
Abstract
Melanosis of the urinary bladder, so-called melanosis vesicae, is a rare condition characterized by dark, velvety bladder mucosa observed by cystoscopy examination. Up to 20 examples have been reported in the English literature, and the etiology of this disease still needs to be discovered. We present an 82-year-old woman with a history of pelvic organ prolapse-associated urinary symptoms. The patient was found to have pigmented urinary bladder mucosa on cystoscopy and underwent a total hysterectomy and bladder mucosal biopsy. Histologically, pigmented granules were evident in the bladder stroma and epithelium, highlighted by Periodic Acid-Schiff (PAS) stain, suggestive of lipofuscin in nature. We outline the diagnostic features of bladder melanosis, discuss the diagnostic mimickers, and thoroughly review the literature on the subject.
Introduction
Urinary bladder melanosis is a recently recognized very rare phenomenon or condition, often incidental findings observed by cystoscope, which is characterized by the deposition of black pigments within the urothelium and lamina propria without the presence of melanocytes. 1 Under cystoscopy, the bladder mucosal surface has a dark brown, velvety look that is frequently patchy or multi-focal. 2 The skin and mucocutaneous tissue of the oral cavity, genitalia, and conjunctiva are commonly affected. Melanin is one of the most common pigments. It is usual to find excess lipofuscin deposition in tissues as well. The amount of lipofuscin changes significantly with age and rises in older people in the heart, liver, skeletal muscle, and adnexal skin structures. Melanosis coli and the black thyroid are examples of specific, non-age-related conditions where lipofuscin deposition occurs. There have also been reports of localized lipofuscinosis in the esophagus, fallopian tubes, and gallbladder. It can be mistaken for hemosiderosis, endometriosis in women, and primary or metastatic melanoma. Its clinical significance still needs to be discovered, and no defined management guidelines are in place. Herein, we report an example of urinary bladder melanosis with a literature review.
Case Report
An 82-year-old woman presented with urge urinary incontinence and voiding dysfunction with a history of stage 4 pelvic organ prolapse. She had no urinary tract infections and was referred for urologic evaluation. Ultrasound showed a significant post-void residual (∼600 ml). Cystoscopy showed pigmented lesions of the bladder and focal diffuse reticular black discoloration of the bladder mucosa (Figure 1). The patient has no history of melanoma. Biopsies taken from the darkly pigmented flat lesions and the reticular pigmented areas demonstrated numerous small aggregates of pigmented granules deposited in the benign urothelium and the lamina propria. The pigments are highlighted by PAS staining (Figure 2), suggestive of lipofuscin in nature. Immunohistochemical stains for S-100, HMB-45, Melan-A, and SOX10 were performed and are negative for melanocytes (Figure 2). The endoscopic and histopathologic findings are consistent with bladder melanosis. The patient underwent a hysterectomy and is currently asymptomatic one year after the cystoscopy.
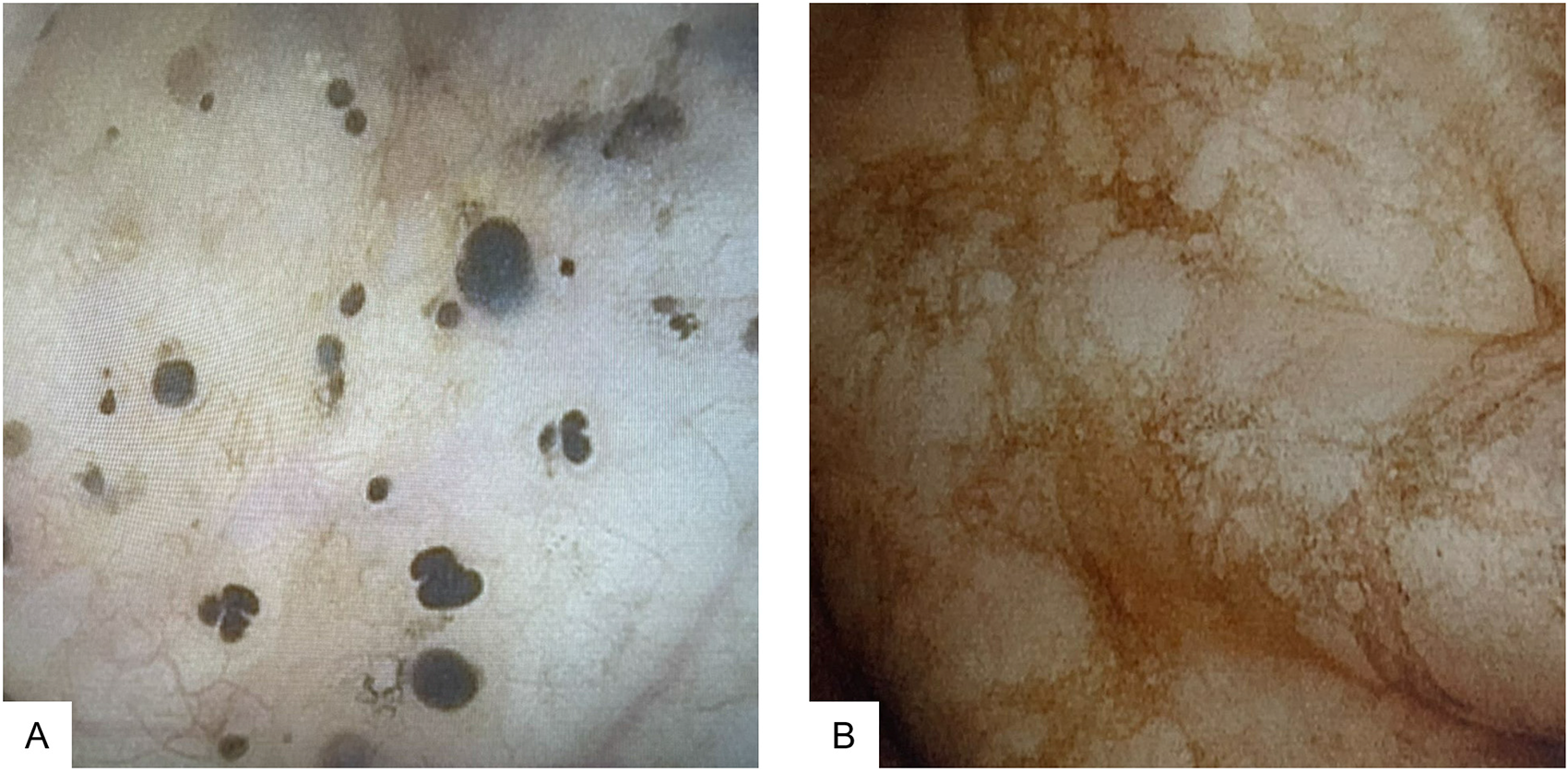
Cystoscopy showed scattered black lesions and focal diffuse reticular black pigmentation of the bladder mucosa.
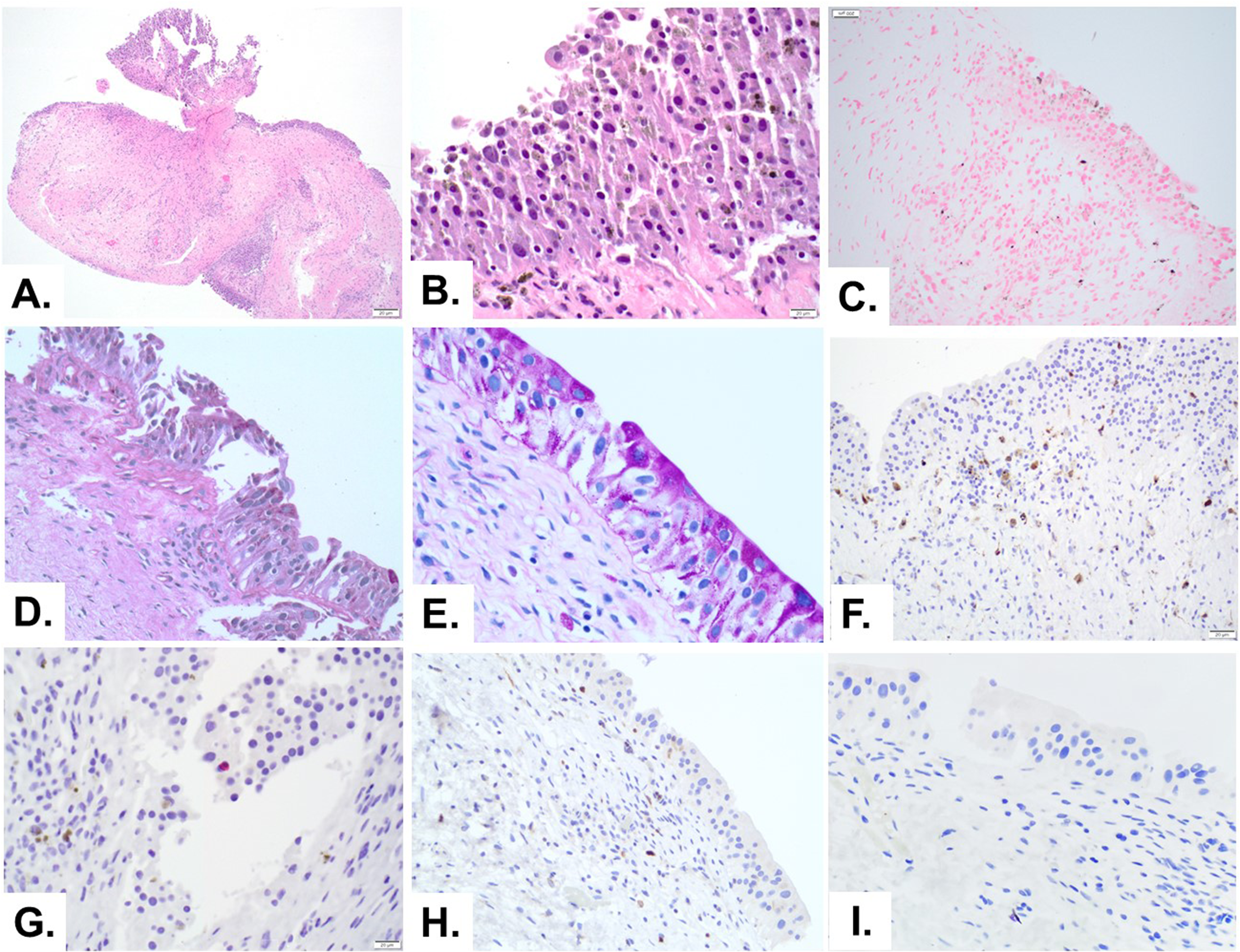
Melanosis in bladder biopsy. (A and B) The hematoxylin-eosin stain of bladder mucosa shows aggregates of black granules in the mucosa and lamina propria. (C) Fontana-Masson staining shows pigments in the mucosa are mainly negative. (D and E) Periodic acid-Schiff staining highlights the pigments, suggestive of lipofuscin in nature. Immunohistochemical stains for S-100 (F), HMB-45 (G), MelanA (H), and SOX10 (I) are negative for melanocytes with pigments in the background.
Discussion
According to medical dictionaries (such as Merriam-Webster Medical Dictionary), melanosis is the unexpected discoloration or dark pigmentation of tissues discovered upon gross inspection. It is brought on by the abnormal deposition or development of black or dark pigment (melanin and occasionally other pigments) in the tissues. According to this definition, melanosis does not always require that the pigment is melanin, and “melanosis coli” is the term used to describe the black coloring of the colonic mucosa caused by an accumulation of lipofuscin. A more specific definition is that melanosis refers to increased tissue pigmentation brought on by melanin pigmentation. Pseudomelanosis is used in this context to describe accumulations of lipofuscin that give tissues a dark brown to black hue.
Up to 20 examples of melanosis of the urinary bladder have been documented in the English literature. Only a few instances have “lipofuscinosis,” and most recorded cases of dark staining of the bladder mucosa have been attributed to melanin.1–3 These have been seen in men and women between the ages of 41–86; most patients are Caucasians with no urothelial atypia.
Clinically, the patients have presented with non-specific symptoms, including urinary frequency, incontinence, dysuria, malodorous urine, nocturia, hematuria, and recurrent cystitis. 3 The bladder lining exhibits diffuse or regional dark brown to black discoloration with no site preference under the cystoscope. Histologically, dark brown pigments are primarily found in the urothelial cells3–7 with or without pigment-laden macrophages in the superficial lamina propria.3,4,8 The pigments are non-refractory and granular and can form globules of varying sizes. Fontana Masson stain is positive for the pigments, whereas PAS and iron stains are negative. The melanin pigment disappears upon melanin bleaching using strong oxidizing agents such as potassium permanganate or hydrogen peroxide.
Lipofuscin and hemosiderin deposits should be distinguished from melanin pigments. Lipofuscin deposits are more common in colonic biopsy specimens known as melanosis coli or lipofuscinosis coli. They are usually associated with colonic stasis/constipation with laxative use. Under colonoscopy, the intestinal mucosa usually shows dark discoloration, and histological examination reveals pigment-laden macrophages in the lamina propria. The melanotic pigment is due to undigested and oxidized lipidic residues, which increase oxidative stress in the urothelium. Long-term ciprofloxacin medication 3 and phenacetin abuse, 4 both of which stimulate the formation of free radicals during metabolism, have been linked to lipofuscinosis of the urinary bladder. The pigment is positive for PAS, Sudan black B or long Ziehl-Neelson acid-fast stains, and bleach resistant. Lipofuscin accumulation has also been shown in superficial urothelial cells of the urinary bladder in aging mice with significantly increased levels of oxidative stress. 5
Hemosiderin is an intracellular storage form of iron produced by the phagocytic digestion of hematin. They appear as a golden yellow-brown intracellular or extracellular pigment which is positive for iron stains. Excess iron deposition in tissue is known as hemosiderosis, which occurs predominantly in hepatocytes and the reticuloendothelial system (spleen, bone marrow, and liver). Hemosiderosis of the urinary bladder is rare and was reported in a man with multiple a history of blood transfusions as part of treatment for his anaplastic anemia. Histologically, the urothelial mucosa showed prominent hemosiderin deposits and hemosiderin-laden macrophages in the lamina propria with unremarkable urothelium. 6 The pigments are positive for iron stains.
Most notably, primary vesical or metastatic malignant melanoma is the most common differential diagnosis of bladder melanosis. Malignant melanoma is characterized by proliferating of malignant melanocytic cells with pleomorphic nuclei, spindle and polygonal cytoplasmic contours, and intracytoplasmic melanin pigment.7–9 However, the presence of melanocytes, usually identified by immunohistochemistry positivity for S-100 and HMB-45, was not consistently found in all described bladder melanosis examples. As in normal skin, the urothelial cells appear to have taken up melanin in lysosomes rather than via dendritic melanocytes. If present in urinary bladder mucosa, Melanocytic cells are assumed to have migrated improperly from the neural crest during embryogenesis or generated from urothelial stem cells that had undergone aberrant differentiation. Primary malignant melanoma is very rarely identified in the genitourinary tract, and melanoma deposits in these organs are typically assumed to be metastatic unless proven otherwise. Bladder melanosis has been reported to be associated with primary malignant melanoma of the urinary bladder.8,9 Because of the low number of bladder melanosis examples, biological behavior is not well understood, and the longest reported follow-up is ten years without malignant progression. 10 Many authors consider simple melanosis a harmless condition.9–12 There needs to be a guide in the literature on how to handle this illness clinically, mainly on whether cystoscopy surveillance is necessary. A major operation like a cystectomy is not recommended. The authors have decided to keep this patient's bladder melanosis under cystoscopy surveillance.
Conclusion
Melanin pigment or other pigments, such as lipofuscin accumulation in the urothelium and lamina propria, are referred to as urinary bladder melanosis. It is a rare condition that is thought to be benign. Melanin can be distinguished from other pigments, such as lipofuscin and hemosiderin. Primary or metastatic malignant melanoma should be considered as well. A correct diagnosis requires a thorough examination of histological features and the use of specific stains such as Fontana Mason, iron, and PAS, bleach treatment, and immunohistochemistry stains for melanocyte. There needs to be clear guidance on how to handle it clinically due to the rarity and unknown course of urinary bladder melanosis. It might be prudent to initiate cystoscopy surveillance of patients with this condition.
Clinical characteristics of some reported examples of urinary bladder melanosis.
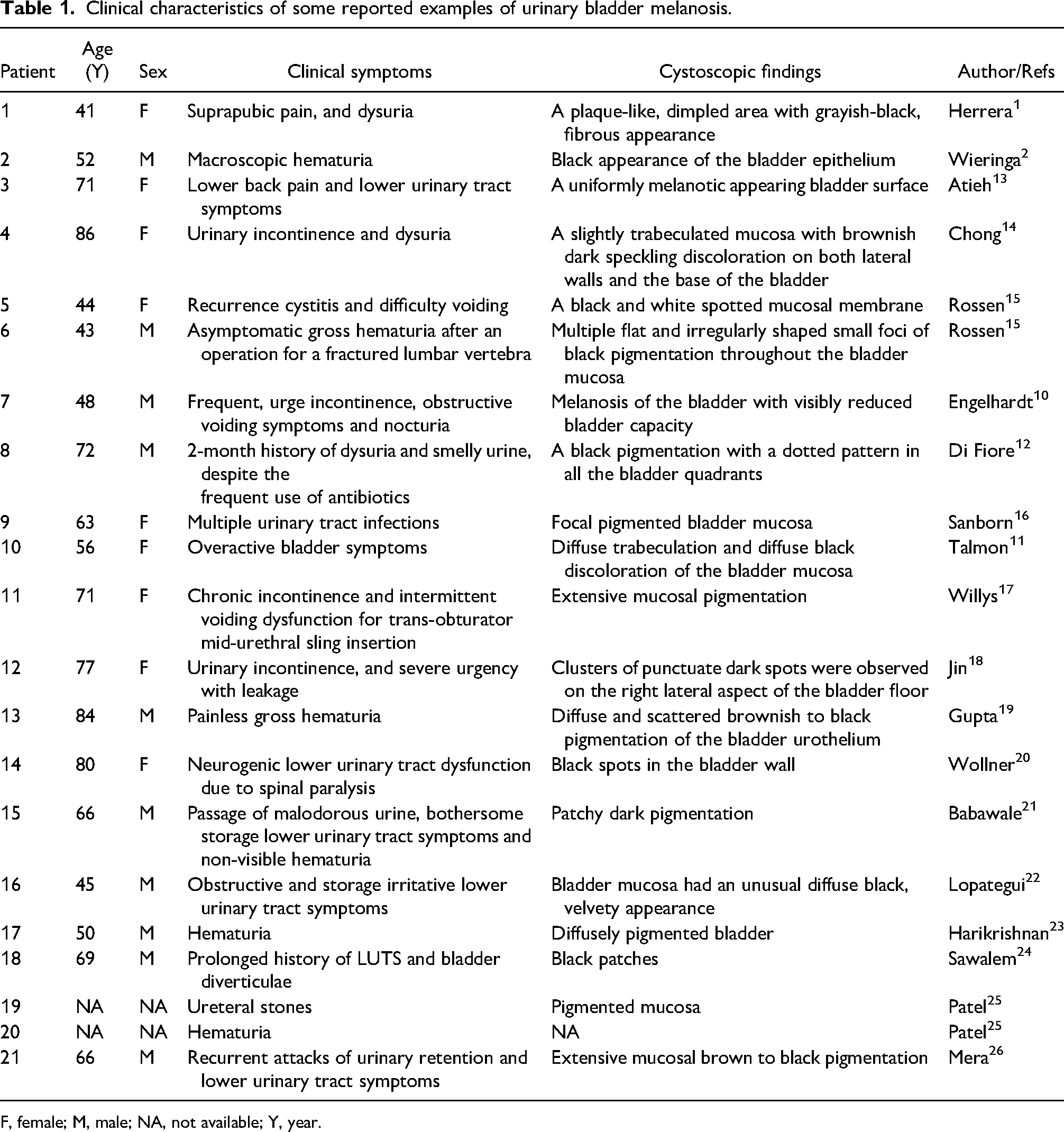
F, female; M, male; NA, not available; Y, year.
Footnotes
Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.