
Abstract
Introduction
HPV infections are the most common pathogens in cervical malignancies, but their prevalence varies between countries and societies. It has been reported that 12% of women worldwide are HPV DNA positive. 1 The clear relationship between cervical cancer and HPV is known, and the most responsible types are HPV 16 and 18. Of the other high-risk-HPV types 31, 33, 35, 39, 45, 51, 52, 56, 58, 59 and 68 were reported to be effective in the rest of the cervical cancer cases.2,3
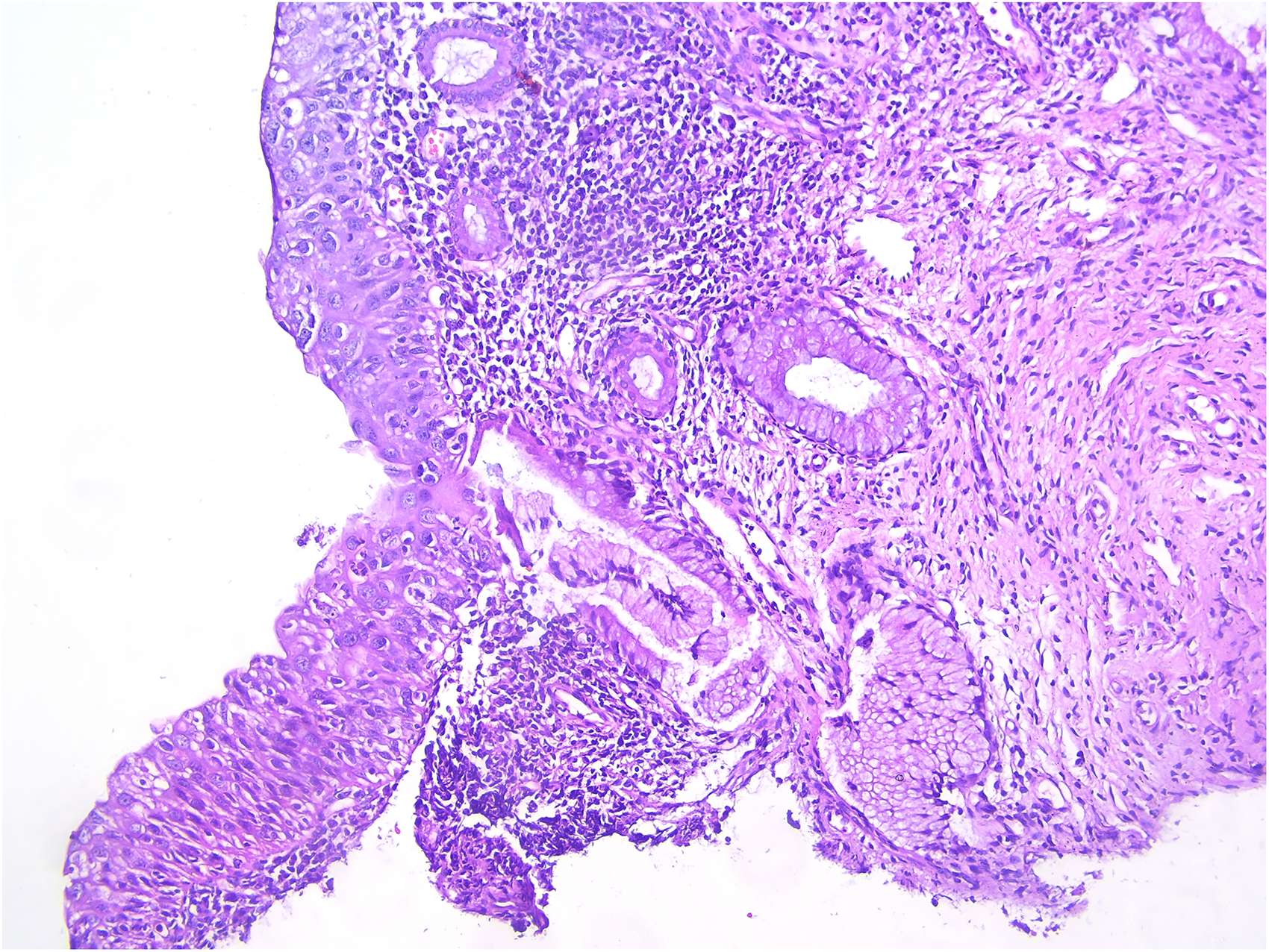
CIN3 appearance in excisional biopsy in an isolated HPV 33 positive case.
The cervical cancer screening guidelines recommend HPV testing in the women aged 25–65 years. If the test is negative, a primary HPV test is recommended every five years. 4 According to the ASCCP (American Society for Colposcopy and Cervical Pathology), the patients whose previous HPV test result is unknown require evaluation with HPV type 16 and 18 cytology-independent colposcopy with high oncogenicity, and the other high-risk group is referred to test repetition 1 year later in case of cytology abnormality.5,6 However, recent studies have shown that genotypes such as HPV 31,33,52 and 58 have a higher risk of ≥CIN 2 + than HPV 18 regardless of cytology (Figure 1). 7
Cervical intraepithelial neoplasia (CIN) types play an important role as preinvasive markers of cervical cancers. In the case of persistence of HPV infections, the risk of progression to cervical cancer increases very much.
8
Genotyping for other
We started our study with the question: “Can we reveal premalignant cervical lesions and possible cancer in a larger number and earlier period by performing colposcopic examination at the time of diagnosis instead of waiting to perform a cotest after 1 year for other high-risk HPV types (such as 31, 33, 35, 45, 51) other than type 16–18?”.
The aim of this study is to compare the colposcopic biopsy results of HPV 16, HPV 18 positive patients and patients with at least one of the high-risk-HPV subtypes and to evaluate the frequency of causing CIN2 + lesions that may require excision.
Material-Method
Our study was planned as a retrospective cohort study in the Gynecology -Oncology Polyclinic of VAN Training and Research Hospital of the University of Health Sciences and approval was obtained from the ethics committee of the same hospital on May 25, 2022 (decision no: 2022/11-04). The study was conducted within the framework of ethical rules in accordance with the Helsinki Declaration. 264 patients who applied to the gynecological oncology outpatient clinic of our hospital between March 2020 and May 2022 were included in the study. Although the screening program is based on HPV in case of HPV positivity, patients are routinely checked for smears. HPV tests used in our country; internationally valid and FDA-approved for its usability in population-based health screening, in vitro diagnostics or test specificity should meet the requirements of the European Guidelines published by Meijer et al (IJC 2009) for low-risk HPV genotypes for CIN2/3 and screening populations with minimal cross-reactivity and this must have been demonstrated in a general population primary cancer screening study with at least 2500 samples.
HPV was reported as other, 48 patients whose HPV type was not specified, 9 patients who underwent one of the excisional procedures with pathology incompatibility with colposcopy, 4 patients who underwent colposcopy due to white cervical lesion and postcoital bleeding, and 1 patient who underwent excision due to CIN1 persistence were excluded from the study, and the remaining 202 patients were included in the study based on the exclusion criteria. The patients younger than 25 years of age and older than 65 years of age, the patients smoking and using combined oral contraceptives (COCs), grandmultiparous patients, hysterectomized patients and pregnant women were excluded from the study. Exclusion criteria in the study were planned with the aim of minimizing the variables between the groups. The patients whose HPV type was not specified were those who applied to our hospital, which is a referral center, with a pathology report. In our national screening program, high-risk HPV types are indicated by their subgroups. Since high-risk HPV groups other than types 16 and 18 were the target of the study, patients whose subtypes were not specified were excluded from the study. In addition, these patients did not have a history of HPV vaccination. Although there is a more specific screening test than the smear HPV test; sensitive and more reliable, therefore, up-to-date and preferred is undoubtedly HPV screening. However, patients whose smear result was reported as a high-grade lesion were considered an exclusion criterion since HPV and colposcopic biopsy / excisional procedure results were compared, but no screening patient with such a pathology report was seen. Again, no cytological anomalies were encountered in the high-risk HPV group, except for 6 patients with ASCUS detected in cytology. As a result of colposcopy, CIN2 + patients who underwent excisional procedure were grouped according to HPV type. During this procedure, the patients who were positive for more than one HPV type were considered positive for the group with all subtypes (If the patient was type 31 and 33 positive, they were included in both the 31 and 33 positive groups). The genotype distribution of patients in the HPV group who required excision due to CIN2 + lesion was examined.
All the patients underwent colposcopy independent of HPV types and 1-3 biopsies were conducted by the same gynecologist oncologist. Conventional cytology and colposcopic biopsy were performed under optimal conditions, mostly in the proliferative phase of the menstrual period, after the treatment of gynecological infection and two days of sexual abstinence. All cytological and pathological samples were evaluated by experienced pathologists.
Data analysis was performed with IBM SPSS Statistics version 26. Colposcopy distributions of the patients included in the study according to HPV groups were analyzed with the chi-square test. Pearson test was used to examine the correlation levels between colposcopy results and HPV positive status of the patients. Correlation coefficient; A relationship between 0.00-0.30 was considered as low, between 0.30-0.70 as a medium level, and between 0.70-1.00 as a high level relationship. Logistic Regression analysis was used to estimate the probability of colposcopy results being a CIN2 + above lesion. In the whole study, the significance levels were carried out by considering the values of 0.05 and 0.01.
Results
202 patients were included in the study. The distribution of the patients included in the study according to HPV groups is shown in Table 1.
Colposcopy Distributions Based on HPV Groups.
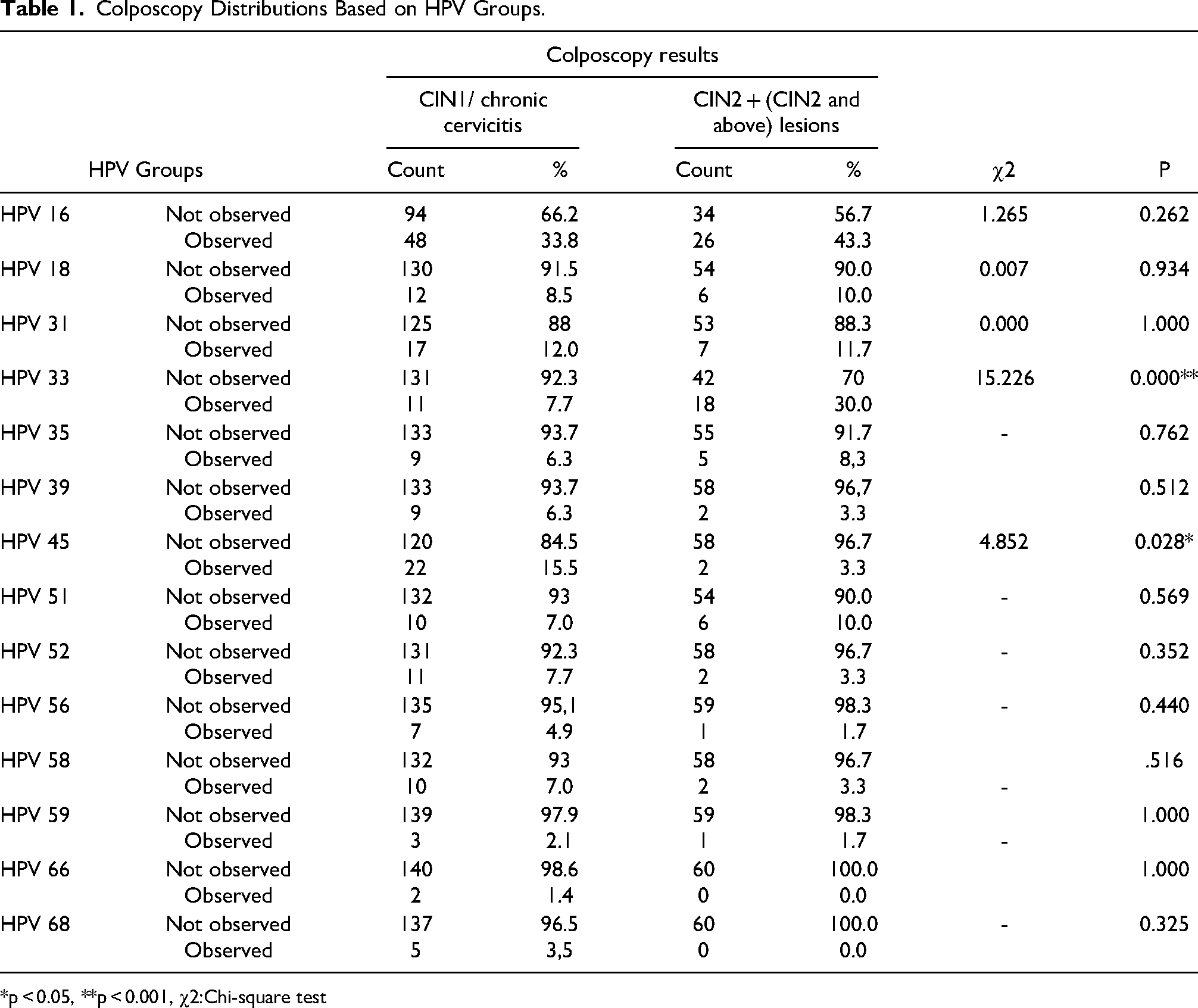
*p < 0.05, **p < 0.001, χ2:Chi-square test
When Table 1 was examined, it was determined that 43.3% of the patients with CIN2 and above lesions had HPV 16, 10% had HPV 18, 11.7% had HPV 31, 30% had HPV 33, 8.3% had HPV 35, 3.3% had HPV 39, 3.3% had HPV 45, 10% had HPV 51, 3.3% had HPV 52, 1.7% had HPV 56, 3.3% had HPV 58, 1.7% had HPV 59% and 0% HPV 66 and HPV 68 positivity. According to the colposcopy results, the HPV 33 and HPV 45 distributions of the patients were found to be different (p < 0.05). It was observed that the incidence of CIN2 + lesions in the patients with HPV 33 positive was higher than the incidence of CIN1 + chronic cervicitis in the patients with HPV 33 positive. However, it was observed that the incidence of CIN2 + lesions in the patients with HPV 45 positive was lower than the incidence of CIN1 / chronic cervicitis in the patients with HPV 45 positive. The mean age of the patients included in the study was 43.58 years.
The incidence of having CIN1 / chronic cervicitis or CIN2 + lesion in colposcopy results of the patients with positive HPV was calculated and shown in Table 2.
Incidence of Colposcopy Results of the Patients with HPV Positive Regarding CIN1 + Chronic Cervicitis or CIN2 + Above Lesion.
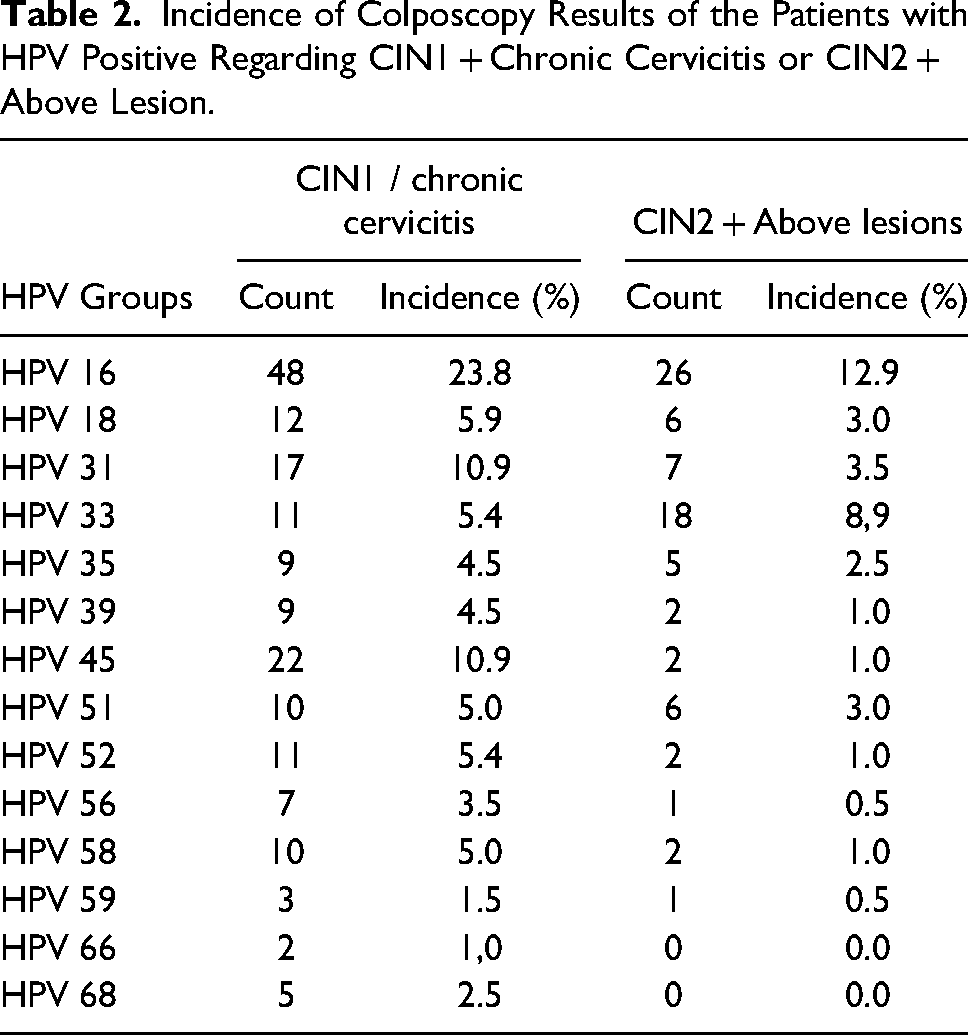
According to the incidence calculation, it was observed that the colposcopy results of the patients were found to be CIN1 / chronic cervicitis mostly when HPV 16 positive had a rate of 23.8% and HPV 45 positive had a rate of 10.9%.
It was observed that the colposcopy results of the patients were found to be CIN2 + lesions mostly when HPV 16 had a rate of 12.9% and HPV 33 had a rate of 8.9%.
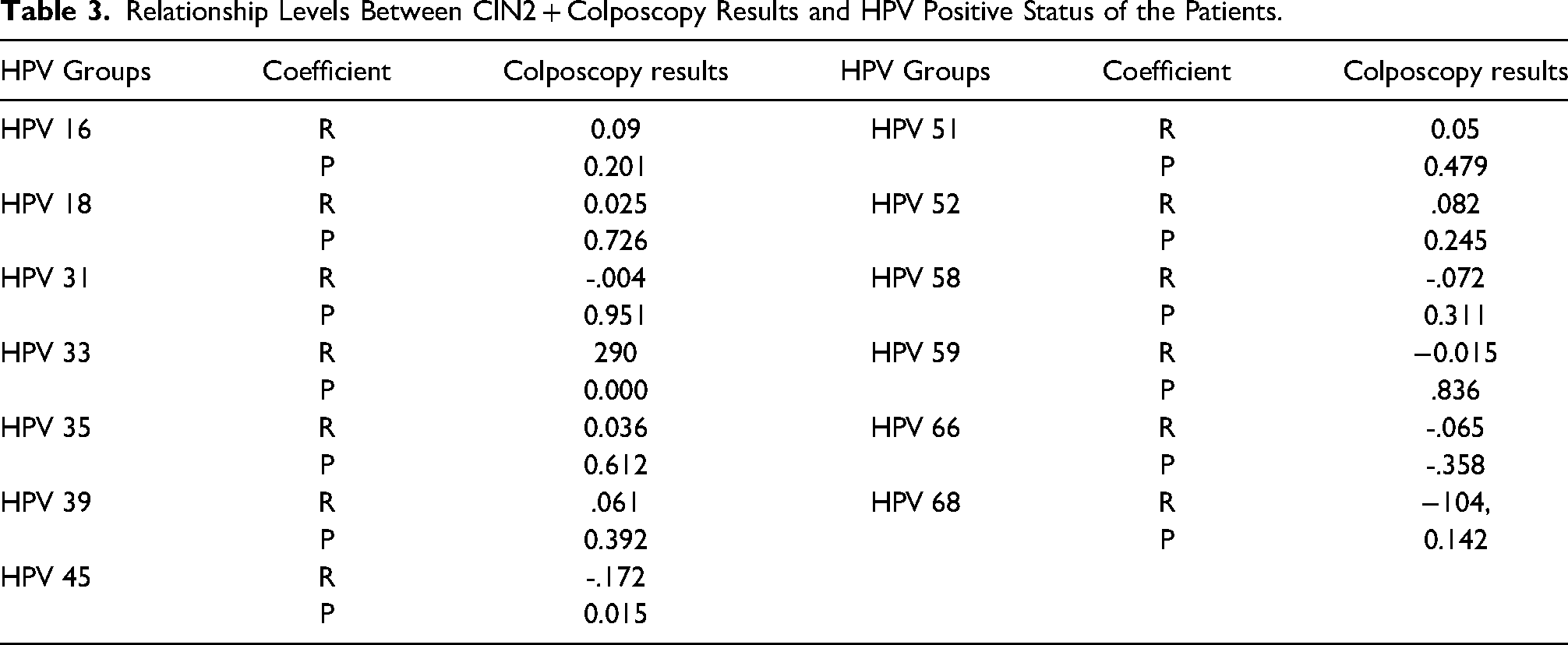
The relationship levels between colposcopy results and HPV positive status of the patients were examined and shown in Table 3. A low positive correlation was found between colposcopy results showing lesions of CIN2 and above and HPV 33 results showing positivity (p < 0.05). However, a low negative correlation was found between colposcopy results showing lesions of CIN2 and above and HPV 45 results showing positivity (p < 0.05). When these results were examined, it was observed that as the HPV 33 positivity of the patients increased, the rate of showing CIN2 and above lesions increased, and contrary to this, as the HPV 45 positivity of the patients increased, the rate of showing CIN2 and above lesions decreased.
Relationship Levels Between CIN2 + Colposcopy Results and HPV Positive Status of the Patients.
The effects of HPV Groups on the presence of CIN1 / chronic cervicitis or CIN2 + Lesions in the colposcopy results of the patients were examined by logistic regression analysis and are shown in Table 4.
Logistic Regression Predicting the Probability of CIN2 + Lesion of Colposcopy Results.
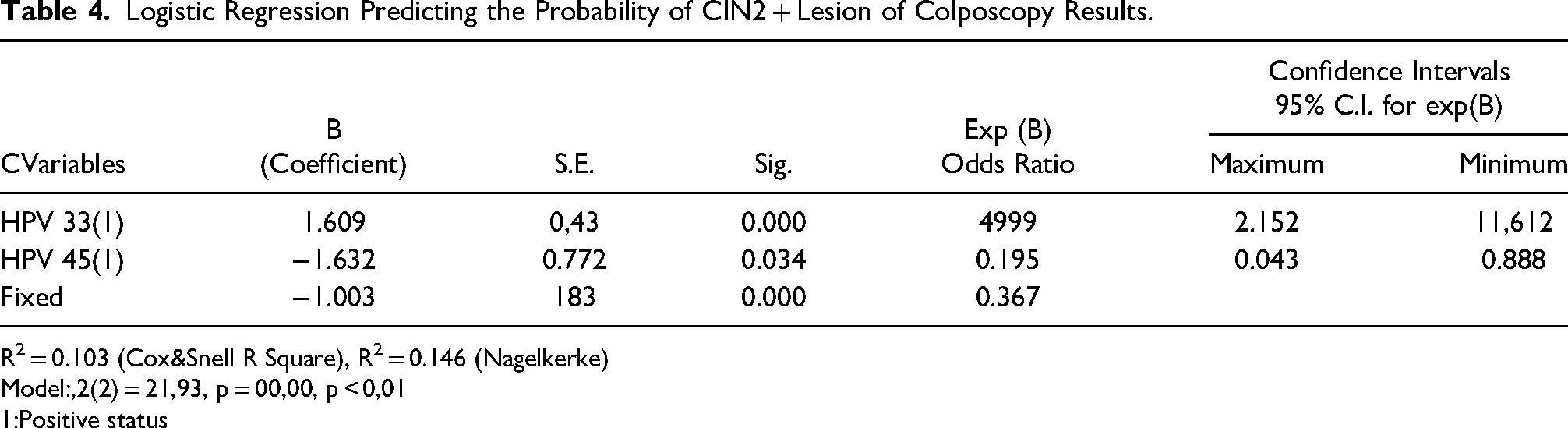
R2 = 0.103 (Cox&Snell R Square), R2 = 0.146 (Nagelkerke)
Model:,2(2) = 21,93, p = 00,00, p < 0,01
1:Positive status
HPV 33 and HPV 45, which were found to be correlated with colposcopy results, are independent variables included in this model. In the established logistic regression analysis, the model was found to be statistically significant (model, 2 (2) = 21.93, p = 00.00, p < 0.01). This model shows that colposcopy results can distinguish the presence of CIN1 / chronic cervicitis or CIN2 + lesions. In this model, the affected and those affected ones were correctly predicted at the rate of 74.8%. Independent variables explain 10.3% of the changes in the colposcopy results of the patients according to Cox & Snell and 14.6% of the changes according to Nagelkerke.
Considering the independent variables in Table 4, it was observed that HPV 33 and HPV 45 positivity were statistically significant variables in predicting the probability of the presence of CIN2 + lesions in the colposcopy results. In this model, when the Exp(B) values were examined, it was observed that a HPV 33 positive patient increased the probability of the presence of CIN2 + lesion in the colposcopy results by 4.999 times, and that a HPV 45 positive patient would decrease the probability of the presence of CIN2 + lesion in the colposcopy results by 0.195 times.
Discussion
Within the scope of our study, we evaluated the relationship between CIN1/ chronic cervicitis or CIN2 + lesion and HPV types according to the colposcopic biopsy results we performed in our clinic. According to the colposcopic biopsy results of 202 patients who were HPV positive, we found that 142 patients had CIN1 / chronic cervicitis and 60 women had ≥ CIN2 + lesions. Of these 60 patients, 26 (43.3%) had HPV 16, 18 (30%) had HPV 33, 10 (11.7%) had HPV 31, and 6 (10%) had HPV 18. The association of HPV 33 with severe cervical intraepithelial lesions was found to be more frequent than HPV 18.
After it was determined that HPV types were the main factor in the formation of cervical malignancies, the importance of these agents increased and protective measures and medical treatment methods started to be discussed in more detail.10,11 The increased risk of developing cervical intraepithelial neoplasia (CIN) and cervical cancer in the presence of HPV 16, 18 and high-risk-HPV types is clear. HPV infection is more common in younger women, but most of them are spontaneously cleaned from the body within the first two years after infection.12,13 According to the International Agency for Research on Cancer (IARC) report, HPV 16/18 accounts for more than 70% of cervical cancers and is responsible for approximately 20% of other high-risk-HPV types (HPV 31, 33, 35, 45, 52 and 58) that are not infected with HPV16/18.2,14
HPV genotype rates differ significantly between societies depending on lifestyle, race and geography differences. This distribution difference data also has an important role for vaccination programs and can change the effectiveness of the screening programs of countries. 15 Bayezıt et al reported that 49% of women with normal cervical cytology were HPV-DNA positive and 75% of women with a high-risk HPV positive had normal cervical cytology. In the same study, the most common HPV types were listed as HPV 58, HPV 16, HPV 31, HPV 33, HPV 11 and HPV 35. 16 In a study in which 1 million women over the age of 30 were screened by HPV test, HPV DNA positivity was found to be 3.5%. The most common HPV genotype in this study was 16, followed by 51, 31, 52, and 18. Among 37,515 HPV positive cases, the rate of cytological abnormality was 19.1%. 17 Although morbidity-mortality and frequency have decreased significantly as a result of screening programs to protect against cervical cancer, it is an important problem especially in developing countries. However, there is diversity in the conduct of screening programs, and discussions are still underway for the best screening model. Among the screening programs, only HPV test, only cytology test or the combination of HPV test and cervical cytology were recommended.18,19 In the review of the literature, it has been observed that false negativity rates can be up to 65% in the patients followed-up only with pap-smear, and in this case, delayed diagnosis, therefore CIN / cervical cancer detection, can be skipped until advanced stages.20,21 In the screening and management of cervical cancer, many countries follow-up patients according to the algorithms of the American Society of Colposcopy and Cervical Pathology (ASCCP). According to the ASCCP guideline, colposcopy is recommended immediately in HPV 16 or 18 positive cases regardless of cytology results and follow-up after 1 year is recommended in the presence of other high-risk-HPV subtypes with negative cytology. 22 In such a case, it has been stated that the risk of cervical intraepithelial neoplasia should be questioned if non-HPV 16–18 high-risk-HPV types are followed-up. 23 In this study, we aimed to contribute to the questioning of possible and unpredictable CIN detection by performing colposcopy immediately after the follow-up procedure to be performed 1 year in the patient groups with high-risk-HPV with negative cytology.
In the study conducted by Wang et al on 1387 women diagnosed with CIN 2 + , high-risk HPV positivity was found to be 91.6%. In the same study, the types most commonly associated with CIN 2 + were listed as HPV 16,58,33 (59.3%, 14.4%, 10.0%) and HPV 18 type was ranked sixth with a rate of 6.0%. 24 In a recent study, HPV 16 was found to be ranked first with 11.2% and HPV 31 was ranked second with 7.5% in the patients with CIN 2 + . In the same study, HPV 18 was reported to be in the moderate risk group with 2.9%. 25 In another comprehensive study, it was reported that HPV 18, which is generally the second most common among high-risk-HPV types, has less relationship with CIN 2 + than thought. 26 In the study conducted by Zhang Q et al, high-risk-HPV infection was detected in a total of 2264 women aged 25 years and older by primary genital system high-risk-HPV infection screening, and colposcopy was recommended for 1916 of them. The distribution of HPV 16, HPV 18 and other high-risk HPV infection was 49.22%, 9.45% and 41.33%, respectively. The most common genotype was HPV 16, it was followed by HPV 58, HPV 52, HPV 18 and HPV 33. There was a difference in the high-risk-HPV distribution associated with CIN. The most common types observed in the women with CIN2 + were HPV 16, HPV 18, HPV 58, HPV 52 and HPV 33, respectively. Two common types, HPV 16 and HPV 18, accounted for 82.6% of total CIN2 + cases. 27 In a study conducted in Thai women, 50% of CIN 2 + lesions were associated with HPV 16 and 18, and CIN 1 was detected in 7% of lesions. 15 In the same study, it was found that high-risk-HPV types other than HPV16 and 18 were in 18.1% of CIN 1 lesions and in 30.8% of ≥ CIN 2 lesions. 15 HPV16 is the most common high-risk-HPV type, followed by HPV 51 and HPV 52. In this study, the prevalence of HPV 18 was only 0.53% (n = 8). 28 We included 202 patients who underwent colposcopic biopsy after exclusion criteria. When the colposcopy results were examined, it was found that 43.3% of the patients with CIN2 + lesions had HPV 16, 30% had HPV 33, 11.7% had HPV 31% and 10% had HPV 18. Among the high-risk-HPV types, HPV type 33 was found to be less than HPV 16 but more common than HPV 18 in terms of association with cervical neoplasia. It was observed that the incidence of CIN2 + lesions in the patients with HPV 33 positive was higher than the incidence of CIN1 / chronic cervicitis in the patients with HPV 33 positive. It was found that the incidence of CIN2 + lesions in the patients with HPV 45 positive was lower than the incidence of CIN1 / chronic cervicitis in the patients with HPV 45 positive. In other words, while a positive correlation was observed between CIN 2 + lesion and HPV 33, a negative correlation was found between HPV 45. Based on the incidence calculations, it was observed that the colposcopy results of the patients were found to be CIN2 + lesions mostly when HPV 16 had a rate of 12.9% and it was followed by HPV 33 with a rate of 8.9%. It was observed that a HPV 33 positive patient increased the probability of having a CIN2 + lesion by 4.9 times. In conclusion, there is also a risk of cervical preinvasive lesions is associated with being infected by the high-risk-HPV types other than HPV types 16 and 18 and this risk cannot be ignored. Although HPV 16 is predominant, HPV 18 and other high-risk HPV genotypes -especially HPV type 33- pose a risk for CIN2 or higher lesions and cervical cancer. Based on the results of this study, we think that colposcopy should be supported immediately after the detection of HPV 33, which has a weak relationship with CIN 1 / chronic cervicitis lesions but increases the risk of CIN 2 + approximately 4.9 times.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Van training and research hospital ethics committee Decision No: 2022/11-04.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The authors have obtained the necessary consent.