
Abstract
Carcinosarcomas of mediastinum are rare and only few well-documented cases are available in the literature. We report a detailed description of mediastinal carcinosarcoma with unique clinical manifestations and immunohistochemical and molecular profiles. A 44-year-old female with an enlarging anterior mediastinal mass was found to have a positive pregnancy test. Thoracoscopic biopsy revealed that the mass represented a carcinosarcoma with adenocarcinoma and chondrosarcoma components. The tumor focally expressed beta-HCG by immunohistochemistry and had KRAS G12A missense mutation by next generation sequencing. The case documents a rare presentation of carcinosarcoma within the mediastinum with uncommon paraneoplastic syndrome and genetic profile. Awareness of these unusual clinical and pathological manifestations of the tumor will help in reaching correct diagnosis and proper management of such patients.
Keywords
Background
Carcinosarcoma is a rare malignancy that is defined as a biphasic tumor composed of epithelial (carcinomatous) and malignant heterologous mesenchymal (sarcomatous) components. 1 carcinosarcoma are most common in the uterus but also occur in other organs including lung. 2 Only rare carcinosarcoma have been documented in the mediastinum.3–8 In the mediastinum, the tumor is presumed to originate from the thymus, or from the lung with invasive spread into mediastinum. Here we provide a detailed clinicopathological description of carcinosarcoma presenting within the mediastinum and showing unusual paraneoplastic and genetic profiles.
Case Presentation
A 44-year-old female, nonsmoker, G9P9009 with past medical history of beta thalassemia, and obesity presented for evaluation of recurrent left pleural effusion. She initially reported radiating left chest pain and progressive exertional dyspnea for over 6 months. While seeking medical attention, she was noted to have elevated urine beta-subunit of human chorionic gonadotropin (beta-HCG) levels (up to 20.7 mIU/mL; normal non-pregnant levels <10 mIU/mL), however, gynecological examination found no signs of pregnancy. Chest x-ray showed a persistent near complete opacification of the left hemithorax suggesting a large mediastinal mass and a partially loculated left pleural effusion. Computed tomography (CT) of the chest revealed a heterogeneous and multi-septate mass occupying the majority of the left hemithorax. The midportion of the mass measured 13.2 × 16.4 cm. Extensive compressive atelectasis of the left lung with partial aeration of the left lower lobe was seen. The lobar atelectasis in the left upper lobe and additional compressive atelectatic foci in the left lower lobe suggested that the lesion did not originate in the lungs (Figure 1). The staging positron emission tomography/computed tomography (PET/CT) demonstrated a hypermetabolic mediastinal and juxta diaphragmatic lymph nodes worrisome for metastatic adenopathy, left-sided pleural effusion with FDG avidity, and non-specific uptake with the left axillary lymph node. There was no extrathoracic disease on PET/CT. Magnetic resonance imaging (MRI) of the brain was negative for intracranial metastasis. The patient underwent video-assisted thoracoscopic pleural biopsy. The light microscopic examination of the biopsy material revealed a cytologically malignant biphasic neoplasm composed of adenocarcinoma and malignant mesenchymal components (Figure 2A and B). Both components were intimately interspersed and present throughout entire biopsy material. The sarcomatoid component was composed of pleomorphic highly proliferative mitotically active spindled cells forming fascicles (Figure 2C and D) and foci of malignant cartilage (Figure 2E). The adenocarcinoma component was composed of mucin producing glands (Figure 2F). By immunohistochemistry, the epithelioid and gland forming cells were positive for keratin AE1/AE3, keratin 7, and focally positive for keratin 5/6 and p40. The mucinous glandular epithelium was also focally positive for CDX2, keratin 20, and GATA3. The chondrosarcomatous component was immunoreactive with S100. Occasional single cells and clusters of cells within glandular component (Figure 2G) and within sarcomatous component (Figure 2H) were immunoreactive with beta-HCG. Immunostains for SALL4, OCT3/4, WT1, PAX8, SOX10, smooth muscle actin, desmin, TTF1, and PDL1 were negative. Based on the morphological and immunohistochemical findings, the tumor was subclassified as carcinosarcoma. Next generation sequencing reveled TP53 N131Y missense mutation (with variant allele fraction of 72.4%) and KRAS G12A missense mutation (with 57.7% variant allele fraction), and copy number gain in MYB, MYC, and PRKN, with tumor mutation burden of 4.2 m/Mb, and stable microsatellite instability status. Following the biopsy, the patient received 1 cycle of carboplatin and paclitaxel as an inpatient. Despite 6 cycles of cytoxan, doxorubicin, and cisplatin (CAP), no significant tumor size reduction was seen. Subsequently she received a total of 2 cycles of pembrolizumab and 46 Gy out of intended 66 Gy of radiotherapy to the mass (Figure 3). Due to development of septic shock, acute kidney insufficiency, and cardiac dysfunction from tumor invasion to the pulmonary veins and left atrium the intended treatment could not be completed. The tumor was resistant to the CAP chemotherapy, PD-1 blockade, and radiotherapy. The patient developed progressive hypoxic respiratory failure, became ventilator dependent, and ultimately passed away.
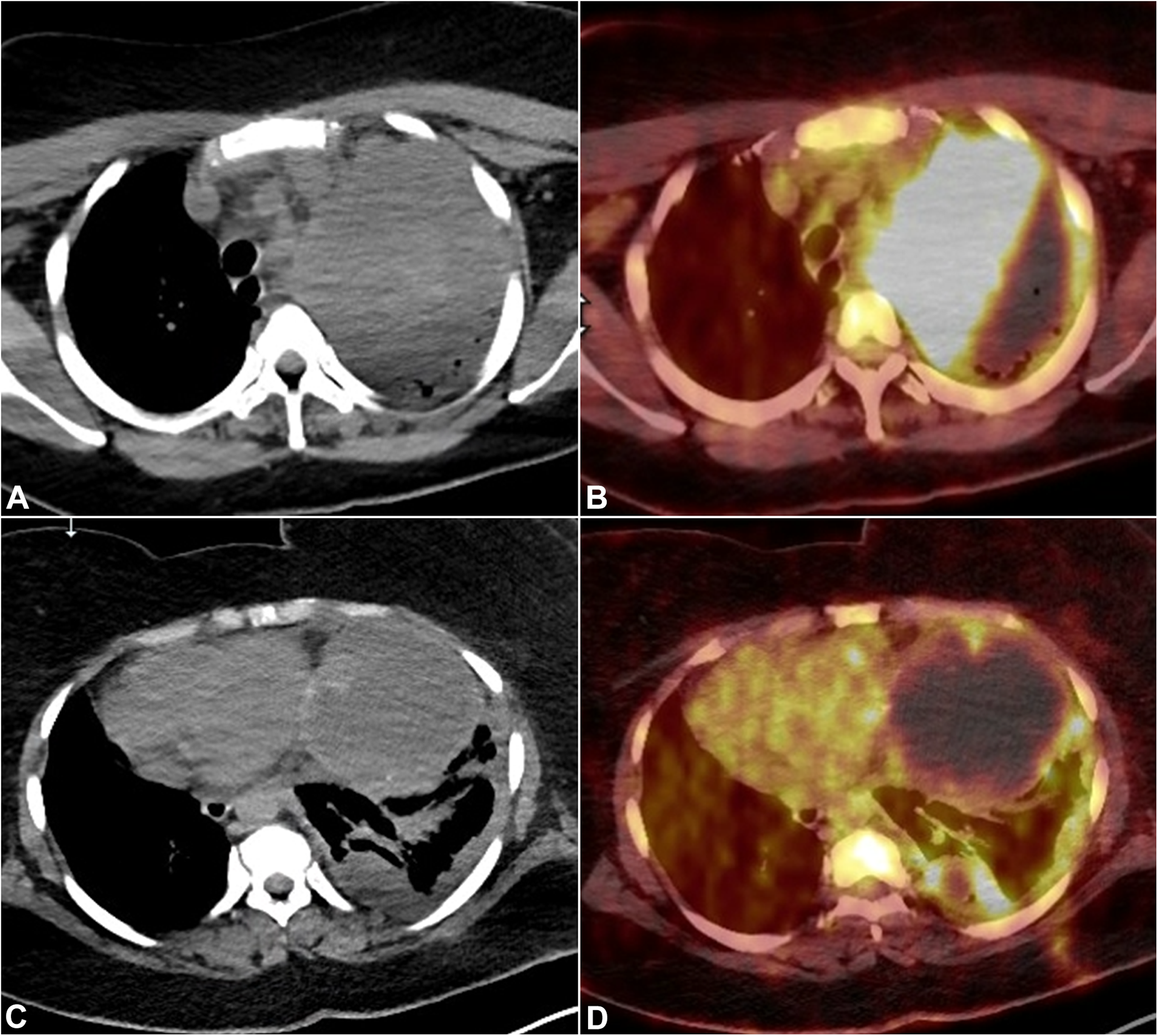
Imaging findings. Axial chest images at the level of mid-trachea demonstrates subtle hyperattenuation of a left mediastinal mass and left upper lobar compressive atelectasis. There are patent air bronchograms within the atelectatic left upper lobe (A). There is markedly increased metabolic activity (maximum SUV of 23.5) within the solid component of the mediastinal mass. Note lack of metabolic activity in the atelectatic left upper lobe (B). Axial chest images at the level of diaphragm show a large cystic component of the mass (C) and left sided nodular pleural thickening with increased metabolic activity within left pleura (D). Computed tomography (CT) and fused positron emission tomography/computed tomography (PET/CT), respectively.
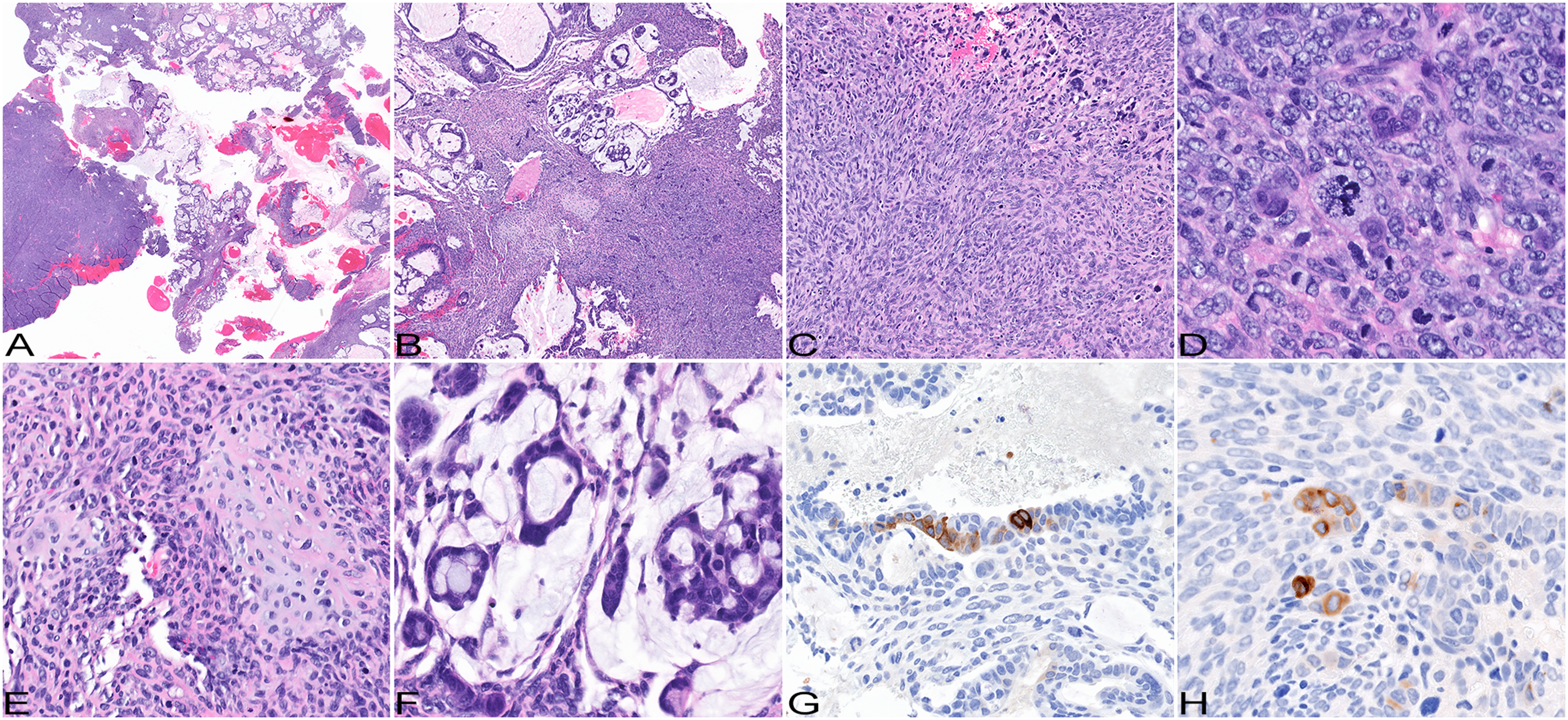
Pathological findings. Pleural biopsy shows a biphasic malignant tumor (A and B); hematoxylin and eosin, original magnification ×4 and ×20. Its less differentiated sarcomatoid component is represented by spindle cells forming fascicles (C), large epithelioid and multinucleated giant cells (D), and malignant cartilage (E); hematoxylin and eosin, original magnification ×100, ×200, and ×200, respectively. Its better differentiated glandular component is represented by papillary, micropapillary, and acinar structures producing abundant mucin (F); hematoxylin and eosin, original magnification ×100. Large epithelioid and tumor giant cells scattered within glandular (G) and sarcomatoid components (H) are positive for beta-HCG; immunohistochemistry, original magnification ×200 and ×200, respectively.
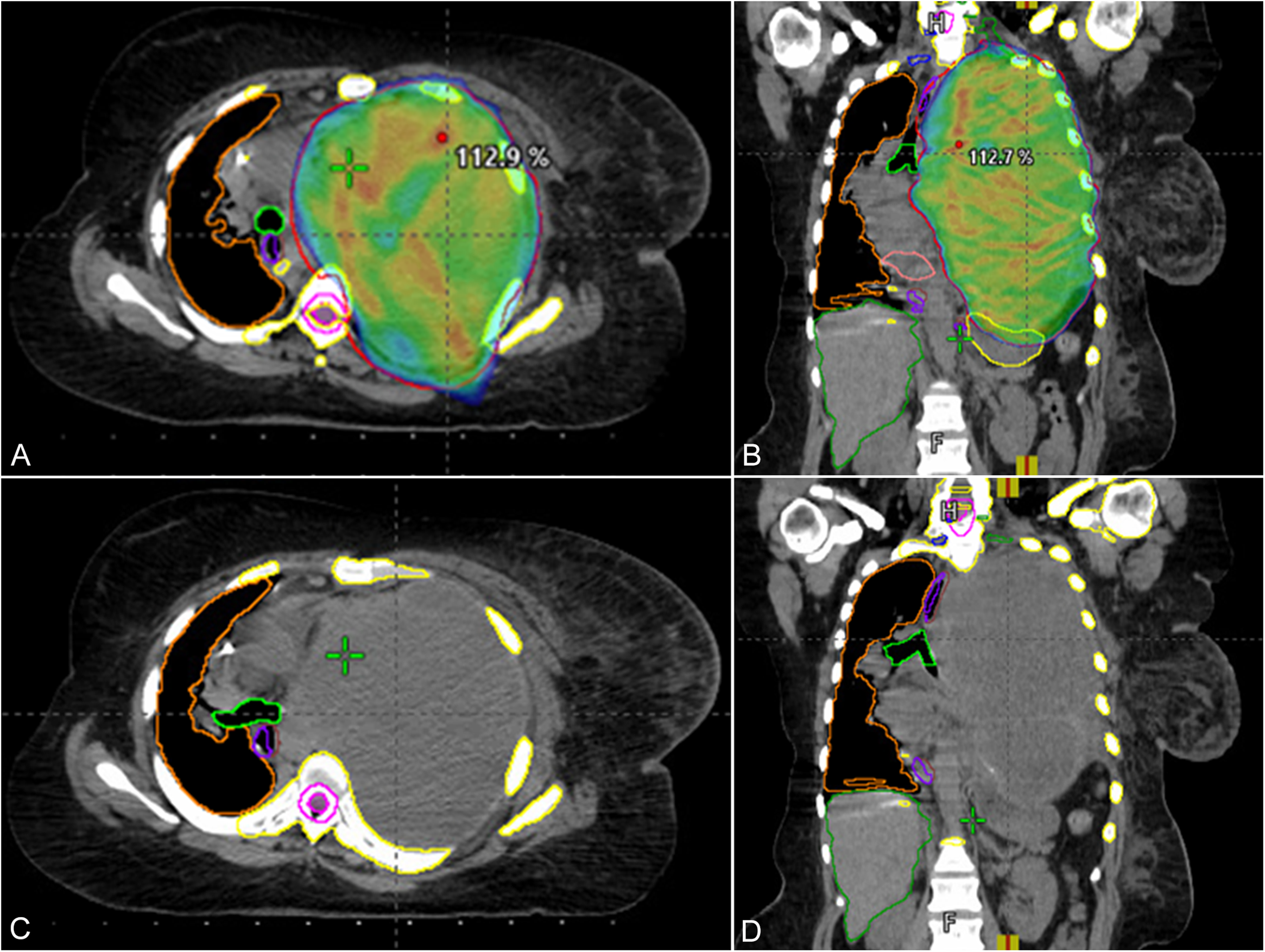
Radiotherapy treatment plan. Computed tomography of chest on admission for septic shock 2 days after 46 Gy show the mass is essentially unchanged in size and mediastinum and heart are shifted to the right. Axial (A, C) and coronal (B, D) views of the mass and radiation treatment dose cloud (>95% isodose line).
Discussion
Based on the tumor location and elevated urine beta-HCG, a germ cell tumor with somatic type malignancy was the main differential diagnostic consideration in this patient. Gonadal germ cell tumor with somatic type malignancy are rare however up to 30% of germ cell tumors with somatic type malignancy occur in the mediastinum.9,10 With rare exceptions germ cell tumors with somatic type malignancy occur in adult males and manifest as a spectrum of malignant tumors including chondrosarcoma and adenocarcinoma.11–13 While the possibility of germ cell tumor with somatic type malignancy cannot be completely excluded, the patient's sex, the lack of conventional germ cell tumor morphology, the low levels of beta-HCG production, and the tumor's immunoprofile with negative germ cell tumor markers (SALL4 and OCT3/4) make that diagnosis unlikely.
Ectopic beta-HCG expression by non-trophoblastic malignancies has been documented in some carcinomas including of lung origin14–16 and therefore a lung primary was also considered in the differential diagnosis. However, the lack of expression of lung specific markers (such as TTF1) and the imaging findings (a dominant tumor mass within the anterior mediastinum with obtuse pushing margins and no air bronchograms within the mass) are more in keeping with its thymic rather than pulmonary origin. Thymic tissue is known to contain cells of varying histogenesis including mucin producing cells. The later are commonly evident during thymic involution accompanied by cystic degeneration and/or thymic cysts and are thought of as an origin of thymic carcinomas. 17
KRAS mutations are found in up to 29.1% of NSCLC, they have also been documented in a low percentage of soft tissue sarcomas (1.33%). 18 Thus, while unusual the observed molecular profile of the tumor in our patient is consistent with what one expects to see in carcinosarcoma, possibly reflecting the genetic make-up of the mucinous adenocarcinoma component.
The epithelial to mesenchymal transition is suggested to play a role in carcinosarcoma pathogenesis. 19 Due to low incidence and poor prognosis, the carcinosarcoma treatment approaches are not well established. 20 Surgery is beneficial as a principal diagnostic mean and standard treatment approach. Radiation therapy and cisplatin and epirubicin based chemotherapy have also been reported, however, their role is still controversial, and no regimen of adjuvant treatment has been established. The radiation and chemotherapy were largely ineffective in this patient.
Sarcomatoid carcinoma is defined as a carcinoma with spindled and/or giant cell components. In the lung it is commonly referred to as pleomorphic carcinoma. 1 There is significant morphological overlap between sarcomatoid carcinoma and carcinosarcoma and therefore, the presence of malignant heterologous component is required for the diagnosis of carcinosarcoma. 1 To the best of our knowledge, only rare cases sharing some of the clinicopathological features with our case have been documented in the English language literature within the last 3 decades3–8 (summarized in Table 1). Some of the prior tumors reported as carcinosarcoma would have been now classified as sarcomatoid carcinoma.3–6 As a group these tumors appear to affect both sexes from 5th to 9th decades of life. The presenting symptoms are not specific and include chest pain and dyspnea. In one of the prior reports, a superior vena cava syndrome was observed. If their size is relatively small, the tumors are confined to the anterior mediastinum, while the large lesions compress adjacent structures and may occupy significant part of the thoracic cavity. On review of the published findings, only 2 reports documented the presence of a distinct malignant heterologous component,7,8 both represented by rhabdomyosarcoma thus justifying a diagnosis of carcinosarcoma based on the current WHO criteria. Testing for beta-HCG was performed in only one patient and was within normal limits. In none of the prior publications was the genetic profile of the tumors investigated.
Clinical and Pathological Findings of Selected Cases of Carcinosarcoma and Sarcomatoid Carcinoma of Mediastinum.
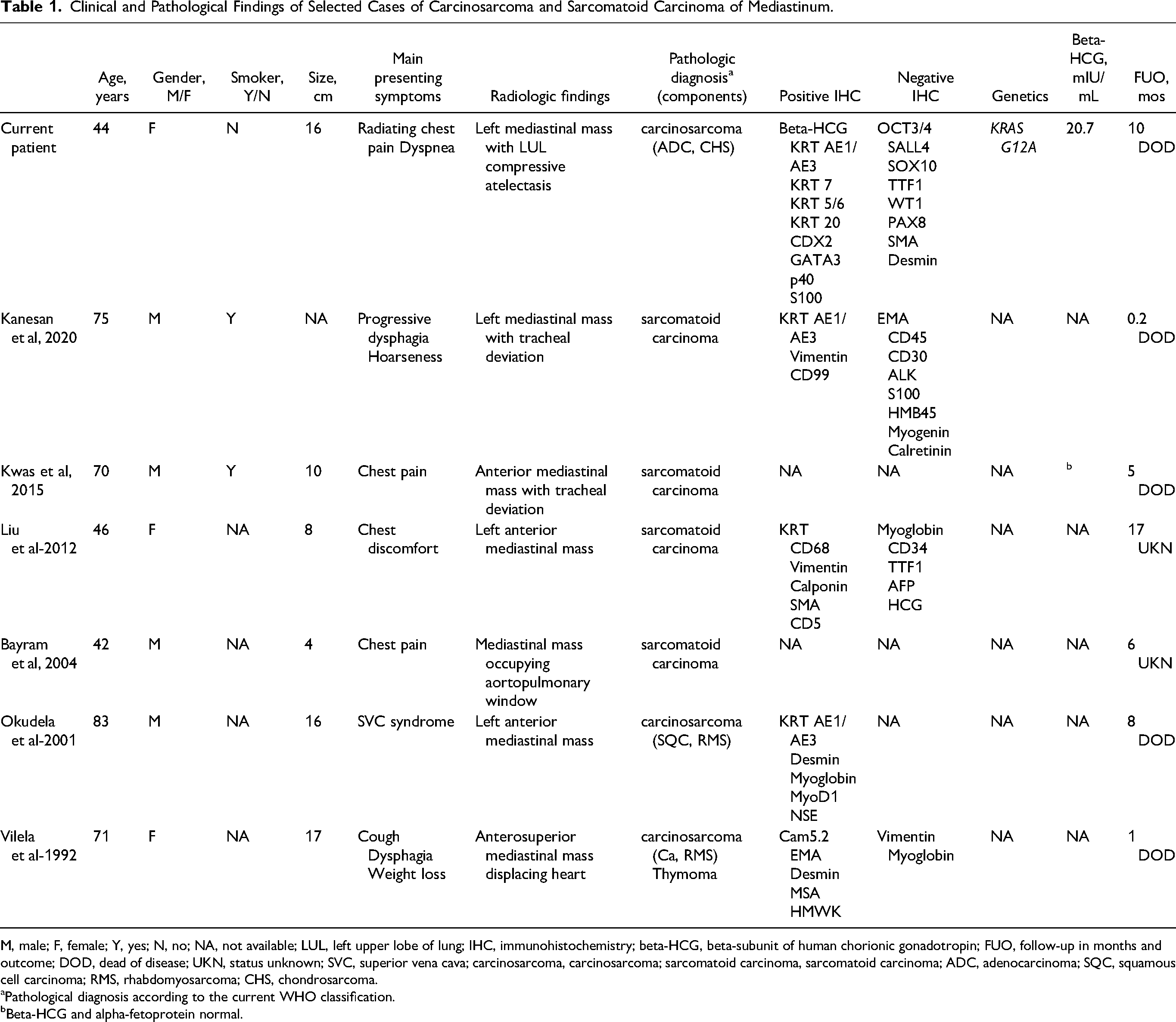
M, male; F, female; Y, yes; N, no; NA, not available; LUL, left upper lobe of lung; IHC, immunohistochemistry; beta-HCG, beta-subunit of human chorionic gonadotropin; FUO, follow-up in months and outcome; DOD, dead of disease; UKN, status unknown; SVC, superior vena cava; carcinosarcoma, carcinosarcoma; sarcomatoid carcinoma, sarcomatoid carcinoma; ADC, adenocarcinoma; SQC, squamous cell carcinoma; RMS, rhabdomyosarcoma; CHS, chondrosarcoma.
Pathological diagnosis according to the current WHO classification.
Beta-HCG and alpha-fetoprotein normal.
In conclusion, this report documents a rare presentation of carcinosarcoma arising within the mediastinum. The tumor beta-HCG production and the presence of a KRAS mutation comprise unique clinical and genetic manifestations of the disease. 21
Footnotes
Abbreviations
Acknowledgments
The authors are thankful to Shawn Scally for excellent assistance in figures preparation.
Author Contributions
NS, MW, DAL, and GAO participated in data collection; NS and KS wrote the manuscript text; MW, CCA, GAO, and KS edited the manuscript. The authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
This study is exempt from the regulatory requirements of the National Institutes of Health (NIH) regarding studies on human subjects, based on the criteria described in section 4 of 46.101(b) of 45 CFR 46 “as research involving the collection or study of existing data, documents, records, if the information is recorded by the investigator in such a manner that subjects cannot be identified, directly or through identifiers linked to the subjects”. According to the institutional guidelines, the patient's consent is not necessary for a case report with de-identified patient specific information.
Trial Registration
Not applicable, because this article does not contain any clinical trials.