
Abstract
Hyalinizing trabecular tumor (HTT), a rare low-malignant-potential thyroid neoplasm, is usually treated with conservative surgery. However, cytomorphological diagnosis of HTT is challenging due to the significant overlap of nuclear features with more common malignancies such as papillary thyroid carcinoma (PTC), which usually requires more radical surgical intervention. To avoid unnecessary overtreatment, a precise diagnosis of HTT is therefore essential. Advances in molecular diagnostics provide the opportunity to overcome the limitations of cytological analysis. We present a case of HTT in a 71-year-old male who was initially suspected to be PTC based on cytopathology. However, further molecular analysis revealed PAX8::GLIS3 gene fusion, classifying the lesion as HTT and preventing surgical overtreatment. We discuss the diagnostic pitfall of cytopathology in HTT and suggest using emerging molecular genetic tools to avoid it.
Introduction
Hyalinizing trabecular tumor (HTT), an uncommon follicular cell-derived thyroid neoplasm, 1 was initially included in the World Health Organization's (WHO) thyroid tumor classification in 2004. 2 In the majority of cases, HTT is a low-malignant-potential tumor 3 and is usually treated with conservative thyroid surgery.1,4 The cytomorphological diagnosis of HTT is challenging due to the significant overlap of nuclear features with more common malignancies such as papillary thyroid carcinoma (PTC). 5 PTC is the most prevalent malignant thyroid tumor 6 and requires radical resection of thyroid. 7
Only 8% of cases result in a definitive preoperative cytological diagnosis of HTT.1,8 Therefore, per the Bethesda System for Reporting Thyroid Cytopathology, this entity is typically classified as indeterminate or suspicious for malignancy, suspicious for PTC. 9 Additionally, per the literature, cytological findings showing more than 2 nuclear pseudoinclusions are reported to be associated with PTC. 10 Nonetheless, the precise diagnosis of HTT is crucial to prevent inappropriate overtreatment. 11 Molecular tests have been developed in recent years to overcome the limitations of the cytological analysis. 12 Particularly, the PAX8::GLIS3 fusion gene has been found to be pathognomonic for HTT.3,4
We present a case of HTT initially suspected to be PTC based on cytological morphology; however, molecular testing (ThyroSeq® v3 GC, ThyroSeq; a joint partnership between the University of Pittsburgh Medical Center and Sonic Healthcare, USA) revealed a PAX8::GLIS3 gene fusion, classifying the lesion as HTT. Our report explores the difficulties of cytopathological diagnosis and the use of emerging molecular genetic tools to enhance diagnostic accuracy and prevent overtreatment.
Case Report
A 71-year-old white male with a history of hypothyroidism, was incidentally discovered to have multiple thyroid nodules following chest imaging performed to evaluate a parapneumonic pleural effusion. Subsequent thyroid ultrasound revealed multiple bilateral thyroid nodules with a subcentimeter nodule in the right lobe adjacent to the isthmus. The patient was clinically followed up with an endocrinologist. His thyroid ultrasound remained stable for 2.5 years. However, when sonographic reassessments indicated progressive enlargement of the nodule of interest (1.5 cm in the greatest dimension), he was referred for a fine needle aspiration (FNA) procedure. The patient underwent an FNA, during the procedure a dedicated pass for ThyroSeq® V3 was performed and collected in a transport vial.
The cytomorphological evaluation of FNA smears showed a hypocellular material with a few clusters of follicular cells with absent stromal hyaline material. The tumor cells were cohesive and exhibited a moderate nuclear to cytoplasmic ratios with enlarged elongated nuclei, nuclear overlapping, and pale chromatin. Few cells showed nuclear grooves; and at least 5 nuclear pseudoinclusions were observed (Figure 1). No papillary formations and psammoma bodies were noted. Based on these cytological features, the FNA was classified as “suspicious for malignancy” (suspicious for PTC). A cell block was not prepared, immunohistochemical stain could not be performed. Due to patient's concerns about the FNA results and proposed surgical intervention, the clinical team ordered a molecular test, ThyroSeq, to confirm the cytological interpretation. The molecular study, ThyroSeq® v3 GC, showed a PAX8::GLIS3 fusion, classifying the tumor as HTT; and, subsequently, a right thyroid lobectomy was performed.
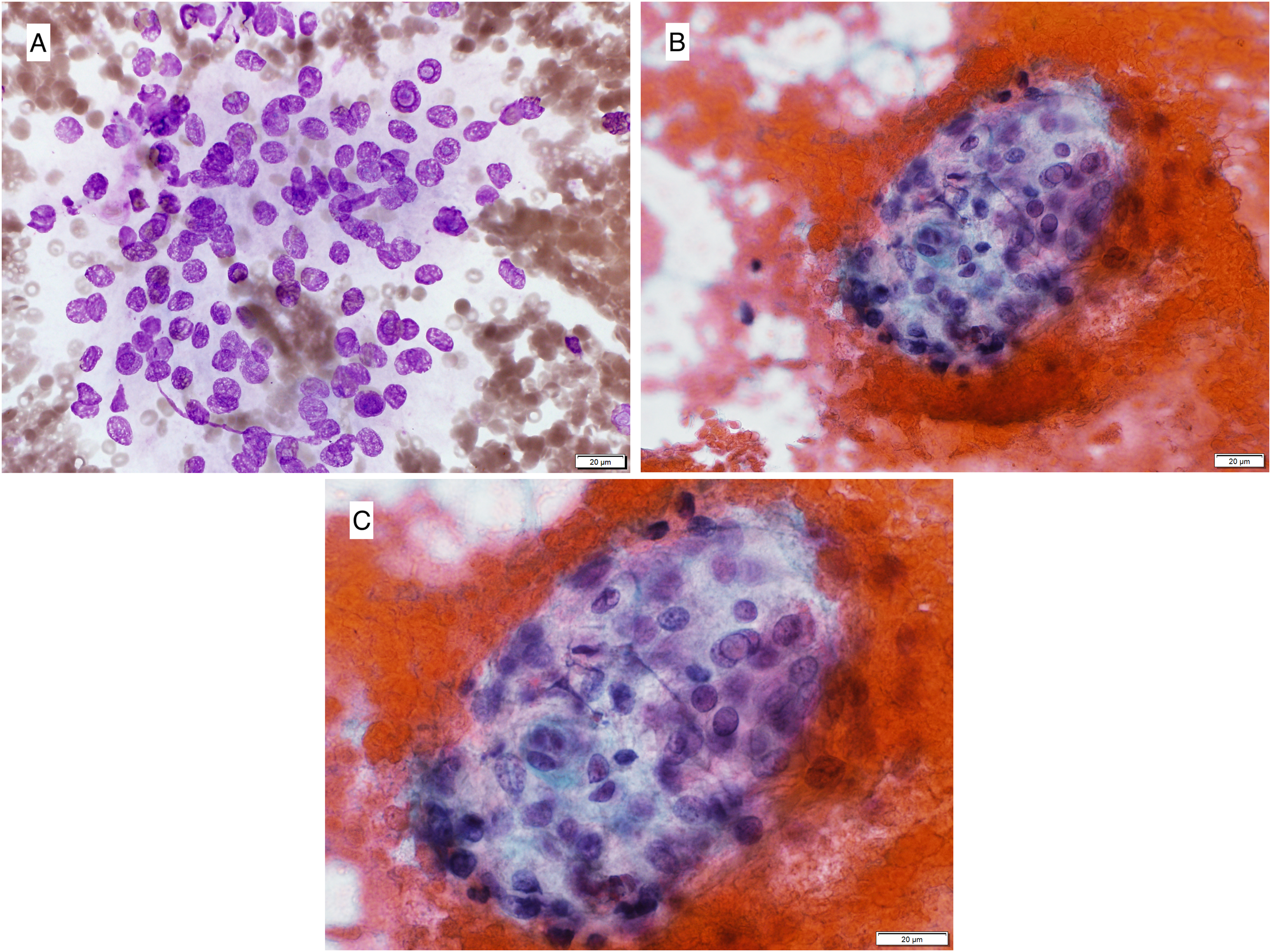
Fine needle aspiration cytology smear of right thyroid nodule. (A) A cluster of tumor cells with frequent intranuclear pseudoinclusions (Diff-Quik, 400x). (B) A cluster of tumor cells with nuclear grooves and pseudoinclusions (Papanicolaou, 400x). (C) A cluster of tumor cells with nuclear grooves and pseudoinclusions (Papanicolaou, 600x).
A gross examination of the surgical specimen revealed that the nodule of interest was a well-circumscribed, partially encapsulated, yellow-tan nodule under the capsule of the right thyroid lobe. On microscopic examination, the lesion showed a trabecular architecture, with marked inter-trabecular and intra-trabecular deposition of hyalinized material (Figure 2). The tumor cells were polygonal to columnar with an eosinophilic to clear cytoplasm. The nuclei were diffusely enlarged with clearing, grooves, and abundant pseudoinclusions. No papillary formations or other malignant morphological features, including capsular or vascular invasion, were observed. An immunohistochemical study showed negativity for calcitonin. Given the prior molecular findings and histological findings, a diagnosis of HTT was reached. The patient has been followed up for a year without local recurrence or metastasis.
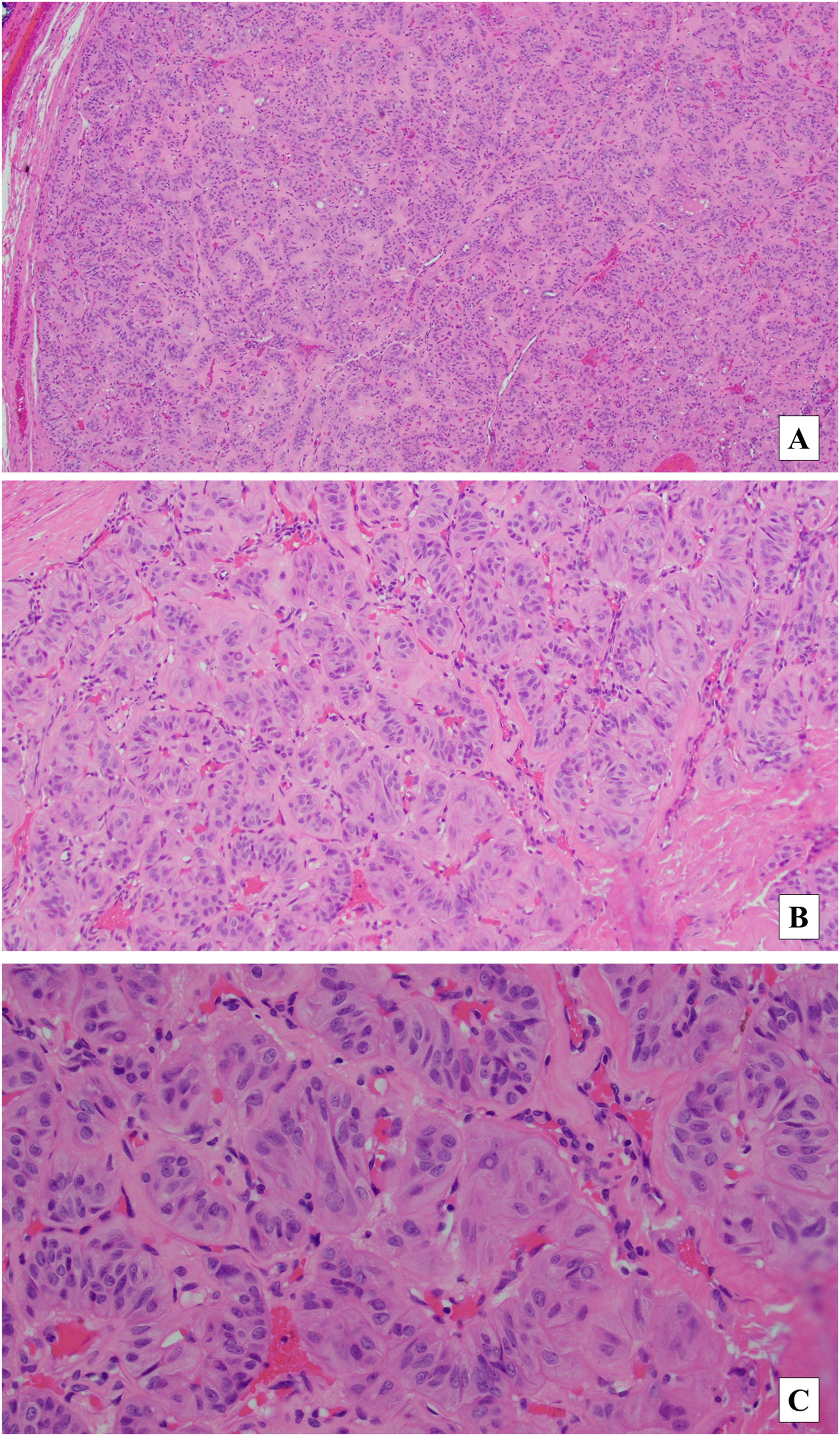
Histological section of hyalinizing trabecular tumor resection specimen. (A) Encapsulated tumor with trabecular architecture (H&E 40x). (B) Cellular nest of polygonal cells in hyalinized stroma (H&E 100x). (C) Cells with elongated nuclei, nuclear pseudoinclusions, nuclear grooves (H&E 400x). Abbreviation: H&E, hematoxylin and eosin.
Discussion
Although initially observed in 1905, HTT was not characterized completely until 1987. 13 HTT was initially assumed to be a benign entity with trabecular growth and hyalinizing stroma. Thus, the term hyalinizing trabecular adenoma was used. 14 However, as some scholars considered the lesion had intermediate malignant potential, 15 the WHO has adopted the term HTT due to the low malignant potential of the tumor.2,16
The cytopathological diagnosis of HTT remains challenging as it displays some cellular characteristics similar to PTC. 17 Despite HTT exhibiting several unique cytomorphological traits such cellular aggregates within hyaline matrix, no papillary formations, low nuclear to cytoplasmic ratio, and fine chromatin, 18 both HTT and PTC can exhibit hypercellularity, and cellular atypia including nuclear clearing, grooves, and pseudoinclusions on FNA.13,19,20 However, the accurate diagnosis of HTT is critical as it guides the course of treatment. In our case, the limiting factor for the cytological interpretation was the specimen cellularity and the lack of hyalinizing material in the smears, and the material was interpreted as “suspicious for PTC.”
Lobectomy is the preferred surgical management for HTT. 21 On the other hand, according to the National Comprehensive Cancer Network (NCCN) guidelines, a diagnosis of PTC or “suspicious for PTC” may require either a thyroidectomy or lobectomy; a more aggressive surgical intervention still might be entertained for our patient. In the guidelines, if there are known distant metastases, extrathyroidal extension, a tumor larger than 4 cm, lateral cervical lymph node metastases, extensive central lymph node metastases, a poorly differentiated tumor, a history of previous radiation, and bilateral nodularity, a total thyroidectomy is recommended. 22 Therefore, although the NCCN guidelines may limit excessive intervention, an inaccurate diagnosis of HTT may still lead to unwarranted overtreatment if the patient has bilateral nodularity. In a large series of HTT cases, Dell’Aquila et al 18 demonstrated that over 80% of HTTs were diagnosed in the indeterminate Bethesda categories, including, 22.2% atypia of undetermined significance, 33.3% suspicious for follicular neoplasm, 28% suspicious for malignancy. Furthermore, Saglietti et al 8 have documented that 60% of published HTT cases were diagnosed as suggestive, suspicious or positive for PTC. Therefore, these patients with HTT might be overtreated and are unnecessarily exposed to additional surgical risks, reduced quality of life, unnecessary healthcare, and treatment costs.
In this respect, molecular testing can yield reliable results and be used as a de-escalation tool to facilitate an accurate diagnosis of HTT and contribute to a reduction in overtreatment.1,3,4 Molecular testing of FNA biopsies for markers such as BRAF, RET/PTC, PAX8/PPAR, and RAS can dramatically enhance the precision of preoperative FNA diagnosis by cytology. 23 Furthermore, the use of molecular markers for cytological samples interpreted as indeterminate groups24–26 including follicular lesions of undetermined significance/atypia of undetermined significance (FLUS/AUS; Bethesda III), follicular neoplasms/suspicious for follicular neoplasm (FN/SFN; Bethesda IV), and suspicious for carcinoma (Bethesda V) categories, are now explicitly recommended in the “2009 Revised American Thyroid Association Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer” 27 and the NCCN guidelines. 22 However, in the NCCN guidelines, a cytological diagnosis of “suspicious for PTC” has the same management as a PTC. 22 This case highlights the importance of the use of ancillary testing even in cases in which the cytomorphology was classified as suspicious for PTC; as the molecular testing in our case revealed the PAX8::GLIS3 fusion. This additional testing prevented surgical overtreatment.
Nikiforov et al 3 highlighted the significance of PAX8::GLIS3 rearrangement as a genetic hallmark of HTT. Using whole-exome, RNA-sequencing, and targeted next-generation sequencing analyses, they identified the PAX8::GLIS3 gene fusion in 93% and PAX8::GLIS1 gene fusion in 7% of histopathologically confirmed HTT cases. GLIS3, a member of the GLI-like zinc finger protein family, functions as a transcription modulator and is involved in thyroid gland development.1,3 Interchromosomal rearrangements that lead to the fusion of the GLIS3 gene to PAX8 produced chimeric transcripts and significant overexpression of extracellular matrix-related genes (multiple collagen genes), likely responsible for excessive collagen synthesis and deposition in HTT. 3 This considerable hyalinization gives these tumors their distinctive microscopic appearance and nomenclature. Furthermore, in their study, they analyzed 220 histopathologically confirmed PTC cases and observed no PAX8::GLIS3 fusion. 3 A recent multi-institutional study validated the findings of Nikiforov et al 3 by confirming the presence of PAX8::GLIS3 fusion in all of the examined histologically verified HTT cases. 4 They also confirmed the genetic specificity of this gene, as none of the control thyroid tumors of various histologies (including PTC) harbored the PAX8::GLIS3 fusion. 4 Although previous publications reported that HTT can harbor RET/PTC1 rearrangements (28.6% according to Papotti et al 28 and 62% according to Cheung et al 29 ), subsequent studies did not support these findings.16,30 BRAF and RAS mutations, which are common in PTC and follicular variant of PTC (FVPTC), respectively, have not yet been discovered in HTT. 16 However, Dell’Aquila et al 18 found a wild type BRAFV600E in all of their reported HTT cases.
Before this molecular evidence, a conclusive diagnosis of HTT was only possible on resected specimens based on their specific morphological characteristics.1,4 Macroscopically, HTT is generally well circumscribed and encapsulated with yellow to tan color variations.13,19 PTC, on the other hand, typically appears as an invasive with poorly defined margins, a firm consistency, and a granular cut surface. 31 Microscopically, HTT demonstrates the trabecular architecture with elongated or polygonal cells arranged perpendicular to the trabecular axis. The presence of abundant hyaline material typically intra-trabecular and often embedding single or groups of tumor cells are the cardinal histological features of HTT.1,4 Cells have voluminous eosinophilic cytoplasm and elongated pale nuclei with irregular borders, grooves, and intranuclear pseudoinclusions. 32 Cytologically, HTT can be confused with PTC due to overlapping nuclear characteristics. 19 However, significant stromal hyaline material, particularly intra-trabecular hyalinization, is relatively uncommon in PTC. 1 This latter finding may be misinterpreted as PTC as it has been described that classic PTC exhibits more than 2 nuclear pseudoinclusions. 33
Nonetheless, intranuclear inclusions and other nuclear features of PTC may be also seen in noninvasive follicular thyroid neoplasm with papillary-like nuclear characteristics (NIFTP) and FVPTC. 33 Therefore, the cytological interpretation should be made with care and a molecular study may help elucidating the diagnosis, as NIFTP and FVPTC show HRAS mutations. 34 These lesions are distinguished on histological examination, NIFTP and FVPTC both exhibit a microfollicular architecture with some nuclear traits resembling PTC. 33 However, nuclear grooves and pseudoinclusions in NIFTP and FVPTC are less evident compared to PTC.35,36 NIFTP shows predominantly follicular growth pattern with < 1% papillary formations, and no capsular or vascular invasion. 37
Conclusion
HTT is usually a low-risk tumor with a favorable prognosis. Available cytopathological diagnostic techniques can create diagnostic dilemmas between HTT and other malignancies, leading to surgical overtreatment. Advances in molecular diagnostics provide the opportunity to improve precise classification of HTT and de-escalate overtreatment. Lack of molecular diagnostics in resource-limited settings remains a major obstacle. Additional studies may be considered to further elucidate the sensitivity and specificity of cytology coupled with molecular studies in the identification of HTT.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Trial Registration
Not applicable, since this report does not contain any clinical trials.