and had been treated with steroids for 10 months. During the laboratory evaluation, her total immunoglobulin E (IgE) count was significantly elevated to 427.0 IU/mL (normal range, <100.0 IU/mL). The QuantiFERON-TB Gold and Aspergillous antigens were positive. The chest CT scan demonstrated bronchiectasis with mucus retention in the right middle lobe. High attenuated mucus level was present on the non-contrast image, and patchy areas of consolidation were combined (Figure 1A). Based on these clinical and radiological findings, the impression was pulmonary tuberculosis, aspergillosis, and lung abscess. Hence, the patient underwent video-assisted thoracoscopic surgery for diagnosis and treatment.
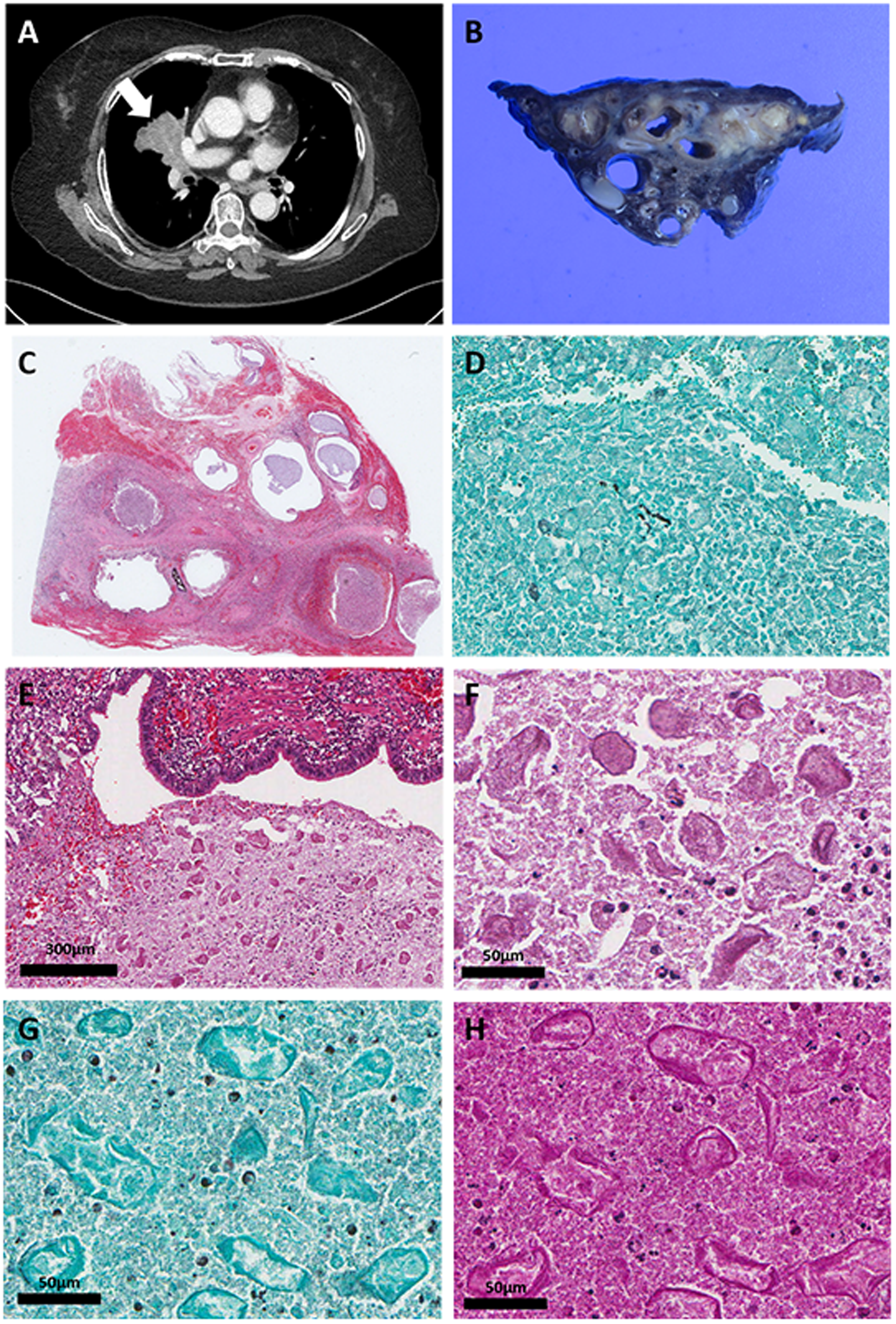
Radiological and pathological findings of pulmonary lesion. (A) The chest computed tomography demonstrated bronchiectasis with mucus retention in right middle lobe. High attenuated mucus showed in non-contrast image and patchy areas of consolidation was combined (arrow). (B) Macroscopically, multiple cystic lesions were observed. White gelatinous materials were present within the cystic lesions. (C) The resected specimen revealed airway destruction by dense inflammation with mucoid impaction (hematoxylin–eosin [H&E], scan view). (D) Fragmented fungal hyphae were positive for GMS. (E) Many structures with various sizes and shapes have been observed in ectatic lumen (H&E, 80×). (F) Ring-shaped structures have been found in various shapes ranging from circular to rectangular, each with irregular stratified walls, lobulated configurations, and central cores (H&E, 400×). (G) In special stain, the rings were negative for GMS (original magnification, 400×). (H) Periodic acid-Schiff highlighted laminated ring-like structures (original magnification, ×400×).
The resected lung specimen measured 8.5 × 8.3 × 2.0 cm. On cut surface, multiple cystic lesions ranging from 0.5 to 2.4 cm in size were observed. White gelatinous materials were present within the cystic lesions (Figure 1B). On scan view, the hematoxylin–eosin (H&E) slide revealed airway destruction by dense inflammation with mucoid impaction (Figure 1C). The ectatic bronchus was filled by necrotic tissue and eosinophilic material. The impacted mucus contains inflammatory cells composed of eosinophils and neutrophils. The walls of the small bronchus were replaced by necrotizing granulomatous inflammation. In the lumen, a scant amount of fragmented fungal hyphae was identified by Grocott-methamine silver (GMS) stain (Figure 1D). Based on clinical manifestation and histological findings, the lesion confirmed to be an allergic bronchopulmonary aspergillosis.
In addition, in the ectatic lumen, acellular laminated ring-like structures were recognized (Figure 1E). The ring-like structures were found in a variety of shapes from round to rectangular, and each had an amorphous, eosinophilic, and central core surrounded by a layered wall. The ring-like structures had a variety of sizes ranging from 30 to 100 um (Figure 1F). In special stain, the rings were negative for GMS, Congo red and von Kossa stain results (Figure 1G). Periodic acid-Schiff highlighted laminated ring-like structures (Figure 1H). These structures were interpreted as LRs. Finally, a diagnosis of allergic bronchopulmonary aspergillosis with LRs was rendered.
The term “Liesegang ring” was first introduced by Ralph E. Liesegang to describe a structure that shows acellular and concentric laminated features. 1 The LR is an incidental finding observed alongside various conditions, including benign cysts, inflammation, and malignant neoplasms.5,9 Morphologically, LRs resembled the ova and cross-sections of Dioctophyma renale or the ova and developing larvae of Trichuris trichiura in renal cysts. Unlike in ova, histopathological findings lacking flattening at the poles and showing marked variations in size and shape can help to differentiate LRs from a parasitic infection. Also, the dual-layer structured wall of LRs can offer a clue to their non-parasitic nature. 10 The eggs of Paragonimus westermani are commonly observed in the lung, and the LRs observed in this case were similar in size to these eggs, requiring differentiation. However, the eggs of this organism are yellowish-brown and ovoid.
The pathogenesis of LRs in human tissue has not been elucidated. In vivo LRs are primarily formed in supersaturated colloidal systems, and cystic or inflammatory processes could potentially play a role in the formation of this environment. 7 Although the mechanism related to LR formation in this case could not be elucidated, it is possible that long-term retention of secretions and degenerated materials in the dilated bronchi may be related to their formation.
In conclusion, LR is a rare and incidental finding during pathological examination, and pathologists should be aware of its structures to avoid its misdiagnosis as a parasitic infection. We presented a case of allergic bronchopulmonary aspergillosis with LRs mimicking parasite eggs. This case report will help to clarify the histopathological characteristics of LRs and to establish a precise differential diagnosis.
Footnotes
Authors’ Contributions
Ae Ri Ahn, Jong Jin Sung, and Myoung Ja Chung summarized the pathological and genomic data; Min Gi Shin and Yong Chul Lee summarized the clinical data; Ae Ri Ahn, Jong Jin Sung, and Myoung Ja Chung contributed as pathologists; Ae Ri Ahn, Jong Jin Sung, and Myoung Ja Chung organized the study and wrote the manuscript. All authors read and approved the final manuscript.
Ethics
This case report was approved by Jeonbuk National University Hospital Institutional Review Board (approval no. IRB 2022-08-034). Patient consent was obtained for publication. This case report was conducted in accordance with the Declaration of Helsinki of 1975.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.